
Abstract
Background
Concussion is common in the sporting arena and is often challenging to diagnose. The development of wearable head impact measurement systems has enabled measurement of head kinematics in contact sports.
Objectives
The objective of this systematic review was to determine the characteristics of head kinematics measured by an accelerometer system among male athletes diagnosed with concussion.
Methods
A systematic search was conducted in July 2015. Inclusion criteria were English-language studies published after 1990 with a study population of male athletes, in any sport, where objectively measured biomechanical forces were reported in the setting of a concussive event. The random effects meta-analysis model was used to combine estimates of biomechanical force measurements in concussed athletes.
Results
Thirteen studies met the inclusion criteria, the majority of which were conducted with high school and college football teams in the US. Included studies measured a combination of linear and rotational acceleration. The meta-analysed mean peak linear head acceleration associated with a concussive episode was 98.68 g (95 % CI 82.36–115.00) and mean peak rotational head acceleration was 5776.60 rads/s2 (95 % CI 4583.53–6969.67). The estimates of the biomechanical forces were consistent across studies, with I 2 values of 0 % for both meta-analyses.
Conclusions
Head impact monitoring through accelerometery has been shown to be useful with regard to characterising the kinematic load to the head associated with concussion. Future research with improved clinical outcome measures and head kinematic data may improve accuracy when evaluating concussion, and may assist with both interpretation of biomechanical data and the development and utilisation of implementation strategies for the technology.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
This systematic review attempted to determine the biomechanics of concussive head impacts among male athletes in any sport. |
Mean peak linear head acceleration associated with a concussive episode was 98.68 g (95 % CI 82.36–115.00) and mean peak rotational head acceleration was 5776.60 rads/s2 (95 % CI 4583.53–6969.67). |
These findings do not define a concussion threshold but are useful with regard to characterising the kinematic load to the head associated with concussion. |
1 Introduction
In Australia, 80–90 % of traumatic brain injuries (TBIs) sustained are classified as mild TBIs (mTBIs) [1, 2]. Evidence suggests that 21 % of all TBIs occur during sporting activity and equate to an incidence rate of 170 per 100,000 of general population [3]. Concussion is a growing concern in the sporting arena, with an estimated 1.6–3.8 million sport-related concussions occurring annually in the US alone [1]. Concussion, a subset of TBI, is a complex pathophysiological process affecting the brain, induced by biomechanical forces and resulting in impairment of neurological function, often without readily identifiable structural injury on standard neuroimaging [4].
The incidence of concussion is likely to be underestimated, primarily due to under- or delayed diagnosis [5, 6] as concussion is widely underreported in both the sporting arena and the broader community [7, 8]. The development of instrumentation to measure head kinematic responses during head impacts in sport resulted from a need to better understand the biomechanics of concussion in sport and concussion aetiology. Goals of head instrumentation include measuring head impact exposure, improving head protection and assisting in the medical management of athletes [9–11].
Head impact data suggest that the majority of recorded impacts are skewed towards the low end of the severity spectrum. Although these impacts pose minimal risk of observable concussion, the long-term consequences of repetitive subconcussive head impacts remain largely unknown [12, 13]. Repeated head impact has been recently linked with chronic traumatic encephalopathy (CTE) through several case studies; however, given the absence of cross-sectional, longitudinal, or prospective studies, the association is not yet established [14–17].
Previous reviews conducted examining head impact biomechanics have focussed solely on American Football [18, 19] and have included issues pertaining to the overall assessment and management of sports-related concussion [20]. The objective of this systematic review was to determine the characteristics of measured head kinematics in the setting of concussion among male athletes in any sport in which head impact was measured by an accelerometer system. On average, female and youth athletes sustain concussions at lower magnitudes when compared with males [21]. These populations have been excluded in order to keep the biomechanical data consistent and improve external validity when applied to a male population.
