
Abstract
We retrospectively analyzed 294 patients with primary soft tissue sarcoma followed between 1996 and 2002 in Ankara Oncology Hospital. There were 170 male and 124 female patients with the age range of 16–80 years. The primary tumor was in the extremity in 72.9% of the patients. We determined lung metastasis in 102 (85%) out of the 120 patients as distant metastasis. The most common adult sarcomas were liposarcoma (16.3%), malignant mesenchymal tumor (MMT) (13.9%), malignant fibrous histiocytoma (MFH) (11.2%), rhabdomyosarcoma (10.2%) and synovial sarcoma (10.2%). Seventeen patients (5.3%) had grade 1 tumor, 143 patients (52.2%) had grade 2 tumor, and 112 patients (41.4%) had grade 3 tumor. In 45 patients (15.3%), the grade of the tumors is unknown. The tumor size was 0 to <5 cm in 54 cases (19.4%), 5–10 cm in 117 cases (41.9%) and >10 cm in 108 cases (38.7%). In 15 cases (5.1%), tumor size was unknown. Ninety-five patients (32.4%) were treated with adjuvant chemotherapy, and 125 patients (42.7%)) were treated with palliative chemotherapy. Prognostic factors influencing the overall survival were tumor size, grade, adjuvant radiotherapy and chemotherapy. Adjuvant radiotherapy had influence on disease-free survival. While tumor grade and size showed a significant value for predicting local recurrence, grade, localization of tumor, adjuvant chemotherapy and radiotherapy had an impact on metastasis development. The 1-year overall survival for all patients was 73.4%, 3-year overall survival was 51.8%, and 5-year overall survival was 45.1%.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Sarcomas are malignant tumors derived from cells of mesenchymal origin. They account for 1% of all malignancies [1]. The American Cancer Society’s most recent estimates for soft tissue sarcomas in the United States are for 2009 (adults and children): about 10,660 new soft tissue sarcomas will be diagnosed. A total of 3,820 Americans are expected to die of soft tissue sarcomas. A study from our hospital showed a 3% incidence of soft tissue sarcomas in 8,146 patients with cancer [2].
The dominant pattern of metastasis for soft tissue sarcoma is hematogenous. The distant metastasis usually occurs in lungs, whereas the distant metastasis of primary gastrointestinal and gynecologic sarcomas mainly occurs in the liver. Lymph node metastases may occur in rhabdomyosarcoma, synovial sarcoma, epithelioid sarcoma, liposarcoma, fibrosarcoma, malignant fibrous histiocytoma and dermatofibrosarcoma protuberans [3]. The histological grade of a soft tissue sarcoma remains the most important prognostic factor [4–7]. Rhabdomyosarcomas and synovial sarcomas are high-grade sarcomas.
Soft tissue sarcomas were retrospectively analyzed, and the influence of prognostic factors for overall survival, disease-free survival, local recurrence and distant metastasis was examined.
Materials and methods
We analyzed 319 patients with primary soft tissue sarcoma followed between 1996 and 2002 in Ankara Oncology Hospital. Variables studied included age, sex, tumor size, localization, grade, histopathological subtypes, type of surgery, types of chemotherapy (adjuvant/palliative) and radiotherapy, localization of metastasis, local recurrence, disease-free survival and overall survival. A total of 294 patients were examined, and 25 patients were excluded because of incomplete data.
Statistical analysis
Statistical computations were performed using Statistical Package for the Social Sciences (SPSS 11.5). Continuous variables were expressed as mean ± std. deviation, and categorical variables were expressed as percentage. Overall survival and disease-free survival were estimated according to the Kaplan–Meier method. Univariate and multivariate analyses were performed using the Cox proportional hazards regression model. Statistical significance was defined as P < 0.05.
Results
There were 170 male (57.8%) and 124 female patients (42.2%). Patient age ranged from 16 to 80 years, with a median age of 45 years. Median follow-up was 41 months (range, 2–84 months). The primary tumor involved the upper extremity in 33 patients (11.2%), the lower extremity in 179 patients (60.8%), the trunk in 34 patients (11.5%) and the retroperitoneum in 33 patients (11.2%). The histopathological characteristics of the study population are listed in Table 1.
