
Abstract
Depression is a potentially life threatening affective disorder that is highly prevalent in individuals with autism spectrum disorders (ASD). This study aimed to evaluate the feasibility, acceptability and preliminary efficacy of a cognitive behavioural intervention for depression in adolescents with ASD. Participants were randomly assigned to the intervention group, or wait-list control group. Although recruitment was extremely difficult, attendance was favourable and attrition was low, and participants reported being satisfied with the programme. No significant treatment effect was revealed on the Beck Depression Inventory or Emotion Regulation Questionnaire. However despite the small sample size (n = 20), there was a trending treatment effect measured by the Depression Anxiety Stress Scale: Depression Subscale. Limitations and areas of future research are discussed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Previous research investigating depression in autism spectrum disorders (ASD) suggests high rates in this population, ranging between 17 and 44 %, and varying depending on the age of the sample and measures used (e.g., Green et al. 2000; Kim et al. 2000; Strang et al. 2012). Lugnegård et al. (2011) conducted structured clinical interviews with 54 adults with ASD, and reported 70 % to have had at least one major depressive episode in their lifetime, and 50 % to have had recurring depressive episodes in their lifetime. Furthermore, suicidal behaviour amongst adolescents and young adults with ASD ranges from 7 to 42 % (Hannon and Taylor 2013), as opposed to 4–8 % in typical adolescents and young adults (Cash and Bridge 2009; Gmitrowiez et al. 2003; Resch et al. 2008). This evidence illustrates a significant need for an intervention targeting symptoms of depression in this population.
Previous studies have suggested poor emotion regulation skills to be a contributing factor in elevated rates of depression in ASD. Ehring et al. (2011) illustrated how in non-ASD samples, previously depressed individuals tended to use dysfunctional emotion regulation strategies (e.g., expressive suppression) significantly more, and functional strategies (e.g., cognitive reappraisal) significantly less, than never-depressed individuals. Cognitive reappraisal involves re-evaluating the cause of an emotion, and typically results in reduced experience of the emotion (Goldin et al. 2008). Expressive suppression involves inhibiting the behavioural expression of the emotion (e.g., masking) and typically results in an unchanged or enhanced experience of the emotion (Roberts et al. 2008). Samson et al. (2012) investigated how frequently adults with ASD used these two emotion regulation strategies, and revealed their sample to use reappraisal significantly less, and suppression significantly more, than typical adults. Additionally, our preliminary research tends to suggest that adolescents and young adults with ASD who report the use of reappraisal tend to report fewer symptoms of depression, and adolescents and young adults with ASD who report the use of suppression tend to report more symptoms of depression. This suggests to us that symptoms of depression in the ASD population may be the result of excessive use of dysfunctional emotion regulation strategies, and limited use of functional emotion regulation strategies.
Theoretical Underpinnings of Emotion Regulation Difficulties
Mazefsky and White (2014) discuss the characteristics of ASD that may hinder the emotion regulation process, including poor inhibition and problem solving, change inhibition, sensory sensitivities, and poor cognitive flexibility. Indeed cognitive flexibility has been linked with the ability to down-regulate emotions (Gyurak et al. 2009). However Mazefsky and White (2014) emphasise the role of ToM difficulties and alexithymia. Similarly, Samson et al. (2012) suggested that the use of dysfunctional emotion regulation strategies may be the result of ToM difficulties. ToM is the ability to attribute the mental states of others. There is strong evidence that individuals with ASD typically present with ToM difficulties (e.g., Beaumont and Sofronoff 2008; Kimhi et al. 2014). Mazefsky et al. (2013) suggested that ToM difficulties may hinder one’s ability to accurately evaluate the responses of others in an emotionally provocative situation. This may then hinder attempts to reappraise the situation. Additionally, previous research has suggested a link between the process of assessing the mental states of others and the emotional state of oneself (Frith and Firth 2003; Moriguchi et al. 2006). Therefore ToM difficulties may lead to a difficulty identifying and labelling one’s emotions (alexithymia). Berthoz et al. (2013) revealed 55 % of their sample of 38 adults with ASD endorsed symptoms consistent with alexithymia on the Toronto Alexithymia Scale (TAS; Bagby et al. 1994). Additionally our preliminary research indicated 71 % of a sample of 179 adolescents and young adults with ASD also endorsed symptoms consistent with alexithymia. Furthermore, it was revealed that participants reporting difficulties with identifying and labelling their emotions were also likely to report using less cognitive reappraisal, and more expressive suppression.
To test this theory, the current study included a ToM measure: the Reading the Mind in the Eyes Task (RMET; Baron-Cohen et al. 2001). The RMET requires participants to attribute the mental state of a person after only being presented with a photo of the person’s eyes. This test was designed to detect subtle ToM difficulties in those populations with ASD that with age may have developed other compensatory strategies to pass standard ToM tests, yet still struggle to understand the thoughts and feelings of others in everyday life. For example, Scheeren et al. (2013) did not reveal any differences between young participants (aged 6–20 years) with ASD and typically developing participants on 5 ToM tasks but did find that participants significantly improved on ToM tasks with age. While it involves facial recognition, the RMET was able to reveal significant differences between ASD and non-ASD samples where a basic emotion recognition task could not (Baron-Cohen et al. 1997). If the RMET is significantly associated with measures of emotion regulation, or depression post-intervention, then it would suggest that emotion regulation difficulties may stem from ToM difficulties.
Cognitive Behaviour Therapy for Autism Spectrum Disorders
The evidence linking emotion regulation skills to depression (Campbell-Sills et al. 2006; Ehring et al. 2011) suggests that interventions focusing on increasing the use of cognitive reappraisal may benefit depressed adolescents with ASD. Cognitive behaviour therapy (CBT) typically involves cognitive-restructuring, which is comparable to cognitive reappraisal as it focuses on changing one’s thoughts about the cause of an emotion. CBT has been effective in reducing symptoms of anxiety in children with ASD (e.g., Chalfant et al. 2007; Sofronoff et al. 2005). Ung et al. (2015) conducted a meta-analysis investigating the effect of CBT on anxiety in young people with ASD aged 18 years or younger. They included 14 studies with a pooled sample of 511 participants. The authors revealed a significant treatment effect for participants who had participated in CBT over controls, suggesting that CBT can work for young ASD populations.
However, the only study that appears to target adolescents who have an ASD and depression is a study by McGillivray and Evert (2014), which evaluated a CBT programme targeting depression, anxiety, and stress, in adolescents and young adults with ASD. McGillivray and Evert (2014) assigned 26 adolescents with ASD aged between 15 and 25 to participate in 9 week CBT programme, and 16 adolescents to a wait-list control group. The authors initially did not reveal significant improvement in the treatment group compared to the control group. However they revealed significant improvement in the treatment group over the control group when they only analysed participants who had scored above the normal range on the Depression Anxiety Stress Scale subscales (DASS; Lovibond and Lovibond 1995a) and the Automatic Thoughts Questionnaire (Hollon and Kendall 1980). The treatment group reported a significant drop in the DASS Depression scores relative to the wait-list control group (η2 = .15). However, the intervention group and wait-list control group reported a similar reduction in automatic thoughts associated with depression (η2 < .01). It should be noted however that assignment to the intervention group and wait-list control group was not random and so the outcomes should be treated with caution. The current study aimed to evaluate the feasibility, acceptability and preliminary efficacy of a CBT intervention for depression in adolescents with ASD in a randomised controlled trial. It is important to emphasise that this is a pilot trial, which aims to establish whether a fully powered randomised controlled trial would be feasible to conduct in the future. Feasibility and acceptability of the programme were assessed via participant recruitment, attendance, and satisfaction. Preliminary efficacy was assessed by observing any change in self-reported symptoms of depression and use of emotion regulation strategies. It is important to note that the current study was underpowered to detect an intervention effect. However, if the following research questions are satisfied, it would provide some basis for a larger randomised controlled trial:
-
1.
