
Abstract
Available evidence suggests that self-help treatments may reduce problem gambling severity but inconsistencies of results across clinical trials leave the extent of their benefits unclear. Moreover, no self-help treatment has yet been validated within a French Canadian setting. The current study therefore assesses the efficacy of a French language self-help treatment including three motivational telephone interviews spread over an 11-week period and a cognitive-behavioral self-help workbook. At-risk and pathological gamblers were randomly assigned to the treatment group (n = 31) or the waiting list (n = 31). Relative to the waiting list, the treatment group showed a statistically significant reduction in the number of DSM-5 gambling disorder criteria met, gambling habits, and gambling consequences at Week 11. Perceived self-efficacy and life satisfaction also significantly improved after 11 weeks for the treatment group, but not for the waiting list group. At Week 11, 13% of participants had dropped out of the study. All significant changes reported for the treatment group were maintained throughout 1, 6 and 12-month follow-ups. Results support the efficacy of the self-help treatment to reduce problem gambling severity, gambling behaviour and to improve overall functioning among a sample of French Canadian problem gamblers over short, medium and long term. Findings from this study lend support to the appropriateness of self-help treatments for problem gamblers and help clarify inconsistencies found in the literature. The low dropout rate is discussed with respect to the advantages of the self-help format. Clinical and methodological implications of the results are put forth.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gambling disorder is characterised by persistent and maladaptive gambling behavior that impairs one’s functioning and causes significant psychological distress (American Psychiatric Association [APA] 2013). Depending on the evolution and severity, one’s gambling behaviour can be considered either below the diagnostic threshold (at-risk gambling) or above (pathological gambling or gambling disorder). At-risk gamblers nevertheless experience negative consequences from their gambling, but that do not reach a clinical intensity. Problem gambling can be used to refer to both at-risk and pathological gambling, although there is no consensus regarding the use of this label (Cowlishaw et al. 2014). Williams et al. (2012) report international standardised problem gambling prevalence rates ranging between 0.5 and 7.6% across countries, with a mean rate of 2.3%.
Few problem gamblers seek help. Canadian and American population surveys suggest that between 6 and 29% of adults identified as problem gamblers have used professional help or a support group (Slutske 2006; Suurvali et al. 2008; Volberg et al. 2006). Among problem gamblers who enter treatment, the median dropout rate reaches 26% (Giroux et al. 2015).
Different authors have put forward the use of self-help treatments as part of the solution to overcome the issues of low help-seeking and high dropout rates among problem gamblers (Gainsbury et al. 2014; Pulford et al. 2010; Pulford et al. 2009). Suurvali et al. (2008) noted that when considering informal help such as books and online material, help-seeking rates increased to 30% for at-risk gamblers and to 50% for pathological gamblers. Problem gamblers also expressed interest toward informal treatments which allow confidentiality, flexibility and are self-directed (Cunningham et al. 2008; Faucher-Gravel 2016; Raylu et al. 2008).
Studies that have assessed efficacy of various self-help treatments underline the ability of this type of intervention to decrease problem gambling severity (e.g. Carlbring and Smit 2008; Carlbring et al. 2012; Castren et al. 2013; Diskin and Hodgins 2009; Hodgins et al. 2001, 2004a, 2009; Ladouceur et al. 2015; Petry et al. 2016). However, in their literature review of self-help treatments for problem gambling, Swan and Hodgins (2015) pointed out that studies on these interventions are still scarce and that inconsistencies remain regarding the treatment evaluation methods and the extent of their benefits.
For example, Hodgins et al. (2001) compared two brief treatments (workbook only or combined with one motivational telephone interview) to a waiting list with 102 problem gamblers and noticed, after one month, a significant decrease of gambling habits in the three conditions. Participants receiving the combined treatment showed significantly greater improvement than the waiting list group. Hodgins et al. (2009) further investigated the impact of adding brief telephone support calls to a workbook on problem gambling with a sample of 314 at-risk and pathological gamblers. Again, 59% of gamblers from the control group (n = 65) reported having decreased by half their gambling expenses during the six-week waiting period. A longer waiting period could help determine if improvements of the control group tend to fade or reflect an enduring change.
Self-help treatments usually contain motivational telephone interviews (MI), since such interviews have shown to be more effective to reduce gambling behavior over the short term than interviews without a motivational component (Yakovenko et al. 2015). Nevertheless, the optimal number of MIs to include within self-help treatments has yet to be determined (Rash and Petry 2014). After 12 months, Hodgins et al. (2009) found a similar decrease in problem gambling severity in gamblers allocated to the “MI + brief support calls + workbook” condition than in the “MI + workbook” and workbook only conditions. One study with no control group by Ladouceur et al. (2015) indicated that two MIs with a cognitive-behavioral workbook significantly lowered problem gambling severity and time spent gambling among the 32 problem gamblers who completed the treatment. However, decrease in gambling expenditure was not maintained throughout the six-month follow-up period and the 32% dropout rate (Ladouceur et al. 2015) far exceeded the 4% (Hodgins et al. 2001) and 9% (Hodgins et al. 2009) rates from other studies. An additional MI could help maintain improvements and facilitate treatment retention.
Among their set of recommendations on the reporting of gambling treatment efficacy studies, Walker et al. (2006) suggested that changes on life dimensions impaired by problem gambling be also reported. To date, studies assessing self-help treatments have considered only a limited number of outcome variables, such as gambling behavior (e.g. Hodgins et al. 2001) and the score on a diagnostic or screening instrument (e.g. Campos et al. 2015). Moreover, clinical trials on self-help treatments have been conducted in different locations, but no treatment has yet been validated within a French Canadian setting. Therefore, given the positive outcomes associated with self-help treatments, the validation of a self-help treatment program elaborated in French appears highly relevant.
In line with previous work on self-help treatments for problem gambling, this study aims to assess the efficacy of a self-help treatment elaborated in French for French Canadian at-risk and pathological gamblers. The study will also help to further clarify the impact of this type of treatment on gambling habits and other key variables: self-efficacy, life satisfaction and negatives consequences of gambling.