We determined lung metastasis in 102 patients (85%), bone metastasis in 3 patients (2.4%) and liver metastasis in 2 patients (1.6%), out of the 120 patients with distant metastasis. Local recurrence was noted in 90 patients (29.4%). Treatment consisted of adjuvant radiotherapy in 125 (42.7%) patients and palliative radiotherapy in 57 (19.5%) patients. Chemotherapy was administered to 220 (74.8%) patients. A total of 95 patients (32.3%) were treated with adjuvant chemotherapy (IMA: 60 patients, CyVADIC, 20 patients; VAC, 9 patients; and the other chemotherapy regimens, 6 patients), and 125 (42.5%) were treated with palliative chemotherapy.
The tumor size was 0 to <5 cm in 54 cases (18.4%), 5–10 cm in 117 cases (39.8%), >10 cm in 108 cases (36.7%) and not definite 15 cases (5.1%). The 5-year overall survival was 75% for patients with tumor size 0 to <5 cm; 36.8% for patients with tumor size 5–10 cm; and 32% for patients with tumor size >10 cm. A total of 105 (35.7%) patients had grade 3 tumor; 127 had (43.2%) grade 2 tumor; and 17 (5.8%) had grade 1 tumor. For 45 patients (15.3%), the grade was unknown. The 5-year overall survival was 92.9% for patients with grade 1 tumor; 47.9% for patients with grade 2 tumor; and 27.9% for patients with grade 3 tumor (P = 0.0002). In the multivariate analysis, the mortality rates were 14.8 times higher (2.02–109.2) in grade 3 tumors (P = 0.008) and 9.14 times higher (1.26–66.4) in grade 2 tumors (P = 0.029) than in grade 1 tumors.
There was no significant influence of tumor localization and sex on 5-year survival.
The 5-year overall survival was 53.8% in patients treated with adjuvant chemotherapy and 40.3% without chemotherapy (P = 0.0045). The 1- and 3-year survival for patients treated with chemotherapy was 82.6 and 61.9%, respectively, and without chemotherapy was 69.5 and 46.9%, respectively. The 5-year overall survival was 62.2% in patients treated with adjuvant radiotherapy and 32.1% without radiotherapy (P < 0.0001). According to the multivariate analysis, the 1- and 3-year survival for patients treated with radiotherapy was 82.6 and 61.9%, respectively, and without radiotherapy was 63.5 and 38.5%; respectively.
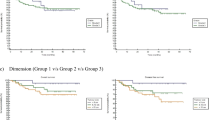
There was no significant difference in overall survival between the age <50 years and the age greater than 50 years (P = 0.9727). The 1-year overall survival for all patients was 73.4%, 3-year overall survival was 51.8%, and 5-year overall survival was and 45.1% (Fig. 1). The tumor grade and size increased the local recurrence rate insignificantly. Local recurrence rate of patients treated with radiotherapy was 22.1% and without radiotherapy was 39.8% (P < 0.001). The metastasis ratio rose significantly with increasing tumor size and grade. The metastasis rates were 6.3% in grade 1 tumor; 36.8% in grade 2 tumor; and 60.6% in grade 3 tumor (P < 0.001). The metastasis rate of patients with a tumor size of 0 to <5 cm was 25.5%; 5–10 cm was 47.9%; and >10 cm was 48.1% (P < 0.001). The patients with extremity tumors (45.9%) had a significantly higher rate of distant metastasis than the patients with tumors in other sites (30%) (P = 0.014). The rate of distant metastasis was significantly lower in the group treated with adjuvant radiotherapy (P < 0.001), but not significantly lower in the group treated with chemotherapy (P = 0.065).

Overall survival for all patients
There was statistically significant influence of tumor size, grade, adjuvant radiotherapy and adjuvant chemotherapy on 1-, 3- and 5-year overall survival. The age, tumor localization and sex did not influence the survival (Table 2). Disease-free survival was longer in the patients with tumor size 0 to <5 cm, compared with the patients with tumor size 5–10 cm and >10 cm (P = 0.0009). Disease-free survival was significantly shorter in the patients with high-grade tumors (P = 0.0005). Age, sex, tumor localization, adjuvant chemotherapy and radiotherapy did not significantly influence on disease-free survival.
The 1-, 3- and 5-year disease-free survival for all patients was 62.0, 43.1 and 41.2%; respectively (Fig. 2).

