
Abstract
Background
Core needle biopsies of sarcomas allow a diagnosis in a high percentage of patients with few complications. However, it is unclear whether the tract needs to be excised to prevent recurrences.
Questions/purposes
We therefore determined the rates of recurrence and metastases in patients with Stage III extremity sarcomas, who underwent wide local resection without excision of the needle tract and also received adjuvant treatment.
Methods
We retrospectively reviewed 59 adult patients with deep, larger than 5 cm, high-grade soft tissue sarcomas of the upper or lower extremity treated between January 1999 and April 2009. All the patients underwent a core needle biopsy. Resection was performed with wide margins. The biopsy tract was not resected during the definitive surgery. Fifty-seven patients (97%) received preoperative and/or postoperative radiation, whereas 49 patients (83%) received chemotherapy. Local recurrence and distant recurrence rates were determined. The minimum followup was 24 months (median, 56 months; range, 24–122 months).
Results
The local recurrence rate was 9%. Fifteen patients (25%) developed metastasis after diagnosis. Seven of the 59 patients (12%) had microscopic positive margins at resection.
Conclusions
Our data demonstrate no increase in local recurrence rates or rates of metastatic disease compared with previously published studies when resection of the core biopsy tract was not performed.
Level of Evidence
Level IV, therapeutic study. See the Guidelines for Authors for a complete description of levels of evidence.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The staging of musculoskeletal sarcomas includes the evaluation of a tissue biopsy in addition to radiologic imaging of the tumor and imaging for the presence of metastasis [35, 38]. Open biopsy had been the mainstay for obtaining tissue samples; however, the safety and efficacy of percutaneous biopsies have been demonstrated in numerous studies [1, 5, 7, 10, 17, 24, 32, 39–41, 48, 59, 61, 63–65].
Needle tract seeding from percutaneous biopsies has been demonstrated in hepatocellular, breast, thyroid, non-Hodgkin’s lymphoma, vertebral metastasis, and renal and brain tumors among others [11, 21, 26, 29, 31, 46, 54]. However, a study of rates of local recurrence in breast cancer demonstrated no increase among patients who underwent a core needle biopsy [20]. In sarcomas, it has been known that open biopsy incisions and tracts should be resected. A case report documented needle tract seeding in a patient with a distal femoral osteosarcoma [15]; we, however, could not find any reports of needle tract seeding after a closed biopsy in soft tissue sarcomas.
Historically reported rates of local recurrence of soft tissue sarcomas range from 13% to 29% and metastases from 22% to 49% [4, 22, 25, 36, 37, 43, 51, 55, 56, 58, 65]. The addition of radiation to the wide resection of sarcomas improves local recurrence rates from 19% to 30% in certain studies, even in patients with microscopically positive margins [3, 12, 16, 27, 30, 52, 53, 60, 62]. Because patients with Stage III tumors receive adjuvant therapies, in addition to wide resection, to treat microscopically positive margins and/or satellite lesions, it is believed this would also treat any potential tumor cells in the core needle tract. The effect of chemotherapy on outcomes of sarcoma treatment is still debatable; however, a few systematic reviews and meta-analyses have demonstrated improvement in local control rates and, in some cases, overall survival with the use of chemotherapy and radiation [2, 19, 42, 45]. A recent report had no local recurrences from a fine needle aspiration biopsy in 20 patients with high-grade soft tissue sarcomas [28]. The needle tract was excised in two patients who had an amputation. Eighty percent of their patients received adjuvant therapy. However, it is unclear whether the risk of local recurrence or metastases is increased when the core needle biopsy tract is not excised in patients receiving adjuvant therapy.
Our primary focus was to determine whether leaving the core needle biopsy tract unresected in adult patients with Stage III extremity sarcomas who underwent wide resection and received adjuvant treatment would lead to an increase in the local recurrence rate. Our secondary goal was to determine if this affected rates of metastasis.