Objective and Hypotheses
This study aimed to assess the efficacy of an enhanced version of a self-help treatment for problem gamblers developed in French by Ladouceur et al. (2015) entitled “JEu me questionne”, comprised of three MIs and a cognitive-behavioral workbook, in contrast with a waiting list control group after an 11-week period. The three following hypotheses were put forth:
-
1.
After 11 weeks, compared with the control group, the treatment group will show a significant decrease in the number of DSM-5 gambling disorder criteria, gambling frequency, time and money spent gambling and a significant increase in self-efficacy (primary outcome variables).
-
2.
After 11 weeks, compared with the control group, the treatment group will show a significant increase in life satisfaction and a significant decrease in negative consequences of gambling (secondary outcome variables).
-
3.
Improvements of the treatment group at Week 11 will be maintained throughout 1-, 6- and 12-month follow-ups, which will translate in an absence of significant deterioration in outcome variables between Week 11 and the follow-ups.
Method
Protocol
The study was conducted as a randomized controlled trial including one group receiving the self-help program (treatment group) and one waiting list group (control group). As opposed to previous studies that have compared a self-help treatment to a control group after 4 (Hodgins et al. 2001) to 8 weeks (Carlbring and Smit 2008), an 11-week comparison period was preferred to help clarify the impact of the treatment.
The minimization method (Pocock and Simon 1975), which aims to reduce between-group differences on predetermined variables, was used to allocate participants to the trial conditions based on gender and the number of DSM-IV-TR (APA 2000)Footnote 1 pathological gambling criteria met with the MinimPy software (Saghaei and Saghei 2011). Differences have indeed been reported between men and women in terms of gambling behavior, gambling consequences and comorbidity rates (Crisp et al. 2004; Ledgerwood et al. 2012; Petry et al. 2005). As for problem gambling severity, it is known to partially predict posttreatment outcome (Crisp et al. 2001; Dowling 2009). Minimization is considered more effective than randomization to produce balanced groups when samples sizes are small (Scott et al. 2002).
Participants
Recruitment took place in the province of Quebec (Canada), from June 2013 to December 2014. Advertisements were placed in mass-circulation daily newspapers, on Facebook, across community-based organizations, the members of a provincial association on addiction treatment and of Quebec Order of Psychologists and on the Loto-Quebec website. Participants from previous or ongoing studies conducted at the research centre and who had consented to be informed about other studies were also offered the treatment.
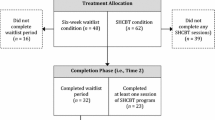
Inclusion criteria were: 18 years and older, having a minimal score of 2 on the Problem Gambling Severity Index (PGSI; Ferris and Wynne 2001), wanting to cut down on gambling, willing to complete a French treatment workbook, and agreeing to the possibility of being allocated to a control group. Individuals expressing suicidal intent or already involved in a gambling treatment were excluded. Because the self-help program was elaborated for both at-risk and pathological gamblers, a PGSI inclusion criterion of 2 was chosen to encourage treatment access to any gambler who wished to receive help. In total, 138 people took part in a screening telephone interview to assess for their eligibility and 62 people were recruited and allocated to the treatment group (n = 31) and the control group (n = 31). Figure 1 presents a flowchart of participants through each step of the study protocol.

Flow of participants through study protocol
Procedure
A screening telephone interview was conducted with interested individuals and eligible participants then provided verbal consent to the study and to the audio recording of phone calls. Non-eligible individuals were given a helpline number and a list of help resources. Within the following days, eligible participants completed an initial assessment over the phone and were allocated to the trial groups. The treatment group then completed a first MI and the workbook and consent form were mailed. Participants were encouraged to complete the workbook at their own pace. Two other MIs were conducted at the third and eighth week following mailing of the workbook. MIs lasted between 20 and 45 min. The control group was informed of the waiting delay during a phone call after the initial assessment and the consent form was mailed. Two other 10 min phone calls were conducted using the same time frame as the MIs. Both groups completed an assessment 11 weeks later. The control group was then given the program and the treatment group completed 1-, 6- and 12-month follow-up telephone assessments. Compensations in the form of gift vouchers were given after each assessment, ranging from 10$ for the first one to 50$ for the last. This study was approved by the sectorial research ethics committee of Université Laval, the Comité en psychologie et en sciences de l’éducation (# 2012-079/Phase I A-2/29-11-2013).
Material
Screening
Sociodemographic Data
A 12 multiple-choice items questionnaire was used to assess for eligibility and to document gender, origin, age, marital status, number of children, education level, employment and income.
Problem Gambling Severity Index (PGSI; Ferris and Wynne 2001)
This problem gambling screening measure was taken from the Canadian Problem Gambling Index and divides gamblers into five categories: non-gamblers and non-problem gamblers (score of 0), low-risk (1 and 2), moderate-risk (3–7), and problem (8 and more). The PGSI shows a good internal consistency (Cronbach’s alpha = 0.84) and a criterion validity similar to that of the DSM-IV (APA 1994).
Initial Assessment, Week 11 Assessment, and 1-, 6- and 12-Month Follow-Ups
Pathological Gambling Diagnostic Interview (PGDI), DSM-5 Version (CQEPTJ 2013)
The PGDI is comprised of 50 questions and was used to evaluate DSM-5 gambling disorder (APA 2013; four criteria met or more indicate a gambling disorder) and the negative consequences of gambling over nine areas of functioning (social, marital and family life, work, mood, sleep, physical health, finances and quality of life). For each consequence, participants answered on a Likert-type scale ranging from 0 (not at all/no problem) to 5 (enormous/severe problems). The PGDI also collected motives for seeking help, treatment goal, alcohol and drug use while gambling and other addictions. A shorter version was used for the Week 11 assessment and the follow-ups, in which DSM-5 gambling disorder criteria were evaluated with a modified time frame to specifically cover the time period between the assessments.
Gambling-Related Items
Three open-ended questions evaluated gambling frequency, time and money spent gambling during the month preceding assessments.
Self-Efficacy Questionnaire
This questionnaire was used to identify high-risk gambling situations. For each situation identified by the participants, they were asked using the same question to evaluate their level of confidence in their ability to control their gambling on a scale from 0 (not at all) to 10 (totally). The psychometric properties of this instrument have not been validated. Self-efficacy was re-evaluted at each assessment using the same high-risk situations identified in the initial assessment.