Is it feasible to recruit and engage adolescents with ASD and depression through a CBT programme that aims to address depressive symptomatology?
-
2.
Do the adolescents with ASD find the programme acceptable and useful?
-
3.
Does the CBT programme reduce self-reported symptoms of depression the use of expressive suppression, and increase the use of cognitive reappraisal?
-
4.
Do the effects of the programme remain stable 3 months post-intervention?
-
5.
Are ToM difficulties associated with self-reported emotion regulation skills and symptoms of depression?
Method
Participants
Recruitment
Recruitment for the trial ran between July 2013 and June 2014. Methods used to recruit participants included the distribution of flyers to schools and clinics around south east Queensland, Facebook groups, and autism associations (e.g., Asperger’s Services Australia, and Autism Queensland). Although the study was very well advertised, response rates were much lower than expected.
Eligibility
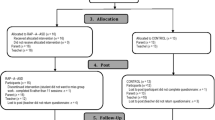
Ninety three enquiries were received about the programme, of which only 42 agreed to be assessed for eligibility (see Fig. 1 for CONSORT diagram). To be considered eligible, participants had to satisfy four conditions. First, participants needed to have scored 14 or higher on the Beck Depression Inventory (BDI; Beck et al. 1996). Seven adolescents scored below 14 on the BDI, indicating that they had minimal or no depressive symptoms, and so no change in depressive symptoms would be expected. Third, if participants answered “I would like to kill myself” or “I would kill myself if I had the chance” on question nine of the BDI, they underwent a suicide risk assessment. If the participant was considered at high risk of suicide, they were excluded from the programme and referred to more appropriate services that could provide immediate support. Six adolescents were deemed to be high risk and were referred. Participants were also assessed using the Wechsler Abbreviated Scale of Intelligence (WASI; Psychological Corporation 1999) and were required to show a verbal intelligence quotient (VIQ) of at least 85. This is because the programme requires at least an average level of comprehension, especially when cognitive strategies are discussed with the participants. A VIQ of 85 was set as the cut-off as this is 1 standard deviation below the average VIQ, excluding the bottom 16 %. Four adolescents were assessed as having a VIQ less than 85 and were excluded from the study. Last, participants required a diagnosis of an ASD from a Medical Practitioner, Paediatrician, Psychiatrist, Psychologist, or multi-disciplinary team. Due to the time requirements of the WASI and baseline questionnaires, conducting a diagnostic test such as the ADOS (Lord et al. 2000) on the same visit was not feasible and would have required a second visit to the clinic to assess eligibility. Because there were already great difficulties getting participants into the clinic for the first visit, requiring participants to come back for a second visit to assess eligibility likely would have substantially reduced the number of participants to be randomised, reducing generalisability of the results. Therefore this study relied on parental reports of previous clinical diagnosis, including who the doctor was and when the diagnosis was received. Furthermore parents were also interviewed with the Asperger Syndrome (and High-Functioning Autism) Diagnostic Interview (ASDI), which is based on Gillberg’s criteria for Asperger’s syndrome (Ehlers and Gillberg 1993; Gillberg and Gillberg 1989; see below). Two adolescents did not have a diagnosis and were excluded from the study. To reduce bias in parental reports, ineligible participants (except adolescents with a VIQ below 85) were to be placed into their own group and still receive the programme. The remaining 23 adolescents were randomised via a computer-generated random sequence programme into either the intervention group or the wait-list control group. Following randomisation, one adolescent from the intervention group and one from the wait-list control group withdrew from the study. A further participant in the wait-list control group was hospitalised for suicidal ideation despite not presenting with suicidal ideation on the day of assessment and withdrew from the study. In the end, 20 participants were present at the start of the trial (M age = 15.75, SD age = 1.37, 12 males).

CONSORT diagram. Dotted lines indicate the time-points for the treatment versus wait-list control group analyses
Measures
Demographics Questionnaire
Participants completed a demographics questionnaire requesting age, gender, ethnicity, birthplace, details of diagnosis, education, and medication use.
Measures Used to Screen for Diagnosis
Australian Scale for Autism Spectrum Conditions (ASASC)
The ASASC (Garnett et al. 2013) is a 44-item ASD profiling measure for parents of children and adolescents aged between 5 and 19 years with a diagnosis of ASD. It addresses five dimensions of ASD: difficulty understanding emotions, orientation towards facts, sensory sensitivity, difficulty with social communication, and rigid adherence to routines. It is designed to help profile the symptomatology of children and adolescents with ASD. For each item, parents compare their child to a typical child on a particular trait, and respond on a 5-point scale with 1 = “Very much less often than a typical child” and 5 = “Very much more often than a typical child”. The internal reliability of the scale in this sample was good (α = .87).
Asperger Syndrome (and High-Functioning Autism) Diagnostic Interview (ASDI)
The ASDI (Gillberg et al. 2001) is a diagnostic interview conducted by a clinician with a relative of the individual with ASD (typically the parent). The interview focuses on six areas of ASD: social interaction impairments, special interests, routines, speech peculiarities, non-verbal communication problems, and motor clumsiness. According to Gillberg et al. (2001), 100 % of his validation sample met at least five out of six criteria. In the current study, 11 met all 6 criteria, 7 met 5 criteria, and 2 met 4 criteria.
Measures Used to Screen for Depression Symptoms
Beck Depression Inventory-II (BDI)
The BDI-II (Beck et al. 1996) is a 21-item questionnaire measuring symptoms of depression. Each item consists of four statements revolving around a feeling or an issue (e.g., self-dislike). Participants are asked to pick one statement out of the four that best describes the way they had been feeling over the past 2 weeks. The statements are coded from 0 = e.g., “I feel the same about myself as ever” to 3 = e.g., “I dislike myself”. The internal reliability of the scale in this sample was excellent (α = .94). Factor analysis of the BDI-II reveals a two-factor structure, one measuring cognitive-affective symptoms (e.g., agitation, loss of interest), and one measuring somatic symptoms (changes in sleeping patterns; Beck et al. 1996; Whisman et al. 2000). Therefore it can be considered a measure of psychobiological symptoms of depression.