Disease-free survival for all patients
Discussion
Soft tissue sarcomas occur in the extremities (60%), gastrointestinal tract (GIST) (25%), retroperitoneum (15–20%), and head and neck region [8]. In our study; sarcomas are located in the extremities in 72.4% of patients (upper extremity 11.3%, lower extremity 61%), in the trunk 11.6%, in the retroperitoneum 10.9% and in the head and neck region 4.1%. Histological subtype and grade indicate the biological behavior and metastatic spread of the sarcomas. A study on 1,240 patients with sarcoma showed that the histology of MFH was 28%, liposarcoma was 15%, synovial sarcoma was 10%, rhabdomyosarcoma was 5% and unclassified sarcoma was 11%. MFH and liposarcomas were frequently located in extremities, whereas leiomyosarcomas were in abdomen [5]. In our study, the most common adult sarcomas were liposarcoma (16.3%), MMT (13.9%), MFH (11.2%), synovial sarcoma (10.2%), rhabdomyosarcoma (10.2%) and leiomyosarcoma (7.8%). The most common histological subtypes were liposarcoma and MFH in extremities and leiomyosarcoma in retroperitoneum, as consistent with literature. The high rate of MMT in our study can be explained with the limited number of well-developed center that can perform immunohistochemical staining.
Tumor grade is a significant prognostic factor for overall survival [9]. In this study, the 5-year overall survival was determined as, 92.9% for patients with grade 1 tumor; 47.9% for patients with grade 2 tumor; and 27.9% for patients with grade 3 tumor (P = 0.0002).
The most common site of distant metastasis in sarcomas is the lung. Visceral and retroperitoneal sarcomas show a propensity to metastasize to the liver and peritoneum [10]. In a study, the lung was noted to be the most common site of distant metastases in patients with MFH (23%), synovial sarcoma (19%) and leiomyosarcoma (15%) [11]. In our study, 20.1% of patients had distant metastasis. The common sites were the lungs (85%), bone (2.4%) and liver (1.6%). Synovial sarcoma (56.6%), MFH (48.5%) and rhabdomyosarcoma were the most frequent cause of lung metastases. Our findings were consistent with the literature [10]. Tumor grade and size showed a significant value for predicting metastasis development. Adjuvant radiotherapy decreased the rate of distant metastasis, but adjuvant chemotherapy had no effect on development of distant metastasis. The mortality rate in tumors of size >10 cm was 2.81 (1.49–5.31) times higher than the tumors of the size 5–10 cm (P < 0.0001) and 1.96 (1.04–3.7) times higher than the tumors of size 0 to <5 cm (P = 0.038).
In several studies, age greater than 50 years, positive microscopic margin, presentation with locally recurrent tumor and histological subtype were found to be predictive factors for the local recurrence [9]. In our study, age, sex, localization and grade did not predict local recurrence. Tumor size and histological subtypes (Kaposi’s sarcoma, liposarcoma, MFH and rhabdomyosarcoma) influenced local recurrence but were statistically insignificant. Adjuvant radiotherapy significantly decreased the local recurrence. Insufficient cancer surgery services in our country and inadequate biopsy techniques could have changed the results.
In soft tissue sarcomas, adjuvant chemotherapy reduces local recurrence and distant metastasis rate and provides survival advantage [12–14]. In the studies of “Intergroup Sarcoma Study Group”, ECOG and Boston, chemotherapy with doxorubicin had no influence on overall survival and disease-free survival [15]. A study from Rizzoli Orthopedic Institute denoted that the disease-free survival was 79% in the adjuvant chemotherapy arm and 45% in the observation arm [12]. Adjuvant combination chemotherapy found to have a positive impact on the local control and disease-free survival, but not on the overall survival in the study of European Organization for Research and Treatment of Cancer (EORTC) [13]. In the study of Italian Sarcoma Group, overall survival was found 72% in chemotherapy arm and 55% in control arm (P = 0.002) [14]. A meta-analysis of combination chemotherapy stated no significant difference in overall survival between chemotherapy arm and control arm [15]. Zalupski et al. showed 10% improvement in overall survival (81 vs. 71%; P = 0.0005) and 15% improvement in disease-free survival (68 vs. 53%; P < 0.00001) with adjuvant chemotherapy [16]. In other meta-analysis, 10-year disease-free survival was found to be higher (55 vs. 45%; P = 0.0001) in chemotherapy arm, but the improvement in overall survival was not statistically significant (54 vs. 50%; P = 0.12). In the subgroup analysis, 7% improvement in overall survival was denoted in patients with extremity sarcoma in chemotherapy arm (P = 0.029) [17]. In our study, adjuvant chemotherapy was performed to 95 patients with high-grade sarcoma. The 5-year overall survival was 53.8% in patients treated with adjuvant chemotherapy and 40.3% without chemotherapy (P = 0.0045). We determined 13.5% improvement in overall survival. There was no benefit of adjuvant chemotherapy on disease-free survival (P = 0.5662). This inconsistency with literature may be the result of insufficiently detailed data on patients in the years 1996–2000.