Life Satisfaction Questionnaire (Simoneau et al. 2004)
This questionnaire was used to measure life satisfaction regarding 14 aspects: health, physical fitness, sleep, level of energy, social activities, family relationships, marital relationships, studies or employment, finances, psychological well-being, physical appearance, self-esteem, sexual relations and overall pleasure in life. For each item, the participant answered on a scale from one (very unsatisfied) to 5 (very satisfied). Psychometric properties of this instrument have not been documented.
Treatment Evaluation and Workbook Adherence Questionnaire
This questionnaire was used to assess treatment goal (abstinence or controlled gambling), if goal was reached, and workbook completion. Seven Likert-type questions ranging from one (very low satisfaction) to 5 (very high satisfaction) evaluated participants’ satisfaction with the treatment components and six open-ended questions gathered their comments.
Other Measures
French version of the Beck Anxiety Inventory (BAI; Beck et al. 1988), Beck Depression Inventory (BDI-II; Beck et al. 1996) and Short Alcohol Dependence Data Questionnaire (SADDQ; Tremblay et al. 2001) were used at each assessment to evaluate participants’ anxiety, depression and alcohol use. However, these data were not considered as outcome variables in the statistical analyses regarding the efficacy of the treatment, because they were not directly targeted by the intervention.
Material Specific to the Study Conditions
Control Interview Guide
An interview guide was developed to assist the therapists during the phone calls made with participants in the control group. The guide recommended to confirm with the participant the waiting delay and to give further information on this procedure, if required. Applying this interview guide, the therapist was allowed to discuss gambling habits with the participants, but had to remain neutral and not use any motivational interviewing techniques. The guide also specified to assess for any psychological distress in the participants.
Motivational-Type Interview Guide
These interview guides were all similar in form, except the first one that included a short feedback on the gambler’s initial assessment. Following these guides, the therapist elicited change talk in the gambler by tackling motivations and advantages to modify gambling behavior. The importance to cut down or stop gambling and confidence in achieving this goal were then assessed and strengthened. The guides specified to reinforce progress. If required, the interview guide planned to discuss and to help solve obstacles met during treatment. The gambler was also invited to set realistic goals to achieve between interviews.
“JEu me questionne” Treatment Workbook (JMQ; CQEPTJ 2012)
An updated version of the JMQ workbook developed by Ladouceur et al. (2015) was used for the study. Modifications were brought to the workbook based on the comments gathered in the study of Ladouceur et al. (2015). The version used for the purpose of this study included, for instance, additional informative readings as well as accounts of former participants’ experience with the program. The 145 pages workbook is written in French and is divided in five chapters. The first section emphasizes the gambler’s motivation and benefits to change and the second section helps the gambler identify high-risk gambling situations and strategies to address them. The third phase focuses on the setting of a treatment goal (abstinence or controlled gambling) and provides information about gambling traps. The fourth phase aims to identify gambling-related thoughts and to understand their contribution in the maintenance of problem gambling behavior. The last chapter focuses on cognitive restructuring and relapse-prevention. Additional readings and tools on relaxation techniques and problem solving are presented in the appendices. Each workbook chapter provides worksheets to record gambling habits.
Therapists
Screenings, assessments, MIs and control interviews were all conducted by psychology doctoral-level students under the supervision of a clinical psychologist. Forty-five participants were assigned a team of two therapists, one who conducted the assessments and the other the treatment or control interviews, whereas 17 participants were assigned one therapist who completed these two tasks, due to scheduling problems. To test for an impact of this protocol modification on the results, repeated measures analyses of variance based on a mixed linear model were conducted for the number of DSM-5 gambling disorder criteria (APA 2013) and monthly gambling habits, including an effect for the number of therapists assigned to the participants. No significant main interaction effect was found for the number of therapists, F(1, 54) = 0.47, p = 0.50, nor for the interaction between time, group and the number of therapists, F(1, 51) = 0.21, p = 0.65.
Integrity of Interviews
Two independent raters who did not act as therapists in the study assessed the integrity of MIs and control interviews. Thirty-four recordings (17 control interviews, 17 MIs), making for 25% of available recordings, were randomly selected. A scoring grid was elaborated for the purpose of this study in order to evaluate each recording on two criteria: the importance of change and confidence in one’s ability to change. The proper application of the study protocol implied that control group interviews would meet none of the criteria whereas the MIs would meet one or two criteria, as specified by the Motivational-type interview guides. An interrater agreement was made on all scores. Two disagreements were found and discussed until a consensus was reached. Overall, 100% of control interviews met no criteria and 100% of MIs met both criteria.
Analyses
Analyses were conducted with SPSS (version 22) and SAS (version 9.4) softwares. Descriptive statistics of the sample were first computed. Content of open-ended questions was coded into main themes. Research hypotheses were tested using repeated measures analyses of variance based on the linear mixed model. All participants were included in the analyses, even those who did not complete the Week 11 assessment or the follow-ups. The linear mixed model has a low sensitivity to randomly missing data and allows to use all available information for each participant (Gueorguieva and Krystal 2004). Since missing data in this study are due to treatment dropout and to the non-applicability of some items to all participants (e.g. consequences of gambling on marital relationship for a single person), missing data were most likely missing at random rather than missing completely at random (Dziura et al. 2013). For each analysis, the compound symmetry and unstructured covariance structures were considered. Akaike information criterion was used to select the best-fitting model. When examination of Student residuals suggested a violation of the homogeneity of variances or normality, a heterogeneous variance term was added to the model or variable transformations were carried out.
To test for treatment efficacy, a series of analyses was conducted considering main effects of group (treatment and control), of time (initial and Week 11 assessments) and a time × group interaction, with p value of 0.05. A posteriori contrasts with a Bonferroni adjusted p value (0.05/2 = 0.025) examined differences when significant interaction effects were found. A second set of analyses was conducted to test for differences between Week 11 and follow-ups (Month 1, 6 and 12) on outcome variables for the treatment group. In case of a significant time effect, a posteriori contrasts were planned with a Bonferroni adjusted p value (p = 0.05/3 = 0.017).
