
Abstract
Self-directed treatments for gambling disorder have been developed to attract individuals who are reluctant to seek formal treatment. Self-directed treatments provide individuals with information and support to initiate a recovery program without attending formal treatment. In this study, an online version of a previously evaluated telephone-based intervention package is compared to a brief online normative feedback intervention called Check Your Gambling. In a randomized controlled trial design, participants with gambling problems who were not interested in formal treatment (N = 181) were recruited through media announcements. After a baseline telephone assessment, participants were assigned to have access to either the brief Check Your Gambling, or the extended self-management tools intervention. Follow-up assessments were conducted at 3, 6, and 12 months post baseline by blinded interviewers. Participant nominated collaterals were contacted to validate self-reported gambling involvement. The follow-up rate at 12 months was 78%. Participants in both conditions showed significant reductions in days of gambling and problem severity but no differences between conditions were found, contrary to the primary hypothesis. Lack of previous treatment for gambling and higher baseline self-efficacy predicted fewer days of gambling in both conditions. Self-efficacy increased over time but did not appear to mediate changes in gambling. Participants who were most engaged in the extended online program showed better outcomes. Those with low engagement showed a slower trajectory of change but equivalent improvements by 12 months. The extended online intervention was not associated with better outcomes than the brief Check Your Gambling intervention. Future research needs to explore the attractiveness, uptake, and effectiveness of online interventions with and without therapist support to understand their potential role in gambling disorder treatment systems.
Trial Registration ISRCTN06220098.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Previous research has demonstrated the effectiveness of brief interventions for people with gambling difficulties (Swan and Hodgins 2015). These interventions have been delivered in face-to-face formats (Diskin and Hodgins 2009; Petry et al. 2008), by telephone (Abbott et al. 2018) and via self-help workbooks delivered through the mail (Boudreault et al. 2018; Hodgins et al. 2009; Labrie et al. 2012; Oei et al. 2018). Clinical trials have shown modest positive impacts compared with waitlist controls (Petry et al. 2017; Yakovenko and Hodgins 2016), that are sustained over 12–24-month follow-up periods. Because the majority of individuals with gambling problems do not seek formal treatment, even if it is readily available (Cunningham 2005), this brief, largely self-directed approach is promising. Individuals frequently report a desire to “do it on their own”, or at least try. Providing attractive and effective alternatives that offer people brief support for self-recovery is a sensible public health response to minimizing harms associated with gambling.
Internet-based treatment for mental health and substance use disorders is increasingly popular and is consistently found to be efficacious (Andersson and Carlbring 2017; Riper et al. 2014). However, only a limited amount of controlled research has been conducted with gambling disorder, despite the fact that individuals with gambling problems often report accessing information and support online (Castren et al. 2013; Rodda et al. 2018). Most recently, an Australian randomized controlled study (Casey et al. 2017) compared an internet-based cognitive behavioural treatment (CBT) program to an internet-based monitoring, feedback and support intervention, and a waitlist control. Both internet-based treatments were associated with better gambling severity outcomes than the 6-week waitlist, although the attrition rate was very high in both interventions (61%). Relative to the monitoring, feedback and support intervention, the CBT intervention had better outcomes on stress reduction and quality of life, and it was rated as more satisfactory. Outcomes were maintained over a 1-year follow-up.
An earlier controlled study from Sweden evaluated a web-based therapist-assisted CBT intervention compared with a waitlist control (Carlbring and Smit 2008). Three-month outcomes for participants receiving the treatment were superior to those on the waitlist. In a subsequent uncontrolled trial of the CBT intervention, early results were sustained over 3 years (Carlbring et al. 2012).
This Swedish intervention included the active involvement of a therapist. The issue of whether individuals benefit from brief contact with a professional, even if they are wanting to direct their own recoveries, is unresolved (Goslar et al. 2017). In our previous work, individuals who received a brief motivational interview by telephone and a mailed self-help workbook had better outcomes than individuals who received the workbook without the telephone contact. Similarly, a recent study of callers to a gambling helpline also showed that callers who only received telephone support had outcomes similar to those who also received a mailed workbook (Abbott et al. 2018). Although these results suggest that personal contact may be the most influential feature of the intervention, other studies across a variety of mental health disorders have not found a benefit of therapist support over entirely self-directed interventions (Campos et al. 2015; Labrie et al. 2012).