Depression Anxiety Stress Scale (DASS)
The current study used the 21-item version of the DASS (Lovibond and Lovibond 1995a). It contains seven items for each subscale: depression, anxiety, and stress. Only the depression scale was used in the current study as an additional measure for symptoms of depression. There is precedent for using both the BDI and the DASS in an evaluation study, with the DASS depression subscale as a secondary outcome measure (e.g., Ree and Craigie 2007; Ruwaard et al. 2009). The depression subscale measures the psychological symptoms of depression, focusing on the core construct of depression (i.e. loss of positive affect). Participants respond to a variety of statements and indicate if in the past week that statement applied to them using a 4-point scale ranging from 0 = “did not apply to me at all” to 3 = “applied to me very much”. The internal reliability of the depression subscale in this sample was very good (α = .85).
Measure of Emotion Regulation
Emotion Regulation Questionnaire (ERQ)
The ERQ (Gross and John 2003) is a 10-item measure designed to assess participants’ use of two prominent emotion regulation strategies: cognitive reappraisal and expressive suppression. The cognitive reappraisal subscale contains six items (e.g., “I control my emotions by changing the way I think about the situation I am in”), and the expressive suppression subscale contains four items (e.g., “I control my emotions by not expressing them”). Participants respond to each item on a 7-point likert scale with 1 = “strongly disagree” and 7 = “strongly agree”. The internal reliabilities for the reappraisal and suppression subscales in this sample were very good (α = .86) and good (α = .72) respectively.
Measure of Theory of Mind
Reading the Minds in the Eyes Task (RMET)
The RMET (Baron-Cohen et al. 2001) is a 36-item questionnaire designed to assess ToM. Each item contains a cropped photograph of a person’s eyes, and the participant is asked to determine the mental state of that person from a selection of four mental states (e.g., impatient, amused, embarrassed). A lower score indicates difficulties with ToM. The scale had fair internal reliability (α = .68).
Measure of Cognitive Ability
Wechsler Abbreviated Scale of Intelligence (WASI)
The WASI (Psychological Corporation 1999) is an intelligence test designed to be an abbreviated version of the Wechsler Adult Intelligence Test, containing four subtests: vocabulary, similarities, block design, and matrix reasoning. The vocabulary and similarities subtests are used to estimate VIQ, and the block design and matrix reasoning subtests are used to estimate performance IQ. Full scale IQ is estimated from all four subtests.
Cognitive Behavioural Intervention
The cognitive behavioural intervention was designed by Attwood and Garnett (2013) and called Exploring Depression: Cognitive behaviour therapy to understand and cope with depression. The programme was conducted in a group setting with 3–4 participants per group. Two provisionally registered clinical psychologists, supervised by two senior clinical psychologists, delivered 11 one-hour sessions to each group. Attwood and Garnett, the creators of the Exploring Depression programme, ran workshops to train the probationary clinical psychologists to deliver the material. The first 10 sessions were conducted weekly, and the final session was conducted 4 weeks later as a booster session. The sessions explored different ‘tools’ or strategies the adolescents could use in order to manage symptoms of depression. These consisted of self-awareness tools, physical tools, pleasure tools, thinking tools, social tools, and relaxation tools. Each strategy was represented by a hardware tool and the programme represented as a tool box.
The self-awareness tools involved practising a self-awareness activity, similar to mindfulness, and the programme also goes through activities with the adolescents to help them identify times they felt sad, and to rate their feelings on those occasions. The physical tools involve scheduling physical activities into the week, to improve the adolescent’s physical health and well-being. The pleasure tools involve scheduling activities that the adolescents enjoy, such as pursuing their special interest, or expressing their emotions through art or music. The thinking tools involve thought-challenging and cognitive restructuring. The social tools involve scheduling social activities to help combat feelings of loneliness. Lastly, examples of relaxation tools involved meditation and listening to relaxing music, to help the adolescents feel calm if they ever felt distressed. Throughout the sessions, these tools were discussed with the adolescents, and they were able to choose which tools worked best for them (see Table 4, in “Appendix” for session outlines). Every session assigned home projects for the adolescents to complete before the following session. Home projects involved scheduling the tools they had learned that session into their weekly planner, and completing a self-monitoring sheet to record when they used the tools they had learned, and how they felt before and after they used those tools. The booster session was treated as a re-cap on the tools and an opportunity for feedback on the programme.
Procedure
The study received ethics approval from the Behavioural and Social Sciences Ethics Review Committee at the University of Queensland (UQ) and parent consent was obtained for all participants. Interested adolescents were invited to complete the demographics questionnaire, the DASS, the ERQ, and the RMET online via Qualtrics (2013) in their own time before their first visit to UQ. They were then invited to the School of Psychology Clinic at UQ with their parents to assess their eligibility for the programme. Parents were interviewed using the ASDI and were asked to complete the ASASC. The adolescents were asked to complete the BDI, and the WASI was administered. Diagnostic history (who made the clinical diagnosis and when) was reported by the parents, and the ASDI and ASASC were used as additional screens. Adolescents without a diagnosis of ASD, with a BDI below 14, or a VIQ below 85, or who were actively suicidal were ineligible for the study and were referred to further sources of assistance.
Eligible participants were then randomly assigned to either receive the intervention immediately or to a wait-list control group to receive the intervention later. Participants assigned to the intervention condition received the intervention for 10 weeks. At week five, participants in the intervention condition completed the BDI for a second time to gauge their progress at the halfway point of the programme, and screen for any changes in suicidal ideation. In the 10th week, participants in both the intervention and wait-list groups completed the BDI, the DASS, and the ERQ (post measures). Ethical considerations precluded further delaying treatment for depression to a high-risk group, and participants in the wait-list control group started their 10-week schedule of the intervention on the completion of the treatment group’s 10th session. In week 14, participants in the intervention condition participated in the booster session of the intervention, and completed post measures. In week 22 (8 weeks post-booster follow-up) parents of participants in the intervention condition were contacted for the adolescents to complete the post measures.
Results
Intervention Versus Wait-List Group
Data Preparation
Data completed via online survey was exported into an SPSS (IBM Corp. 2011) data-file, which was then compiled with data completed on paper. For the between-group comparisons, the intervention and wait-list control participants completed all pre-post measures . Therefore there was no missing data. A series of t-tests were conducted to check for baseline differences between the treatment group and the wait-list control group (see Table 1). A t test revealed that the treatment group scored significantly higher on the AQ than the wait-list control group. However, AQ scores were not significantly correlated with any outcome measures at baseline or post-intervention, and the F test for the AQ when it was included as a covariate for each ANOVA was not significant (see Table 2). Therefore, the AQ was not included as a covariate in the final analyses (Lomax and Hahs-Vaughn 2012).
Depression
A 2 (Condition; Intervention vs Control) × 2 (Time; Baseline vs Post-Intervention) mixed factorial ANOVA was conducted to investigate the effect of the intervention on BDI scores. As can be seen in Fig. 2, the analysis revealed no significant main effect of condition or time [F(1, 18) = 0.54, p = .474, η2 = .03 and F(1, 18) = 0.96, p = .341, η2 = .05 respectively], and did not reveal a significant interaction between condition and time [F(1, 18) = 0.02, p = .893, η2 < .01].

