
Abstract
The Generation R Study is a population-based prospective cohort study from fetal life until young adulthood. The study is designed to identify early environmental and genetic causes of normal and abnormal growth, development and health during fetal life, childhood and adulthood. The study focuses on four primary areas of research: (1) growth and physical development; (2) behavioural and cognitive development; (3) diseases in childhood; and (4) health and healthcare for pregnant women and children. In total, 9,778 mothers with a delivery date from April 2002 until January 2006 were enrolled in the study. General follow-up rates until the age of 4 years exceed 75%. Data collection in mothers, fathers and preschool children included questionnaires, detailed physical and ultrasound examinations, behavioural observations, and biological samples. A genome wide association screen is available in the participating children. Regular detailed hands on assessment are performed from the age of 5 years onwards. Eventually, results forthcoming from the Generation R Study have to contribute to the development of strategies for optimizing health and healthcare for pregnant women and children.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The Generation R Study is a population-based prospective cohort study from fetal life until young adulthood. The study is designed to identify early environmental and genetic causes of normal and abnormal growth, development and health during fetal life, childhood and adulthood. The study focuses on four primary areas of research: (1) growth and physical development; (2) behavioural and cognitive development; (3) diseases in childhood; and (4) health and healthcare for pregnant women and children. The background and specific lines of investigation have been described in detail previously [1–3]. The main outcomes and determinants are presented in Tables 1 and 2. The general aims of the study are: (1) To describe normal and abnormal growth, development and health from fetal life until young adulthood; (2) To identify biological, environmental and social determinants of normal and abnormal growth, development and health from fetal life until young adulthood; (3) To develop and evaluate strategies for prevention and early identification of groups at risk.
Special interest is in exploring the role of early environmental exposures and genetic variants in pathways leading to common diseases during fetal life, childhood and adulthood, of which various examples have been published in this journal [4–15].
Main outcomes include risk factors for cardiovascular disease, type 2 diabetes, obesity, asthma, psychopathology and riks factors such as impaired physical activity [16–70]. Results forthcoming from the Generation R Study have to contribute to the development of strategies for optimizing health and healthcare for pregnant women and children.
Study area
The Generation R Study is conducted in Rotterdam, the second largest city in the Netherlands. Rotterdam is situated in the Western part of the Netherlands on almost 80 km south from Amsterdam, the capital of the Netherlands. The total population consists of about 600,000 inhabitants of almost 150 different ethnicities. The study area is well defined by postal codes and covers more than half of the cities inhabitants (almost 350,000 inhabitants) [16]. The largest ethnic groups in this population are the Dutch (56%), Surinamese (9%), Turkish (7%), Moroccan (6%), Dutch Antillean (3%) and Cape Verdian (3%) groups [2]. The percentages of the non-Dutch groups are higher in younger age groups [2]. The number of children born in this study area is about 4,300 per year. Measurements in the prenatal phase of the study were conducted in two well-equipped research centers in the study area, with a close collaboration with midwives and hospitals. In the preschool period, detailed measurements were conducted in a dedicated research center in the Erasmus Medical Center—Sophia Children’s Hospital and routine care data were collected in five hospitals and sixteen child health centers located in this area.
Study design
Overview
The Generation R Study is a population-based prospective cohort study from fetal life until young adulthood. Mothers with a delivery date between April 2002 and January 2006 were eligible. Extensive assessments have been carried out in mothers and fathers and are currently performed in their children (Tables 3, 4). Assessments in pregnancy were planned in early pregnancy (gestational age < 18 weeks), mid-pregnancy (gestational age 18–25 weeks) and late pregnancy (gestational age > 25 weeks). These measurements are considered as first, second and third trimester measurements. The fathers were assessed once in pregnancy. The children form a prenatally recruited birth-cohort that will be followed until young adulthood. In the preschool period, which in the Netherlands refers to the period from birth to the age of 4 years, data collection was performed by a home-visit at the age of 3 months, questionnaires at the ages of 2, 6, 12, 18, 24, 30, 36 and 48 months and visits to the routine child health centres at the ages 2, 3, 4, 6, 11, 14, 18, 24, 30, 36 and 45 months (Table 4). Additional, more detailed assessments of fetal and postnatal growth and development have been conducted in a randomly selected subgroup of Dutch children and their parents at a gestational age of 32 weeks and postnatally at the ages of 1.5, 6, 14, 24, 36 and 48 months (Tables 3, 4).
Dutch is defined as two parents and four grandparents born in the Netherlands. From the age of 5 years onwards, regular detailed hands on assessment are performed in all children and their parents in a well-equipped, dedicated research center.
Eligibility and enrolment
Eligible mothers were those who were resident in the study area at their delivery date and had a delivery date from April 2002 until January 2006. We aimed to enroll mothers in early pregnancy (gestational age < 18 weeks) but enrolment was allowed until birth of their child. Midwives and obstetricians informed eligible mothers about the study at their first prenatal visit in routine care, handed out the information package and asked these mothers to make an appointment for the first ultrasound examination. The study staff contacted these mothers by phone for additional information about the study and in person at the ultrasound examination to obtain informed consent. Mothers who were not approached in pregnancy, were approached and enrolled in the first months after birth of their child when newborns visit the routine child health centers [2]. The fathers were not approached directly by the study staff but the mothers were informed about the importance of involvement of the fathers in the study.
Study cohort
Parents
In total, 9,778 mothers were enrolled in the study (Fig. 1). Of these mothers, 91% (n = 8,880) was enrolled in pregnancy. Only partners from mothers enrolled in pregnancy were invited to participate. In total, 71% (n = 6,347) of all fathers was enrolled. The general characteristics of the mothers and fathers are presented in Table 5. Of all participating mothers, enrolment was in early pregnancy in 69% (n = 6,691), in mid-pregnancy in 19% (n = 1,918), in late pregnancy in 3% (n = 271) and at birth of their child in 9% (n = 898). Of all pregnant women enrolled, 94% (n = 8,356), 6% (n = 516) and 0.1% (n = 8) were first, second and third pregnancies in the study, respectively. A total of 1,232 pregnant women and their children were enrolled in the subgroup for additional detailed studies. Ethnicity of participating mothers and partners was defined according the classification of Statistics Netherlands [71, 72]. The largest ethnic groups were the Dutch, Surinamese, Turkish and Moroccan groups. The ethnic distribution differed only moderately from that of the population in the study area [71]. Mean household income in Rotterdam is about €1600 per month and the percentage subjects with a secondary or higher education level in Rotterdam is 56% [71]. The educational level of participating mothers and their partners was classified in groups according to the classification of Statistics Netherlands [73]. Ethnic background, educational level and occupational status are of major interest and are studied as determinants of health and behavioural outcomes [74–91]. Both household income and highest followed educational level in mothers and fathers in the study cohort suggest a selection towards a higher socioeconomic status than in the whole study. This pattern is similar as in other large scale cohort studies [92]. However, differences between the population and cohort characteristics may also be due to selective missing values of ethnicity and socio-economic status in the questionnaires. Socio-economic status is related to various perinatal and postnatal health outcomes and of major interest in the study [93–109].

Enrolment and measurements until the age of 4 years
Children at birth and overall response
Among the live births, 51% were male and 49% female. These percentages are similar to the population figures in the Netherlands and in Rotterdam [71]. The percentages of children born preterm or with low birth weight are smaller than expected on the basis of the population figures. This seems to reflect a selection toward a relative more healthy study population. Estimation of the precise number of eligible pregnant women in the study area is difficult since there is no satisfactory registry of pregnancies. Therefore, it was not attempted to identify overall response rates of pregnant women. Since the children form a prenatally recruited birth-cohort, the overall response of the study has been established at birth and is 61%.