2 Methods
This systematic review was conducted and reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement [22]. A protocol was registered on PROSPERO (registration number CRD42015024857) and can be accessed at http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42015024857.
2.1 Information Sources
The search strategy involved a combination of keywords and subject headings from the MEDLINE, PubMed, Cochrane Library, Scopus, PsycINFO and SPORTDiscus databases (1990–July 2015). The following keywords (truncated as appropriate) were used: ‘head acceleration’, ‘accelerometer’, ‘sensor*’, ‘acceleration’, ‘biomechanics’, ‘injury threshold’, ‘concuss*’ (concussion, concussed, concussive), ‘brain inj*’ (brain injury, injuries), ‘head inj*’ (head injury, injuries), ‘mild traumatic brain injury’, ‘head impact’, ‘sport injury’, ‘sport*’, ‘athlete*’, ‘football’, ‘soccer’, ‘ice hockey’, ‘rugby’, ‘boxing’, ‘lacrosse’, ‘wrestling’, ‘tae kwon doe’, ‘karate’, and ‘martial arts’. Medical Subject Heading (MeSH)/EMTREE terms used included ‘acceleration’, ‘accelerometry’, ‘brain concussion’, ‘post-concussion syndrome’, ‘brain injuries’, and ‘sports’. Reference lists of identified relevant studies and recent books were hand-searched to identify further studies. Citations were downloaded to Endnote and duplicates removed.
2.2 Study Inclusion Criteria
Studies were included if they met the following inclusion criteria: the study was published in English post-1990, included a population of male athletes in any sport and objectively measured biomechanical forces, specifically linear and rotational acceleration, with a head instrumentation system, and linked the measured forces to a clinical diagnosis of concussion. Studies conducted on high school and collegiate athletes were eligible for inclusion in this systematic review. Inclusion and exclusion criteria are described in Table 1.
2.3 Study Selection
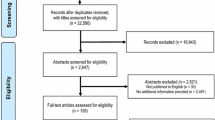
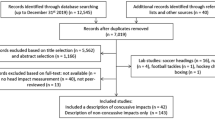
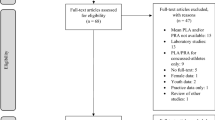
Two review authors independently screened publication titles and abstracts using the predefined eligibility criteria. Any citation selected by either author was retrieved for full-text review. The same two review authors independently assessed the eligibility of full-text articles for inclusion. Differences in screening decisions were resolved by discussion or consultation with a senior member of the review team. The study selection process was documented according to the PRISMA flowchart [23].
2.4 Data Collection
Data on level of sport, method of head acceleration measurement, session type, helmeted versus non-helmeted population, brand of head impact monitoring system used and sources of study funding were extracted. The number of participants, number of head impacts and the biomechanical data (mean peak linear and rotational acceleration) for concussive impacts were also extracted. For those studies that presented individual participant data for the biomechanical measures, we aggregated the measures for inclusion in the meta-analysis.
2.5 Risk of Bias Assessment
The Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) framework was used to assess the risk of bias in the included studies. It assesses four study domains: patient selection, index test, reference standard and flow of patients through the study. All four domains are assessed for risk of bias, with the first three also assessed for concerns regarding applicability [24]. Signalling questions were tailored as appropriate for this review. Risk of bias and applicability was identified as either ‘high’, ‘low’ or ‘unclear’ in each of the domains.
2.6 Meta-Analysis
Studies were first grouped according to whether they measured mean peak linear or rotational acceleration in the setting of concussion. As studies were considered clinically homogenous (in terms of population, sport setting and outcomes) we undertook meta-analyses of mean peak linear and rotational acceleration for participants who experienced a concussive event. We combined estimates using inverse-variance weighting, using a random effects model, where the between-study variance was estimated using DerSimonian and Laird’s method of moments estimator [25]. Heterogeneity between studies was assessed using the Chi-square statistic and quantified using the I 2 statistic. Statistical analyses were conducted using Stata version 11.0 (StataCorp LP, College Station, TX, USA).