In another line of research, the effect of providing brief personalized normative feedback on reducing problematic gambling has also been examined in a small group of randomized controlled trials. In personalized normative feedback (PNF) interventions, an individual’s gambling behaviours and beliefs are compared with population norms to facilitate individual movement toward the norm. A meta analyses uncovered six randomized trials that generally found that these PNF interventions are associated with reduced gambling on at least some variables (Marchica and Derevensky 2016). However, the interventions were inconsistent in their effects and further research is necessary to explore the impact of PNF implementation on a wide-scale basis.
Two of these six PNF studies evaluated Check Your Gambling (CYG), a Canadian internet-based intervention that invites individuals to complete a self-assessment of gambling that leads to a personalized feedback report (Cunningham et al. 2012; Cunningham et al. 2009). In the first of these studies, CYG was associated with reduced spending on gambling at a 3-month follow-up when compared with a no intervention control group. The second study, which had a 6-month follow-up, included an additional condition, CYG excluding the normative feedback component, which was hypothesized to be less effective than the full CYG, but more effective than the no intervention control. In fact, results showed that CYG without the normative feedback was the most effective intervention. It was associated with less frequent gambling compared with the other groups.
More recently, Luquiens and colleagues conducted a randomized trial in the context of a commercial online poker site in France (Luquiens et al. 2016). Customers were invited to complete a brief screen for gambling problems and those who scored in the problem range were invited to participate in a study where they were randomly assigned to one of four groups: (a) an email report that provided PNF on their problem gambling screening score; (b) a downloadable cognitive behavioural workbook; (c) the workbook plus six sessions of email guidance by a therapist; or (d) a waitlist control. Follow-ups at 6 and 13 weeks were conducted when the problem gambling screening measure was re-administered. A major finding of the study was the large drop-up rate across all conditions, ranging from 83% in the waitlist to 97% in the guided workbook conditions. However, gambling expenditure data were available for all participants from the online gambling site. These data showed no overall group differences and few changes in gambling over time. Unfortunately, whether participants used the resources provided (e.g., downloaded the workbook, opened the email report) was not tracked. Moreover, the study incorporated a very minimal PNF intervention as it was limited to the problem gambling screening score and did not include any gambling behaviour variables. The Cunningham et al. (2012) study suggested that personalized feedback on gambling behaviour variables, but not necessarily normative feedback, was important (although the authors do stress that the lack of impact observed could be due to the way the norms were presented in this particular trial). These inconsistencies emphasize the need for further research to clarify the effectiveness of PNF interventions.
The current study extends the previous research in two ways. First, the self-help workbook provided to individuals by mail in previous evaluations (Hodgins et al. 2001, 2004a, 2009; Hodgins and Makarchuk 2002) was programmed to be an interactive online self-management program. It included a comprehensive set of self-management tools along with motivational goal setting exercises without the provision of therapist support (i.e., the extended intervention). Second, the study compared this relatively more comprehensive intervention to a briefer one. The comparison condition was Check Your Gambling (Cunningham et al. 2009), which also was entirely self-directed, but much briefer in style (i.e., the brief intervention).
The study hypotheses are outlined in the study protocol paper (Hodgins et al. 2013). The primary hypothesis was that individuals assigned to the extended intervention would show greater reductions in gambling over a 12-month follow-up than those assigned to the brief intervention. Two potential moderators were hypothesized: higher baseline self-efficacy (hypothesis 2) and no treatment-seeking history would be associated with better outcome (hypothesis 3). Additionally, two mediators were hypothesized: The level of engagement with resources among participants assigned to the extended intervention was hypothesized to mediate outcome (hypothesis 4), and increased self-efficacy was hypothesized to mediate outcome in both interventions (hypothesis 5).
Methods
Participants
Full details of the protocol are published elsewhere (Hodgins et al. 2013). Participants were recruited from across Canada using print and online media announcements asking for individuals who were concerned about their gambling and interested in web-based self-directed treatment. Those interested were assessed by telephone for eligibility. To be included in the study, participants must have (a) been at least 18 years of age; (b) perceived a gambling problem; (c) scored 3 or greater on the Problem Gambling Severity Index (PGSI; (Currie et al. 2013; Ferris and Wynne 2001); (d) gambled in the past month, (e) not currently involved in treatment or Gamblers Anonymous and; (f) had the ability to access an English-language website. Participants were also asked to provide the name and contact information for a family member or friend who could act as a corroborator of their gambling self-reports.
Procedure
A baseline assessment was completed by telephone after which participants were randomly assigned (50:50 allocation) to one of two conditions: brief or extended intervention. Randomization to conditions was stratified using a minimization algorithm, MINIM (Aiken 1982), based upon gender, problem gambling severity, and treatment history.