Patients and Methods
Between January 1999 and April 2009, 288 adult patients (18 years of age and older) underwent core needle biopsies of primary soft tissue sarcomas at two tertiary cancer centers. Tumors were considered primary if the patient had no intervention (including biopsy) before their presentation to either cancer center. We excluded 174 patients with tumors located in the trunk, shoulder, and pelvis; patients with recurrent disease; or those who underwent an amputation as the definitive treatment. This left 114 patients with high-grade tumors, which measured greater than 5 cm in the largest dimension at surgical resection and were located deep to the superficial fascia (American Joint Commission on Cancer Type III [49]). Eighteen patients were lost to followup and 37 did not have up to 24 months of followup or died before that. Most local recurrences occur within 2 to 3 years after resection [18, 36, 51, 56]. Thus, we included 59 patients in the study. Mean age was 56.8 ± 17.1 years. There were 28 male and 31 female patients. Minimum followup was 24 months (median, 56 months; range, 24–122 months). We obtained institutional review board approval and the medical records of these patients were reviewed.
All patients underwent a preoperative workup, which included a history and physical, radiographic imaging of the extremity (radiographs and MRI), CT scans of the lungs to evaluate for metastatic disease, and for patients with leiomyosarcomas, an abdominal and pelvis CT scan was also performed. All patients were reviewed at a multidisciplinary tumor conference where treatment plans were discussed. Tumors were described based on their location. Demographic data including age at presentation, history, sex, and race were also reviewed. Mean measurement of the largest tumor dimension was 12 cm (SD ± 6.4). The most common sarcoma subtype determined by final histopathologic diagnosis was high-grade undifferentiated pleomorphic sarcoma (Table 1).
Core needle biopsy was performed on all the patients in this study. Biopsies were performed in the clinic under local anesthesia; in the imaging suite, guided by either ultrasound or CT; or in the operating room using a Tru-cut, Temno, or Jamshidi needle (Cardinal Health, McGaw Park, IL, USA; Care Fusion, San Diego, CA, USA). In no case was an incisional biopsy performed. Five patients underwent two biopsies in the clinic as a result of insufficient tissue from the first attempt. One patient had an ultrasound-guided biopsy after an unsuccessful clinic biopsy. Clinic biopsies were performed after informed consent was obtained and the area was prepped and draped in a standard sterile fashion. One percent lidocaine was infiltrated into the area with a 25-gauge needle for local anesthesia. A subcentimeter skin incision, using a Number 11 blade, was made and a 14-gauge core needle was advanced into the mass. Several passes were made and tissue cores were taken directly to the pathology laboratory for histologic analysis. A bandage was placed over the incision. A similar process was performed in the imaging suite by fellowship-trained musculoskeletal radiologists under the guidance of the treating orthopaedic surgeon for the image-guided biopsies after a discussion between both specialists regarding the path for biopsy-sparing neurovascular and other vital structures. Patients who could not tolerate a clinic biopsy were taken to the operating room and under monitored anesthesia care, a small incision after local anesthesia was made over the mass. Through this, a 14-gauge needle was passed into the mass. Samples were taken to the pathology laboratory and the patient awakened from anesthesia. There were no complications from the core needle biopsy procedures. There was a variation between the two institutions where the biopsies were performed. One institution performed all biopsies in the clinic, whereas the other performed 70% in the clinic.
All biopsy material was reviewed by pathologists and the material underwent frozen microscopic analysis. Biopsy samples were deemed diagnostic if there was adequate tissue to make a diagnosis.
All patients were discussed in a multidisciplinary tumor conference at each institution and treatment plans were determined. A total of 57 patients (97%) received radiation therapy (Table 2). Four patients received postoperative interstitial brachytherapy. Interstitial catheters were placed at the time of surgery in single-plane geometry to cover the entire tumor bed. Catheters were loaded with Iridium-192 sources approximately 5 to 6 days after surgery. The median dose was 3500 cGy. Four patients were enrolled in a radiation and dendritic stem cell vaccine trial and received dendritic stem cells in addition to external beam radiation therapy.
