
Abstract
Although our understanding of microorganisms has advanced significantly and antimicrobial therapy has become increasingly available, infection remains a major cause of patient morbidity and mortality. The use of radiopharmaceuticals for diagnosis of infection is increasing due to their ability to distinguish between septic and aseptic inflammation. A wide range of radiopharmaceuticals have been proposed to visualize infection and inflammation scintigraphically. Ceftazidime a cephalosporin antibiotic used to treat bacterial infections was investigated to label with 99mTc. Labeling was performed using sodium dithionite as reducing agent at 100 °C for 10 min and radiochemical analysis involved ITLC and HPLC methods. The stability of labeled antibiotic was checked in the presence of human serum at 37 °C up to 24 h. The maximum radiolabeling yield was 95.4 ± 2.0 % corresponding to a specific activity of 178 GBq/mmol. Bacterial binding assay was performed with S. aureus and the in vivo distribution was studied in mice. Images showed minimal accumulation in nontarget tissues, with an average target/nontarget ratio of % 1.4 ± 0.2.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
A wide range of radiopharmaceuticals have been proposed to visualize infection and inflammation scintigraphically. Radiolabeled leukocytes and 67Ga-citrate are the most commonly applied radiopharmaceuticals [1, 2]. Various 99mTc labeled agents such as polyclonal and monoclonal antibodies [3], cytokines [4], chemo tactic peptides [5, 6], HMPAO leukocytes [7] and human defensins [8–11] have been introduced or proposed to visualize bacterial infections and sterile inflammatory processes. Also radiolabeled leucocytes can be considered as “gold standard” that can visualize a majority of infectious and inflammatory lesions but it is labor-intensive and the in vitro labeling carries risks of handling potentially contaminated blood and also requires specialized equipment, taking approximately 3 h [12].
The use of radiolabeled antibiotics presents a promising approach for the precise diagnosis and detection of infectious lesions, because they specifically bind to the bacterial components, making it possible to differentiate between infectious and sterile lesions [13]. Antibiotics localize in the infectious focus, where they are frequently taken up and metabolized by microorganisms. Ciprofloxacin is a first generation fluroquinolone antibiotic which is active against both gram positive and gram negative bacteria. It binds to DNA gyrase and topoisomerase IV enzymes and thus interferes with the strand cutting and resealing function during DNA replication in bacteria [14]. Solanki et al. [15, 16] labeled ciprofloxacin with 99mTc in 1993, supplied under the name of Infecton. They used formamidine sulphonic acid as the reducing agent that had to be boiled before use. Later the preparation was modified by using stannous tartarate reduction method that did not require boiling, but the pH of injectable radiopharmaceutical was quite low at 4 [13]. Both these methods used two-vial kits for final preparation, whereas most of the clinically used radiopharmaceuticals in nuclear medicine imaging are single-vial kits. Besides, significant amount of colloid formation upon reconstitution with 99mTcO −4 has also been reported with this kit [16].
Bhardwaj et al. [17] have recently reported formulating a single vial kit for the preparation of 99mTc-ciprofloxacin which appears to have better shelf life and stability as compared to the available alternatives. This kit contains stannous tartarate as a reducing agent and NaCl or KCl as excipients.
Second and third generation cephalosporines, including cefuroxime and ceftizoxime have been labeled with 99mTc previously and our group reported the radiolabeling of cefotaxime in 2011 [18, 19]. Ceftizoxime has a wide spectrum of activity to the beta lactamase, binds onto the bacterial wall, and inhibits the synthesis of bacterial wall, which drives to bacterial death. It has the half life of 1.7 h being almost totally eliminated within 24 h. ceftizoxime and cefotaxime structural formulas differ only by an acetoxy group at position 3 on the beta-lactam ring.
Ceftazidime is the other third-generation cephalosporin antibiotic with the biological half life of 1.6–2 h. Like other third-generation cephalosporines, it has broad spectrum activity against gram positive and gram negative bacteria.