Scores generated by linear mixed model analyses correspond to least square means (LSM) and standard errors (SE). These mean scores were based on raw means for each time and group combination, and were estimated considering an uneven number of individuals due to attrition and correlations between measurement times. Therefore, LSMs computed for Week 11 by the second set of analyses slightly differ as they also take into account correlations with follow-up measures. For the self-efficacy outcome variable, a random effect of the participant was added to the analysis models to take into account the specific high-risk situations for each participant that were re-evaluted across measurement times. Instead of using total scores, items measuring life satisfaction and negatives consequences of gambling were analysed separately with p value of 0.01 for main effects and Bonferroni adjustments for a posteriori contrasts. This analysis strategy was chosen in order to identify which specific life areas would change following participation in the treatment. It should be noted that analyses derived from linear mixed models do not produce sum of squares and therefore do not allow to calculate effect sizes and their estimation based on other parameters could be imprecise (Bakeman 2005).
To define clinical change, the continuous variable of DSM-5 gambling disorder criteria was dichotomized to classify gamblers as sub-clinical (less than four criteria met) or pathological (four criteria met and more). A repeated measures logistic regression model was computed to determine if there was a significant change in the probability of being classified as pathological gambler at Week 11, looking at time, group and time × group effects.
Results
Sample Description and Retention in the Study Protocol
Table 1 presents sociodemographic variables for both groups. Student t test, Chi square and Mann–Whitney U tests were used to examine between-group differences at the initial assessment and revealed no significant differences on these measures. As for dropout from the study protocol, 13% of the treatment group (n = 4) and the control group (n = 4) did not complete the Week 11 assessment. A logistic regression model was used to try to predict dropout from the study at Week 11, for which ten variables measured at the initial assessment were selected (marital status, age, duration of problem gambling, prior help for gambling, number of pathological gambling diagnostic criteria, SADDQ, BAI and BDI scores, frequency and time spent gambling). At alpha level of 0.05, none of the variables included in the model were significantly associated with the probability of dropping out from the study protocol before Week 11, p = 0.09–0.97. The model had a good predictive ability (area under the ROC curve, c = 0.821). The participation rate of the treatment group reached 80% at Month 1 and 6 (n = 25) and 74.2% at Month 12 (n = 23).
Impact of the Self-Help Treatment on Problem Gambling Severity, Monthly Gambling Habits and Self-Efficacy
Table 2 shows LSMs and SE of primary and secondary outcome variables according to the group and measurement time.
Number of DSM-5 Footnote 2 Gambling Disorder Criteria (APA 2013 )
The time × group interaction effect was significant, F(1, 54) = 16.03, p < 0.001, and indicated a significant reduction in diagnostic criteria between the initial assessment and Week 11 for the treatment group, F(1, 54) = 48.72, p < 0.001. No significant differences were found for the control group between the two assessments, F(1, 96) = 0.73, p = 0.39. Mean number of gambling disorder criteria met by the treatment group remained similar between Week 11 and 1-, 6- and 12-month follow-ups, F(71) = 2.52, p = 0.07.
The treatment group presented a significantly lower probability of meeting gambling disorder diagnostic criteria at Week 11, F(1, 58) = 16.59, p < 0.001, with a proportion of pathological gamblers dropping from 87.1 to 29.63%. For the control group, the probability of meeting gambling disorder criteria at Week 11 did not change significantly, F(1, 56) = 2.18, p = 0.15, with a proportion of pathological gamblers of 77.42% at the initial assessment and of 59.26% at Week 11.
Monthly Gambling Habits
Time × group effects were significant for gambling frequency, F(1, 51) = 10.70, p = 0.002, time spent gambling, F(1, 52) = 10.16, p = 0.002, and gambling expenditure, F(1, 52) = 8.30, p = 0.006, thus indicating a significant reduction in monthly gambling habits for the treatment group at Week 11. Treatment group gambled significantly less often after 11 weeks of involvement in the treatment, F(1, 28) = 35.12, p < 0.001, and gambling frequency remained similar through Month 1, 6 and 12, F(22) = 1.70, p = 0.20. No significant change in gambling frequency was found for the control group, F(1, 26) = 0.27, p = 0.61.
Hours spent gambling monthly significantly decreased for the treatment group after participating in the treatment, F(1, 28) = 33.23, p < 0.001, whereas no significant change was found for the control group, F(1, 25) = 4.51, p = 0.04. Time spent gambling by the treatment group stayed similar between Week 11 and follow-ups, F(72) = 1.59, p = 0.20.
Treatment group spent significantly less money gambling at Week 11, F(1, 52) = 37.09, p < 0.001, and mean gambling expenditure remained similar through all follow-ups, F(71) = 0.99, p = 0.40. No significant change in gambling expenditure was found for the control group between the initial assessment and Week 11, F(1, 52) = 4.07, p = 0.05.
Self-Efficacy
A significant time × group effect was found, F(1, 122) = 6,79, p = 0.01, reflecting a significant improvement in self-efficacy for the treatment group 11 weeks after beginning the treatment, F(1, 120) = 16.54, p < 0.001, which then remained at a similar level through Month 1, 6 and 12, F(79) = 0.99, p = 0.40. The control group did not present any significant change in self-efficacy, F(1, 124) = 0.05, p = 0.82.
Impacts of the Self-Help Treatment on Negative Consequences of Gambling and Life Satisfaction
Negative Consequences of Gambling
A significant time × group effect was found for social life, F(1, 58) = 7.10, p = 0.01. Compared with the initial assessment, the treatment group perceived significantly less consequences of gambling over social life at Week 11, F(1, 58) = 34.52, p < 0.0001. Mean score of consequences on social life then remained stable through Month 1 to 12, F(69) = 1.34, p = 0.27. A significant time × group effect for finances was found, F(1,53) = 15.11, p < 0.001, indicating that the treatment group perceived significantly less gambling consequences over finances at Week 11, F(1, 53) = 50.24, p < 0.0001, that remained stable at Month 1, 6 and 12, F(71) = 2.63, p = 0.06. Finally, a significant time × group interaction effect was found for quality of life, F(1, 44) = 8.12, p = 0.007. Mean number of negative consequences on quality of life for the treatment group decreased at Week 11, F(1, 28) = 11.71, p = 0.001, and remained similar throughout follow-ups, F(71) = 0.95, p = 0.42. No significant changes were found for the control on any of these three subscales, p = 0.05–0.83.