The effect of the intervention on BDI scores versus wait-list group
A second 2 (Condition) × 2 (Time) mixed factorial ANOVA was conducted to investigate the effect the programme had on depression levels, however this time with the DASS depression subscale. Similarly to the BDI, there was no significant main effect of condition or time [F(1, 18) = 0.28, p = .602, η2 = .02, and F(1, 18) = .96, p = .339, η2 = .04 respectively]. However unlike the BDI, the interaction between condition and time showed a trend towards significance [F(1, 18) = 3.86, p = .065, η2 = .17; see Fig. 3].

The effect of the intervention on DASS depression scores versus wait-list group
Given the small sample size and pilot nature of the study, this trending interaction was explored. The simple effect of time for the wait-list control group was not significant [F(1, 9) = .37, p = .556, η2 = .04], representing no change between pre-intervention (M = 21.60, SD = 11.03) and post-intervention (M = 23.93, SD = 11.58). However, the simple effect of time for the intervention group was significant [F(1, 9) = 6.11, p = .035, η2 = .40]. This revealed that participants in the intervention group experienced a significant drop in DASS depression scores from pre-intervention (M = 24.20, SD = 8.97) to post-intervention (M = 17.20, SD = 8.95).
Emotion Regulation Skills
Two additional 2 (Condition) × 2 (Time) mixed factorial ANOVAs were conducted to investigate the impact that the intervention had on the use of two important emotion regulation strategies: cognitive reappraisal and suppression. Again, the analysis did not reveal a significant main effect of group on the use of cognitive reappraisal [F(1, 18) = .24, p = .630, η2 = .01]. However, a significant main effect of time was revealed [F(1, 18) = .4.93, p = .039, η2 = .21; see Fig. 4], showing a significant increase in the use of cognitive reappraisal across both groups from pre-intervention (M = 20.35, SD = 7.58) to post-intervention (M = 24.80, SD = 8.06). There was no significant interaction between group and time [F(1, 18) = .14, p = .713, η2 = .01).

The effect of the intervention on ERQ: reappraisal scores versus wait-list group
Similarly to cognitive reappraisal, there was no main effect of condition on the use of expressive suppression [F(1, 18) = .22, p = .646, η2 = .01]. However unlike the use of cognitive reappraisal, there was also no main effect of time on the use of suppression [F(1, 18) = 1.90, p = .185, η2 = .09]. There was also no significant interaction between condition and time [F(1, 18) = .82, p = .376, η2 = .04].
Secondary Analyses: Aggregated Effect of the Programme
Data Preparation
Given the small sample size for the primary analyses, a series of supplementary analyses were conducted, in which the data from intervention group and the wait-list control group were combined to determine the effectiveness of the programme over time. One wait-list control participant provided post-measures for the intervention vs wait-list analyses, but declined to partake in the treatment programme and was therefore excluded from the supplementary analyses. A second wait-list control participant was unable to be contacted to complete the post-questionnaires. This participant was also excluded from the supplementary analyses. After excluding these two participants, there was still missing data from measures taken at the booster session and the 3-month follow-up (see Fig. 1 for details). As the data were missing completely at random (Little’s missing completely at random χ2(9085) < .01, p > .999), no variables or participants were missing more than 50 % of data (Hair et al. 2009), and only 7.40 % of data were missing overall, multiple imputation was employed to handle the missing data. Multiple imputation has been shown to be superior to other methods of dealing with missing data (such as list-wise deletion or last-observation-carried-forward) when the data are missing completely at random, even with very small sample sizes (Barnes et al. 2006).
Depression
A one way repeated measures ANOVA was conducted to investigate the change in BDI scores across time. A significant main effect of time was revealed [F(4, 68) = 4.56, p = .008, η2 = .21; see Fig. 5]. A series of t-tests revealed no change between pre-intervention BDI scores (M = 27.94, SD = 16.11) and BDI scores after 5 weeks [M = 28.38, SD = 16.39, t(68) = .17, p = .868]. However, there was a significant drop in BDI scores between week five and post-intervention [M = 22.99, SD = 16.76, t(68) = 3.16, p = .006], which was maintained at the booster session [M = 19.95, SD = 15.00, t(68) = 3.55, p = .002]. Despite a mean drop of eight points in BDI scores, the average participant still scored in the moderate depression range. While BDI scores post-intervention were only trending to be lower than pre-intervention scores [t(68) = 1.93, p = .071], BDI scores at the booster session were significantly lower than pre-intervention [t(68) = 3.59, p = .002]. Again, BDI scores taken at the booster session showed a trend to be lower than BDI scores taken post-intervention [t(68) = 1.97, p = .066]. However at 3 months post-intervention, BDI scores increased (M = 28.27, SD = 15.50) such that the levels of depression the adolescents experienced were significantly greater than at the booster session [t(68) = 3.48, p = .003]. In fact, at 3 months post-intervention, BDI scores were no longer significantly different from pre-intervention, week five, or post-intervention BDI scores [t(68) = .11, p = .893, t(68) = .03, p = .934, and t(68) = 1.65, p = .118 respectively]. It is important to remember that there were no wait-list control comparisons for measures taken at the booster session or 3 months post-intervention.

Follow-up trajectory of BDI scores using the combined data for intervention and control groups after the control groups completed the intervention. *Indicates significant differences
A second one-way ANOVA exploring depression levels was conducted, this time using DASS Depression scores. Again, a significant main effect of time was revealed [F(3, 51) = 5.15, p = .007, η2 = .23; see Fig. 6]. This was followed up with a series of pair-wise t-tests. There was a significant decrease in DASS depression scores post-intervention (M = 16.33, SD = 12.02) compared to pre-intervention [M = 23.33, SD = 9.87, t(51) = 2.48, p = .024]. Depression scores then remained constant between post-intervention and the booster session [M = 15.05, SD = 7.69, t(51) = .66, p = .518], with booster session depression scores also being significantly lower than pre-intervention scores [t(51) = 3.51, p = .003]. However as illustrated by the BDI scores, DASS depression scores increased significantly at 3 months post-intervention (M = 21.23, SD = 9.50) compared to the booster session [t(51) = 3.07, p = .008]. This rise in depression scores at 3 months meant that participants were no longer significantly less depressed compared to when they started the programme [t(51) = 0.83, p = .422], and were not significantly different from post-intervention scores [t(51) = 1.70, p = .111].

Follow-up trajectory of DASS depression scores using the combined data for intervention and control groups after the control groups completed the intervention. *Indicates significant differences
Emotion Regulation Skills
Two one-way ANOVAs were conducted to investigate how the use of reappraisal and suppression changed during and after the programme. A significant main effect of time on the use of cognitive reappraisal was revealed [F(3, 51) = 4.18, p = .010, η2 = .20; see Fig. 7]. A series of t tests were conducted to investigate this effect. T tests revealed a significant increase in the use of cognitive reappraisal to manage emotions post-intervention (M = 26.28, SD = 6.98) compared to pre-intervention (M = 19.72, SD = 7.72, t(51) = 2.96, p = .009; see Fig. 7). Then, the use of cognitive reappraisal did not change significantly at the booster session 4 weeks post-intervention [M = 24.81, SD = 6.84, t(51) = .840, p = .412]. However, the reported use of cognitive reappraisal by the adolescents at the booster session was no longer significantly more than pre-intervention, but was now a trend [t(51) = 2.02, p = .060]. At the 3 month follow-up, the use of cognitive reappraisal decreased significantly compared to post-intervention use [M = 22.44, SD = 5.88, t(51) = 2.47, p = .032]. However there was no significant difference between the use of cognitive reappraisal at the 3 month follow-up and at the booster session [t(51) = 1.81, p = .103], and was not significantly different from pre-intervention use of reappraisal to manage emotions [t(51) = 1.18, p = .259].