Follow-up assessments were conducted at 3, 6, and 12 months post randomization. Telephone interviews were conducted by research assistants who were blinded to the participant allocation. In the case that telephone contact was not made after repeated attempts, a link to an online assessment was provided to participants via email. Participants were also asked to provide the name of one or more individuals (e.g., family or friends) to act as a collateral who could confirm their self-reports of gambling. Collaterals were successfully interviewed for 53% of participants. Participants who did not identify a locatable collateral had lower lifetime problem gambling severity and shorter length of problem but did not differ on other characteristics. Consistent with previous findings (Hodgins et al. 2009), good agreement (Cicchetti 1994) between participants and collaterals for reports of days of gambling (Intraclass correlation coefficient = .73) and for fair agreement on dollars lost (Intraclass correlation coefficient = .44). The mean number of days and dollars reported did not differ between collaterals and participants, t(88) = 0.42, p = .67; t(88) = 0.87, p = .39.
Participants were provided $25 in Canadian currency in the form of a gift card for each follow-up assessment completed. Ethical approval for the study was provided by University of Calgary Conjoint Faculties Ethic Review Board.
Intervention Conditions
Brief: Check Your Gambling
In Check Your Gambling (CYG), participants were asked to complete a brief assessment in order to receive a personalized feedback report “to help give you a picture of your gambling and let you know how your gambling compared to other Canadians” (Hodgins et al. 2013). CYG provided normative feedback on gambling frequency and problem severity, and brief advice on how to reduce or stop gambling. This intervention has been previously evaluated (Cunningham et al. 2009, 2012) with small effects. It provides a credible comparison condition.
Extended: Self-Change Tools
The self-change tools (SCTs) extended intervention provided an online set of self-assessment activities and behavioural and cognitive strategies for reducing or quitting gambling (Hodgins et al. 2013). The content was drawn from self-directed written materials evaluated in previous research (Diskin and Hodgins 2009; Hodgins et al. 2001, 2004a, 2007, 2009; Hodgins and Makarchuk 2002).
Outcome Variables
Mean days of gambling per month and the NORC DSM-IV Screen for Gambling Problems (NODS) (Gerstein et al. 1999; Hodgins 2004) symptom total score (0–10) were the primary outcome variables. As outlined in the protocol paper, the sample size target (N = 180) was designed to detect a difference of about two gambling days per month and one NODS point between conditions at each follow-up. These are medium size effects, sufficiently large enough to have clinical relevance.
Mean dollars lost per gambling day, total dollars lost and self-rated improvement were secondary outcome variables. Days gambled and gambling expenditure were collected using the timeline follow-back interview method (Hodgins and Makarchuk 2003). The baseline scores summarized gambling for the 3 months pretreatment, and summary outcome scores were calculated for 3-, 6- and 12-months post baseline. Self-rated goal obtainment (did you meet your goal over the past 3 months?) was assessed by an ordinal scale (not at all, partially, mostly, or completely).
Measures
The Problem Gambling Severity Index (Ferris and Wynne 2001) was used to assess problem gambling severity for the past year at baseline and at the 12-month follow-up. The PGSI yields a total score (α = .81 in this sample) but also assesses problem gambling status (8 or greater) (Currie et al. 2013). DSM-IV pathological gambling was measured using the NORC DSM Screen for Gambling Problems (NODS; (Gerstein et al. 1999), lifetime and past 3-month versions (α = .83 in this sample) at baseline and the 3 month version at each follow-up. Self-efficacy was measured at these same times using the total score of Gambling Abstinence Self-efficacy Scale (Hodgins et al. 2004b) (α = .92 in this sample).
Statistical Analyses
All analyses were conducted using SPSS version 24, and PROCESS version 3.1. The intention-to-treat primary outcome hypotheses comparing outcome over time (i.e., days of gambling per month, NODS) for the two conditions were analyzed using linear mixed models with random intercepts, which included all available data per participant and restricted maximum likelihood to handle missing data. Separate models were conducted for each primary outcome variable, controlling for the baseline values of the outcome. The same analytic approach was used for the continuous secondary outcome variables (i.e., dollars lost, dollars per gambling day lost). The distribution for each variable was examined and transformations were undertaken when warranted. Model results were unchanged so results for untransformed data are presented. For the ordinal, self-rated goal obtainment variable, generalized estimation equation (GEE) modeling was conducted, including condition and time (i.e., 3, 6, and 12 months) as factors.