Participation in postnatal follow up studies
As described above, 9,778 mothers were enrolled in the study and gave birth to 9,745 known live born children. The logistics of the postnatal follow up studies were embedded in the municipal routine child care system and restricted to the study area. In total 1,163 children lived outside this definite study area at birth and were therefore not approached for the postnatal follow up studies during the preschool period. Of the remaining 8,582 children, 689 (8%) mothers did not give consent for the postnatal phase of the study leaving 7,893 children for the postnatal follow-up studies. Reasons for non-participation in the postnatal follow up studies were primarily time restrictions or plans for moving from the study area. Of the total of 7,893 mothers, 598 (7.5%) gave a restricted consent and did not want to participate in the questionnaire studies. In total 7588 (78%) children or their parents participated in at least one measurement during the preschool period, of whom 6845 (90%) completed at least one questionnaire.
Data collection in the prenatal phase
Physical examinations
Physical examinations were planned at each visit in early pregnancy, mid-pregnancy and late pregnancy and included height, weight and blood pressure measurements of both parents. Overall response rates for these specific measurements in mothers and fathers are similar as the visit percentages presented in Fig. 1. Since there was a wide range of gestational age at each visit, these measurements are used in the analyses as gestational age adjusted measurements [110].
Questionnaires
Mothers received four postal questionnaires and father received one postal questionnaire in the prenatal phase (Table 3). All questionnaires are available in three languages (Dutch, English and Turkish). If needed, further support for verbal translation of questionnaires is available in Arabic, Portuguese and French. Each questionnaire comprises about 25 pages and takes about 30–45 min to be completed [2]. Topics in these questionnaires were:
-
Mother 1: medical and family history, previous pregnancies, quality of life, life style habits, housing conditions, ethnicity, educational level;
-
Mother 2: diet, including macronutrients and micronutrients;
-
Mother 3: current pregnancy, quality of life, life style habits, psychopathology;
-
Mother 4: current pregnancy, quality of life, life style habits, working conditions, household income, self-esteem;
-
Father: medical history, family history, life style habits, educational level, psychopathology.
Overall response rates for these questionnaires varied from 77 to 91% (Fig. 1). However, the response rates of specific questions may be lower due to missing values within questionnaires.
Fetal ultrasound examinations
Fetal ultrasound examinations were performed at each prenatal visit. Overall response rates for these ultrasound examinations were in general similar to the visit percentages given in Fig. 1. These ultrasound examinations were used for both establishing gestational age and assessing fetal growth patterns. These methods have previously been described in detail [111, 112]. Establishing gestational age by using the first day of the last menstrual period is not reliable for a variety of reasons including the large number of women who do not know their exact date, have irregular menstrual cycles or amenorrhea, use oral contraceptive pills or bleed in early pregnancy [113]. Using fetal ultrasound data such as crown-rump length or biparietal diameter for pregnancy dating seems to overcome these problems but does not allow growth studies of these measurements since no growth variability between subjects is assumed. Pregnancy dating-curves have been derived in a subsample of the cohort including subjects with complete data on both the first day of the last menstrual period and crown-rump length or biparietal diameter and used to date the gestational age [111]. Subsequently, longitudinal curves of all fetal growth measurements (head circumference, biparietal diameter, abdominal circumference and femur length) were created resulting in standard deviation scores for all of these specific growth measurements. Various sociodemographic and lifestyle related determinant seems to affect these fetal growth and birth outcomes [114–119]. Also, specific fetal growth patterns seem to be associated with outcomes in childhood [120–123]. We have demonstrated in a subgroup study among mothers with a known and reliable last menstrual period, that various life style related factors affect first trimester growth [124]. Placental haemodynamics including resistance indices of the uterine and umbilical arteries have been assessed in second and third trimester [125]. Detailed measurements of fetal brain, cardiac and kidney development have been performed in the subcohort [126–129].
Pregnancy complications and outcomes
The obstetric records of mothers have been looked up in the hospitals and mid-wife practices. Specialists in the relevant field code items in these records, and used for validation studies for maternal reported data [130, 131]. The major pregnancy outcomes, including live births, induced abortion fetal or perinatal loss, pregnancy induced hypertension, preeclampsia, and gestational diabetes are known in 99% of all enrolled mothers. These outcomes are related to various exposures of interest [132–148]. In all children known to be born alive, information about sex, birth weight and gestational age is available. Currently, efforts are made to link the Generation R dataset to existing national databases for pregnancy and the neonatal period [149, 150].
Biological samples
Blood samples were collected in early and mid-pregnancy and at birth. Procedures for collection, processing and storage of biological samples have been described previously in detail [151]. The planned amounts of venous blood taken were 35 and 20 ml in early pregnancy and mid-pregnancy, respectively, from the mother and 10 ml from father. At delivery, 30 ml cord blood was collected. Blood samples are currently available for 97, 83 and 67% of the participating mothers, partners and children, respectively. Due to several clinical complications in mother and child, it was not always possible to collect cord blood. Subsequently, availability rates of cord blood samples in children born preterm or with low birth weight are lower than expected. Plasma and serum samples has been distributed in small aliquots (each 250 μl) and stored at −80°C. Maternal and cord blood samples have been used for measuring dietary biomarkers (folate, homocystein, total vitamin B12, free vitamin B12) levels; angiogenesis biomarkers (soluble fms-like tyrosine kinase-1 (sFlft-1), Placental growth factor (PlGF)); thyroid hormone levels (thyroid-stimulating hormone (TSH), free thyroxine (FT4)) and thyroid antibody levels, inflammation markers (high-sensitivity C-reactive protein (hs CRP); and celiac disease and Helicobacter Pylori antibodies [152–154]. Urine samples of mothers have been collected from February 2004 until November 2005 and are stored for future measurements. Response rates for these urine samples are 85, 97 and 96% in early, mid- and late pregnancy respectively. These urine samples are used for measurement of several environmental exposures, and metabolites. Urine samples have been used for measurement of Chlamydia, and pesticides, bisphenol A, and phthalates levels [155, 156].
DNA and genome wide association studies
DNA from both parents (whole blood) and children (cord blood) has been extracted, normalised and plated and is currently used for several genotype studies. A genome wide association scan (GWAS) using the Illumina 610 Quad platform is available for the participating children. For genotyping, we used the infrastructure of the Genetic Laboratory of the Department of Internal Medicine (www.glimdna.org) that was also used for creation of the GWAS datasets of the Rotterdam Study, a prospective cohort study among more than 10,000 adults [157, 158]. The GWAS dataset underwent a stringent QC process whereby Individuals with low call rates or sex mismatches were excluded, and SNPs with low call rates were excluded. In addition, ethnic composition of the sample was estimated by Identity-By-State Analysis, using Principal Component Analysis, and cryptic familial relationships were identified through Identity-By-Descent analysis]. To maximize genome coverage and allow inter-study comparisons, we used MACH (version 1.0.15) software to impute genotypes at each of the 2.5 million autosomal CEPH HapMap II (release 22) SNPs for Europeans and European-Americans [159]. Criteria such as high levels of missing data (SNP call rate < 98%), highly significant departures from Hardy-Weinberg equilibrium (P < 1.10–6), or low Minor Allele Frequencies (MAF < 1%) were used to determine which SNPs to include in the imputation step. Most GWAS analyses are strongly embedded in the recently started Early Growth Genetics (EGG) Consortium and Early Genetics and Longitudinal Epidemiology (EAGLE) Consortium, in which several birth cohort studies combine their GWAS efforts focused on multiple outcomes in fetal life, childhood and adolescence [160, 161]. The power of large scale consortia has been shown previously [162–170]. Also, strategies for genetic scoring analyses are being developed to estimate predictive values of identified genetic variants [171, 172]. Although a GWAS is available in children, we use DNA from both children and parents for genotyping for candidate gene or replication studies [173–182]. Missing data in DNA samples in children will be collected by blood sampling or other methods at follow-up measurements.