Follow-up trajectory of ERQ: cognitive reappraisal scores using the combined data for intervention and control groups after the control groups completed the intervention. *Indicates significant differences
The main effect of time on the use of expressive suppression was not significant [F(3, 51) = 2.25, p = .108, η2 = .12]. This meant there was no change in suppression scores across the timeline of the programme.
Correlates of Programme Outcomes
To investigate the effect of ToM difficulties on emotion regulation difficulties and programme outcomes, a series of semi-partial correlations were conducted. Semi-partial correlations provide the unique correlation between variables while controlling for other overlapping measures. First, semi-partial correlations between RMET scores and baseline BDI, DASS Depression, ERQ Reappraisal, and ERQ Suppression scores were conducted to establish whether baseline ToM difficulties impacted baseline emotion regulation ability. Second, semi-partial correlations between RMET and participants’ change between baseline and post-intervention were conducted to investigate whether ToM difficulties impacted upon programme outcomes. It should be noted that because the BDI and the DASS Depression subscale measure the same construct, the BDI was not controlled for when calculating the semi-partial correlation between RMET and DASS Depression scores and vice versa. Both sets of semi-partial correlations are shown in Table 3. When controlling for DASS Depression, BDI, and Suppression scores, RMET scores were significantly positively associated with reappraisal scores, meaning the greater participants scored on the RMET the more they reported to use cognitive reappraisal to regulate their emotions. Interestingly when controlling for ERQ: Suppression and ERQ: Reappraisal change scores, RMET scores were positively associated with BDI change scores. This meant the greater participants scored on the RMET, the worse their depression symptoms became according to the BDI. Despite this, RMET scores were also negatively associated with ERQ: Suppression change scores, meaning participants that scored high on the RMET tended to mask their emotions less towards the end of the intervention compared to baseline.
Feasibility and Acceptability Measures
Participant Recruitment
Recruitment of this population was extremely difficult. It was evident from the slow uptake and feedback that parents were experiencing difficulty convincing their adolescent children to participate in the programme. Many parents called asking about the programme, while expressing concern that their child would not agree to it. Several adolescents withdrew after being assessed for eligibility because they did not wish to participate in the programme. It seemed that by the time the participants had reached adolescence, many of the parents had already taken their children to other programmes or participated in other research projects that did not meet their needs, and a common reason given for withdrawal or loss of interest in the programme was the adolescent was “sick of being studied like a guinea pig”. Other parents reported their children were too nervous about the programme running in a group setting, and some adolescents denied having depression or resisted because they felt they did not need help.
Willingness to participate was not the only issue impacting participant numbers. Almost half of the participants assessed for eligibility were not eligible for the programme. The biggest barrier for eligibility was the depression level of the participants. Six participants were excluded for presenting with a moderate or high suicide risk and needed referral to more appropriate and immediate sources of support. Suicidal ideation was a prominent feature in this population. In addition to the six participants excluded for suicidal ideation, one eligible participant was hospitalised for suicidal ideation post-screening. Additionally, several months after the programme started one participant deemed ineligible for presenting with minimal depression symptoms was hospitalised for intentionally drinking bleach to self-harm. This meant that of the 42 participants assessed for eligibility, 19 % were either excluded due to high suicidal ideation, or were hospitalised for suicidal ideation or self-harming behaviour.
Programme Attendance
In total, 19 adolescents started the intervention. Of those 19 adolescents, only 1 withdrew from the 10th session for personal reasons and never returned. There was nothing to indicate that the adolescent withdrew because of dissatisfaction with the programme itself. For the 18 adolescents who finished the intervention, if an adolescent missed a session, then they had the opportunity to attend a one-on-one catch-up session with the psychologists along with their parent. This opportunity was accepted on every occasion. A total of 23 one-on-one catch-up sessions were arranged, and the maximum number of catch-up sessions a single participant received was 4. Overall, once an adolescent started the programme they stayed with it and ensured that they covered the material despite many crisis situations occurring in their lives.
Participant Satisfaction
For 15 adolescents and 7 parents, the booster sessions were audio-recorded so that their feedback on the programme could be taken into consideration. Of the 15 adolescents, 14 reported they enjoyed the programme. The adolescent who reported not enjoying the programme herself stated she would recommend it to others, because she acknowledged the usefulness of the tools. The group setting was considered by most of the adolescents to be the most helpful element of the programme and helped to combat loneliness. Adolescents generally found the tools helpful, but there were individual differences in which strategies were endorsed.
Discussion
The current study aimed to evaluate the feasibility of conducting a larger randomised controlled trial of a new group cognitive behavioural intervention targeting depression in adolescents with ASD. The first research question asked whether it was feasible to recruit and engage adolescents with ASD and depression for a CBT programme targeting depression. The primary evidence against feasibility was the difficulty recruiting eligible participants. This was initially surprising given the evidence of need for an intervention targeting depression in adolescents with ASD (Green et al. 2000; Kim et al. 2000, Lugnegård et al. 2011; Strang et al. 2012). However one explanation for this is that depression does lead to a lack of motivation and engagement, and so difficulty in recruitment may not reflect a lack of need but one of the complications of depression. Furthermore 19 % of adolescents assessed for eligibility were either excluded due to high suicidal ideation, or were hospitalised for suicidal ideation or self-harming behaviour. This reflects previous research illustrating that suicidal ideation is a major concern for this population, with the prevalence of suicidal behaviour amongst adolescents and young adults with ASD ranging from 7 to 42 % (Hannon and Taylor 2013), as opposed to 4–8 % in typical adolescents and young adults (Cash and Bridge 2009; Gmitrowiez et al. 2003; Resch et al. 2008). This poses the question of whether a randomised controlled trial is an appropriate means to determine the efficacy of a programme for depression in this population.
Despite these difficulties, there was preliminary evidence for acceptability of the programme once participants started the intervention. This was demonstrated with a 100 % attendance rate (including catch-up sessions) and high retention rate with only one family leaving the programme prematurely. Additionally the programme had a high proportion of adolescents reporting to enjoy the programme, with only one adolescent stating she did not find the programme helpful. Again this adolescent stated that she would still recommend the programme to others.
The second research question asked whether the programme was effective at reducing symptoms of depression, use of expressive suppression, and increasing the use of cognitive reappraisal. The BDI showed no significant change between post-intervention and pre-intervention or across the two groups. However, the DASS Depression subscale did show preliminary evidence to suggest that the programme may be effective in reducing symptoms of depression. Analysing the DASS Depression scores revealed an interaction trending towards significance. While there was no change observed in DASS Depression scores for adolescents in the wait-list control group, adolescents in the intervention group experienced a significant drop in DASS Depression scores. This mirrors the effect of McGillivray and Evert (2014) CBT programme, which showed a significant drop in DASS Depression scores for participants with ASD who reported baseline DASS Depression scores in the above normal range. McGillivray and Evert (2014) did not use the BDI as an outcome measure.