For hypotheses 2 and 3, the effect of moderators (i.e., baseline self-efficacy, treatment history) on the primary outcome variables were assessed by adding each as a fixed effect predictor in the linear mixed models. For hypothesis 4, the effect of use of the program resources was assessed by including a website engagement factor as a predictor in a linear mixed model analysis of participants assigned to the extended intervention. The website engagement factor reflected the number of the six Self-change Tools modules accessed (none, low = 1, medium = 2–4, high = 5–6). Finally, for hypothesis 5 (assessing change in self-efficacy as a mediator), a change score was calculated to reflect change in self-efficacy from baseline to 3 months. This mediator was entered into the PROCESS macro Model 4 (Hayes 2013) to obtain biased corrected 95% bootstrapped confidence intervals (CIs) of the indirect effect (5000 iterations) in separate models predicting days of gambling and NODS scores at 6 months.
Results
Participants
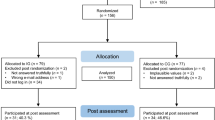
A total of 386 individuals were assessed for eligibility. Of these, 187 completed the baseline assessment and were randomized—92 to the brief condition and 95 to the extended condition. Figure 1 provides a CONSORT flow diagram that shows that the majority of those not randomized self-excluded from the study by not completing the baseline assessment. Figure 1 also reports the number of follow-up assessments completed for each condition at each time point. Missing data were primarily related to attrition. Overall, 158 (84%) of participants completed at least one follow-up assessment and 123 (66%) completed all three follow-up assessments, with no difference between conditions. A comparison of baseline characteristics (see Table 1 for variables compared) indicated that participants followed and non-followed differed on only three variables. Those followed were more likely to have some post-secondary education (p <.004), more likely to be Caucasian (p <.001) and less likely to be Aboriginal (p <.01). No differences in any gambling history variables were uncovered.

CONSORT flow diagram
Table 1 displays the baseline demographic and gambling variables by condition, showing that there were no statistically significant differences in these variables. The sample was 53% male with a mean age of 46.8 years (SD = 12.0). The majority were Caucasian (63%) and 16% were Aboriginal. About a third were married (30%) and 39% were single and never married. Most had some post-secondary education (89%) and over half were employed (56%).
Most participants met the DSM-IV criteria for Pathological Gambling (89%), and the PGSI cutoff for problem gambling (97%). The majority had made a previous attempt to reduce or quit gambling (83%) and 37% reported previous gambling treatment. The most frequent types of gambling were electronic gambling machines (60%) and casino table games (37%).
Primary Hypothesis
Table 2 provides the parameter estimates for the mixed linear regression models assessing the primary hypothesis. The results were consistent across the primary outcome variables, with significant time effects (improvement in days of gambling and problem severity from baseline to 3 months, maintained at 6 and 12 months). There were no differences between conditions. The same pattern was found for total dollars lost. For dollars lost per gambling day, there was a significant time effect but only the 12-month follow-up differed from the baseline value. Table 3 provides estimated mean values for these variables.
In terms of self-rated goal obtainment, the GEE analyses yielded a significant time effect (Wald χ2(2) = 10.1, p < .006), but no group main effect (p = .97) or group x time interaction (p = .26). Table 4 provides the goal obtainment by group and time. Parameter estimates indicated improved outcomes from 3 to 12 months, β = .39, SE = .15, Wald χ2(1) = 7.0, p < .008, but not from 3 to 6 months, β = .15, SE = .15, Wald χ2(1) = 0.9.
Hypotheses 2 and 3: Self-Efficacy and Treatment History as Moderators
Baseline self-efficacy (median split of baseline Gambling Abstinence Self-Efficacy Scale, GASS, total score) and previous treatment history (37%) were added as binary predictors to the linear mixed models to assess hypotheses 2 and 3, respectively. For self-efficacy and days of gambling, there was a main effect for self-efficacy in that individuals with higher self-efficacy gambled less overall, F(1, 182.2) = 7.8, p < .006. Counter to the hypothesis, there was no significant interaction with condition. There was, however, a significant interaction between self-efficacy and time, F(3, 460.7) = 2.6, p < .05. Table 5 provides the estimated means for this effect. Individuals with higher self-efficacy at baseline showed a steeper reduction in days of gambling but did not differ at 12 months from those with lower baseline self-efficacy.
For self-efficacy and NODS scores, there was a main effect for self-efficacy, such that individuals with higher self-efficacy had lower NODS scores (EM = 5.1, SE = 0.22) than those with lower self-efficacy (EM = 6.9, SE = .26), F(1, 191.2) = 29.1, p < .0001. Counter to the hypothesis, there was no significant interaction with condition or time.