Data collection in the first 4 postnatal years
Physical examinations
At the age of 3 months, home visits were performed to assess neuromotor development using an adapted version of Touwen’s Neurodevelopmental examination [183–185]. Information about growth (length (height), weight, head circumference) is collected at each visit to the routine child health centres in the study area using standardized procedures. These visits are planned at the ages 2, 3, 4, 6, 11, 14, 18, 24, 30, 36 and 48 months. Response rates for these visits vary between 70 and 97% [186].
Questionnaires
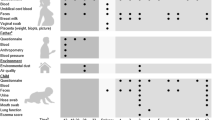
During the preschool period, mothers receive 8 questionnaires and fathers receive one questionnaire. Each questionnaire comprises about 25 pages. Items included in these questionnaires and their references are demonstrated in Table 6 [187–223]. Response rates based on the number of send questionnaires are showed in Fig. 1. Due to logistical constraints and implementation of questionnaires after the first group of children reached a certain age, not all children received each questionnaire. Thus, although response rates may be similar, the absolute number of completed questionnaires could differ between different ages. Response rates presented in Fig. 1 are based on the number of send questionnaires.
Hands on assessments and observations in subgroup
During the preschool period, children participating in the subgroup studies have been invited six times to a dedicated research center. Measurements at these visits included physical examinations (height, weight, head circumference, skinfold thickness and waist- hip ratio, Touwen’s Neurodevelopmental Examination at the ages of 1.5, 6, 14, and 24 months) and ultrasound examinations (brain structures at 1.5 months and cardiac and kidney structures at the ages of 1.5, 6 and 24 months, abdominal fat at the age of 24 months) [224–237]. Dual × Energy Absorptiometry (DXA) scanning was performed in a subgroup of children at the age of 6 months [238]. Similarly Fractional Exhaled Nitric Oxide (FeNO) has been measured in only 50% of all children at the ages of 6 and 24 months. Blood pressure was measured at the age of 24 months [239]. Observations of parent-child interaction and behaviour, such as executive function, heart rate variability, infant-parent attachment, moral development, and compliance with mother and child have been performed at the ages of 14, 36 and 48 months and with father and child at the age of 48 months [240, 241]. Biological materials have been collected, including bacterial colonization measured by nasal- and nasopharyngeal swabs at the ages of 1.5, 6, 14 and 24 months, cortisol day rhythm measured by repeated salivary samples at the age of 14 months and, if parents give consent, blood samples at the ages of 6, 14 and 24 months [242–251]. Response rates for these blood samples are about 30%, mainly because of lack of parental consent.
Measurements from the age of 5 years
From the age of 5 years onwards, we plan to invite all participating children to a well-equipped and dedicated research center in the Erasmus Medical Center—Sophia Children’s Hospital every 3 years. Currently, all children aged 5–6 years are invited to participate in hands on measurements, behavioural observations and biological sample collection. The total visit takes about 2.5 h and all measurements are grouped in thematic 20 min blocks. These measurements are focused on several health outcomes including asthma, bacterial carriage, infectious diseases, behaviour and cognition, body composition, eye and tooth development, heart and vascular development, kidney growth and function, and obesity. These measurements will be used as both outcomes and determinants for health outcomes in later life. Cardiovascular, metabolic and bone measurements are also conducted in mothers. Clinically relevant results are discussed with the parents and, if needed, children or mothers are referred to their general practitioner, paediatrician or other relevant health care provider. All children are expected to have visited our research center in summer 2011. Currently ideas for follow up studies including detailed imaging studies using Magnetic Resonance Imaging (MRI), are discussed and tested in subgroups.
Ethical issues
The general design, all research aims and the specific measurements in the Generation R Study have been approved by the Medical Ethical Committee of the Erasmus Medical Center, Rotterdam. New measurements will only be embedded in the study after approval of the Medical Ethical Committee. Participants are asked for their written informed consent for the four consecutive phases of the study (prenatally, birth to 4 years, 4–16 years, and from 16 years onwards). At the start of each phase, mothers and their partners received written and oral information about the study. Even with consent of the parents, when the child is not willing to participate actively, no measurements are performed.
Follow up and retention strategies
Thus far, loss to follow up seems to be limited. Major efforts are made to keep the children and parents involved in the study and to minimize loss to follow up to prevent bias in future studies. Several strategies have been implemented and are currently part of the study design:
-
Addresses: new addresses of participants, which are known by the municipal health service are forwarded to the study staff;
-
Newsletters: participants receive four newsletters per year, in which several results of the study are presented and explained, questions of participants are answered and new research initiatives are presented;
-
Presents and discounts: all children who visit our research center receive small presents. Also, discount offers are regularly part of the newsletter;
-
Transport costs: all costs for transport and parking related to visits to the research center are paid by Generation R;
-
Reminders for questionnaires: when the questionnaire has not been returned within 3 weeks, a kind reminder letter is send to the parents. After 6 weeks, when the questionnaire has still not been returned, the parents receive a phone call. If necessary, help for completing the questionnaire is offered and the importance of filling in the questionnaire is explained once more during this phone call;
-
Individual feedback: if clinically relevant, all results of hands-on measurements are discussed with the parents at the visit. If necessary, follow up appointments with the general practitioner or pediatrician are planned;
-
Support for ethnic minorities: all study materials such as questionnaires, newsletters, website, and information folders are available in three languages (Dutch, English, and Turkish). Furthermore, staff from different ethnic minorities is available and able to verbally translate these materials into Arabic, French and Portuguese. With this, the study staff is able to communicate to all participants.
-
Care-cases: children and parents who showed low response rates for different measurements, showed difficulties in completing questionnaires or require additional explanation or support are considered as care-cases. Care—cases have a more individual based approach and are pro-actively contacted by one dedicated member of the study staff.
New methods for contacting participants, which have been used in other more recently started studies, including use of internet, sms and e-mail, are currently being explored [92, 252–262].
Data management and privacy protection
Data collected by measurements in the research centers are directly entered onto written forms and into the electronic database. Data collected by questionnaires are scanned and manually entered into an electronic database by a commercial bureau. Random samples of all questionnaires are double checked by study staff members to monitor the quality of this manual data entry process. The percentage of mistakes is kept as low as possible and does not exceed 3% per questionnaire. Open text fields are entered into the electronic database exactly as they are filled in on the questionnaires. In a secondary stage, these open text fields are cleaned and coded by a specialist in the relevant field. All measurements are centrally checked by examination of the data including their ranges, distributions, means, standard deviations, outliers and logical errors. Data outliers and missing values are checked on the original forms and might be imputed and subsequent appropriate statisticial techniques are used [263–274]. The data of one specific measurement are only distributed for analyses after data collection and preparation is completed for that measurement for the whole cohort. Datasets needed for answering specific research questions are centrally built from different databases. All information in these datasets that enables identification of a particular participant (including identification number used for the logistics of the study, names and dates) is excluded before distribution to the researchers. The datasets for researchers include subject unique identification numbers that enable feedback about one subject to the data manager but do not enable identification of that particular subject.