3 Results
Of the 6581 de-duplicated citations initially identified, 58 citations were sourced in full text. Of these, 39 manuscripts were excluded for not reporting appropriate outcomes or not providing the raw biomechanical data for concussive episodes. In addition, one manuscript was excluded due to an overlap of data [26]. A further three manuscripts [27–29] were excluded as data from these studies were collated in one included study [30]. A further two studies were excluded as they addressed youth [31] and female athletes [21]. Hence, a total of 13 studies were included in the review (Fig. 1).

Study selection process
3.1 Study Characteristics
All included studies were prospective cohort studies. The majority recruited American Football athletes at either a high school, collegiate level, or both, with two also incorporating data from ice hockey [6, 32] and one study solely addressing amateur rugby union athletes [13]. Accelerometers employed in all studies except King et al. [13] were instrumented helmets using the Head Impact Telemetry (HIT) System (Simbex, Lebanon, NH, USA) technology as a part of the Sideline Response System (Riddell, Elyria, OH, USA). King et al. employed instrumented mouthguards(X2 Biosystems, Seattle, WA, USA) in their study as rugby union is an unhelmeted sport [13]. All included studies measured head kinematics in both practice and games. Study characteristics are described in Table 2.
3.2 Concussion Definitions and Assessment
In the five studies that reported a definition of concussion, this was consistently defined as an impact-induced alteration in mental status [32–36]. In those studies that did not define concussion, the diagnosis was left to the trainer or medical professional [6, 12, 13, 30, 37–40].
All included studies identified concussive impacts through clinical diagnosis. It is unclear whether sideline assessment tools such as the Sports Concussion Assessment Tool (SCAT) [41] were utilised to assist in the diagnosis of concussion. Demographic and biomechanical data extracted are described in Table 3.
3.3 QUADAS-2: Risk of Bias and Applicability Concerns
Patient selection risk of bias and applicability concerns were assessed as low risk in the majority of studies [12, 13, 30, 32–40, 42]. The study by Duhaime et al. [6] was considered to have a high risk of bias and applicability concerns as four concussive events were excluded due to the lack of biomechanical data.
All included studies were considered to have a high risk of bias for index testing as biomechanical data were interpreted with the knowledge of all included concussive events. Furthermore, despite previous validation of head impact measurement systems [43–45], the validity of biomechanical data recorded could not be adjusted for in this review. When considering applicability concerns for index testing, almost half of the studies included [6, 13, 37–40] were deemed to be high risk as they were either directly funded by or had a co-author who had a vested financial interest in the accelerometery system used in each study. Two studies [34, 36] did not provide information on sources of funding or conflicts of interest, and a further five [12, 30, 32, 33, 35] included studies were deemed to have a low risk of bias with no conflict of interest identified.
Reference standard risk of bias was considered to be unclear as, although it was interpreted without knowledge of biomechanical forces, it cannot be known whether all concussions were identified by clinical staff. Due to the nature of concussion, it is unlikely that all concussions were identified by clinical staff and this cannot be adjusted for in this review. Applicability concerns were considered low risk in all included studies. Flow and timing was considered low risk in all studies. Results are described in Table 4.
3.4 Biomechanical Data Associated with Concussion
Meta-analysis of the mean peak linear acceleration in concussed patients across 12 studies (3074 participants) reported a pooled mean of 98.68 g (95 % CI 82.36–115.00). There was no evidence of statistical heterogeneity (I 2 statistic = 0.0 %; p = 0.944) (see Fig. 2).

Pooled mean peak linear acceleration in the setting of concussion. Weights are from random effects analysis. CI confidence interval
Meta-analysis of the mean peak rotational acceleration in concussed patients across nine studies (3203 participants) reported a pooled mean of 5776.60 rads/s2 (95 % CI 4583.53–6969.67). There was no evidence of statistical heterogeneity (I 2 statistic = 0.0 %; p = 0.824) (see Fig. 3).