For treatment history and days of gambling, there was no significant interaction with condition. There was, however, a significant interaction between treatment history and time, F(3, 458.4) = 3.1, p < .03. Table 5 provides the estimated means for this effect. Individuals with a history of treatment did not different at 3 and 6 months from those without a treatment history but at 12 months were gambling more.
For treatment history and NODs score, there was a main effect for treatment, such that individuals with past treatment had higher NODS scores (EM = 6.6, SE = 0.28) than those with no previous treatment (EM = 5.4, SE = .22), F(1, 189.5) = 10.9, p < .001. Counter to the hypothesis, there was no significant interaction with condition or time.
Hypothesis 4: Use of Website
Fifty-seven percent of participants accessed the assigned website over the course of the study, with no difference between conditions (59% brief, 55% extended). Of those assigned to the extended intervention, 31% had low engagement, 38% moderate engagement, and 31% high engagement. To examine the effect of accessing the website for participants assigned to the extended intervention (hypothesis 4), level of engagement (0–4) was added as a factor to the linear mixed model. For days of gambling, the hypothesized engagement × time interaction was not significant, but there was a main effect for engagement, F(3, 82.8) = 2.7, p < .05. The pattern of means indicated that the highly engaged participants gambled fewer days (EM = 12.2, SE = 2.4) than moderate, low, and non-engaged participants (EM = 18.9, 21.6, 18.8; SE = 2.1, 2.6, 1.6 respectively). For the NODS score, there was a significant engagement × time interaction, F(9, 218.8) = 2.3, p < .02. The estimated means are plotted in Fig. 2. Highly engaged participants showed a linear decrease in NODS scores over time. Post hoc tests indicated that non-engaged and moderately engaged participant showed a small initial decrease at 3-months and then stable scores. The low engagement participants showed a slower trajectory but by 12 months had similar mean scores to the highly engaged participants.

NODS scores over time by level of engagement with online tools
Hypothesis 5: Change in Self-Efficacy as a Mediator
The mean change in self-efficacy was 6.7 points (range − 57 to + 69). The PROCESS model indicated that intervention type was not differentially associated with GASS change, B = 5.14, SE = 4.25, t(123) = 1.2, p = .23. Change in self-efficacy, controlling for intervention condition, was not associated with days of gambling at 6 months, B = .04, SE = .09, t(123) = 0.47, p = .64, but was associated with NODS scores, B = .05, SE = .01, t(123) = 4.72, p < .0001. Evidence for mediation was not found. Neither bootstrapped indirect effect of intervention type on days of gambling nor NODS via change in self-efficacy was significant, B = .20, SE = .68, 95% CI [− 1.91, 0.99] and B = .22, SE = .21, 95% CI [− .15, .68].
Discussion
The study attracted a group of participants that resemble treatment-seeking populations in terms of demographics and severity of problem. Fully 37% of the sample had received previous treatment. Three months after their initial baseline assessment, participants reported significantly improved functioning, including fewer days of gambling, less gambling expenditure, and less problem gambling severity. Changes in expenditure per gambling day and goal obtainment were slower but were meaningfully improved by 12 months. By 12 months, participants reported meeting their goals at least partially (34.9%), mostly (18.5%) or completely (20.5%). In the absence of an appropriate control group it is unclear whether this change is associated with exposure to the interventions versus some sort of natural recovery process, reactivity to the research contacts and assessments, or statistical regression to the mean. A waiting list or attention control design was not included in this study for two reasons. First, previous research with a telephone workbook version of these materials had been shown to be superior to waitlist controls (Hodgins et al. 2001, 2004a, 2009). Second, the main major hypothesis was that the extended version of the intervention would yield better outcomes than the brief normative feedback intervention, a comparison that does not require an attentional non-active control. Nonetheless, inclusion of such a control condition would be informative.
Counter to the primary hypothesis, participants assigned to the brief versus extended self-directed options had similar outcomes across the primary and secondary outcome variables. Offering a more extended set of self-management tools did not improve outcomes. The two moderator hypotheses were partially supported. Participants with higher baseline self-efficacy showed a sharper decline in days of gambling than did those lower in self-efficacy. The difference at the 3-month follow-up was large (11 days of gambling). However, the two groups did not differ by the 12-month follow-up. This finding suggests that enhancing self-efficacy at the start of a change attempt may be helpful. Enhancement of self-efficacy is one goal of motivational interviewing, which has been successfully used with gambling addiction (Yakovenko et al. 2015). However, this study did not find support for self-efficacy as a mediator. It appears that changes in self-efficacy mirror changes in gambling but do not mediate them.