Forty-nine patients (83%) received chemotherapy (Table 2). The majority received a doxorubicin and ifosfamide-based chemotherapy regimen. Doses were 75 mg/m2 Adriamycin, 10 g/m2 ifosfamide, and 50 mg/m2 cisplatin per cycle.
All patients underwent wide local resections performed by fellowship-trained orthopaedic and surgical oncologists at the two institutions. Patients who underwent amputations were excluded from this study. Tumor size was determined at the time of resection by the pathologist as the greatest diameter of the gross specimen. Protocols at both institutions were similar in the handling of resected specimens. Tumors were oriented and sent fresh to the pathology department. In the pathology laboratory, tumors were handled according to the College of American Pathologists protocol for soft tissue tumors [47]. The specimen was marked with ink and one section per centimeter of maximum dimension was obtained. These were mostly taken from grossly heterogeneous areas. At the margins, sections were oriented perpendicular to the ink margin. Areas with macroscopic tumor close to the margin were sent for microscopic analysis. During retrospective review, margins that were free from tumor by > 5 mm were defined as R0, R1 margins were equal to or less than 5 mm to the inked surface, whereas R2 margins were macroscopically positive for tumor [43]. There were 52 R0 resection margins, seven R1 margins, and no R2 margins. Of those with R1 margins, two underwent a reresection to R0 margins (Table 2).
Patient followup entailed physical examination and imaging studies on a routine timetable. Patients were seen every 3 months for the first 2 years for a history and physical examination, radiographs and MRI of the limb, chest CT scans, and abdomen and pelvis CT scans in patients with leiomyosarcomas. After 2 years patients were seen every 6 months and after 5 years seen annually. After 5 years either a chest radiograph or a CT scan was obtained. The followup period was measured from the date of biopsy to last followup or death, whereas time to local recurrence was from the date of biopsy to the date the first local recurrence was diagnosed. Survival data were obtained from the medical records, patient contact, and the Social Security Death Index (http://ssdi.rootsweb.ancestry.com/cgi-bin/ssdi.cgi).
Descriptive statistics were used for overall patient characteristics. Fisher’s exact test was used to compare local recurrence and metastatic rates between R1 and R0 margin groups. Statistical analysis was performed using IBM SPSS statistics (Version 19.0; SPSS, Chicago, IL, USA).
Results
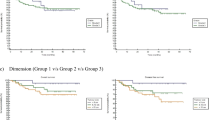
There were five local recurrences (9%). Median time to local recurrence was 13 months (range, 6-22 months). All five patients with a local recurrence underwent a repeat resection (Table 3). Fifteen patients developed distant disease (25%). Median time to development of distant disease was 22 months (range, 9–37 months). Seventy-five percent of these patients had metastasis to the lungs.
Two patients with a microscopically positive resection margin (R1) had a local recurrence (Table 4). An R1 margin did not increase the rate of a local recurrence (p = 0.1) or metastasis (p = 0.99). The results of this study were compared with previously published rates of local recurrence and metastasis (Table 5).
Discussion
There is a concern of needle tract seeding from percutaneous biopsies. Although demonstrated in various other types of cancer, there are no reports of needle tract seeding in closed biopsy of soft tissue sarcoma. The purpose of this study was to determine whether core needle biopsy tracts that were not intentionally resected during wide local resections of large (> 5 cm), deep, high-grade extremity sarcomas in adult patients who also received adjuvant treatment (chemotherapy and/or radiation) had an untoward effect on local recurrence or metastatic rates.
The limitations of our study include a relatively small number of patients. Sarcomas are rare tumors with an estimated 10,520 new cases in the United States in 2010 [6]. The rationale behind selecting patients with high-grade, deep and large tumors was that these have been consistently reported to be factors that increase the risk of local recurrence and/or of metastasis [4, 8, 9, 13, 14, 18, 22–24, 33, 34, 36, 37, 43, 44, 50, 51, 55–57] and these tumors are typically treated with adjuvant treatment, making them a more homogenous group for our research purposes. The inclusion criterion was limited to primary tumors, eliminating those patients with prior treatments or biopsy at outside institutions. Although that limited the number of study patients, we believe this enhanced the study by decreasing confounding variables. Second, we lacked concurrent controls and used historic data for comparison. A cohort of patients who had the needle biopsy tract resected for comparison would have strengthened the study. Third, five patients were lost to followup, two of whom developed metastasis at a median of 3 months after diagnosis. Although none of these patients had a local recurrence at last followup, the total number of local recurrences and metastases may be altered by improved followup. Finally, this was a retrospective study of a specific group of patients with high-grade tumors treated with a multimodality treatment approach (with radiation and/or chemotherapy); the study results may not be applicable to patients who do not receive adjuvant treatment.