Statistical power
Due to expected missing values and loss to follow-up, most analyses in the study are not based on data in all subjects. Therefore, power calculations demonstrated in Tables 7 and 8 are based on 7,000 subjects in the whole cohort and 700 subjects in the focus cohort. Table 8 demonstrates that for a normally distributed continuous outcome it is possible to detect with a type I error of 5% and a type II error of 20% (power 80%) a difference of 0.11 SD in the whole cohort and of 0.35 SD in the focus cohort if 10% of all subjects has the relevant exposure. Table 8 presents for dichotomous outcomes that with the same type I and II errors, it is possible to detect a relative risk of 1.39 in the whole cohort and of 2.48 in the focus cohort if 10% of all subjects has the relevant exposure and the 1 year incidence of the outcome of interest is 10%. Rates of most dichotomous environmental and genetic exposures in the Generation R Study are expected to vary generally between 10 and 20%. The presented power calculations are rather conservative since most studies will assess the effects of continuously instead of dichotomous measured exposures and studies may be focused on outcomes collected in more than only 1 year. Furthermore, the Generation R Study has a large number of measurements repeated over time, which may increase the accuracy of measuring the true underlying value and may thereby increase the statistical power for these measurements.
Collaboration
The Generation R Study is conducted by several research groups from the Erasmus Medical Center in close collaboration with the Erasmus University Rotterdam and the Municipal Health Service Rotterdam area. Since the data collection is still ongoing and growing, the number of collaborating research groups in and outside the Netherlands is expected to increase in the coming years. The study has an open policy in regard to collaboration with other research groups. Request for collaboration should primarily be pointed to Vincent Jaddoe (v.jaddoe@erasmusmc.nl). These requests are discussed in the Generation R Study Management Team regarding their study aims, overlap with ongoing studies, logistic consequences and financial contributions. After approval of the project by the Generation R Study Management Team and the Medical Ethical Committee of the Erasmus Medical Center, the collaborative research project is embedded in one of the four research areas supervised by the specific principal investigator.
References
Hofman A, Jaddoe VW, Mackenbach JP, Moll HA, Snijders RF, Steegers EA, Verhulst FC, Witteman JC, Büller HA. Growth, development and health from early fetal life until young adulthood: the Generation R Study. Paediatr Perinat Epidemiol. 2004;18:61–72.
Jaddoe VW, van Duijn CM, van der Heijden AJ, Mackenbach JP, Moll HA, Steegers EA, Tiemeier H, Uitterlinden AG, Verhulst FC, Hofman A. The Generation R Study: design and cohort update until the age of 4 years. Eur J Epidemiol. 2008;23(12):801–11.
Jaddoe VW. Fetal nutritional origins of adult diseases: challenges for epidemiological research. Eur J Epidemiol. 2008;23(12):767–71.
Lawlor DA, Batty GD, Clark H, McIntyre S, Leon DA. Association of childhood intelligence with risk of coronary heart disease and stroke: findings from the Aberdeen Children of the 1950s cohort study. Eur J Epidemiol. 2008;23(10):695–706.
Lawlor DA, Cooper AR, Bain C, Davey Smith G, Irwin A, Riddoch C, et al. Associations of birth size and duration of breast feeding with cardiorespiratory fitness in childhood: findings from the avon longitudinal study of parents and children (ALSPAC). Eur J Epidemiol. 2008;23(6):411–22.
Nguyen QM, Srinivasan SR, Xu JH, Chen W, Berenson GS. Influence of childhood parental history of type 2 diabetes on the pre-diabetic and diabetic status in adulthood: the Bogalusa heart study. Eur J Epidemiol. 2009;24(9):537–9.
Osler M, Lund R, Kriegbaum M, Andersen AM. The influence of birth weight and body mass in early adulthood on early coronary heart disease risk among Danish men born in 1953. Eur J Epidemiol. 2009;24(1):57–61.
Pearce MS, Relton CL, Parker L, Unwin NC. Sex differences in the association between infant feeding and blood cholesterol in later life: the Newcastle thousand families cohort study at age 49–51 years. Eur J Epidemiol. 2009;24(7):375–80.
Rask CU, Olsen EM, Elberling H, Christensen MF, Ornbol E, Fink P, et al. Functional somatic symptoms and associated impairment in 5–7-year-old children: the Copenhagen child cohort 2000. Eur J Epidemiol. 2009;24(10):625–34.
Rzehak P, Sausenthaler S, Koletzko S, Bauer CP, Schaaf B, von Berg A, et al. Period-specific growth, overweight and modification by breastfeeding in the GINI and LISA birth cohorts up to age 6 years. Eur J Epidemiol. 2009;24(8):449–67.
Alatupa S, Pulkki-Raback L, Hintsanen M, Ravaja N, Raitakari OT, Telama R, et al. School performance as a predictor of adulthood obesity: a 21-year follow-up study. Eur J Epidemiol. 2010;25(4):267–74.
Fraga AM, Fraga GP, Stanley C, Costantini TW, Coimbra R. Children at danger: injury fatalities among children in San Diego county. Eur J Epidemiol. 2010;25(3):211–7.
Ghasemi A, Zahediasl S, Azizi F. Nitric oxide and clustering of metabolic syndrome components in pediatrics. Eur J Epidemiol. 2010;25(1):45–53.
Heys M, Jiang C, Schooling CM, Zhang W, Cheng KK, Lam TH, et al. Is childhood meat eating associated with better later adulthood cognition in a developing population? Eur J Epidemiol. 2010;25(7):507–16.
Huisman M, Araya R, Lawlor DA, Ormel J, Verhulst FC, Oldehinkel AJ. Cognitive ability, parental socioeconomic position and internalising and externalising problems in adolescence: findings from two European cohort studies. Eur J Epidemiol. 2010;25(8):569–80.
Wiesbauer F, Blessberger H, Goliasch G, Holy EW, Pfaffenberger S, Tentzeris I, et al. Elevated risk of myocardial infarction in very young immigrants from former Yugoslavia. Eur J Epidemiol. 2009;24(11):691–6.
Vikan T, Johnsen SH, Schirmer H, Njolstad I, Svartberg J. Endogenous testosterone and the prospective association with carotid atherosclerosis in men: the Tromso study. Eur J Epidemiol. 2009;24(6):289–95.
Turin TC, Kita Y, Rumana N, Sugihara H, Morita Y, Tomioka N, et al. Incidence, admission and case-fatality of acute myocardial infarction: weekend versus weekday in a Japanese population: 16-year results from Takashima AMI registry (1988–2003). Eur J Epidemiol. 2009;24(2):93–100.
Andreotti G, Menashe I, Chen J, Chang SC, Rashid A, Gao YT, et al. Genetic determinants of serum lipid levels in Chinese subjects: a population-based study in Shanghai, China. Eur J Epidemiol. 2009;24(12):763–74.
Ruan L, Chen W, Srinivasan SR, Xu J, Toprak A, Berenson GS. Plasma homocysteine is adversely associated with glomerular filtration rate in asymptomatic black and white young adults: the Bogalusa heart study. Eur J Epidemiol. 2009;24(6):315–9.
Qi Y, Niu W, Zhu T, Zhou W, Qiu C. Synergistic effect of the genetic polymorphisms of the renin-angiotensin-aldosterone system on high-altitude pulmonary edema: a study from Qinghai-Tibet altitude. Eur J Epidemiol. 2008;23(2):143–52.
Regidor E, Astasio P, Calle ME, Martinez D, Ortega P, Dominguez V. The association between birthplace in different regions of the world and cardiovascular mortality among residents of Spain. Eur J Epidemiol. 2009;24(9):503–12.
Oliveira A, Barros H, Azevedo A, Bastos J, Lopes C. Impact of risk factors for non-fatal acute myocardial infarction. Eur J Epidemiol. 2009;24(8):425–32.
Niemiec P, Zak I, Wita K. The M235T polymorphism of the AGT gene modifies the risk of coronary artery disease associated with the presence of hypercholesterolemia. Eur J Epidemiol. 2008;23(5):349–54.