This difference in findings between the DASS Depression scale and the BDI is puzzling as both are widely used measures of depression with acceptable psychometric properties (Crawford and Henry 2003; Ronk et al. 2013; Richter et al. 1998). They are also typically correlated with each other (Lovibond and Lovibond 1995b), which was replicated in the current study (r = .84, p < .001 at baseline, r = .71, p < .001 post-intervention). It is possible that the different results are due to factor differences between the scales. The BDI tends to measure both the cognitive-affective and somatic symptoms of depression (Beck et al. 1996; Whisman et al. 2000), while the DASS Depression subscale tends to focus on the cognitive-affective symptoms (Lovibond and Lovibond 1995a). A CBT programme focusing on cognitive restructuring may be more likely to influence cognitive-affective symptoms of depression as opposed to somatic symptoms.
When the intervention group and wait-list control group were combined, a significant drop in depression scores was observed for the DASS depression scale after both groups had received the intervention. A similar pattern was observed for the BDI. However it was at the booster session, 4 weeks post-intervention, when BDI scores were significantly lower than pre-intervention scores (also observed with DASS depression scores). This allows us to be cautiously optimistic that the Exploring Depression programme can help in reducing symptoms of depression in adolescents with ASD. However, due to the lack of control group for the booster session, these findings should be interpreted with caution. Furthermore scores across both measures increased after 3 months suggesting that there needs to be a greater emphasis during and after the programme on maintaining the strategies when therapy has been completed.
It was also hypothesised that over the 10 weeks there would be a significant increase in the use of cognitive reappraisal for the intervention group but not for the wait-list control group. Contrary to this hypothesis, both groups significantly increased their use of cognitive reappraisal from baseline. This result was surprising as there was nothing to indicate the wait-list control group should increase in the use of cognitive reappraisal. While the use of cognitive reappraisal has been shown to increase with age (McRae et al. 2012), an increase of this magnitude is still unexpected. However, the follow-up analyses did again reveal a significant decrease at 3 months post-intervention, suggesting a decrease in the use of cognitive reappraisal in the absence of the intervention. Again it is important to remember that there was no control group 3 months post-intervention, and the wait-list control group at 10 weeks showed an equivalent increase in cognitive reappraisal use from baseline compared to the intervention group. Therefore this finding should be interpreted with caution.
Despite predictions, the Exploring Depression programme seemed to have no impact on participants’ use of expressive suppression. While the programme does not target the use of expressive suppression specifically, it was expected that once the participants were taught a variety of functional emotion regulation strategies, they would decrease their use of dysfunctional strategies (i.e., suppression).
The final analyses attempted to investigate the influence of ToM on emotion regulation difficulties and programme outcomes, through a series of correlations. A significant positive semi-partial correlation was revealed between RMET scores and baseline reappraisal scores, suggesting that ToM difficulties may be associated with a decreased use of baseline reappraisal scores. Furthermore, a significant negative semi-partial correlation was revealed between RMET scores and participants’ change in their use of suppression, suggesting that minimal ToM difficulties may be related to a decrease in the use of dysfunctional emotion regulation strategies. It had been theorised that poor ToM ability would have a negative impact on one’s ability to identify and label emotions (alexithymia; Frith and Firth 2003; Moriguchi et al. 2006) and our preliminary research suggests that this may in turn influence what emotion regulation strategies are used. These findings provide preliminary support for this theory, and to the authors’ knowledge, is the first to measure the direct relationship between ToM ability and emotion regulation in adolescents with ASD. However the preliminary aspect should be emphasised as these are associations without evidence for causal relationship. To our surprise, a significant positive semi-partial correlation was revealed between RMET scores and BDI change scores. This meant that participants performing well on a ToM task actually tended to develop worse symptoms of depression as measured by the BDI. No such relationship was revealed between RMET scores and DASS Depression scores.
Limitations and Challenges of this Research
One of the primary limitations of this study was the use of self-report measures to assess eligibility and outcome. Seven of the adolescents assessed for eligibility scored very low on the BDI and therefore were not eligible. As depression was assessed through self-report, it is unknown whether these adolescents were indeed not depressed, or had difficulty labelling their emotions. This was one of the drawbacks of using self-report measures in this project. Mazefsky et al. (2011) illustrated how adolescents with ASD tend to under-report symptoms of depression on self-report measures when compared to a structured diagnostic interview. The decision to use self-reported BDI as a screen for eligibility was based on our preliminary research with a sample of 179 adolescents and young adults with ASD. Furthermore despite the sample showing high endorsement for alexithymia, we also observed a high rate (38 %) of self-reported severe depression according to the DASS. This was on par with depression rates revealed through clinical interviews (30 %; Green et al. 2000) and parental reports (44 %; Strang et al. 2012). A strong association between alexithymia and self-reported depression scores was also revealed in our preliminary research, indicating those who reported to have great difficulty labelling their emotions were still able to report high levels of depression. It was for this reason that parental reports or structured interview for depression were not considered at the start of the trial. However given the relative ease of introducing a parental measure of depression, future trials should employ such measures.
The second challenge faced when running the programme was participant motivation, especially with respect to the homework projects. The homework projects in intervention involved scheduling the tools into their weekly planner, and then recording how they felt before and after using those tools. Homework is an essential part of CBT, as it encourages participants to practice and generalise the tools they have learned in session into their everyday lives, and helps prevent relapse (Kazantzis and Lampropoulos 2002). In fact, homework compliance has been shown to predict improved intervention outcomes (Mausbach et al. 2010). However, homework compliance has been shown to be poor even in typically developing depressed adolescents (Gaynor et al. 2006), likely due to a lack of motivation and engagement associated with depression. Poor homework compliance in the current sample may have had a negative impact on the effectiveness of the programme. Many participants stated that because the scheduling of the tools into their weekly planner was part of the project, it was rarely completed. Several parents suggested that the scheduling of the activities into the weekly planner should be completed during the group session rather than being part of the homework. This would provide a clear plan for the adolescents rather than leaving the adolescents to create their own plans in their own free time. Lastly, as participants were either in the intervention group or a wait-list control group, participants were not blind to the condition they were in and so the results may have been influenced by participant bias.
Future Directions and Conclusion
To the authors’ knowledge, the current study was the first pilot of a randomised controlled trial of a CBT programme for depression in adolescents with ASD. There was mixed preliminary evidence for feasibility, given the low recruitment rate and high suicidality of this population. However both attendance and satisfaction from participants were high, supporting acceptability of such programmes. Furthermore there was cautionary evidence that the programme may be effective in reducing symptoms of depression. However, given the use of self-report measures, small sample size, and lack of control group at follow-up, the results should be interpreted with caution. This study highlights the difficulties and challenges of working with a depressed population with ASD, especially with recruitment, compliance, and suicidal ideation. While it would be beneficial to replicate this study with a bigger sample size, future research needs to investigate possible motivators for adolescents with depression to participate in a depression intervention.
References
Attwood, T., & Garnett, M. (2013). Exploring depression: Cognitive behaviour therapy to understand and cope with depression. London: Jessica Kingsley Publishers.