Depending on the previous promising results of the existing radiopharmaceuticals used for infection imaging [10, 18, 20–25] and our recently reported 99mTc labeled antibiotics intended for infection imaging, finding the more sensitive and specific infection tracers motivates us to this research. In this paper to compare other radiolabeled antibiotics in the same group of cephalosporines as the follow of our previous works [26], we describe the optimum condition for radiolabeling of ceftazidime with the most widely used imaging radionuclide, 99mTc. Factors affecting the radiolabeling yield of the complex and biological distribution bearing animals were studied in details.
Experimental
Reagents
All chemicals were purchased from Merck or Fluka. Chemicals and solvents were of highest purity and analytical grade and used without further purification. 99mTc-pertechnetate was supplied by AEOI, as 99Mo/99mTc generator.
All radioactivity measurements were carried out using NaI (Tl) scintillation counter (ORTEC Model 4001 M Minibin & Power Supply).
Radiolabeling procedure
Ceftazidime (2.5 mg) was dissolved in 200 μl distilled water. To determine the optimal amount of reducing agent, sodium dithionate in different concentrations (4.25–8.25 mg/200 μl NaHCO3 0.5 %) was added. The Then 370–740 MBq freshly eluted pertechnetate solution (in max. 1 ml of saline) was added into the vial in different pH ranges between 7.5 and 10.5. Finally the reaction mixture was heated in a boiling water bath for different times from 5 to 60 min.
Radiochemical and HPLC analysis of 99mTc-ceftazidime
The labeling yield and radiochemical purity were determined by thin layer chromatography. The reaction product was spotted on silica gel ITLC-SG strips (Sigma Chemical Company, USA) (10 × 1.5 cm2 sheets) and developed in acetone and ACD (citrate-dextrose buffer solution) as the mobile phase. After developing, they were cut into 1 cm pieces and counted with a NaI (Tl) detector equipped with a single channel analyzer.
Analytical reverse phase high performance liquid chromatography (RP-HPLC) was performed on a JASCO 880-PU intelligent pump HPLC system equipped with a multiwave length detector and a flow through RAYtest-Gabi gamma detector. CC 250/4.6 Nucleosil 120-5 C18 column from Teknokroma was used for analytical HPLC. A mixed solvent containing 10 % ethanol and 0.2 M phosphate buffer, pH 7.2 and flow rate 0.5 ml/min was used for analytical HPLC.
Stability of 99mTc-ceftazidime in human serum
The affinity of the labeled antibiotic to human serum proteins was examined by mixing 1 ml of labeled ceftazidime with activity between 5 and 20 mCi to 1 ml of human serum in a vial. The sample was incubated in 37 °C for 24 h and 100 μl of reaction mixture was placed on a Sephadex G25-column to evaluate the complex affinity to plasma protein. After washing the column with PBS or normal saline, activity bound to serum protein and labeled ceftazidime was measured with a well-type gamma counter.
To test the serum stability of 99mTc-ceftazidime complex, we added 1 ml of freshly prepared human serum to 100 μl of labeled antibiotic. The mixture was incubated in 37 °C for 24 h then the serum protein was denatured by mixing 100 μl of the solution with 100 μl absolute ethanol. After that, the mixture was centrifuged at 2,000 g in 4 °C for 10 min. Radiochemical stability was determined by taking samples of 10 μl of supernatant at different times up to 24 h of incubation that were analyzed by ITLC.
In vitro binding of 99mTc-ceftazidime to bacteria
Binding of 99mTc-ceftazidime to bacteria was assessed by the method described previously [27–29]. Briefly, 0.1 ml 99mTc-ceftazidime (37 MBq) was transferred to a test tube. Then, 0.9 ml of 50 % (v/v) 0.01 M acetic acid in phosphate buffer (Na-PB, pH 7.5) containing approximately 1 × 108 colony forming units (CFU) per ml viable Staphylococcus aureus were added. The mixture was incubated for 1 h at 4 °C and thereafter the vials were centrifuged in a pre-cooled centrifuge for 5 min at 2,000 g at 4 °C. The supernatant was removed, and the radioactivity in the bacterial pellet was gently re-suspended in 1 ml of Na-PB and re-centrifuged as above. The supernatant was removed and the radioactivity in the bacterial pellet was determined by gamma counter. The radioactivity related to bacteria was expressed in percent of the added 99mTc activity bounded to viable bacteria in regard to total 99mTc.