A significant time effect was found for marital life, F(1, 30) = 14.28, p < 0.001, family life, F(1, 56) = 16.24, p < 0.001, mood, F(1, 47) = 13.03, p < 0.001, and sleep, F(1, 53) = 12.11, p = 0.001, indicating a decrease in these negative consequences subscales for both groups. No significant effects were found for work and physical health, p = 0.10–0.17.
Life Satisfaction
A significant time × group interaction effect was found for satisfaction with social activities, F(1, 53) = 9.26, p = 0.004. Mean satisfaction of the treatment group significantly increased at Week 11, F(1, 27) = 15.87, p < 0.001, and remained similar throughout follow-ups, F(71) = 2.53, p = 0.06. Regarding finances, a significant time × group effect was obtained, F(1, 54) = 9.43, p = 0.003. Participants in the treatment group were significantly more satisfied with their finances at Week 11, F(1, 54) = 9.43, p = 0.003, and their satisfaction level did not differ significantly during the follow-up period, F(71) = 0.25, p = 0.86. A significant interaction effect was found for psychological well-being, F(1, 56) = 12.33, p < 0.001, indicating that the treatment group perceived an improvement in their well-being at Week 11, F(1, 56) = 27.74, p < 0.001, which remained similar through Month 1–12, F(96) = 0.59, p = 0.62. No significant changes were noted on these three subscales for the control group, p = 0.16–0.76.
A significant time effect was found for satisfaction regarding overall pleasure in life, indicated an increase in satisfaction for all participants at Week 11, F(1, 56) = 7.45, p = 0.008. No significant effects were found for the other subscales, p = 0.03–0.99.
Satisfaction with the Treatment Program and Workbook Completion
When asked about positive aspects of the program at Week 11, participants in the treatment group (n = 27) reported having appreciated the workbook, the telephone interviews conducted by therapists with an empathic and non-judgemental attitude and the overall awareness and reflection raised regarding problem gambling. When asked for suggestions on ways to improve the program, some participants did not find any aspects to improve or modify whereas others suggested to modify elements of the workbook or to add more telephone support. Two participants reported not having liked the self-directed approach and one participant did not find the therapist support well-adjusted to individual needs.
At Week 11, participants in the treatment group were asked to rate their satisfaction with the results obtained in the program; 56% reported they were satisfied or highly satisfied, 41% moderately satisfied and one person was unsatisfied. Of the 27 participants of the treatment group assessed at Week 11, 29% had completed their workbook. Of the 25 participants who provided data at Month 1 and 6, 56 and 68% had completed their workbook respectively. Finally, 70% of the 23 participants who provided data at Month 12 reported having finished their workbook by that time.
Discussion
This study aimed to assess the efficacy of a self-help treatment developed in French by comparing it to a waiting list group. As anticipated, the significant differences between the groups after 11 weeks on most outcome variables confirm therapeutic gains for participants who took part in the treatment program. The second hypothesis regarding a significant decrease in negative consequences caused by gambling and an increase in life satisfaction is partly supported as changes were only found for specific subscales of these outcome variables. Overall, consistent with findings from Swan and Hodgins (2015), results from this study support the efficacy of the self-help treatment for at-risk and pathological gamblers.
Gamblers who took part in the treatment program significantly improved regarding their gambling problem, as shown by the mean number of diagnostic criteria decreasing below the diagnostic threshold after 11 weeks, and then remaining stable throughout follow-ups. Likewise, increase in self-efficacy underlines that gamblers felt more in control when facing their high-risk gambling situations, which is consistent with the cognitive-behavioral approach of the workbook (Hodgins et al. 2004b). By providing appropriate material and therapist support, the self-help treatment offers a simple treatment alternative that allows problem gamblers to quickly put changes into place by themselves.
As opposed to the study by Ladouceur et al. (2015) in which improvement regarding gambling expenditure was not maintained at Month 6, all gambling behavior outcome variables in this study remained stable through all follow-ups. These results are similar to those of Carlbring and Smit (2008) and Hodgins et al. (2001, 2004a, b, 2009). Tools provided in the workbook that aimed to foster better control of one’s gambling habits seem to have been on target. Moreover, the additional information and accounts from former participants of the program may have encouraged participants in this study to remain involved in the treatment. As a matter of fact, a greater proportion of participants had completed their workbook at the follow-up assessments than at Week 11, which suggests that they kept on reading and implementing the material from the workbook, even after motivational support with the therapist was over. This most likely contributed to maintain the improvements in time.
To date, various combinations of self-help treatments have been evaluated (Rash and Petry 2014). The treatment in this study offered three motivational interviews (MI), which seemed to positively influence the participants, although different combinations were not compared. Carlbring and Smit (2008) also found benefits to the inclusion of weekly feedback telephone interviews over an eight-week treatment period. On the other hand, Hodgins et al. (2009) did not find additional value from multiple brief support phone calls compared to a single MI. It should be noted that MIs in this study were designed to guide participants in their treatment and address their ambivalence, rather than to provide support only. Further studies should specifically compare the combination of a workbook with one or several MIs that follow a similar canvas in order to clarify the number of interviews to offer for an optimal outcome.
Furthermore, although the precise number of therapist contacts to include in a self-help treatment has yet to be determined, most participants in this study and in other brief treatments (e.g. Hodgins et al. 2001, 2009) positively evaluated therapist contact and some even reported they would have appreciated additional phone calls. Therapist contact thus contributes to participants’ satisfaction with the program, which is noteworthy given that treatment satisfaction is directly related to a higher level of post-treatment functioning and to a reduction of gambling habits (Monnat et al. 2014). Therefore, even during a self-directed treatment process, validation of gamblers’ experience through motivational phone calls as well as the provision of appropriate treatment material are key components.