The second moderator hypothesis was that lack of previous treatment history would be associated with better outcomes. This hypothesis was based upon previous findings looking at predictors of outcome in brief treatments (Hodgins et al. 2009). The hypothesis was partially supported, with better outcomes found at 12-month follow-up only. Again, the effect was large with a difference of 9 days of gambling between those with and without a treatment history. This finding has implications for stepped care models, in which treatment history may prove to be a useful, easily assessed matching factor in determining optimal level of care (Hodgins and Schluter 2018).
It is interesting that the partial support for both these moderator hypotheses was limited to one of the primary outcome variables, days of gambling. It may be that the other outcome variable, problem gambling severity, is not as specific.
One important observation in this study, consistent with previous research, was the large proportion of participants who failed to visit their assigned website even once. Over 40% never followed the link provided, despite their stated intention to reduce or stop gambling. This finding argues for the benefit of some personal contact, including motivational enhancement, which was a component of the earlier version of the extended intervention. However, we had anticipated that offering a fully self-directed online intervention would be attractive to individuals reluctant to discuss their problems with another person. The private nature would reduce a potential barrier to access. Our design did not capitalize on this possibility very well as individuals needed to complete assessments by telephone with study personnel. This engagement likely improved follow-up rates, but also likely injected some confounding therapeutic benefit. The extended intervention was publicly available during this trial. The demographics of those users were similar except that they appeared to be younger on average, and younger than the typical treatment seeking population. The public site also attracted more participants during the recruitment phase although comparisons are difficult because of different advertising strategies.
The brief CYG intervention is designed to be completed in one visit, but the extended intervention provides a set of modules. Engagement in these modules was variable with equal numbers of participants showing low, moderate and high engagement. Our hypothesis that engagement would mediate outcome was supported for problem gambling severity. The highly engaged individuals had the best outcomes. Of interest, however, is that the low engaged individuals (i.e., those who visited 1 or 2 modules) showed a slower trajectory but ultimately had 12-month outcomes similar to those who were highly engaged. More examination of the impact of the use of online resources is important. Use of the resources on the public version of this site were similarly variable.
This study has a number of strengths, including sufficient statistical power, and a good follow-up rate. As with all studies of gambling behaviour, the primary outcomes are based upon self-report data, which is imperfect. However, these data were carefully collected and collaterals were used to promote accuracy and to assess validity. Nonetheless, the data contain some unknown amount of unreliability.
Future research needs to explore the attractiveness, uptake, and effectiveness of online interventions with and without therapist support. It is important that attention be paid to self-change processes that may be initiated by simple enrollment in trials, and to assess change associated with use of various intervention features. As in other areas of mental health and addictions, online interventions show promise although there is much to be learned about how they work with whom and why.
References
Abbott, M., Hodgins, D. C., Bellringer, M., Vandal, A. C., Palmer Du Preez, K., Landon, J., et al. (2018). Brief telephone interventions for problem gambling: A randomized controlled trial. Addiction, 113(5), 883–895. https://doi.org/10.1111/add.14149.
Aiken, M. (1982). A program for balancing the allocation of subjects to treatment in a clinical trial. Computers in Biomedical Research, 15(5), 519–524.
Andersson, G., & Carlbring, P. (2017). Internet-assisted cognitive behavioral therapy. Psychiatric Clinics of North America, 40(4), 689–700. https://doi.org/10.1016/j.psc.2017.08.004.
Boudreault, C., Giroux, I., Jacques, C., Goulet, A., Simoneau, H., & Ladouceur, R. (2018). Efficacy of a self-help treatment for at-risk and pathological gamblers. Journal of Gambling Studies, 34(2), 561–580. https://doi.org/10.1007/s10899-017-9717-z.
Campos, M. D., Rosenthal, R. J., Chen, Q., Moghaddam, J., & Fong, T. W. (2015). A self-help manual for problem gamblers: The impact of minimal therapist guidance on outcome. International Journal of Mental Health and Addiction, 14(4), 579–596. https://doi.org/10.1007/s11469-015-9579-5.
Carlbring, P., Degerman, N., Jonsson, J., & Andersson, G. (2012). Internet-based treatment of pathological gambling with a three-year follow-up. Cognitive Behaviour Therapy, 41(4), 321–334. https://doi.org/10.1080/16506073.2012.689323.
Carlbring, P., & Smit, F. (2008). Randomized trial of internet-delivered self-help with telephone support for pathological gamblers. Journal of Consulting and Clinical Psychology, 76(6), 1090–1094. https://doi.org/10.1037/a0013603.