Pooled mean peak rotational acceleration in the setting of concussion. Weights are from random effects analysis. CI confidence interval
4 Discussion
This is the first systematic review including meta-analyses to quantify the biomechanical head impact responses associated with a diagnosis of concussion from practice and game impacts sustained across multiple sports. Our findings are consistent with those of Pellman et al. [46] and McIntosh et al. [47], who both used impact reconstruction methods to study concussion. Applications of these findings include performance requirements for helmets and protocols for the medical assessment of a real-time monitored athlete, for example triggering the removal from play for clinical assessment of an athlete who is exposed to an impact greater than the reported pooled peak head accelerations.
While this review reports on quantitative values reported among concussed cases, it is important to consider that these findings are limited in not defining a concussion threshold and may be conservative estimates in not being representative of all impacts [5, 29, 48]. An important observation is that many head impacts recorded above the mean values reported do not result in concussion [35, 40]. Data on the incidence of non-concussive impacts with kinematic responses equal to or greater than the magnitude associated with concussion in each included study were unable to be extracted; however, based on previous findings [29, 48], it is estimated that the majority of impacts at magnitudes associated with a diagnosis of concussion do not result in a concussion. Greenwald et al. collated 3476 impacts >98.9 g, of which only 11 (0.3 %) resulted in a concussion [48]. In their respective studies, Guskiewicz et al. and Broglio et al. both note that symptomatology of concussive episodes did not correlate with biomechanical data [33, 36]. In addition, widely varying magnitudes of acceleration at which concussion is sustained were observed [33, 36]. Schnebel et al. and Rowson et al. reported that little is known about the individual risk factors that contribute to the incidence and severity of concussive episodes, further illustrating the difficulties in defining an injury threshold [34, 40]. In finite element simulations of concussive impacts, Patton et al. [49] observed that the brain regions were sensitive to head impact location and component accelerations and velocities, suggesting that peak resultant values exclusively may be limited [50]. Furthermore, variable individual tolerance to head impact and the difficulty in determining the true effect of multiple head impacts over time periods pose additional limitations to defining an injury threshold.
Improvement in the clinical utility of head acceleration data may be achieved through consideration of impact location. Using a linear acceleration threshold of 96.1 g, Broglio et al. used a classification and regression tree (CART) model to accurately predict 10 identified concussions out of 47 impacts exceeding the injury tolerance level (21.3 % sensitivity) [35].
Previous reviews examining head impact biomechanics in solely American Football have found similar forces associated with a diagnosis of concussion. Forbes et al. reported that high-school players who were concussed experienced an average linear acceleration of 93.9 g and an average rotational acceleration of 6505.2 rads/s2, whereas college athletes experienced an average of 118.4 g of linear acceleration and 5311.6 rad/s2 of rotational acceleration [18]. The limitations of biomechanical data were also highlighted by the authors, as less than 1 % of impacts that surpassed the mean accelerations associated with concussion actually resulted in concussion [18]. In their review of concussion biomechanics, Broglio et al. noted that variation in athlete size, and strength, along with equipment, impact direction, impact readiness and several other variables, may influence injury risk [19]. While the authors reported that a concussion threshold is yet to be identified, they noted that emerging from research into concussion biomechanics is the consistent importance of linear acceleration, rotational acceleration and impact location as predictive of concussive impacts [19].
A number of concussion clinical evaluation tools have been developed (SCAT3, Standardized Assessment of Concussion, etc.) to improve recognition of concussion symptomatology and diagnosis. Although useful, they should not take the place of clinician judgement and are limited in identifying individuals who require screening for concussion and in those individuals with delayed-onset concussion [4, 6]. In addition, high error rates for the concentration portion of assessment have been demonstrated, highlighting the importance of baseline testing [51, 52]. Biomechanical data used in conjunction with clinical markers (e.g. balance or motor incoordination, disorientation, confusion or vomiting), video analysis and sideline assessment may provide more reliable measures of concussion and/or justification for removal of a player from competition and initiation of a structured monitoring programme of clinical assessments, when clinical observations are indeterminate.