Following recommendations made by Walker et al. (2006) on the reporting of outcomes in gambling treatment studies, this study provides additional insight into the functioning of participants by documenting the impact of the self-help treatment on negative consequences of gambling and life satisfaction. The treatment group reported a decrease in negative gambling consequences over social life, finances and quality of life and, coherently, a greater satisfaction with social activities, finances and psychological well-being than the control group. These results highlight that, through a better control of their gambling behavior, the participants noticed improvements in the areas directly affected by problem gambling.
However, participants in both groups reported less gambling consequences on family and marital life, mood and sleep at Week 11. The mere fact of knowing that a help resource was going to be provided may have raised hopes in gamblers and led them to perceive less consequences over their mood and relationships, which could explain the overall improvement of participants on these dimensions, regardless of the study condition. To increase treatment outcome on family and marital life, the self-help treatment could offer documentation to the relatives upon request from the gamblers. Such a strategy could then help decrease relationship problems (Hodgins et al. 2007).
Positive changes in specific life satisfaction subscales also suggest that the treatment does not target every life dimension of the participants (e.g. self-esteem, studies/work). On that matter, Sander and Peters (2009) recommend to emphasize development of coping skills with daily life problems which frequently occur among problem gamblers. Finally, negative consequences from gambling most likely offer a more direct and precise measure of outcome whereas life satisfaction may be prone to more subjectivity and vary according to external factors other than problem gambling.
Treatment dropout is worth-mentioning. The 13% dropout rate at Week 11 in the present study is close to those reported by Hodgins et al. (2001, 2009), but is markedly lower than the 32% rate found by Ladouceur et al. (2015). Unlike in the study by Ladouceur et al. (2015) where treatment outcome was assessed once the workbook was completed by participants, specific assessment times and gift vouchers with increasing rather than fixed amounts may have encouraged retention in the study. Because gamblers were not required to have completed their workbook, they may have felt more incline to participate in the telephone interviews. This methodological element should not be overlooked when aiming to restrict missing data due to treatment dropout, as it is a major issue in problem gambling treatment studies (Giroux et al. 2015; Melville et al. 2007). The provision of three MIs may also have helped to strengthen the therapeutic alliance and, consequently, retention in the study.
Most participants in the treatment group reported having completed their workbook at their own pace, whereas a few participants had not completed the workbook at Month 12. This finding echoes a proposition by Pulford et al. (2010) according to which the adaptation of treatment to match individual needs is essential. Similarly, problem gamblers who have previously sought treatment also pointed out that a flexible treatment format may encourage a greater number of gamblers to seek help and persevere in treatment (Faucher-Gravel 2016; Hing et al. 2014). The self-help program thus allows each individual to customize treatment to their needs, and this has shown to be helpful to a great proportion of problem gamblers in this study.
This study is the first to report efficacy data of a self-help treatment for problem gambling with French Canadian participants. The assessment of the efficacy of the self-help treatment on several outcome measures and inclusion of a 12-month follow-up are also strengths of this study. However, methodological limitations must be acknowledged. First, the dependent variables were collected using self-report questionnaires. Despite efforts to ensure that two different therapists would conduct assessments and MIs with a same participant, this situation could not be completely avoided. Nevertheless, a statistical analysis revealed no significant interaction effect for the number of therapists on the results. The fact that therapists who conducted the assessments were not blind to the trial condition may have introduced bias. Although a comparison with the control group beyond 11 weeks could have brought even more clarifications, the waiting period in this study far exceeds that of similar studies (e.g. Carlbring and Smit 2008; Hodgins et al. 2001). Lastly, the use of non-validated questionnaires to measure life satisfaction, negative consequences of gambling and self-efficacy is another limitation.
Conclusion and Recommendations
This study brings further evidence to the literature on self-help treatments for problem gambling and support the use of the “JEu me questionne” treatment program with French Canadian problem gamblers. Improvements found over a short period of time and that were maintained up to the 12-month follow-up suggest that self-help treatments can be offered as a treatment option, especially in contexts where access to conventional group or individual psychotherapy imply extended waiting time. Furthermore, positive outcomes found for most participants highlight the fact that this intervention is suitable for both at-risk and pathological gamblers. Even if the present study compared a single treatment combination with a control group, it seems that both the workbook and telephone interviews have contributed to the outcome and participants reported that they appreciated both elements. Therefore, it seems that even in a self-directed program, feedback from a therapist is a key-component. Future studies should assess the respective contribution of both components in order to determine the most effective combination.
Notes
DSM-IV-TR (APA 2000) was the current version at the beginning of the study. Allocation of participants was therefore completed based on the number of criteria met according to this version of the DSM.
Five participants were evaluated according to DSM-IV pathological gambling criteria (APA 1994) that were still in effect when the study protocol began. The assessment was then modified with the DSM-5 criteria for the other participants. For the five individuals who were not assessed according to DSM-5, a score was drawn for the DSM-IV score, leaving out the illegal acts criterion that was withdrawn in the latest DSM version. Since comparative analyses conducted including and excluding these participants gave similar results, results thus include the entire sample.
References
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: American Psychiatric Publishing.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4, text revision ed.). Washington, DC: American Psychiatric Publishing.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.
Bakeman, R. (2005). Recommended estimated effect size statistics for repeated measures designs. Behavior Research Methods, 37, 379–384. doi:10.3758/BF03192707.
Beck, A. T., Epstein, N., Brown, G., & Steer, R. A. (1988). An inventory for measuring clinical anxiety: Psychometric properties. Journal of Consulting and Clinical Psychology, 56, 893–897. doi:10.1037/0022-006X.56.6.893.
Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Manual for the Beck depression inventory—II. San Antonio, TX: Psychological Corporation.
Campos, M. D., Rosenthal, R. J., Chen, Q., Moghaddam, J., & Fong, T. W. (2015). A self-help manual for problem gamblers: The impact of minimal therapist guidance on outcome. International Journal of Mental Health Addiction. doi:10.1007/s11469-015-9579-5.
Carlbring, P., Degerman, N., Jonsson, J., & Andersson, G. (2012). Internet-based treatment of pathological gambling with a three-year follow-up. Cognitive Behaviour Therapy, 41, 321–334. doi:10.1080/16506073.2012.689323.