The most effective agents are doxorubicin (response rate: 20%), dacarbazine and ifosphamide (response rate: 20–25%) in advanced adult soft tissue sarcoma [18, 19]. The response rate of combination chemotherapy with doxorubicin + dacarbazin is 17% [20], doxorubicin + ifosphamide or epirubicine + ifosphamide is 25% [18, 21], MAID is 32% and CyVADIC is 20% [22]. In our study, 58 (20%) patients had metastatic disease at presentation. The most common chemotherapy regimens used in these patients were IMA (81%), CyVADIC (13.7%) and VAC (5.1%). There was no statistically significant difference in overall survival between the patients treated with and without chemotherapy. The second-line chemotherapy regimens also did not have an impact on the overall survival.
Age, sex, tumor size, grade and localization are declared as prognostic factors on overall survival in the literature [23]. Positive microscopic margin, age and localization of recurrence are the prognostic factors for the local recurrence [24]. Adverse prognostic factors of retroperitoneal sarcomas are high-grade tumor, incomplete resection and unresectable disease [25]. In our study, the 1-, 3- and 5-year overall survival rates were consistent with the literature [26]. According to this study, the statistically significant prognostic factors influencing the overall survival in adult soft tissue sarcoma were tumor size, grade, adjuvant radiotherapy and chemotherapy. Age, sex and tumor localization found to have no impact on overall survival. The factors influencing on disease-free survival were tumor size and grade.
In conclusion, researches regarding the molecular mechanisms of metastatic sarcoma will most likely be the basis of new effective therapeutic regimens in this complex tumor group.
References
The American Cancer Society; cancer reference information. What are the key statistics about soft tissue sarcoma? www.cancer.org.
Alkış N, Utkan G, Durnalı AG, Arslan ÜY, Çelenkoğlu G, Tokluoğlu S, et al. Epidemiologic properties of patients who had admitted to Ankara oncology hospital department of medical oncology. Ann Oncol. 2006;17(supll: 9):abst: 830.
Charles AF, Dennis AC. Sarcomas. In: Dennis AC, Mary CT, editors. Manual of clinical oncology. 6th ed. Philadelphia: Lippincott Williams and Wilkins; 2009. p. 384–96.
Coindre JM, Terrier P, Bui NB, Bonicho F, Collin F, Doussal VL, et al. Prognostic factors in adult patients with locally controlled soft tissue sarcoma. A study of 546 patients from the French federation of cancer centers sarcoma group. JCO. 1996;14:869–77.
Coindre JM, Terrier P, Guillou L, Le Doussal V, Collin F, Ranchère D, et al. Predictive value of grade for metastasis development in the main histologic types of adult soft tissue sarcomas: a study of 1,240 patients from the French federation of cancer centers sarcoma group. Cancer. 2001;91:1914–24.
Costa J, Wesley RA, Glatstein E, Rosenberg SA. The grading of soft tissue sarcomas: results of a clinicopathological correlation in a series of 163 cases. Cancer. 1984;53:530–41.
Guillou L, Coindre JM, Bonichon F, Nguyen BB, Terrier P, Collin F, et al. Comparative study of the national cancer institute and French federation of cancer centers sarcoma group grading systems in a population of 410 adult patients with soft tissue sarcoma. JCO. 1997;15:350–62.
National Comprehensive Cancer Network; Practice guideline in oncology v.2.2009, www.nccn.org.
Pisters PW, Leung DH, Woodruff J, Shi W, Brennan MF. Analysis of prognostic factors in 1,041 patients with localized soft tissue sarcomas of the extremities. JCO. 1996;14(5):1679–84.
Muray FB, Samuel S, Robert GM, Brian OS. Sarcomas of the soft tissue and bone. In: DeVita VT, Lawrence TS, Rosenberg SA, editors. Cancer principles & practice of oncology. 8th ed. Philadelphia: Lippincott Williams and Wilkins; 2009. p. 1741–94.
Temple LK, Brennan MF. The role of pulmonary metastasectomy in soft tissue sarcoma. Semin Thorac Cardiovasc Surg. 2002;14(1):35–44.
Gherlinzoni F, Bacci G, Picci P, Capanna R, Calderoni P, Lorenzi EG, et al. A randomized trial for the treatment of high-grade soft-tissue sarcomas of the extremities: preliminary observations. JCO. 1986;4(4):552–8.