Our primary aim was to determine if an unresected core needle tract would lead to higher local recurrence rates than that reported in the literature. There were five local recurrences (9%) among our patients, which was lower than numerous studies that evaluated local recurrences in patients with soft tissue sarcomas (13%-39%) [4, 22, 25, 36, 37, 43, 51, 55, 56, 58, 65]. Some of these studies included all tumor grades, superficial and deep tumors as well as trunk wall and retroperitoneal tumors. The median time to local recurrence in this study of 13 months was in line with the majority of the literature that reports local recurrences occurring in the first 2 to 3 years [18, 36, 51, 56]. A positive microscopic surgical resection margin status did not have an adverse effect on local recurrence rates; however, as a result of the small number of local recurrences, a definitive conclusion could not be drawn from this. Five patients had more than one attempt at a core needle biopsy with the first demonstrating nondiagnostic tissue, and one of these patients had a local recurrence. We found no increase in the incidence of a local recurrence from more than one attempt at a biopsy. An important note is that all biopsies were performed either by the orthopaedic oncologist or by a musculoskeletal radiologist after discussion with the treating surgeon. The careful planning of a biopsy path is critical to not contaminate vital structures.
We found metastases in 15 patients (25%). This was equal to or lower compared with previous studies (22%–49%) [4, 22, 25, 36, 37, 43, 51, 55, 56, 58, 65]. Margin status did not have a statistically negative effect on the rate of metastases; however, given the small number of R1 margins, a conclusion cannot be drawn from this either.
This was a retrospective study evaluating the effect of retained core needle biopsy tract in patients with high-grade sarcomas receiving adjuvant treatment. The site of a needle biopsy is very small and unless it is specifically marked afterward, identifying its location becomes a difficult task. Because it is the practice to treat Stage III tumors with adjuvant therapies at these two institutions, it was believed that any microscopic cells in the tract would be treated with these therapies as would any microscopic positive margins or satellite lesions.
The goals of this study were to determine whether there was an increased rate of local recurrence and metastases in a patient population with unresected core needle biopsy tracts and large (> 5 cm), deep, high-grade extremity sarcomas that underwent wide local resection and adjuvant therapies. Compared with the current sarcoma literature, the local recurrence and metastatic rates in this patient population were similar or lower. These results indicate that retained core needle biopsy tract does not increase the risk of local recurrence or metastatic rates in this specific patient population. However, these results should not be extrapolated to all soft tissue sarcomas or to sarcomas treated without adjuvant therapy. A multidisciplinary management approach, like in the treatment of all sarcomas, is essential.
References
Adams SC, Potter BK, Pitcher DJ, Temple HT. Office-based core needle biopsy of bone and soft tissue malignancies: an accurate alternative to open biopsy with infrequent complications. Clin Orthop Relat Res. 2010;468:274–2780.
Adjuvant chemotherapy for localised resectable soft tissue sarcoma in adults. Cochrane Database Syst Rev. 2000;4:CD001419.
Alektiar KM, Velasco J, Zelefsky MJ, Woodruff JM, Lewis JJ, Brennan MF. Adjuvant radiotherapy for margin-positive high-grade soft tissue sarcoma of the extremity. Int J Radiat Oncol Biol Phys. 2000;48:1051–1058.
Alkis N, Muallaoglu S, Kocer M, Arslan UY, Durnali AG, Tokluoglu S, Celenkoglu G, Paksoy F, Coskun U. Primary adult soft tissue sarcomas: analysis of 294 patients. Med Oncol. 2011;28:391–39.