Carlbring, P., & Smit, F. (2008). Randomized controlled trial of Internet-delivered self-help with telephone support for pathological gamblers. Journal of Consulting and Clinical Psychology, 76, 1090–1094. doi:10.1037/a0013603.
Castren, S., Pankakoski, M., Tammimen, M., Lipsanen, J., Ladouceur, R., & Lahti, T. (2013). Internet-based CBT intervention for gamblers in Finland: Experiences from the field. Scandinavian Journal of Psychology, 54, 230–235. doi:10.1111/sjop.12034.
Centre québécois d’excellence pour la prévention et le traitement du jeu (CQEPTJ). (2012). JEu me questionne. Québec: Université Laval.
Centre québécois d’excellence pour la prévention et le traitement du jeu (CQEPTJ). (2013). Entrevue diagnostique sur le jeu pathologique, version DSM-5. Québec: Université Laval.
Cowlishaw, S., Merkouris, S., Chapman, A., & Radermacher, H. (2014). Pathological and problem gambling in substance use treatment: A systematic review and meta-analysis. Journal of Substance Abuse Treatment, 46, 98–105. doi:10.1016/j.jsat.2013.08.019.
Crisp, B. R., Thomas, S. A., Jackson, A. C., Smith, S., Borrell, J., Ho, W., et al. (2004). Not the same: A comparison of female and male client seeking treatment from problem gambling counselling services. Journal of Gambling Studies, 20, 283–299. doi:10.1023/B:JOGS.0000040280.64348.d1.
Crisp, B. R., Thomas, S. A., Jackson, A. C., & Thomason, N. (2001). Partners of problem gamblers who present for counselling: Demographic profile and presenting problems. Journal of Family Studies, 7, 208–2016. doi:10.5172/jfs.7.2.208.
Cunningham, J. A., Hodgins, D. C., & Toneatto, T. (2008). Problem gamblers’ interest in self-help services. Psychiatric Services, 59, 695–696. doi:10.1176/appi.ps.59.6.695-a.
Diskin, M. K., & Hodgins, D. C. (2009). A randomized controlled trial of a single session motivational intervention for concerned gamblers. Behaviour Research and Therapy, 47, 382–388. doi:10.1016/j.brat.2009.01.018.
Dowling, N. (2009). Client characteristics associated with treatment attrition and outcome in female pathological gambling. Addiction Research and Theory, 17, 205–219. doi:10.1080/16066350802346193.
Dziura, J. D., Post, L. A., Qing, Z., Zhixuan, F., & Peduzzi, P. (2013). Strategies for dealing with missing data in clinical trials: From design to analysis. Yale Journal of Biology and Medicine, 86, 343–358.
Faucher-Gravel, A. (2016). Comment favoriser l’utilisation des ressources d’aide chez les joueurs problématiques? (Doctoral dissertation). Retrieved from http://theses.ulaval.ca/archimede/?wicket:interface=:2::::.
Ferris, J. & Wynne, H. (2001). The Canadian problem gambling index: Final report. Ottawa: Canadian Centre on Substance Abuse.
Gainsbury, S., Hing, N., & Suhonen, N. (2014). Professional help-seeking for gambling problems: Awareness, barriers and motivators for treatment. Journal of Gambling Studies, 30, 503–519. doi:10.1007/s10899-013-9373-x.
Giroux, I., Demers, B., Jacques, C., Sévigny, S., & Bouchard, S. (2015). Synthèse des connaissances sur l’entrée, la persistance et l’abandon des joueurs pathologiques en traitement. Rapport remis au Fonds de recherche du Québec - Société et culture (FRQ-SC). Québec: Université Laval.
Gueorguieva, R., & Krystal, J. H. (2004). Move over ANOVA: Progress in analyzing repeated-measures data and its reflection in papers published in the Archives of General Psychiatry. Archives of General Psychiatry, 61, 310–317. doi:10.1001/archpsyc.61.3.310.
Hing, N., Nuske, E., Tolchard, B., & Russel, A. (2014). What influences the type of help that problem gamblers choose? A preliminary grounded theory model. International Journal of Mental Health and Addiction, 13, 241–256. doi:10.1007/s11469-014-9525-y.
Hodgins, D. C., Currie, S. R., Currie, G., & Fick, G. H. (2009). Randomized trial of brief motivational treatments for pathological gamblers: More is not necessarily better. Journal of Consulting and Clinical Psychology, 77, 950–960. doi:10.1037/a0016318.
Hodgins, D. C., Currie, S. R., & el-Guebaly, N. (2001). Motivational enhancement and self-help treatments for problem-gambling. Journal of Consulting and Clinical Psychology, 69, 50–57. doi:10.1037/0022-006X.69.1.50.
Hodgins, D. C., Currie, S., el-Guebaly, N., & Peden, N. (2004a). Brief motivational treatment for problem gambling: A 24-month follow-up. Psychology of Addictive Behaviors, 18, 293–296. doi:10.1037/0893-164X.18.3.293.
Hodgins, D. C., Peden, N., & Makarchuk, K. (2004b). Self-efficacy in pathological gambling treatment outcome: Development of a gambling abstinence self-efficacy scale (GASS). International Gambling Studies, 4, 99–108. doi:10.1080/14459790412331296947.
Hodgins, D. C., Toneatto, T., Makarchuk, K., Skinner, W., & Vincent, S. (2007). Minimal treatment approaches for concerned significant others of problem gamblers: A randomized controlled trial. Journal of Gambling Studies, 23, 215–230. doi:10.1007/s10899-006-9052-2.
Ladouceur, R., Fournier, P., Lafond, S., Boudreault, C., Goulet, A., Sévigny, S., et al. (2015). Impacts of a self-help treatment program for problem gamblers. Canadian Journal of Addiction, 6(2), 37–42.
Ledgerwood, D. M., Wiedemann, A. A., Moore, J., & Arfken, C. L. (2012). Clinical characteristics and treatment readiness of male and female problem gamblers calling a state gambling helpline. Addiction Research and Theory, 20, 162–171. doi:10.3109/16066359.2011.588815.
Melville, K. M., Casey, L. M., & Kavanagh, D. J. (2007). Psychological treatment dropout among pathological gamblers. Clinical Psychology Review, 27, 944–958. doi:10.1016/j.cpr.2007.02.004.