Differences in head impact exposure may result in different clinical presentations. An immediate diagnosis of concussion is more closely associated with single high-magnitude impacts, whereas delayed diagnosis of concussion is associated with moderate impacts at an increased frequency [38, 42]. However, when evaluating the influence of subconcussive head impacts on the concussion threshold, Eckner et al. found no evidence to support the cumulative impact theory that a series of subconcussive impacts could lower an athlete’s concussion threshold [53]. The effect of cumulative head impacts on a concussion threshold remains unknown.
Female and youth athletes were excluded from analysis in this review as these populations sustain concussions at lower magnitudes, on average [21, 31, 54]. In a study of the biomechanics of concussive head impacts in female collegiate ice hockey players, Wilcox et al. reported the average linear and rotational acceleration of concussive impacts to be 43.0 ± 11.5 g and 4030 ± 1435 rads/s2, respectively [21]. Furthermore, biomechanical data available for head impacts in female athletes are limited. There are a reasonable amount of data available examining head impact biomechanics in youth athletes [31, 55–65]. Despite this, few studies report concussive events in their study periods, leaving the population small [31, 55, 57, 63]. Furthermore, the large age-group variation between studies makes analysis troublesome. Therefore, the findings of this review are only applicable to a male population.
Unfortunately, not all studies reporting biomechanical forces associated with concussive events provided linear and rotational acceleration data, and such studies were therefore unable to be included in the analysis. Despite careful inspection of methodology and exclusion of multiple studies due to multiple collated datasets [37, 38, 40], we were unable to completely ascertain whether there was an overlap of data between the included studies.
5 Conclusions
Head impact monitoring through accelerometery has been shown to be useful with regard to characterising the kinematic load to the head associated with concussion.
It is not definitive in diagnosing or assisting with a diagnosis of concussion. This is due to a number of factors, including the lack of an identified concussion injury threshold and the extensive range of magnitudes at which players sustain concussion, as evidenced by wide confidence intervals and no evidence of heterogeneity between studies. Reported biomechanical forces may be used as alerts, in real-time monitoring or retrospectively, when screening athletes with potential concussion. Future research with improved clinical outcome measures and head kinematic data may improve accuracy when evaluating concussion, and may assist with both interpretation of biomechanical data and the development and utilisation of implementation strategies for the technology. Additionally, further investigation into biomechanical forces associated with concussion in non-helmeted and female athletes is recommended in order to develop an understanding of concussion within these populations of athletes.
References
Langlois JA, Rutland-Brown W, Wald MM. The epidemiology and impact of traumatic brain injury: a brief overview. J Head Trauma Rehabil. 2006;21(5):375–8.
O’Rance L. Disability in Australia: acquired brain injury. Canberra: Australian Institute of Health and Welfare; 2007.
Theadom A, Starkey NJ, Dowell T, et al. Sports-related brain injury in the general population: an epidemiological study. J Sci Med Sport. 2014;17(6):591–6.
McCrory P, Meeuwisse WH, Aubry M, et al. Consensus statement on concussion in sport: the 4th international conference on concussion in sport held in Zurich, November 2012. Br J Sports Med. 2013;47(5):250–8.
Rowson S, Duma SM. Brain injury prediction: assessing the combined probability of concussion using linear and rotational head acceleration. Ann Biomed Eng. 2013;41(5):873–82.
Duhaime AC, Beckwith JG, Maerlender AC, et al. Spectrum of acute clinical characteristics of diagnosed concussions in college athletes wearing instrumented helmets: clinical article. J Neurosurg. 2012;117(6):1092–9.
Williamson IJS, Goodman D. Converging evidence for the under-reporting of concussions in youth ice hockey. Br J Sports Med. 2006;40(2):128–32.