Altuntas AO, Slavin J, Smith PJ, Schlict SM, Powell GJ, Ngan S, Toner G, Choong PF. Accuracy of computed tomography guided core needle biopsy of musculoskeletal tumours. A N Z J Surg. 2005;75:187–191.
American Cancer Society. Cancer Facts and Figures 2010. Atlanta, GA, USA: American Cancer Society; 2010.
Ball AB, Fisher C, Pittam M, Watkins RM, Westbury G. Diagnosis of soft tissue tumours by Tru-Cut biopsy. Br J Surg. 1990;77:756–758.
Bell RS, O’Sullivan B, Liu FF, Powell J, Langer F, Fornasier VL, Cummings B, Miceli PN, Hawkins N, Quirt I, et al. The surgical margin in soft-tissue sarcoma. J Bone Joint Surg Am. 1989;71:370–375.
Canter RJ, Beal S, Borys D, Martinez SR, Bold RJ, Robbins AS. Interaction of histologic subtype and histologic grade in predicting survival for soft-tissue sarcomas. J Am Coll Surg. 2010;210:191–198.
Carrino JA, Khurana B, Ready JE, Silverman SG, Winalski CS. Magnetic resonance imaging-guided percutaneous biopsy of musculoskeletal lesions. J Bone Joint Surg Am. 2007;89:2179–2187.
Chen YJ, Chang GC, Chen WH, Hsu HC, Lee TS. Local metastases along the tract of needle: a rare complication of vertebroplasty in treating spinal metastases. Spine (Phila Pa 1976). 2007;32:615–618.
Cheng EY, Dusenbery KE, Winters MR, Thompson RC. Soft tissue sarcomas: preoperative versus postoperative radiotherapy. J Surg Oncol. 1996;61:90–99.
Coindre JM, Terrier P, Bui NB, Bonichon F, Collin F, Le Doussal V, Mandard AM, Vilain MO, Jacquemier J, Duplay H, Sastre X, Barlier C, Henry-Amar M, Mace-Lesech J, Contesso G. Prognostic factors in adult patients with locally controlled soft tissue sarcoma. A study of 546 patients from the French Federation of Cancer Centers Sarcoma Group. J Clin Oncol. 1996;14:869–877.
Coindre JM, Trojani M, Contesso G, David M, Rouesse J, Bui NB, Bodaert A, De Mascarel I, De Mascarel A, Goussot JF. Reproducibility of a histopathologic grading system for adult soft tissue sarcoma. Cancer. 1986;58:306–309.
Davies NM, Livesley PJ, Cannon SR. Recurrence of an osteosarcoma in a needle biopsy track. J Bone Joint Surg Br. 1993;75:977–978.
Davis AM, O’Sullivan B, Turcotte R, Bell R, Catton C, Chabot P, Wunder J, Hammond A, Benk V, Kandel R, Goddard K, Freeman C, Sadura A, Zee B, Day A, Tu D, Pater J. Late radiation morbidity following randomization to preoperative versus postoperative radiotherapy in extremity soft tissue sarcoma. Radiother Oncol. 2005;75:48–53.
Dupuy DE, Rosenberg AE, Punyaratabandhu T, Tan MH, Mankin HJ. Accuracy of CT-guided needle biopsy of musculoskeletal neoplasms. AJR Am J Roentgenol. 1998;171:759–762.
Eilber FC, Rosen G, Nelson SD, Selch M, Dorey F, Eckardt J, Eilber FR. High-grade extremity soft tissue sarcomas: factors predictive of local recurrence and its effect on morbidity and mortality. Ann Surg. 2003;237:218–226.
Figueredo A, Bramwell VH, Bell R, Davis AM, Charette ML, the Members of the Cancer Care Ontario Practice Guidelines Initiative Sarcoma Disease Site Group. Adjuvant chemotherapy following complete resection of soft tissue sarcoma in adults: a clinical practice guideline. Sarcoma. 2002;6:5–18.