Merry AH, Boer JM, Schouten LJ, Feskens EJ, Verschuren WM, Gorgels AP, et al. Validity of coronary heart diseases and heart failure based on hospital discharge and mortality data in the Netherlands using the cardiovascular registry Maastricht cohort study. Eur J Epidemiol. 2009;24(5):237–47.
Mayer O Jr, Simon J, Plaskova M, Cifkova R, Trefil L. N-terminal pro B-type natriuretic peptide as prognostic marker for mortality in coronary patients without clinically manifest heart failure. Eur J Epidemiol. 2009;24(7):363–8.
Britton A, Malik M, Marmot M. The cardioprotective effects of alcohol consumption: does cardiac autonomic function play a role? Eur J Epidemiol. 2008;23(2):105–8.
Casiglia E, Schiavon L, Tikhonoff V, Bascelli A, Martini B, Mazza A, et al. Electrocardiographic criteria of left ventricular hypertrophy in general population. Eur J Epidemiol. 2008;23(4):261–71.
Chimonas T, Fanouraki I, Liberopoulos EN, Chimonas E, Elisaf M. Diverging trends in cardiovascular morbidity and mortality in a low risk population. Eur J Epidemiol. 2009;24(8):415–23.
Greiser KH, Kluttig A, Schumann B, Swenne CA, Kors JA, Kuss O, et al. Cardiovascular diseases, risk factors and short-term heart rate variability in an elderly general population: the CARLA study 2002–2006. Eur J Epidemiol. 2009;24(3):123–42.
Dorr M, Wallaschofski H, Friedrich N. Association of low total testosterone levels and prevalent carotid plaques: result of the study of health in Pomerania. Eur J Epidemiol. 2009;24(7):389–91.
Dragano N, Hoffmann B, Stang A, Moebus S, Verde PE, Weyers S, et al. Subclinical coronary atherosclerosis and neighbourhood deprivation in an urban region. Eur J Epidemiol. 2009;24(1):25–35.
Fallah N, Mohammad K, Nourijelyani K, Eshraghian MR, Seyyedsalehi SA, Raiessi M, et al. Nonlinear association between serum testosterone levels and coronary artery disease in Iranian men. Eur J Epidemiol. 2009;24(6):297–306.
Faramawi MF, Wildman RP, Gustat J, Rice J, Abdul Kareem MY. The association of the metabolic syndrome with QTc interval in NHANES III. Eur J Epidemiol. 2008;23(7):459–65.
Gasparrini A, Gorini G, Barchielli A. On the relationship between smoking bans and incidence of acute myocardial infarction. Eur J Epidemiol. 2009;24(10):597–602.
Gemes K, Ahnve S, Janszky I. Inflammation a possible link between economical stress and coronary heart disease. Eur J Epidemiol. 2008;23(2):95–103.
Hedlund E, Pehrsson K, Lange A, Hammar N. Country of birth and survival after a first myocardial infarction in Stockholm, Sweden. Eur J Epidemiol. 2008;23(5):341–7.
Thomas W, Birgit R, Edith S. Changing geographical distribution of diabetes mellitus type 1 incidence in Austrian children 1989–2005. Eur J Epidemiol. 2008;23(3):213–8.
Spencer EA, Pirie KL, Stevens RJ, Beral V, Brown A, Liu B, et al. Diabetes and modifiable risk factors for cardiovascular disease: the prospective million women study. Eur J Epidemiol. 2008;23(12):793–9.
Romon I, Jougla E, Balkau B, Fagot-Campagna A. The burden of diabetes-related mortality in France in 2002: an analysis using both underlying and multiple causes of death. Eur J Epidemiol. 2008;23(5):327–34.
Sabanayagam C, Shankar A, Li J, Pollard C, Ducatman A. Serum gamma-glutamyl transferase level and diabetes mellitus among US adults. Eur J Epidemiol. 2009;24(7):369–73.
Olafsdottir E, Aspelund T, Sigurdsson G, Thorsson B, Benediktsson R, Harris TB, et al. Unfavourable risk factors for type 2 diabetes mellitus are already apparent more than a decade before onset in a population-based study of older persons: from the age, gene/environment susceptibility-reykjavik study (AGES-Reykjavik). Eur J Epidemiol. 2009;24(6):307–14.
Pires de Sousa AG, Pereira AC, Marquezine GF, Marques do Nascimento-Neto R, Freitas SN, de C Nicolato RL, et al. Derivation and external validation of a simple prediction model for the diagnosis of type 2 diabetes mellitus in the Brazilian urban population. Eur J Epidemiol. 2009;24(2):101–9.
Manda SO, Feltbower RG, Gilthorpe MS. Investigating spatio-temporal similarities in the epidemiology of childhood leukaemia and diabetes. Eur J Epidemiol. 2009;24(12):743–52.
Balk L, Hoekstra T, Twisk J. Relationship between long-term coffee consumption and components of the metabolic syndrome: the Amsterdam growth and health longitudinal study. Eur J Epidemiol. 2009;24(4):203–9.
Aarts S, van den Akker M, van Boxtel MP, Jolles J, Winkens B, Metsemakers JF. Diabetes mellitus type II as a risk factor for depression: a lower than expected risk in a general practice setting. Eur J Epidemiol. 2009;24(10):641–8.
Bindraban NR, van Valkengoed IG, Mairuhu G, Koster RW, Holleman F, Hoekstra JB, et al. A new tool, a better tool? Prevalence and performance of the International Diabetes Federation and the National Cholesterol Education Program criteria for metabolic syndrome in different ethnic groups. Eur J Epidemiol. 2008;23(1):37–44.
Bloch F, Jegou D, Dhainaut JF, Rigaud AS, Coste J, Lundy JE, et al. Can metabolic abnormalities after a fall predict short term mortality in elderly patients? Eur J Epidemiol. 2009;24(7):357–62.
Heidemann C, Boeing H, Pischon T, Nothlings U, Joost HG, Schulze MB. Association of a diabetes risk score with risk of myocardial infarction, stroke, specific types of cancer, and mortality: a prospective study in the European prospective investigation into cancer and nutrition (EPIC)-Potsdam cohort. Eur J Epidemiol. 2009;24(6):281.
Corpeleijn E, Bakker SJ, Stolk RP. Obesity and impaired renal function: potential for lifestyle intervention? Eur J Epidemiol. 2009;24(6):275–80.
Klenk J, Nagel G, Ulmer H, Strasak A, Concin H, Diem G, et al. Body mass index and mortality: results of a cohort of 184, 697 adults in Austria. Eur J Epidemiol. 2009;24(2):83–91.
Reuser M, Bonneux L, Willekens F. The burden of mortality of obesity at middle and old age is small. A life table analysis of the US health and retirement survey. Eur J Epidemiol. 2008;23(9):601–7.
Setia MS, Quesnel-Vallee A, Abrahamowicz M, Tousignant P, Lynch J. Convergence of body mass index of immigrants to the Canadian-born population: evidence from the National Population Health Survey (1994–2006). Eur J Epidemiol. 2009;24(10):611–23.
Ahmed LA, Schirmer H, Bjornerem A, Emaus N, Jorgensen L, Stormer J, et al. The gender- and age-specific 10-year and lifetime absolute fracture risk in Tromso, Norway. Eur J Epidemiol. 2009;24(8):441–8.
Bruyere O, Varela AR, Adami S, Detilleux J, Rabenda V, Hiligsmann M, et al. Loss of hip bone mineral density over time is associated with spine and hip fracture incidence in osteoporotic postmenopausal women. Eur J Epidemiol. 2009;24(11):707–12.
de Luise C, Brimacombe M, Pedersen L, Sorensen HT. Chronic obstructive pulmonary disease and mortality following hip fracture: a population-based cohort study. Eur J Epidemiol. 2008;23(2):115–22.