Partition coefficient (log P value)
About 100 μl of the labeled compound was mixed with 0.9 ml water and 1 ml of n-octanol on a vortex mixer for about 1 min the two phases were allowed to separate. Equal aliquots of the organic and aqueous layers were withdrawn and measured for radioactivity to determine the partition coefficient (log p = activity in octanol/activity in water). The log p data are reported as an average plus the standard variation based on the results from the three independent measurements.
Animal biodistribution
Male Swiss mice, weighing 25–30 g were infected by injecting 0.1 ml of saline containing 1 × 108 CFU bacteria into right thigh muscle. After 24 h, they were injected under ether anesthesia with 74 MBq of 99mTc-ceftazidime in saline into the tail vein. At 1 h after injection, accumulation of the tracer in infected area was assessed by planar scintigraphy under ether anesthesia. For ex vivo counting, mice were sacrificed after 1, 2 and 24 h and organs of interest were collected, weighed and radioactivity was measured in a γ-counter.
Statistical analysis
The calculations of means and standard deviations were performed on Microsoft Excel. Student’s t test was used to determine statistical significance. Differences at the 95 % confidence level (p < 0.05) were considered significant.
Results and discussions
Radiolabeling, radiochemistry and radiochemical purity
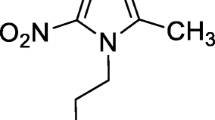
The chemical structure of ceftazidime is presented in Fig. 1. The various complexes of 99mTc may be formed by interactions between electron donor atoms and reduced technetium. In order to form bonds with technetium, the structure must contain electron donors such as oxygen, nitrogen and sulfur. Although the exact complex structure is not known, results showed that ceftazidime coordinated with 99mTc because of its electron donor atoms in its structure [30, 31].

Structure of ceftazidime
Labeling efficiency, radiochemical purity and stability were assessed by RTLC. In RTLC-SG chromatography using Acetone as the solvents, reduced 99mTc and 99mTc-ceftazidime remained at the point of spotting, while free 99mTcO −4 moved towards the solvent front. In using ACD solution as solvent, reduced 99mTc and 99mTcO −4 moved to the front, where as 99mTc-ceftazidime remained at the point of spotting. The maximum radiolabeling yield of ceftazidime was 92 ± 2 % and it was stable at least for 12 h. The HPLC elution time were 650 ± 36 S for pertechnatate and 750 ± 42 S for 99mTc-ceftazidime (Fig. 2).

HPLC radiochromatogram of just pertechnetate appeared in 650 s (up) and 99mTc-ceftazidime complex started from 750 s (down). Conditions: solvent: 10 % ethanol on 0.2 M phosphate buffer, pH 7.2, column: RP C18, flow rate: 0.5 ml/min
Sodium dithionate was chosen for the reduction of 99mTc from +7 to lower valence state, which facilitate its chelating by compounds of diagnostic impotence. The effects of sodium dithionite amount as reducing agent are summarized in Fig. 3. The data showed that the radiochemical yield was dependent on the amount of sodium dithionite present in the reaction mixture. The effect of reducing agent was studied between 4.25 and 8.25 mg of sodium dithionite. The results in Fig. 3 showed that, efficient yield was achieved by using 7.25 mg of sodium dithionite. Below this value, the reducing agent is not sufficient for complete reduction of pertechnetate to form 99mTc-complex and, by increasing the amount of reducing agent the labeling yield decreased again. This may be due to the fact that the most of the ligand molecules were consumed in the formation of the complexes, so the pertechnetate is reduced to insoluble technetium (IV) 99mTcO2·xH2O in the absence of ligand.

Effect of sodium dithionite content
The effect of pH was shown in Fig. 4. The pH of the reaction medium was found to play an important role in the labeling process. The effect of pH on the radiolabeling yield was examined for pH 7.5–10. The highest labeling yield obtained at pH 8.5–9.