Fitzal F, Sporn EP, Draxler W, Mittlbock M, Taucher S, Rudas M, Riedl O, Helbich TH, Jakesz R, Gnant M. Preoperative core needle biopsy does not increase local recurrence rate in breast cancer patients. Breast Cancer Res Treat. 2006;97:9–15.
Fowler N, Asatiani E, Cheson B. Needle tract seeding after bone marrow biopsy in non-Hodgkin lymphoma. Leuk Lymphoma. 2008;49:156–158.
Gronchi A, Lo Vullo S, Colombo C, Collini P, Stacchiotti S, Mariani L, Fiore M, Casali PG. Extremity soft tissue sarcoma in a series of patients treated at a single institution: local control directly impacts survival. Ann Surg. 2010;251:506–511.
Herbert SH, Corn BW, Solin LJ, Lanciano RM, Schultz DJ, McKenna WG, Coia LR. Limb-preserving treatment for soft tissue sarcomas of the extremities. The significance of surgical margins. Cancer. 1993;72:1230–1238.
Heslin MJ, Lewis JJ, Woodruff JM, Brennan MF. Core needle biopsy for diagnosis of extremity soft tissue sarcoma. Ann Surg Oncol. 1997;4:425–431.
Heslin MJ, Woodruff J, Brennan MF. Prognostic significance of a positive microscopic margin in high-risk extremity soft tissue sarcoma: implications for management. J Clin Oncol. 1996;14:473–478.
Ito Y, Asahi S, Matsuzuka F, Nakamura Y, Amino N, Miyauchi A. Needle tract implantation of follicular neoplasm after fine-needle aspiration biopsy: report of a case. Thyroid. 2006;16:1059–1062.
Jebsen NL, Trovik CS, Bauer HC, Rydholm A, Monge OR, Hall KS, Alvegard T, Bruland OS. Radiotherapy to improve local control regardless of surgical margin and malignancy grade in extremity and trunk wall soft tissue sarcoma: a Scandinavian sarcoma group study. Int J Radiat Oncol Biol Phys. 2008;71:1196–1203.
Kaffenberger BH, Wakely PE Jr, Mayerson JL. Local recurrence rate of fine-needle aspiration biopsy in primary high-grade sarcomas. J Surg Oncol. 2010;101:618–621.
Karwowski JK, Nowels KW, McDougall IR, Weigel RJ. Needle track seeding of papillary thyroid carcinoma from fine needle aspiration biopsy. A case report. Acta Cytol. 2002;46:591–595.
Khanfir K, Alzieu L, Terrier P, Le Pechoux C, Bonvalot S, Vanel D, Le Cesne A. Does adjuvant radiation therapy increase loco-regional control after optimal resection of soft-tissue sarcoma of the extremities? Eur J Cancer. 2003;39:1872–1880.
Kim JE, Kim CY, Kim DG, Jung HW. Implantation metastasis along the stereotactic biopsy tract in anaplastic astrocytoma: a case report. J Neurooncol. 2003;61:215–218.
Kissin MW, Fisher C, Carter RL, Horton LW, Westbury G. Value of Tru-cut biopsy in the diagnosis of soft tissue tumours. Br J Surg. 1986;73:742–744.
Koea JB, Leung D, Lewis JJ, Brennan MF. Histopathologic type: an independent prognostic factor in primary soft tissue sarcoma of the extremity? Ann Surg Oncol. 2003;10:432–440.
Lewis JJ, Leung D, Heslin M, Woodruff JM, Brennan MF. Association of local recurrence with subsequent survival in extremity soft tissue sarcoma. J Clin Oncol. 1997;15:646–652.
Mankin HJ, Lange TA, Spanier SS. The Classic: the hazards of biopsy in patients with malignant primary bone and soft-tissue tumors. The Journal of Bone and Joint Surgery, 1982;64:1121–1127. Clin Orthop Relat Res. 2006;450:4–10.
Massi D, Beltrami G, Mela MM, Pertici M, Capanna R, Franchi A. Prognostic factors in soft tissue leiomyosarcoma of the extremities: a retrospective analysis of 42 cases. Eur J Surg Oncol. 2004;30:565–572.