Bramwell V, Rouesse J, Steward W, Santoro A, Schraffordt-Koops H, Buesa J, et al. Adjuvant CYVADIC chemotherapy for adult soft tissue sarcoma—reduced local recurrence but no improvement in survival: a study of the European organization for research and treatment of cancer soft tissue and bone sarcoma group. JCO. 1994;12(6):1137–49.
Frustaci S, Gherlinzoni F, Paoli AD, Bonetti M, Azzarelli A, Comandone A, et al. Adjuvant chemotherapy for adult soft tissue sarcomas of the extremities and girdles: results of the Italian randomized cooperative trial. JCO. 2001;19(5):1238–47.
Antman K, Ryan L, Borden E, Wood WC, Lerner HL, Corson JM, et al. Pooled results from three randomized adjuvant studies of doxorubicin versus observation in soft tissue sarcoma: 10 year results and review of literature. In: Salmon SE, editor. Adjuvant therapy of cancer VI. Philadelphia: W.B. Saunders Company; 1991. p. 529–42.
Zalupski MM, Ryan JR, Hussein ME, Baker LH. Defining the role of adjuvant chemotherapy for patients with soft tissue sarcoma of the extremities. In: Salmon SE, editor. Adjuvant therapy of cancer VII. Philadelphia: JB Lippincott; 1993. p. 385–92.
Adjuvant chemotherapy for localized resectable soft-tissue sarcoma of adults: meta-analysis of individual data, Sarcoma Meta-analysis Collaboration. Lancet 1997;350 (9092):1647–1654.
Casson AG, Putnam JB, Natarajan G, Johnston DA, Mountain C, McMurtrey M, et al. Five-year survival after pulmonary metastasectomy for adult soft tissue sarcoma. Cancer. 1992;69(3):662–8.
Gary TV, James AW, Deborah LD, Constantine K, Nicholas JP, Hiroshi T. Resection of lung metastases from soft-tissue sarcomas. A multivariate analysis. Arch Surg. 1992;127(12):1407–11.
Weksler B, Lenert J, Bruce NG, Burt M. Isolated single lung perfusion with doxorubicin is effective in eradicating soft tissue sarcoma lung metastases in a rat model. J Thorac Cardiovasc Surg. 1994;107:50–4.
Santoro A, Tursz T, Mouridsen H, Verweij J, Steward W, Somers R, et al. Doxorubicin versus CYVADIC versus doxorubicin plus ifosfamide in first- line treatment of advanced soft tissue sarcomas: a randomized study of the European organization for research and treatment of cancer soft tissue and bone sarcoma group. JCO. 1995;13(7):1537–45.
Lorıgan PC, Verweıj J, Papaı Z, Rodenhuıs S, Cesne AL, Leahy M, et al. On behalf of the EORTC SOFT TISSUE AND BONE SARCOMA GROUP. Randomised phase III trial of two investigational schedules of ifosfamide versus standard dose doxorubicin in patients with advanced or metastatic soft tissue sarcoma (ASTS). Proc Am Soc Clin Oncol (ASCO). 2002 (abs. 1616).
Glabbeke MV, van Oosterom AT, Oosterhuis JW, Mouridsen H, Crowther D, Somers R, et al. prognostic factors for the outcome of chemotherapy in advanced soft tissue sarcoma: an analysis of 2, 185 patients treated with anthracycline-containing first-line regimens—a European organization for research and treatment of cancer soft tissue and bone sarcoma group study. JCO. 1999;17(1):150.
Collin CF, Friedrich C, Godbold J, Hajdu S, Brennan MF. Prognostic factors for local recurrence and survival in patients with localized extremity soft tissue sarcoma. Semin Surg Oncol. 1988;4:30–7.
Pirayesh A, Chee Y, Helliwell TR, Hershman MJ, Leinster SJ, Fordham MV, et al. The management of retroperitoneal soft tissue sarcoma: a single institution experience with a review of the literature. Eur J Surg Oncol. 2001;27:491–7.
Öztop İ, Yılmaz U, Havıtçıoğlu H, Şen M, Demirkan B, Özkal S, et al. Our experience of patents with soft tissue sarcomas treated between 1990 and 2002. Turkish J Hematol Oncol. 2003;13(2):61–71.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Alkis, N., Muallaoğlu, S., Koçer, M. et al. Primary adult soft tissue sarcomas: analysis of 294 patients. Med Oncol 28, 391–396 (2011). https://doi.org/10.1007/s12032-010-9450-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12032-010-9450-2