Effect of pH on the labeling yield of 99mTc-ceftazidime
The effect of heating time (shown on Table 1) on the formation of the 99mTc-ceftazidime shows that by increasing the optimum time for heating the vial is 15 min, and with increasing the heating time the radiolabeling yield will decrease up to 76.5 %.
Serum study and bacterial binding assay
The affinity of the labeled antibiotic to human serum proteins after 24 h was about 25 ± 5 % and labeled antibiotic was stable in human serum with radiochemical purity of more than 85 % after 24 h.
In vitro testing of 99mTc-ceftazidime to S. aureus showed 35 % of radioactivity bound to bacteria. It should be mentioned that in the in vitro competition assay we observed the inhibition of binding of 99mTc-ceftazidime to S. aureus by unlabeled ceftazidime with maximal inhibition of approximately 80 % when 100-fold excess of unlabeled antibiotic was used as competitor.
In vivo experiments
Based on data presented in Table 2, we conducted biodistribution analysis of 99mTc-ceftazidime complex in normal and abscess-bearing mice at different time intervals post injection. For non targeted organs (liver, spleen, heart and lung) the uptake of the tracer was similar, to a large extent, to the normal mice. In most organs, the activity (expressed as percent injected dose/g organ, ID/g Organ) declined at 4 h post injection. One possible advantage of 99mTc-ceftazidime over 99mTc-ciprofloxacine (Infecton) is lesser hepato-biliary excretion with the new radiotracer. Lower intestinal excretion would be advantageous in identifying infective intestinal lesions. Accumulation of the complex in the infected tight muscles as indicated by T/NT ratio was 1.4 ± 0.2 1 h post injection. The kidney shows the maximal activity 1 h post injection and it shows the main route of excretion of the radiotracer. As opposed to Infecton, ceftazidime is more rapidly depurated from the organism, thus diminishing the circulating pool and favoring the specific capture by the infectious site.
The log p value of the complex was found to be −2.1 ± 0.2 reflecting its low lipophilicity. The low n-octanol/water partition coefficient is also associated with the lower and shorter retention in background tissues and blood [32]. Therefore, the nature of radiolabeled antibiotic might result in lower uptake in the normal tissues and faster clearance so as to obtain favorable target to non-target (tissues) ratios and these results are in accordance with the biodistribution results.
Typical Scintigrams of mice’ with infectious thigh muscle at 1 h after injection of radiotracer are shown in Fig. 5, as it is clear in the scintigram, high uptakes of activity in infection site with low accumulation in non-infected muscle. Upon autopsy the bacterial infection had the same appearance as demonstrated on the Scintigraphic image.

Typical scintigram of infected mice with thigh muscle infection at 1 h post injection
Infecton, a wide spectrum fluoroquinolone, have a biological half-life of 3.5–4.5 h. Approximately 60 % of the injected activity has been recovered in urine by 24 h post injection [33, 34]. Since ciprofloxacin has a low molecular weight (MW = 331.3), low degree of interaction with plasma protein (20–40 %) and a biological half-life of 4.5 h, it can be considered that, it would interact with a variety of factors before interacting with bacteria.
Ceftizoxime, third generation cephalosporin, has a half life of 1.7 h, being almost totally eliminated within 24 h after administration [35]. As opposed to Infecton, ceftizoxime is more rapidly depurated from the organism, thus diminishing the circulating pool and favoring the specific capture by the infectious site over the non-specific but high biliary excretion was seen by radiolabeled ceftizoxime [36].
From the same category, ceftazidime, with the biological half life of 1.7 h (MW = 546.58) has a lower degree of interaction with plasma protein (25 ± 5 %). New radiotracer eliminates mainly from the kidney and log p value proves this matter. 99mTc-ceftazidime has a higher uptake in the septic abscess than the non-infected muscle (p < 0.05) and its uptake in the septic muscle remains stable along 1 h post injection. Finally, considering the criteria for obtaining an ideal radiopharmaceutical, 99mTc-ceftazidime fits the criteria better and may be applied for infection imaging.