Emaus N, Omsland TK, Ahmed LA, Grimnes G, Sneve M, Berntsen GK. Bone mineral density at the hip in Norwegian women and men-prevalence of osteoporosis depends on chosen references: the Tromso Study. Eur J Epidemiol. 2009;24(6):321–8.
Forsen L, Berntsen GK, Meyer HE, Tell GS, Fonnebo V. Differences in precision in bone mineral density measured by SXA and DXA: the NOREPOS study. Eur J Epidemiol. 2008;23(9):615–24.
Moayyeri A, Kaptoge S, Luben RN, Wareham NJ, Bingham S, Reeve J, et al. Estimation of absolute fracture risk among middle-aged and older men and women: the EPIC-Norfolk population cohort study. Eur J Epidemiol. 2009;24(5):259–66.
Yaegashi Y, Onoda T, Tanno K, Kuribayashi T, Sakata K, Orimo H. Association of hip fracture incidence and intake of calcium, magnesium, vitamin D, and vitamin K. Eur J Epidemiol. 2008;23(3):219–25.
Hugg T, Ruotsalainen R, Jaakkola MS, Pushkarev V, Jaakkola JJ. Comparison of allergic diseases, symptoms and respiratory infections between Finnish and Russian school children. Eur J Epidemiol. 2008;23(2):123–33.
Berg-Beckhoff G, Schuz J, Blettner M, Munster E, Schlaefer K, Wahrendorf J, et al. History of allergic disease and epilepsy and risk of glioma and meningioma (INTERPHONE study group, Germany). Eur J Epidemiol. 2009;24(8):433–40.
Graff-Iversen S, Anderssen SA, Holme IM, Jenum AK, Raastad T. Two short questionnaires on leisure-time physical activity compared with serum lipids, anthropometric measurements and aerobic power in a suburban population from Oslo, Norway. Eur J Epidemiol. 2008;23(3):167–74.
Jacobi D, Charles MA, Tafflet M, Lommez A, Borys JM, Oppert JM. Relationships of self-reported physical activity domains with accelerometry recordings in French adults. Eur J Epidemiol. 2009;24(4):171–9.
Lagerros YT. Physical activity—the more we measure, the more we know how to measure. Eur J Epidemiol. 2009;24(3):119–22.
Lagerros YT, Bellocco R, Adami HO, Nyren O. Measures of physical activity and their correlates: the Swedish national march cohort. Eur J Epidemiol. 2009;24(4):161–9.
Matthiessen J, Biltoft-Jensen A, Rasmussen LB, Hels O, Fagt S, Groth MV. Comparison of the Danish physical activity questionnaire with a validated position and motion instrument. Eur J Epidemiol. 2008;23(5):311–22.
Seabra AF, Mendonca DM, Goring HH, Thomis MA, Maia JA. Genetic and environmental factors in familial clustering in physical activity. Eur J Epidemiol. 2008;23(3):205–11.
Saleheen D, Zaidi M, Rasheed A, Ahmad U, Hakeem A, Murtaza M, et al. The Pakistan risk of myocardial infarction study: a resource for the study of genetic, lifestyle and other determinants of myocardial infarction in South Asia. Eur J Epidemiol. 2009;24(6):329–38.
Orsini N, Bellocco R, Bottai M, Hagstromer M, Sjostrom M, Pagano M, et al. Validity of self-reported total physical activity questionnaire among older women. Eur J Epidemiol. 2008;23(10):661–7.
Centre for Research and Statistics, Rotterdam (COS). 2005. http://www.cos.rotterdam.nl.
Statistics Netherlands. Allochtonen in Nederland 2004. Voorburg/Heerlen: Statistics Netherlands; 2004.
Troe EJ, Raat H, Jaddoe VW, Hofman A, Looman CW, Moll HA, Steegers EA, Verhulst FC, Witteman JC, Mackenbach JP. Explaining differences in birthweight between ethnic populations. The Generation R Study. BJOG. 2007;114:1557–65.
Statistics Netherlands. Standaard Onderwijsindeling 2003. Voorburg/Heerlen: Statistics Netherlands; 2004.
Troe EJ, Raat H, Jaddoe VW, Hofman A, Steegers EA, Verhulst FC, et al. Smoking during pregnancy in ethnic populations: the Generation R Study. Nicotine Tob Res. 2008;10(8):1373–84.
Chote AA, Koopmans GT, Redekop WK, de Groot CJ, Hoefman RJ, Jaddoe VW, et al. Explaining ethnic differences in late antenatal care entry by predisposing, enabling and need factors in the Netherlands. The Generation R Study. Matern Child Health J. 2010. doi:10.1007/s10995-010-0619-2.
Chote AA, de Groot CJ, Bruijnzeels MA, Redekop K, Jaddoe VW, Hofman A, et al. Ethnic differences in antenatal care use in a large multi-ethnic urban population in the Netherlands. Midwifery. 2009. doi:10.1016/j.midw.2009.07.008.
El Marroun H, Tiemeier H, Jaddoe VW, Hofman A, Mackenbach JP, Steegers EA, et al. Demographic, emotional and social determinants of cannabis use in early pregnancy: the Generation R Study. Drug Alcohol Depend. 2008;98(3):218–26.
Timmermans S, Jaddoe VW, Mackenbach JP, Hofman A, Steegers-Theunissen RP, Steegers EA. Determinants of folic acid use in early pregnancy in a multi-ethnic urban population in The Netherlands: the Generation R Study. Prev Med. 2008;47(4):427–32.
van Rossem L, Vogel I, Steegers E, Moll H, Jaddoe V, Hofman A, et al. Breastfeeding patterns among ethic minorities: the Generation R Study. J Epidemiol Community Health. 2009. doi:10.1136/jech.2009.095380.
Silva LM, Steegers EA, Burdorf A, Jaddoe VW, Arends LR, Hofman A, Mackenbach JP, Raat H. No midpregnancy fall in diastolic blood pressure in women with a low educational level: the Generation R Study. Hypertension. 2008;52:645–51.
Silva LM, Coolman M, Steegers EA, Jaddoe VW, Moll HA, Hofman A, et al. Low socioeconomic status is a risk factor for preeclampsia: the Generation R Study. J Hypertens. 2008;26(6):1200–8.
Silva L, Coolman M, Steegers E, Jaddoe V, Moll H, Hofman A, et al. Maternal educational level and risk of gestational hypertension: the Generation R Study. J Hum Hypertens. 2008;22(7):483–92.
Silva LM, Jansen PW, Steegers EA, Jaddoe VW, Arends LR, Tiemeier H, et al. Mother’s educational level and fetal growth: the genesis of health inequalities. Int J Epidemiol. 2010. doi:10.1093/ije/dyq069.
Jansen PW, Tiemeier H, Jaddoe VW, Hofman A, Steegers EA, Verhulst FC, et al. Explaining educational inequalities in preterm birth: the Generation R Study. Arch Dis Child Fetal Neonatal Ed. 2009;94(1):F28–34.
Jansen PW, Tiemeier H, Looman CW, Jaddoe VW, Hofman A, Moll HA, et al. Explaining educational inequalities in birthweight: the Generation R Study. Paediatr Perinat Epidemiol. 2009;23(3):216–28.
Jansen PW, Tiemeier H, Verhulst FC, Burdorf A, Jaddoe VW, Hofman A, et al. Employment status and the risk of pregnancy complications: the Generation R Study. Occup Environ Med. 2010;67(6):387–94.