Casey, L. M., Oei, T. P. S., Raylu, N., Horrigan, K., Day, J., Ireland, M., et al. (2017). Internet-based delivery of cognitive behaviour therapy compared to monitoring, feedback and support for problem gambling: A randomised controlled trial. Journal of Gambling Studies, 33(3), 993–1010. https://doi.org/10.1007/s10899-016-9666-y.
Castren, S., Pankakoski, M., Tamminen, M., Lipsanen, J., Ladouceur, R., & Lahti, T. (2013). Internet-based CBT intervention for gamblers in Finland: Experiences from the field. Scandinavian Journal of Psychology, 54(3), 230–235.
Cicchetti, D. V. (1994). Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychological Assessment, 6(4), 284–290. https://doi.org/10.1037/1040-3590.6.4.284.
Cunningham, J. A. (2005). Little use of treatment among problem gamblers. Psychiatric Services, 56(8), 1024–1025. https://doi.org/10.1176/appi.ps.56.8.1024.
Cunningham, J. A., Hodgins, D. C., Toneatto, T., & Murphy, M. (2012). A randomized controlled trial of a personalized feedback intervention for problem gamblers. PLoS ONE, 7(2), e31586. https://doi.org/10.1371/journal.pone.0031586.
Cunningham, J. A., Hodgins, D. C., Toneatto, T., Rai, A., & Cordingley, J. (2009). Pilot study of a personalized feedback intervention for problem gamblers. Behavior Therapy, 40(3), 219–224. https://doi.org/10.1016/j.beth.2008.06.005.
Currie, S. R., Hodgins, D. C., & Casey, D. M. (2013). Validity of the Problem Gambling Severity Index interpretive categories. Journal of Gambling Studies, 29(2), 311–327. https://doi.org/10.1007/s10899-012-9300-6.
Diskin, K. M., & Hodgins, D. C. (2009). A randomized controlled trial of a single session motivational intervention for concerned gamblers. Behaviour Research and Therapy, 47(5), 382–388. https://doi.org/10.1016/j.brat.2009.01.018.
Ferris, J., & Wynne, H. (2001). The Canadian Problem Gambling Index: Final report. Ottawa: Canadian Centre on Substance Abuse.
Gerstein, D. R. M. S., Toce, M., Hoffman, J., Palmer, A., & Johnston, R. (1999). Gambling impact and behavior study. Report of the National Gambling Impact Study Commission. Chicago: National Opinion Research Center.
Goslar, M., Leibetseder, M., Muench, H. M., Hofmann, S. G., & Laireiter, A. R. (2017). Efficacy of face-to-face versus self-guided treatments for disordered gambling: A meta-analysis. Journal of Behavioral Addictions, 6(2), 142–162. https://doi.org/10.1556/2006.6.2017.034.
Hayes, A. F. (2013). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. New York: Guilford.
Hodgins, D. C. (2004). Using the NORC DSM Screen for Gambling Problems as an outcome measure for pathological gambling: psychometric evaluation. Addictive Behaviors, 29(8), 1685–1690. https://doi.org/10.1016/j.addbeh.2004.03.017.
Hodgins, D. C., Currie, S. R., Currie, G., & Fick, G. H. (2009). Randomized trial of brief motivational treatments for pathological gamblers: More is not necessarily better. Journal of Consulting and Clinical Psychology, 77(5), 950–960. https://doi.org/10.1037/a0016318.
Hodgins, D. C., Currie, S. R., & el-Guebaly, N. (2001). Motivational enhancement and self-help treatments for problem gambling. Journal of Consulting and Clinical Psychology, 69(1), 50–57.
Hodgins, D. C., Currie, S. R., el-Guebaly, N., & Diskin, K. M. (2007). Does providing extended relapse prevention bibliotherapy to problem gamblers improve outcome? Journal of Gambling Studies, 23(1), 41–54. https://doi.org/10.1007/s10899-006-9045-1.
Hodgins, D. C., Currie, S. R., el-Guebaly, N., & Peden, N. (2004a). Brief motivational treatment for problem gambling: a 24-month follow-up. Psychology of Addictive Behaviors, 18(3), 293–296. https://doi.org/10.1037/0893-164x.18.3.293.
Hodgins, D. C., Fick, G. H., Murray, R., & Cunningham, J. A. (2013). Internet-based interventions for disordered gamblers: Study protocol for a randomized controlled trial of online self-directed cognitive-behavioural motivational therapy. BMC Public Health, 13, 10. https://doi.org/10.1186/1471-2458-13-10.