Bagby, R. M., Parker, J. D. A., & Taylor, G. J. (1994). The twenty-item Toronto alexithymia scale-I. Item selection and cross-validation of the factor structure. Journal of Psychosomatic Research, 38(1), 23–32.
Barnes, S. A., Lindborg, S. R., & Seaman, J. W. (2006). Multiple imputation techniques in small sample clinical trials. Statistics in Medicine, 25, 233–245.
Baron-Cohen, S., Jolliffe, T., Mortimore, C., & Robertson, M. (1997). Another advanced test of theory of mind: Evidence from very high functioning adults with autism or Asperger syndrome. Journal of Child Psychology and Psychiatry, 38(7), 813–822.
Baron-Cohen, S., Wheelwright, S., Hill, J., Raste, Y., & Plumb, I. (2001). The “reading the mind in the eyes” test revised version: A study with normal adults, and adults with Asperger syndrome or high-functioning autism. Journal of Child Psychology and Psychiatry, 42(2), 241–251.
Beaumont, R. B., & Sofronoff, K. (2008). A new computerised advanced theory of mind measure for children with Asperger syndrome: The ATOMIC. Journal of Autism and Developmental Disorders, 38, 249–260.
Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Beck depression Inventory manual (2nd ed.). San Antonio: Psychological Corporation.
Berthoz, S., Lalanne, C., Crane, L., & Hill, E. L. (2013). Investigating emotional impairments in adults with autism spectrum disorders and the broader autism phenotype. Psychiatry Research, 208(3), 257–264.
Campbell-Sills, L., Barlow, D. H., Brown, T. A., & Hofmann, S. G. (2006). Acceptability and suppression of negative emotion in anxiety and mood disorders. Emotion, 6(4), 587–595.
Cappadocia, M. C., Weiss, J. A., & Pepler, D. (2012). Bullying experiences among children and youth with autism spectrum disorders. Journal of Autism and Developmental Disorders, 42, 266–277.
Cash, S. J., & Bridge, J. A. (2009). Epidemiology of youth suicide and suicidal behaviour. Current Opinion in Pediatrics., 21(5), 613–619.
Chalfant, A., Rapee, R., & Carroll, L. (2007). Treating anxiety disorders in children with high-functioning autism spectrum disorders: A controlled trial. Journal of Autism and Developmental Disorders, 37, 1842–1857.
Crawford, J. R., & Henry, J. D. (2003). The depression anxiety stress scales (DASS): Normative data and latent structure in a large non-clinical sample. British Journal of Clinical Psychology, 42, 111–131.
Ehlers, S., & Gillberg, C. (1993). The epidemiology of Asperger Syndrome. Journal of Child Psychology and Psychiatry, 34, 1327–1350.
Ehring, T., Tuschen-Caffier, B., Schnṻlle, J., Fischer, S., & Gross, J. J. (2011). Emotion regulation and vulnerability to depression: Spontaneous versus instructed use of emotion suppression and reappraisal. Emotion, 10(4), 563–572.
Frith, U., & Firth, C. D. (2003). Development and neurophysiology of mentalizing. Philosophical Transactions of the Royal Society of London. Series B, 358, 459–473.
Garnett, M. S., Attwood, T., Peterson, C., & Kelly, A. B. (2013). Autism spectrum conditions among children and adolescents: Psychometric properties of a new profiling tool. Australian Journal of Psychology, 65, 206–213.
Gaynor, S. T., Lawrence, P. S., & Nelson-Gray, R. O. (2006). Measuring homework compliance in cognitive-behavioral therapy for adolescent depression: Review, preliminary findings, and implications for theory and practice. Behavior Modification, 30, 647–672.
Gillberg, I. C., & Gillberg, C. (1989). Asperger syndrome: Some epidemiological considerations. A Research Note, Journal of Child Psychology and Psychiatry, 30, 631–638.
Gillberg, C., Gillberg, C., Rastam, M., & Wentz, E. (2001). The Asperger syndrome (and high-functioning autism) diagnostic interview (ASDI): A preliminary study for a new structured clinical interview. Autism, 5(1), 57–66.
Gmitrowiez, A., Szymczak, W., Kotlieka-Anezak, M., & Rabe-Jablonska, J. (2003). Suicidal ideation and suicide attempt in Polish adolescents: Is it a suicidal process? International Journal of Adolescent Medicine and Health, 15(2), 113–124.
Goldin, P. R., McRae, K., Ramel, W., & Gross, J. J. (2008). The neural bases of emtoion regulation: Reapprasial and suppression of negative emotion. Biological Psychiatry, 63, 577–586.
Green, J., Gilchrist, A., Burton, D., & Cox, A. (2000). Social and psychiatric functioning in adolescents with Asperger syndrome compared with conduct disorder. Journal of Autism and Developmental Disorders, 30(4), 279–293.
Gross, J. J., & John, O. P. (2003). Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. Journal of Personality and Social Psychology, 85(2), 348–362.
Gyurak, A., Goodkind, M. S., Madan, A., Kramer, J. H., Miller, B. L., & Levenson, R. W. (2009). Do tests of executive function predict ability to down-regulate emotions spontaneously and when instructed to suppress? Cognitive, Affective, and Behavioral Neuroscience, 9(2), 144–152.
Hair, J. F., Black, W. C., Babin, B. J., & Anderson, R. E. (2009). Multivariate data analyses (7th ed.). Upper Saddle River: Prentice Hall.
Hannon, G., & Taylor, E. P. (2013). Suicidal behaviour in adolescents and young adults with ASD: Findings from a systematic review. Clinical Psychology Review, 33(8), 1197–1204.
Hollon, S., & Kendall, P. (1980). Cognitive self-statements in depression: Development of an automatic thoughts questionnaire. Cognitive Therapy and Research, 4(4), 383–395.
IBM Corp. (2011). IBM SPSS statistics for Windows (version 20.0) [computer software]. Armonk, NY: IBM Corp.
Kazantzis, N., & Lampropoulos, G. K. (2002). Reflecting on homework in psychotherapy: What can we conclude from research and experience? Journal of Clinical Psychology, 58, 577–585.
Kim, J. A., Szatmari, P., Bryson, S. E., Streiner, D. L., & Wilson, F. J. (2000). The prevalence of anxiety and mood problems among children with autism and Asperger syndrome. Autism, 4, 117–132.
Kimhi, Y., Shoam-Kugelmas, D., Ben-Artzi, G. A., Ben-Moshe, I., & Bauminger-Zviely, N. (2014). Theory of mind and executive function in preschoolers with typical development versus intellectually able preschoolers with autism spectrum disorder. Journal of Autism and Developmental Disorders, 44, 2341–2354.
Locke, J., Ishijima, E. H., Kasari, C., & London, N. (2010). Loneliness, friendship quality, and the social networks of adolescents with high-functioning autism in an inclusive school setting. Journal of Research in Special Education Needs, 10(2), 74–81.
Lomax, R. G., & Hahs-Vaughn, D. L. (2012). An introduction to statistical concepts (3rd ed.). New York: Taylor & Francis Group.