McCrea M, Hammeke T, Olsen G, et al. Unreported concussion in high school football players: implications for prevention. Clin J Sport Med. 2004;14(1):13–7.
Beckwith JG, Greenwald RM, Chu JJ. Measuring head kinematics in football: correlation between the head impact telemetry system and Hybrid III headform. Ann Biomed Eng. 2012;40(1):237–48.
Chu JJ, Beckwith JG, Crisco JJ, et al. A novel algorithm to measure linear and rotational head acceleration using single-axis accelerometers. J Biomech. 2006;39:S534.
Crisco JJ, Chu JJ, Greenwald RM. An algorithm for estimating acceleration magnitude and impact location using multiple nonorthogonal single-axis accelerometers. J Biomech Eng. 2004;126(6):849–54.
Funk JR, Rowson S, Daniel RW, et al. Validation of concussion risk curves for collegiate football players derived from HITS data. Ann Biomed Eng. 2012;40(1):79–89.
King D, Hume PA, Brughelli M, et al. Instrumented mouthguard acceleration analyses for head impacts in amateur rugby union players over a season of matches. Am J Sports Med. 2015;43(3):614–24.
McKee AC, Cantu RC, Nowinski CJ, et al. Chronic traumatic encephalopathy in athletes: progressive tauopathy after repetitive head injury. J Neuropathol Exp Neurol. 2009;68(7):709–35.
Gardner A, Iverson GL, McCrory P. Chronic traumatic encephalopathy in sport: a systematic review. Br J Sports Med. 2014;48(2):84–90.
Davis GA, Castellani RJ, McCrory P. Neurodegeneration and sport. Neurosurgery. 2015;76(6):643–55 (discussion 655–6).
Maroon JC, Winkelman R, Bost J, et al. Chronic traumatic encephalopathy in contact sports: a systematic review of all reported pathological cases. PLoS One. 2015;10(2):e0117338.
Forbes JA, Awad AJ, Zuckerman S, et al. Association between biomechanical parameters and concussion in helmeted collisions in American football: a review of the literature. Neurosurg Focus. 2012;33(6):E10.
Broglio SP, Surma T, Ashton-Miller JA. High school and collegiate football athlete concussions: a biomechanical review. Ann Biomed Eng. 2012;40(1):37–46.
King D, Brughelli M, Hume P, et al. Assessment, management and knowledge of sport-related concussion: systematic review. Sports Med. 2014;44(4):449–71.
Wilcox BJ, Beckwith JG, Greenwald RM, et al. Biomechanics of head impacts associated with diagnosed concussion in female collegiate ice hockey players. J Biomech. 2015;48(10):2201–4.
Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1.
Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–9.
Whiting PF, Rutjes AW, Westwood ME, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155(8):529–36.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177–88.
Rowson S, Duma SM. Development of the STAR evaluation system for football helmets: integrating player head impact exposure and risk of concussion. Ann Biomed Eng. 2011;39(8):2130–40.
Duma SM, Manoogian SJ, Bussone WR, et al. Analysis of real-time head accelerations in collegiate football players. Clin J Sport Med. 2005;15(1):3–8.
Funk JR, Duma SM, Manoogian S. Development of concussion risk curves based on head impact data from collegiate football players. Injury Biomechanics Research. In: Proceedings of the 34th international workshop. Dearborn, MI; 2006. pp. 1–15.
Funk JR, Duma SM, Manoogian SJ, et al. Biomechanical risk estimates for mild traumatic brain injury. Annu Proc Assoc Adv Automot Med. 2007;51:343–61.
Duma SM, Rowson S (eds). Every newton hertz: a macro to micro approach to investigating brain injury. In: Conf Proc IEEE Eng Med Biol Soc; 2009, pp. 1123–6.
Munce TA, Dorman JC, Thompson PA, et al. Head impact exposure and neurologic function of youth football players. Med Sci Sports Exerc. 2015;47(8):1567–76.