Conclusion
In this study labeling of ceftazidime, a with 99mTc- was 95.4 ± 2.0 %. The labeling of 99mTc-ceftazidime was performed by using sodium dithionite as a reducing agent. The labeling of 99mTc-ceftazidime was optimal in the following reaction mixture: ceftazidime (2.5 mg in 200 μl distilled water), 7.25 mg of Na2S2O4 in 200 μl NaHCO3 0.5 %, pH: 8.5–9, reaction time: 10 min and reaction temperature: 100 °C. The resulting complex is quite stable and labeling of 95.4 ± 2.0 % is maintained for up to 12 h. The complex formed by chelation of 99mTc with ceftazidime is a very strong and stable as suggested by in vitro serum stability and in vivo bio-distribution experiment.
As a compare to Infecton, we observed that the radiolabeling yield of ceftazidime (95.4 ± 2.0 %) is better than ciprofloxacin (>90 %) and also radiolabeling of ciprofloxacin has some limits and some difficulties that are not included in the radiolabeling of ceftazidime [37]. In addition, the clearance route of ciprofloxacin is from liver but this antibiotic showed an improvement in excretion pathway from liver to kidney followed by an accumulation of radioactivity in infected areas. These promising characteristics make our new radiotracer as a very suitable candidate for diagnostic of infectious foci in nuclear medicine and it can be introduced as an alternative radiotracer for infection imaging agent.
References
Becker W (1995) The contribution of nuclear medicine to the patient with infection. Eur J Nucl Med 22(10):1195–1211
Das SS, Hall AV, Wareham DW, Britton KE (2002) Infection imaging with radiopharmaceuticals in the 21st century. Braz Arch Biol Technol 45:25–37
Pak KY, Nedelman MA, Tam SH, Wilson E, Daddona PE (1992) Labeling and stability of radiolabeled antibody fragments by a direct 99mTc-labeling method. Int J Rad Appl Instrum B 19(6):669–677
Signore A, D’Alessandria C, Annovazzi A, Scopinaro F (2002) Radiolabeled cytokines for imaging chronic inflammation. Braz Arch Biol Tech 45:15–23
Knight LC (2003) Non-oncologic applications of radiolabeled peptides in nuclear medicine. Q J Nucl Med 47(4):279–291
Weiner RE, Thakur ML (2001) Radiolabeled peptides in diagnosis and therapy. Semin Nucl Med 31(4):296–311
Cardoso VN, Plaza PJ, Roca M, Armero F, Martín-Comin J (2002) Assessment of inflammatory bowel disease by using two different (99 m)Tc leucocyte labeling methods. Nucl Med Commun 23(8):715–720
Yeaman MR, Yount NY (2003) Mechanisms of antimicrobial peptide action and resistance. Pharmacol Rev 55(1):27–55
Gandomkar M, Najafi R, Shafiei M, Mazidi M, Goudarzi M, Mirfallah SH et al (2009) Clinical evaluation of antimicrobial peptide [(99 m)Tc/Tricine/HYNIC(0)]ubiquicidin 29–41 as a human-specific infection imaging agent. Nucl Med Biol 36(2):199–205
Gandomkar M, Najafi R, Mazidi M, Goudarzi M, Mirfallah SH (2008) New peptid based freezed-dried kit [99 mTc-HYNIC]- UBI 29–41 as a human specific infection imaging agent. Iran J Nucl Med 16(1):25–30
Gandomkar M, Najafi R, Mazidi M, Mirfallah SH, Goudarzi M (2009) Three different procedures in labeling of Ubiquicidin with technetium 99m: a comparative study. Iran J Radiat Res 7(2):97–104