McKee MD, Liu DF, Brooks JJ, Gibbs JF, Driscoll DL, Kraybill WG. The prognostic significance of margin width for extremity and trunk sarcoma. J Surg Oncol. 2004;85:68–76.
Mendenhall WM, Indelicato DJ, Scarborough MT, Zlotecki RA, Gibbs CP, Mendenhall NP, Mendenhall CM, Enneking WF. The management of adult soft tissue sarcomas. Am J Clin Oncol. 2009;32:436–442.
Mitsuyoshi G, Naito N, Kawai A, Kunisada T, Yoshida A, Yanai H, Dendo S, Yoshino T, Kanazawa S, Ozaki T. Accurate diagnosis of musculoskeletal lesions by core needle biopsy. J Surg Oncol. 2006;94:21–27.
Moore TM, Meyers MH, Patzakis MJ, Terry R, Harvey JP Jr. Closed biopsy of musculoskeletal lesions. J Bone Joint Surg Am. 1979;61:375–380.
Ogilvie CM, Torbert JT, Finstein JL, Fox EJ, Lackman RD. Clinical utility of percutaneous biopsies of musculoskeletal tumors. Clin Orthop Relat Res. 2006;450:95–100.
Pervaiz N, Colterjohn N, Farrokhyar F, Tozer R, Figueredo A, Ghert M. A systematic meta-analysis of randomized controlled trials of adjuvant chemotherapy for localized resectable soft-tissue sarcoma. Cancer. 2008;113:573–581.
Pisters PW, Leung DH, Woodruff J, Shi W, Brennan MF. Analysis of prognostic factors in 1,041 patients with localized soft tissue sarcomas of the extremities. J Clin Oncol. 1996;14:1679–1689.
Ramanathan RC, A’Hern R, Fisher C, Thomas JM. Prognostic index for extremity soft tissue sarcomas with isolated local recurrence. Ann Surg Oncol. 2001;8:278–289.
Rosenberg SA, Tepper J, Glatstein E, Costa J, Young R, Baker A, Brennan MF, Demoss EV, Seipp C, Sindelar WF, Sugarbaker P, Wesley R. Prospective randomized evaluation of adjuvant chemotherapy in adults with soft tissue sarcomas of the extremities. Cancer. 1983;52:424–434.
Rowe LR, Mulvihill SJ, Emerson L, Gopez EV. Subcutaneous tumor seeding following needle core biopsy of hepatocellular carcinoma. Diagn Cytopathol. 2007;35:717–721.
Rubin BP, Cooper K, Fletcher CDM, Folpe AL, Gannon FH, Leigh Hunt J, Lazar AJ, Montag AG, Peabody TD, Pollock RE, Qualman SJ, Reith JD, Rosenberg AE, Weiss SW, Krausz T; Members of the Cancer Committee, College of American Pathologists. Protocol for the examination of specimens from patients with tumors of the soft tissue. Arch Pathol Lab Med. 2010;134:e31–39.
Skrzynski MC, Biermann JS, Montag A, Simon MA. Diagnostic accuracy and charge-savings of outpatient core needle biopsy compared with open biopsy of musculoskeletal tumors. J Bone Joint Surg Am. 1996;78:644–649.
Soft tissue sarcoma. AJCC Cancer Staging Manual. 7th ed. New York, NY, USA: Springer; 2010:291–296.
Stojadinovic A, Leung DH, Allen P, Lewis JJ, Jaques DP, Brennan MF. Primary adult soft tissue sarcoma: time-dependent influence of prognostic variables. J Clin Oncol. 2002;20:4344–4352.
Stojadinovic A, Leung DH, Hoos A, Jaques DP, Lewis JJ, Brennan MF. Analysis of the prognostic significance of microscopic margins in 2084 localized primary adult soft tissue sarcomas. Ann Surg. 2002;235:424–434.