Lord, C., Risi, S., Lambrecht, L., Cook, E. H., Leventhal, B. L., DiLabore, P. C., et al. (2000). The autism diagnostic observation schedule-generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders, 30(3), 205–223.
Lovibond, S. H., & Lovibond, P. F. (1995a). Manual for the depression anxiety stress scales (2nd ed.). Sydney: Psychology Foundation.
Lovibond, P. F., & Lovibond, S. H. (1995b). The structure of negative emotional states: Comparison of the depression anxiety stress scales (DASS) with the Beck depression and anxiety inventories. Behavioural Research and Therapy, 33(3), 335–343.
Lugnegård, T., Hallerbäck, M. U., & Gillberg, C. (2011). Psychiatric comorbidity in young adults with a clinical diagnosis of Asperger syndrome. Research in Developmental Disabilities, 32, 1910–1917.
Mausbach, B. T., Moore, R., Roesch, S., Cardenas, V., & Patterson, T. L. (2010). The relationship between homework compliance and therapy outcomes: An updated meta-analysis. Cognitive Therapy and Research, 34, 429–438.
Mazefsky, C. A., Herrington, J., Siegel, M., Scarpa, A., Maddox, B. B., Scahill, L., & White, S. W. (2013). The role of emotion regulation in autism spectrum disorder RH: Emotion regulation in ASD. Journal of the American Academy of Child and Adolescent Psychiatry, 52(7), 679–688.
Mazefsky, C. A., Kao, J., & Oswald, D. P. (2011). Preliminary evidence suggesting caution in the use of psychiatric self-report measures with adolescents with high-functioning autism spectrum disorders. Research in Autism Spectrum Disorders, 5, 164–174.
Mazefsky, C. A., & White, S. W. (2014). Emotion regulation: Concepts & practice in autism spectrum disorder. Child and Adolescent Psychitric Clinics of North America, 23(1), 15–24.
McGillivray, J. A., & Evert, H. T. (2014). Group cognitive behavioural therapy program shows potential in reducing symptoms of depression and stress among young people with ASD. Journal of Autism and Developmental Disorders, 44, 2041–2051.
McRae, K., Gross, J. J., Weber, J., Robertson, E. R., Sokol-Hessner, P., Ray, R. D., et al. (2012). The development of emotion regulation: An fMRI study of cognitive reappraisal in children, adolescents and young adults. Social Cognitive and Affective Neuroscience, 7(1), 11–22.
Moriguchi, Y., Ohnishi, T., Lane, R. D., Maeda, M., Mori, T., Nemoto, K., et al. (2006). Impaired self-awareness and theory of mind: An fMRI study of mentalizing in alexithymia. Neuroimage, 32, 1472–1482.
Psychological Corporation. (1999). Wechsler abbreviated scale of intelligence (WASI) manual. San Antonio: Author
Qualtrics. (2013). Qualtrics (version 37892) [computer software]. Provo: Qualtrics.
Ree, M. J., & Craigie, M. A. (2007). Outcomes following mindfulness-based cognitive therapy in a heterogeneous sample of adult outpatients. Behaviour Change, 24(2), 70–86.
Resch, F., Parzer, P., & Romuald, B. (2008). Self-mutilation and suicidal behaviour in children and adolescents: Prevalence and psychosocial correlates: Results of the BELLA study. European Child and Adolescents Psychiatry, 17(1), 92–98.
Richter, P., Werner, J., Heerlein, A., Kraus, A., & Sauer, H. (1998). On the validity of the Beck depression inventory. A Review. Psychopathology, 31(3), 160–168.
Roberts, N. A., Levenson, R. W., & Gross, J. J. (2008). Cardiovascular costs of emotion suppression cross ethnic lines. International Journal of Psychophysiology, 70, 82–87.
Ronk, F. R., Korman, J. R., Hooke, G. R., & Page, A. C. (2013). Assessing clinical significance of treatment outcomes using the DASS-21. Psychological Assessment, 25(4), 1103–1110.
Ruwaard, J., Schrieken, B., Schrijver, M., Broeksteeg, J., Dekker, J., Vermeulen, H., & Lange, A. (2009). Standardized web-based cognitive behavioural therapy of mild to moderate depression: A randomized controlled trial with a long-term follow-up. Cognitive Behaviour Therapy, 38(4), 206–221.
Samson, A. C., Huber, O., & Gross, J. J. (2012). Emotion regulation in Asperger’s syndrome and high-functioning autism. Emotion, 12(4), 659–665.
Scheeren, A. M., de Rosnay, M., Koot, H. M., & Begeer, S. (2013). Rethinking theory of mind in high-functioning autism spectrum disorder. The Journal of Child Psychology and Psychiatry, 54(6), 628–635.
Sofronoff, K., Attwood, T., & Hinton, S. (2005). A randomised control trial of a CBT intervention for anxiety in children with Asperger syndrome. Journal of Child Psychology and Psychiatry, 46(11), 1152–1160.
Sterling, L., Dawson, G., Estes, A., & Greenson, J. (2008). Characteristics associated with presence of depressive symptoms in adults with autism spectrum disorder. Journal of Autism and Developmental Disorders, 38, 1011–1018.
Strang, J. F., Kenworthy, L., Daniolos, P., Case, L., Wills, M. C., Martin, A., & Wallace, G. L. (2012). Depression and anxiety symptoms in children and adolescents with autism spectrum disorders without intellectual disability. Research in Autism Spectrum Disorders, 6, 406–412.
Ung, D., Selles, R., Small, B. J., & Storch, E. A. (2015). A systematic review and meta-analysis of cognitive-behavioral therapy for anxiety in youth with high-functioning Autism spectrum disorders. Child Psychiatry and Human Development, 46, 533–547.
Van Roekel, E., Scholte, R. H. J., & Didden, R. (2010). Bullying among adolescents with autism spectrum disorders: Prevalence and perception. Journal of Autism and Developmental Disorders, 40, 63–73.
Whisman, M. A., Perez, J. E., & Ramel, W. (2000). Factor structure of the Beck depression inventory second edition (BDI-II) in a student sample. Journal of Clinical Psychology, 58(4), 545–551.
Zablotsky, B., Bradshaw, C. P., Anderson, C., & Law, P. A. (2013). Journal of Developmental and Behavioural Pediatrics, 34, 1–8.
Acknowledgments
This project would like to acknowledge Tony Attwood and Michelle Garnett’s assistance to the project. Attwood and Garnett developed the Exploring Depression programme evaluated in this paper, and conducted two full day workshops to train psychologists to run the groups. This project was conducted as part of Damian Santomauro’s PhD dissertation and was funded by an Australian Postgraduate Award scholarship.
Author Contributions
All authors contributed to conception and design of this study. DS managed participant recruitment, running of the groups, and statistical analyses. KS and JS provided supervision for the groups. DS wrote the initial draft and all coauthors provided input on subsequent versions.
Author information
Authors and Affiliations
Corresponding author
Appendix
Rights and permissions
About this article

Cite this article
Santomauro, D., Sheffield, J. & Sofronoff, K. Depression in Adolescents with ASD: A Pilot RCT of a Group Intervention. J Autism Dev Disord 46, 572–588 (2016). https://doi.org/10.1007/s10803-015-2605-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-015-2605-4