Monnat, S. M., Bernhard, B., Abarbanel, B. L. L., St. John, S., & Kalina, A. (2014). Exploring the relationship between treatment satisfaction, perceived improvements in functioning and well-being and gambling harm reduction among clients of pathological gambling treatment programs. Community Mental Health Journal, 50, 688–696. doi:10.1007/s10597-013-9635-1.
Petry, N., Rash, C. J., & Alessi, S. (2016). A randomized controlled trial of brief interventions for problem gambling in substance abuse treatment patients. Journal of Consulting and Clinical Psychology, 84, 874–886. doi:10.1037/ccp0000127.
Petry, N. M., Stinson, F. S., & Grant, B. F. (2005). Comorbidity of DSM-IV pathological gambling and other psychiatric disorders: Results from the national epidemiologic survey on alcohol and related conditions. Journal of Clinical Psychiatry, 66, 564–574. doi:10.4088/JCP.v66n0504.
Pocock, S. J., & Simon, R. (1975). Sequential treatment assignment with balancing for prognostic factors in the controlled clinical trial. Biometrics, 31, 103–115.
Pulford, J., Adams, P., & Sheridan, J. (2010). Responding to treatment dropout: A review of controlled trials and suggested future directions. Addiction Research and Theory, 18, 298–315. doi:10.3109/16066350903151385.
Pulford, J., Bellringer, M., Abbott, M., Clarke, D., Hodgins, D., & Williams, J. (2009). Barriers to help-seeking for a gambling problem: The experiences of gamblers who have sought specialist assistance and the perceptions of those who have not. Journal of Gambling Studies, 25, 33–48. doi:10.1007/s10899-008-9113-9.
Rash, C. J., & Petry, N. M. (2014). Psychological treatments for gambling disorder. Psychology Research and Behavior Management, 7, 285–295. doi:10.2147/PRBM.S40883.
Raylu, N., Oei, T. P. S., & Loo, J. (2008). The current status and future direction of self-help treatments for problem gamblers. Clinical Psychology Review, 28, 1372–1385. doi:10.1016/j.cpr.2008.07.005.
Saghaei, M., & Saghei, S. (2011). Implementation of an open-source customizable minimization program for allocation of patients to parallel groups in clinical trials. Journal of Biomedical Science and Engineering, 4, 734–739. doi:10.4236/jbise.2011.411090.
Sander, W., & Peters, A. (2009). Pathological gambling: Influence of quality of life and psychological distress on abstinence after cognitive-behavioral inpatient treatment. Journal of Gambling Studies, 25, 253–262. doi:10.1007/s10899-009-9128-x.
Scott, N. W., McPherson, G. C., Ramsay, C. R., & Campbell, M. K. (2002). The method of minimization for allocation to clinical trials: A review. Controlled Clinical Trials, 23, 662–674. doi:10.1016/S0197-2456(02)00242-8.
Simoneau, H., Landry, M., Tremblay, J. (2004). Alcochoix+, un guide pour choisir et atteindre vos objectifs. Montréal, Québec: Recherche et intervention sur les substances psychoactives—Québec (RISQ).
Slutske, W. S. (2006). Natural recovery and treatment-seeking in pathological gambling: Results of two U.S. national surveys. The American Journal of Psychiatry, 163(2), 297–302. doi:10.1176/appi.ajp.163.2.297.
Suurvali, H., Hodgins, D., Toneatto, T., & Cunningham, J. (2008). Treatment seeking among Ontario problem gamblers: Results of a population survey. Psychiatric Services, 59, 1343–1346. doi:10.1176/appi.ps.59.11.1343.
Swan, J. L., & Hodgins, D. C. (2015). Brief interventions for disordered gambling. Canadian Journal of Addiction, 6(2), 29–36.
Tremblay, J., Rouillard, P., & et Sirois, M. (2001). Dépistage/évaluation du besoin d’aide—Alcool/Drogues. Québec, Service de recherche CRUV/CRAT-CA. www.risqtoxico.ca.
Volberg, K. A., Nysse-Carris, K. L., & Gerstein, D. R. (2006). 2006 California problem gambling prevalence survey. Chicago: National Opinion Research Centre (NORC) at the University of Chicago. Retrieved June 22, 2012 from http://www.adp.ca.gov/opg/pdf/CA_Problem_Gambling_Prevalence_Survey-Final_report.pdf.
Walker, M., Toneatto, T., Potenza, M. N., Petry, N., Ladouceur, R., Hodgins, D. C., et al. (2006). A framework for reporting outcomes in problem gambling treatment research: The Banff, Alberta consensus. Addiction, 101, 504–511. doi:10.1111/j.1360-0443.2005.01341.x.
Williams, R. J., Volberg, R. A. & Stevens, R. M. G. (2012). The population prevalence of problem gambling: Methodological influences, standardized rates, jurisdictional differences, and worldwide trends. Report prepared for the Ontario Problem Gambling Research Centre and Ontario Ministry of Health and Long Term Care. Retrieved from https://www.uleth.ca/dspace/bitstream/handle/10133/3068/2012-PREVALENCE-OPGRC%20(2).pdf?sequence=3.
Yakovenko, I., Quigley, L., Hemmelgarn, B. R., Hodgins, D. C., & Ronksley, P. (2015). The efficacy of motivational interviewing for disordered gambling: Systematic review and meta-analysis. Addictive Behaviors, 43, 72–82. doi:10.1016/j.addbeh.2014.12.011.
Funding
This study was made possible by a grant from the Fonds de recherche du Québec—Société et culture in collaboration with the Ministry of Health and Social Services of Quebec (Grant No. 2012-JU-164278). Catherine Boudreault received a scholarship for the writing of this article from the Centre de réadaptation en dépendance de Montréal-Institut universitaire.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all participants for being included in the study.
Rights and permissions
About this article

Cite this article
Boudreault, C., Giroux, I., Jacques, C. et al. Efficacy of a Self-Help Treatment for At-Risk and Pathological Gamblers. J Gambl Stud 34, 561–580 (2018). https://doi.org/10.1007/s10899-017-9717-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10899-017-9717-z