Strander H, Turesson I, Cavallin-Stahl E. A systematic overview of radiation therapy effects in soft tissue sarcomas. Acta Oncol. 2003;42:516–531.
Suit HD, Mankin HJ, Wood WC, Proppe KH. Preoperative, intraoperative, and postoperative radiation in the treatment of primary soft tissue sarcoma. Cancer. 1985;55:2659–2667.
Suzuki K, Takamochi K, Funai K, Kazui T. Needle tract implantation clearly visualized by computed tomography following needle biopsy of malignant mesothelioma. Eur J Cardiothorac Surg. 2006;29:1051.
Tanabe K, Pollock R, Ellis L, Murphy A, Sherman N, Romsdahl M. Influence of surgical margins on outcome in patients with preoperatively irradiated extermity soft tissue sarcomas. Cancer. 1994;73:1652–1659.
Trovik CS, Bauer HC, Berlin O, Tukiainen E, Erlanson M, Gustafson P, Klepp R, Saeter G, Wahlstrom O. Local recurrence of deep-seated, high-grade, soft tissue sarcoma: 459 patients from the Scandinavian Sarcoma Group Register. Acta Orthop Scand. 2001;72:160–166.
Trovik CS, Gustafson P, Bauer HC, Saeter G, Klepp R, Berlin O, Erlanson M, Wahlstrom O, Raabe N. Consequences of local recurrence of soft tissue sarcoma: 205 patients from the Scandinavian Sarcoma Group Register. Acta Orthop Scand. 2000;71:488–495.
Weitz J, Antonescu C, Brennan M. Localized extremity soft tissue sarcoma: improved knowledge with unchanged survival over time. J Clin Oncol. 2003;21:2719–2725.
Welker JA, Henshaw RM, Jelinek J, Shmookler BM, Malawer MM. The percutaneous needle biopsy is safe and recommended in the diagnosis of musculoskeletal masses. Cancer. 2000;89:2677–2686.
Wiklund TA, Alvegard TA, Mouridsen HT, Rydholm A, Blomqvist CP. Marginal surgery and postoperative radiotherapy in soft tissue sarcomas. The Scandinavian Sarcoma Group experience. Eur J Cancer. 1993;29:306–309.
Wu JS, Goldsmith JD, Horwich PJ, Shetty SK, Hochman MG. Bone and soft-tissue lesions: what factors affect diagnostic yield of image-guided core-needle biopsy? Radiology. 2008;248:962–970.
Yang JC, Chang AE, Baker AR, Sindelar WF, Danforth DN, Topalian SL, DeLaney T, Glatstein E, Steinberg SM, Merino MJ, Rosenberg SA. Randomized prospective study of the benefit of adjuvant radiation therapy in the treatment of soft tissue sarcomas of the extremity. J Clin Oncol. 1998;16:197–203.
Yang YJ, Damron TA. Comparison of needle core biopsy and fine-needle aspiration for diagnostic accuracy in musculoskeletal lesions. Arch Pathol Lab Med. 2004;128:759–764.
Yao L, Nelson SD, Seeger LL, Eckardt JJ, Eilber FR. Primary musculoskeletal neoplasms: effectiveness of core-needle biopsy. Radiology. 1999;212:682–686.
Zagars GK, Ballo MT, Pisters PW, Pollock RE, Patel SR, Benjamin RS, Evans HL. Prognostic factors for patients with localized soft-tissue sarcoma treated with conservation surgery and radiation therapy: an analysis of 1225 patients. Cancer. 2003;97:2530–2543.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he or she has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
This work was performed at H. Lee Moffitt Cancer Center & Research Institute, Tampa, FL, USA, and the Department of Orthopaedics and Rehabilitation, University of Miami Miller School of Medicine, Miami, FL, USA.
About this article
Cite this article
Binitie, O., Tejiram, S., Conway, S. et al. Adult Soft Tissue Sarcoma Local Recurrence After Adjuvant Treatment Without Resection of Core Needle Biopsy Tract. Clin Orthop Relat Res 471, 891–898 (2013). https://doi.org/10.1007/s11999-012-2569-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-012-2569-z