Martin-Comin J, Cardoso VN, Plaza P, Roca M (2002) Hank’s balanced salt solution: an alternative resuspension medium to label autologous leukocytes. Braz Arch Biol Technol 45:39–44
Britton KE, Vinjamuri S, Hall AV, Solanki K, Siraj QH, Bomanji J et al (1997) Clinical evaluation of technetium-99m infecton for the localisation of bacterial infection. Eur J Nucl Med 24(5):553–556
Fournier B, Zhao X, Lu T, Drlica K, Hooper DC (2000) Selective targeting of topoisomerase IV and DNA gyrase in Staphylococcus aureus: different patterns of quinolone-induced inhibition of DNA synthesis. Antimicrob Agents Chemother 44(8):2160–2165
Mirshojaei SF, Erfani M, Najafi R, Babaei MH, Talebi MH (2011) J Radioanal Nucl Chem 287:21–25
Solanki KK, Bomanji J, Siraj Q, Small M, Britton KE (1993) J Nucl Med 34:119
Bhardwaj N, Bhatnagar A, Singh AK (2005) Development and evaluation of a single vial cold kit for infection imaging: Tc-99m ciprofloxacin. World J Nucl Med 4:244–251
Tavaras W (2002) Manual de antibioticos e quimioterapicos antiinfecciosos. Atheneu, Sao Paolo
Chattopadhay S, Das SS, Chandra S, De K, Mishra M, Sarkar BR, Sinha S, Ganguly S (2010) Appl Radiat Isot 68:314–317
Zhang J, Guo H, Zhang S, Lin Y, Wang X (2008) Bioorg Med Chem Lett 18:51–57
Roohi S, Moshtaq A, Jehangir M, Ashfagq MS (2006) J Radioanal Nucl Chem 267:561–566
El-Gany EA, El-Kolaly MT, Amine AM, El-Sayed AS, Abdel-Ghelil F (2005) J Radioanal Nucl Chem 266:131–135
Shah SQ, Khan AU, Khan MR (2010) Appl Radiat Isot 68:2255–2260
Shah SQ, Khan AU, Khan MR (2010) Radiochim Acta 99:53–58
Gandomkar M, Najafi R, Shafiei M, Mazidi M, Goudarzi M, Mirfallah SH (2009) Nucl Med Biol 36:199
Gandomkar M, Najafi R, Mazidi M, Mirfallah SH, Goudarzi M (2009) Nucl Med Biol 7(2):97
Barreto VG, Iglesias F, Roca M, Tubau F, Martin-Comin J (2000) Rev Esp Med Nucl 19:479
Shah SQ, Khan AU, Khan (2010) J Radioanal Nucl Chem. doi:10.1007/s10967-010-0871-3
McAfee JG, Gagne G, Subramanian G, Schneider RF (1991) J Nucl Med 32:2126
Sampson CB (1996) Nucl Med Commun 17:648
Vallee F, Lebel M (1991) J Antimicrob Agents Chemother 35:2057
Sonmezoglu K, Sonmezoglu M, Halak M, Akgun I, Turkmen C, Onsel C, Kanmaz B, Solanki K, Britton KE (2001) J Nucl Med 42:567
Yapar Z, Kibar M, Yapar AF, Togrul E, Kayaselcuk U, Sarpel Y (2001) J Nucl med 28:822
Larikka MJ, Ahonen AK, Niemela O, Puronto O, Junila JA, Hamalainen MM, Britton KE, Syrajala HP (2002) Nucl Med Commun 23:655
Larikka MJ, Ahonen MK, Niemela O, Puronto O, Junila JA, Hamalainen MM, Britton KE, Syrajala HP (2002) Nucl Med Commun 23:655
Welling MM, Paulusma-Annema A, Balter HS, Pauwels EK, Nibbering PH (2000) Eur J Nucl Med 27:1865
Mirshojaei SF, Erfani M, Sadat Ebrahimi SE, Talebi MH, Hakj Hassan Abbasi F (2010) Iran J Nucl Med 2010 18(2):45
Acknowledgments
The authors wish to thank Mr. Talebi, Mr. Mazidi and Mr. Mirfallah of the radioisotope department (AEOI) for accompanying in biodistribution and biological tests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mirshojaei, S.F., Erfani, M. & Shafiei, M. Evaluation of 99mTc-ceftazidime as bacterial infection imaging agent. J Radioanal Nucl Chem 298, 19–24 (2013). https://doi.org/10.1007/s10967-013-2418-x
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10967-013-2418-x