Jansen PW, Raat H, Mackenbach JP, Jaddoe VW, Hofman A, Verhulst FC, et al. Socioeconomic inequalities in infant temperament: the Generation R Study. Soc Psychiatry Psychiatr Epidemiol. 2009;44(2):87–95.
Jansen PW, Raat H, Mackenbach JP, Jaddoe VW, Hofman A, van Oort FV, et al. National origin and behavioural problems of toddlers: the role of family risk factors and maternal immigration characteristics. J Abnorm Child Psychol. 2010. doi:10.1007/s10802-010-9424-z.
van Rossem L, Oenema A, Steegers EA, Moll HA, Jaddoe VW, Hofman A, et al. Are starting and continuing breastfeeding related to educational background? The Generation R Study. Pediatrics. 2009;123(6):e1017–27.
van Rossem L, Silva LM, Hokken-Koelega A, Arends LR, Moll HA, Jaddoe VW, et al. Socioeconomic status is not inversely associated with overweight in preschool children. J Pediatr. 2010. doi:10.1016/j.jpeds.2010.06.008.
Jacobsen TN, Nohr EA, Frydenberg M. Selection by socioeconomic factors into the Danish national birth cohort. Eur J Epidemiol. 2010;25(5):349–55.
Rodrigues T, Barros H. Maternal unemployment: an indicator of spontaneous preterm delivery risk. Eur J Epidemiol. 2008;23(10):689–93.
Quansah R, Gissler M, Jaakkola JJ. Work as a physician and adverse pregnancy outcomes: a Finnish nationwide population-based registry study. Eur J Epidemiol. 2009;24(9):531–6.
McFadden E, Luben R, Wareham N, Bingham S, Khaw KT. Occupational social class, risk factors and cardiovascular disease incidence in men and women: a prospective study in the European prospective investigation of cancer and nutrition in Norfolk (EPIC-Norfolk) cohort. Eur J Epidemiol. 2008;23(7):449–58.
McFadden E, Luben R, Khaw KT. Different measures of social class in women and mortality. Eur J Epidemiol. 2009;24(5):231–6.
McFadden E, Luben R, Wareham N, Bingham S, Khaw KT. How far can we explain the social class differential in respiratory function? A cross-sectional population study of 21, 991 men and women from EPIC-Norfolk. Eur J Epidemiol. 2009;24(4):193–201.
McFadden E, Luben R, Wareham N, Bingham S, Khaw KT. Occupational social class, educational level, smoking and body mass index, and cause-specific mortality in men and women: a prospective study in the European prospective investigation of cancer and nutrition in Norfolk (EPIC-Norfolk) cohort. Eur J Epidemiol. 2008;23(8):511–22.
Abatih E, Van Oyen H, Bossuyt N, Bruckers L. Variance estimation methods for health expectancy by relative socio-economic status. Eur J Epidemiol. 2008;23(4):243–9.
Heraclides A, Witte D, Brunner EJ. The association between father’s social class and adult obesity is not explained by educational attainment and an unhealthy lifestyle in adulthood. Eur J Epidemiol. 2008;23(8):573–9.
Lallukka T, Sarlio-Lahteenkorva S, Kaila-Kangas L, Pitkaniemi J, Luukkonen R, Leino-Arjas P. Working conditions and weight gain: a 28-year follow-up study of industrial employees. Eur J Epidemiol. 2008;23(4):303–10.
Laszlo KD, Janszky I, Ahnve S. Income and recurrent events after a coronary event in women. Eur J Epidemiol. 2008;23(10):669–80.
Schlaefer K, Schlehofer B, Schuz J. Validity of self-reported occupational noise exposure. Eur J Epidemiol. 2009;24(8):469–75.
Pfefferle PI, Kramer A. Helicobacter pylori-infection status and childhood living conditions are associated with signs of allergic diseases in an occupational population. Eur J Epidemiol. 2008;23(9):635–40.
Baste V, Riise T, Moen BE. Radiofrequency electromagnetic fields; male infertility and sex ratio of offspring. Eur J Epidemiol. 2008;23(5):369–77.
Muller-Riemenschneider F, Reinhold T, Berghofer A, Willich SN. Health-economic burden of obesity in Europe. Eur J Epidemiol. 2008;23(8):499–509.
Hublin C, Partinen M, Koskenvuo K, Silventoinen K, Koskenvuo M, Kaprio J. Shift-work and cardiovascular disease: a population-based 22-year follow-up study. Eur J Epidemiol. 2010;25(5):315–23.
Leclerc A. Shift-work and cardiovascular disease. Eur J Epidemiol. 2010;25(5):285–6.
Thomas C, Power C. Shift work and risk factors for cardiovascular disease: a study at age 45 years in the 1958 British birth cohort. Eur J Epidemiol. 2010;25(5):305–14.
Ay L, Kruithof CJ, Bakker R, Steegers EA, Witteman JC, Moll HA, et al. Maternal anthropometrics are associated with fetal size in different periods of pregnancy and at birth. The Generation R Study. BJOG. 2009;116(7):953–63.
Verburg BO, Steegers EA, De Ridder M, Snijders RJ, Smith E, Hofman A, Moll HA, Jaddoe VW, Witteman JC. New charts for ultrasound dating of pregnancy and assessment of fetal growth: longitudinal data from a population-based cohort study. Ultrasound Obstet Gynecol. 2008;31:388–96.
Verburg BO, Mulder PG, Hofman A, Jaddoe VW, Witteman JC, Steegers EA. Intra- and interobserver reproducibility study of early fetal growth parameters. Prenat Diagn. 2008;28(4):323–31.
Tunon K, Eik-Nes SH, Grottum P. A comparison between ultrasound and a reliable last menstrual period as predictors of the day of delivery in 15,000 examinations. Ultrasound Obstet Gynecol. 1996;8:178–85.
Jaddoe VW, Verburg BO, de Ridder MA, Hofman A, Mackenbach JP, Moll HA, Steegers EA, Witteman JC. Maternal smoking and fetal growth characteristics in different periods of pregnancy: the Generation R Study. Am J Epidemiol. 2007;165:1207–15.
Bakker R, Steegers EA, Obradov A, Raat H, Hofman A, Jaddoe VW. Maternal caffeine intake from coffee and tea, fetal growth, and the risks of adverse birth outcomes: the Generation R Study. Am J Clin Nutr. 2010;91(6):1691–8.
Bakker R, Pluimgraaff LE, Steegers EA, Raat H, Tiemeier H, Hofman A, et al. Associations of light and moderate maternal alcohol consumption with fetal growth characteristics in different periods of pregnancy: the Generation R Study. Int J Epidemiol. 2010;39(3):777–89.
El Marroun H, Tiemeier H, Steegers EA, Jaddoe VW, Hofman A, Verhulst FC, van den Brink W, Huizink AC. Intrauterine Cannabis exposure affects fetal growth trajectories: the Generation R Study. J Am Acad Child Adolesc Psychiatry. 2009;48(12):1173–81.
Henrichs J, Schenk JJ, Roza SJ, van den Berg MP, Schmidt HG, Steegers EA, Hofman A, Jaddoe VW, Verhulst FC, Tiemeier H. Maternal psychological distress and fetal growth trajectories: the Generation R Study. Psychol Med. 2010;40(4):633–43.
Roza SJ, Verburg BO, Jaddoe VW, Hofman A, Mackenbach JP, Steegers EA, et al. Effects of maternal smoking in pregnancy on prenatal brain development. The Generation R Study. Eur J Neurosci. 2007;25(3):611–7.
Roza SJ, van Lier PA, Jaddoe VW, Steegers EA, Moll HA, Mackenbach JP, et al. Intrauterine growth and infant temperamental difficulties: the Generation R Study. J Am Acad Child Adolesc Psychiatry. 2008;47(3):264–72.