McAllister TW, Ford JC, Ji S, et al. Maximum principal strain and strain rate associated with concussion diagnosis correlates with changes in corpus callosum white matter indices. Ann Biomed Eng. 2012;40(1):127–40.
Guskiewicz KM, Mihalik JP, Shankar V, et al. Measurement of head impacts in collegiate football players: relationship between head impact biomechanics and acute clinical outcome after concussion. Neurosurgery. 2007;61(6):1244–52 (discussion 1252–3).
Schnebel B, Gwin JT, Anderson S, et al. In vivo study of head impacts in football: a comparison of National Collegiate Athletic Association Division I versus high school impacts. Neurosurgery. 2007;60(3):490–5 (discussion 495–6).
Broglio SP, Schnebel B, Sosnoff JJ, et al. Biomechanical properties of concussions in high school football. Med Sci Sports Exerc. 2010;42(11):2064–71.
Broglio SP, Eckner JT, Surma T, et al. Post-concussion cognitive declines and symptomatology are not related to concussion biomechanics in high school football players. J Neurotrauma. 2011;28(10):2061–8.
Beckwith JG, Chu JJ, Crisco JJ, et al. Severity of head impacts resulting in mild traumatic brain injury. Am Soc Biomech. 2009;1144.
Beckwith JG, Greenwald RM, Chu JJ, et al. Timing of concussion diagnosis is related to head impact exposure prior to injury. Med Sci Sports Exerc. 2013;45(4):747–54.
Brolinson PG, Manoogian S, McNeely D, et al. Analysis of linear head accelerations from collegiate football impacts. Curr Sports Med Rep. 2006;5(1):23–8.
Rowson S, Duma SM, Beckwith JG, et al. Rotational head kinematics in football impacts: an injury risk function for concussion. Ann Biomed Eng. 2012;40(1):1–13.
Guskiewicz KM, Register-Mihalik J, McCrory P, et al. Evidence-based approach to revising the SCAT2: introducing the SCAT3. Br J Sports Med. 2013;47(5):289–93.
Beckwith JG, Greenwald RM, Chu JJ, et al. Head impact exposure sustained by football players on days of diagnosed concussion. Med Sci Sports Exerc. 2013;45(4):737–46.
Manoogian S, McNeely D, Duma S, et al. Head acceleration is less than 10 percent of helmet acceleration in football impacts. Biomed Sci Instrum. 2006;42:383–8.
Higgins M, Halstead PD, Snyder-Mackler L, et al. Measurement of impact acceleration: mouthpiece accelerometer versus helmet accelerometer. J Athl Train. 2007;42(1):5–10.
Beckwith JG, Chu JJ, Greenwald RM. Validation of a noninvasive system for measuring head acceleration for use during boxing competition. J Appl Biomech. 2007;23(3):238–44.
Pellman EJ, Viano DC, Tucker AM, et al. Concussion in professional football: reconstruction of game impacts and injuries. Neurosurgery. 2003;53(4):799–812 (discussion 1340–1).
McIntosh AS, Patton DA, Fréchède B, et al. The biomechanics of concussion in unhelmeted football players in Australia: a case–control study. BMJ Open. 2014;4(5):e005078.
Greenwald RM, Gwin JT, Chu JJ, et al. Head impact severity measures for evaluating mild traumatic brain injury risk exposure. Neurosurgery. 2008;62(4):789–98.
Patton DA, McIntosh AS, Kleiven S. The biomechanical determinants of concussion: finite element simulations to investigate brain tissue deformations during sporting impacts to the unprotected head. J Appl Biomech. 2013;29(6):721–30.
Patton DA, McIntosh AS, Kleiven S. The biomechanical determinants of concussion: finite element simulations to investigate tissue-level predictors of injury during sporting impacts to the unprotected head. J Appl Biomech. 2015;31(4):264–8.