Hodgins, D. C., & Makarchuk, K. (2002). Becoming a winner: Defeating problem gambling. Calgary: University of Calgary.
Hodgins, D. C., & Makarchuk, K. (2003). Trusting problem gamblers: Reliability and validity of self-reported gambling behavior. Psychology of Addictive Behaviors, 17(3), 244–248. https://doi.org/10.1037/0893-164x.17.3.244.
Hodgins, D. C., Peden, N., & Makarchuk, K. (2004b). Self-efficacy in pathological gambling treatment outcome: Development of a gambling abstinence self-efficacy scale (GASS). International Gambling Studies, 4(2), 99–108. https://doi.org/10.1080/14459790412331296947.
Hodgins, D. C., & Schluter, M. (2018). The role of treatment in reducing gambling-related harm. In H. Bowden-Jones, C. Dickson, C. Dunand, & O. Simon (Eds.), Problem gambling: Harm-reduction as a public health approach. London: Taylor and Francis.
Labrie, R. A., Peller, A. J., Laplante, D. A., Bernhard, B., Harper, A., Schrier, T., et al. (2012). A brief self-help toolkit intervention for gambling problems: A randomized multisite trial. American Journal of Orthopsychiatry, 82(2), 278–289. https://doi.org/10.1111/j.1939-0025.2012.01157.x.
Luquiens, A., Tanguy, M. L., Lagadec, M., Benyamina, A., Aubin, H. J., & Reynaud, M. (2016). The efficacy of three modalities of Internet-based psychotherapy for non-treatment-seeking online problem gamblers: A randomized controlled trial. Journal of Medical Internet Research, 18(2), e36. https://doi.org/10.2196/jmir.4752.
Marchica, L., & Derevensky, J. L. (2016). Examining personalized feedback interventions for gambling disorders: A systematic review. Journal of Behavioral Addictions, 5(1), 1–10. https://doi.org/10.1556/2006.5.2016.006.
Oei, T. P. S., Raylu, N., & Lai, W. W. (2018). Effectiveness of a self help cognitive behavioural treatment program for problem gamblers: A randomised controlled trial. Journal of Gambling Studies, 34(2), 581–595. https://doi.org/10.1007/s10899-017-9723-1.
Petry, N. M., Ginley, M. K., & Rash, C. J. (2017). A systematic review of treatments for problem gambling. Psychology of Addictive Behaviors, 31(8), 951–961. https://doi.org/10.1037/adb0000290.
Petry, N. M., Weinstock, J., Ledgerwood, D. M., & Morasco, B. (2008). A randomized trial of brief interventions for problem and pathological gamblers. Journal of Consulting and Clinical Psychology, 76(2), 318–328. https://doi.org/10.1037/0022-006x.76.2.318.
Riper, H., Blankers, M., Hadiwijaya, H., Cunningham, J., Clarke, S., Wiers, R., et al. (2014). Effectiveness of guided and unguided low-intensity internet interventions for adult alcohol misuse: A meta-analysis. PLoS ONE, 9(6), e99912. https://doi.org/10.1371/journal.pone.0099912.
Rodda, S., Merkouris, S., Abraham, C., Hodgins, D. C., Cowlishaw, S., & Dowling, N. (2018). Therapist-delivered and self-help interventions for gambling problems: A review of contents. Journal of Behavioural Addictions, 7(2), 1–16. https://doi.org/10.1556/2006.7.2018.44.
Swan, J. L., & Hodgins, D. C. (2015). Brief interventions for disordered gambling. Canadian Journal of Addiction, 6(2), 29–36.
Yakovenko, I., & Hodgins, D. C. (2016). Latest developments in treatment for disordered gambling: Review and critical evaluation of outcome studies. Current Addiction Reports, 3(3), 299–306.
Yakovenko, I., Quigley, L., Hemmelgarn, B. R., Hodgins, D. C., & Ronksley, P. (2015). The efficacy of motivational interviewing for disordered gambling: systematic review and meta-analysis. Addictive Behaviors, 43, 72–82. https://doi.org/10.1016/j.addbeh.2014.12.011.
Funding
This study was funded by Canadian Institute of Health Research (project grant).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hodgins, D.C., Cunningham, J.A., Murray, R. et al. Online Self-Directed Interventions for Gambling Disorder: Randomized Controlled Trial. J Gambl Stud 35, 635–651 (2019). https://doi.org/10.1007/s10899-019-09830-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10899-019-09830-7