Jinguji TM, Bompadre V, Harmon KG, et al. Sport Concussion Assessment Tool—2: baseline values for high school athletes. Br J Sports Med. 2012;46(5):365–70.
Valovich McLeod TC, Bay RC, Lam KC, et al. Representative baseline values on the Sport Concussion Assessment Tool 2 (SCAT2) in adolescent athletes vary by gender, grade, and concussion history. Am J Sports Med. 2012;40(4):927–33.
Eckner JT, Sabin M, Kutcher JS, et al. No evidence for a cumulative impact effect on concussion injury threshold. J Neurotrauma. 2011;28(10):2079–90.
Wilcox BJ, Machan JT, Beckwith JG, et al. Head-impact mechanisms in men’s and women’s collegiate ice hockey. J Athl Train. 2014;49(4):514–20.
Cobb BR, Urban JE, Davenport EM, et al. Head impact exposure in youth football: elementary school ages 9-12 years and the effect of practice structure. Ann Biomed Eng. 2013;41(12):2463–73.
Daniel RW, Rowson S, Duma SM. Head impact exposure in youth football. Ann Biomed Eng. 2012;40(4):976–81.
Daniel RW, Rowson S, Duma SM. Head impact exposure in youth football: middle school ages 12-14 years. J Biomech Eng. 2014;136(9):094501.
McPherson MN, Montelpare WJ, Keightley M, et al. An analysis of head impact profiles and safe hockey behaviors in youth hockey players. J ASTM Int. 2009;6(10):1–7.
Mihalik JP, Blackburn JT, Greenwald RM, et al. Collision type and player anticipation affect head impact severity among youth ice hockey players. Pediatrics. 2010;125(6):e1394–401.
Mihalik JP, Greenwald RM, Blackburn JT, et al. Effect of infraction type on head impact severity in youth ice hockey. Med Sci Sports Exerc. 2010;42(8):1431–8.
Mihalik JP, Guskiewicz KM, Marshall SW, et al. Head impact biomechanics in youth hockey: comparisons across playing position, event types, and impact locations. Ann Biomed Eng. 2012;40(1):141–9.
Reed N, Taha T, Keightley M, et al. Measurement of head impacts in youth ice hockey players. Int J Sports Med. 2010;31(11):826–33.
Urban JE, Davenport EM, Golman AJ, et al. Head impact exposure in youth football: high school ages 14 to 18 years and cumulative impact analysis. Ann Biomed Eng. 2013;41(12):2474–87.
Young TJ, Daniel RW, Rowson S, et al. Head impact exposure in youth football: elementary school ages 7-8 years and the effect of returning players. Clin J Sport Med. 2014;24(5):416–21.
Young TJ, Rowson S, Duma SM, et al. High magnitude head impacts experienced during youth football practices. In: 51st annual rocky mountain bioengineering symposium, RMBS 2014, and 51st international ISA biomedical sciences instrumentation symposium 2014; 2014.
Acknowledgments
The authorship team would like to acknowledge Ms. Lisa Kruesi and Ms. Penny Presta for their assistance in the development of the search strategy.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
James Brennan received a scholarship from Monash University to undertake this systematic review. Joanne McKenzie holds a National Health and Medical Research Council (NHMRC) Australian Public Health Fellowship (1072366).
Conflict of interest
James H. Brennan, Biswadev Mitra, Anneliese Synnot, Joanne McKenzie, Catherine Willmott, Andrew S. McIntosh, Jerome J. Maller and Jeffrey V. Rosenfeld declare that they have no conflicts of interest relevant to the content of this review.
Rights and permissions
About this article

Cite this article
Brennan, J.H., Mitra, B., Synnot, A. et al. Accelerometers for the Assessment of Concussion in Male Athletes: A Systematic Review and Meta-Analysis. Sports Med 47, 469–478 (2017). https://doi.org/10.1007/s40279-016-0582-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-016-0582-1