Henrichs J, Schenk JJ, Schmidt HG, Arends LR, Steegers EA, Hofman A, et al. Fetal size in mid- and late pregnancy is related to infant alertness: the Generation R Study. Dev Psychobiol. 2009;51(2):119–30.
Henrichs J, Schenk JJ, Barendregt CS, Schmidt HG, Steegers EA, Hofman A, et al. Fetal growth from mid- to late pregnancy is associated with infant development: the Generation R Study. Dev Med Child Neurol. 2010;52(7):644–51.
Timmermans S, Jaddoe VW, Hofman A, Steegers-Theunissen RP, Steegers EA. Periconception folic acid supplementation, fetal growth and the risks of low birth weight and preterm birth: the Generation R Study. Br J Nutr. 2009;102(5):777–85.
Mook-Kanamori DO, Steegers EA, Eilers PH, Raat H, Hofman A, Jaddoe VW. Risk factors and outcomes associated with first-trimester fetal growth restriction. JAMA. 2010;303(6):527–34.
Timmermans S, Jaddoe VW, Silva LM, Hofman A, Raat H, Steegers-Theunissen RP, et al. Folic acid is positively associated with uteroplacental vascular resistance: the Generation R Study. Nutr Metab Cardiovasc Dis. 2009. doi:10.1016/j.numecd.2009.07.002.
Verburg BO, Jaddoe VW, Wladimiroff JW, Hofman A, Witteman JC, Steegers EA. Fetal hemodynamic adaptive changes related to intrauterine growth: the Generation R Study. Circulation. 2008;117:649–59.
Verburg BO, Geelhoed JJ, Steegers EA, Hofman A, Moll HA, Witteman JC, Jaddoe VW. Fetal kidney volume and its association with growth and blood flow in fetal life: The Generation R Study. Kidney Int. 2007;72:754–61.
Roza SJ, Steegers EA, Verburg BO, Jaddoe VW, Moll HA, Hofman A, Verhulst FC, Tiemeier H. What is spared by fetal brain-sparing? Fetal circulatory redistribution and behavioral problems in the general population. Am J Epidemiol. 2008;168(10):1145–52.
El Marroun H, Tiemeier H, Steegers EA, Roos-Hesselink JW, Jaddoe VW, Hofman A, Verhulst FC, van den Brink W, Huizink AC. A prospective study on intrauterine cannabis exposure and fetal blood flow. Early Hum Dev. 2010;86(4):231–6.
Coolman M, de Groot CJ, Jaddoe VW, Hofman A, Raat H, Steegers EA. Medical record validation of maternally reported history of preeclampsia. J Clin Epidemiol. 2010;63(8):932–7.
Troude P, L’Helias LF, Raison-Boulley AM, Castel C, Pichon C, Bouyer J, et al. Perinatal factors reported by mothers: do they agree with medical records? Eur J Epidemiol. 2008;23(8):557–64.
Jaddoe VW, Troe EJ, Hofman A, Mackenbach JP, Moll HA, Steegers EA, et al. Active and passive maternal smoking during pregnancy and the risks of low birthweight and preterm birth: the Generation R Study. Paediatr Perinat Epidemiol. 2008;22(2):162–71.
Jaddoe VW, Bakker R, Hofman A, Mackenbach JP, Moll HA, Steegers EA, et al. Moderate alcohol consumption during pregnancy and the risk of low birth weight and preterm birth. The Generation R Study. Ann Epidemiol. 2007;17(10):834–40.
van den Hooven EH, Jaddoe VW, de Kluizenaar Y, Hofman A, Mackenbach JP, Steegers EA, et al. Residential traffic exposure and pregnancy-related outcomes: a prospective birth cohort study. Environ Health. 2009;8:59.
Both MI, Overvest MA, Wildhagen MF, Golding J, Wildschut HI. The association of daily physical activity and birth outcome: a population-based cohort study. Eur J Epidemiol. 2010. doi: 10.1007/s10654-010-9458-0.
Khashan AS, Kenny LC. The effects of maternal body mass index on pregnancy outcome. Eur J Epidemiol. 2009;24(11):697–705.
Abdullah NA, Pearce MS, Parker L, Wilkinson JR, McNally RJ. Evidence of an environmental contribution to the aetiology of cryptorchidism and hypospadias? Eur J Epidemiol. 2007;22(9):615–20.
Astolfi P, De Pasquale A, Zonta LA. Gestational age shortening in single births at term. Italy 1990–1998. Eur J Epidemiol. 2007;22(4):263–5.
Bartels DB, Wenzlaff P, Poets CF. Obstetrical volume and early neonatal mortality in preterm infants. Eur J Epidemiol. 2007;22(11):791–8.
Nabet C, Lelong N, Ancel PY, Saurel-Cubizolles MJ, Kaminski M. Smoking during pregnancy according to obstetric complications and parity: results of the EUROPOP study. Eur J Epidemiol. 2007;22(10):715–21.
Tu YK, Manda SO, Ellison GT, Gilthorpe MS. Revisiting the interaction between birth weight and current body size in the foetal origins of adult disease. Eur J Epidemiol. 2007;22(9):565–75.
Banhidy F, Acs N, Puho EH, Czeizel AE. Maternal acute respiratory infectious diseases during pregnancy and birth outcomes. Eur J Epidemiol. 2008;23(1):29–35.
Hernandez-Diaz S, Wilcox AJ, Schisterman EF, Hernan MA. From causal diagrams to birth weight-specific curves of infant mortality. Eur J Epidemiol. 2008;23(3):163–6.
See LC, Shen YM, Lin SR. Lower early neonatal mortality among singletons in transnational marriage families: Taiwan birth registry. Eur J Epidemiol. 2008;23(7):483–9.
Strandberg-Larsen K, Rod Nielsen N, Nybo Andersen AM, Olsen J, Gronbaek M. Characteristics of women who binge drink before and after they become aware of their pregnancy. Eur J Epidemiol. 2008;23(8):565–72.
Zhu JL, Vestergaard M, Madsen KM, Olsen J. Paternal age and mortality in children. Eur J Epidemiol. 2008;23(7):443–7.
Julihn A, Ekbom A, Modeer T. Maternal overweight and smoking: prenatal risk factors for caries development in offspring during the teenage period. Eur J Epidemiol. 2009;24(12):753–62.
Greenwood DC, Alwan N, Boylan S, Cade JE, Charvill J, Chipps KC, et al. Caffeine intake during pregnancy, late miscarriage and stillbirth. Eur J Epidemiol. 2010;25(4):275–80.
Stichting Perinatale Registratie Nederland. 2010. (www.perinatreg.nl).
Ludvigsson JF, Otterblad-Olausson P, Pettersson BU, Ekbom A. The Swedish personal identity number: possibilities and pitfalls in healthcare and medical research. Eur J Epidemiol. 2009;24(11):659–67.
Jaddoe VW, Bakker R, van Duijn CM, van der Heijden AJ, Lindemans J, Mackenbach JP, Moll HA, Steegers EA, Tiemeier H, Uitterlinden AG, Verhulst FC, Hofman A. The Generation R Study Biobank: a resource for epidemiological studies in children and their parents. Eur J Epidemiol. 2007;22:917–23.
Henrichs J, Bongers-Schokking JJ, Schenk JJ, Ghassabian A, Schmidt HG, Visser TJ, et al. Maternal thyroid function during early pregnancy and cognitive functioning in early childhood: the Generation R Study. J Clin Endocrinol Metab. 2010;95(9):4227–34.
Asfeldt AM, Straume B, Steigen SE, Lochen ML, Florholmen J, Bernersen B, et al. Changes in the prevalence of dyspepsia and Helicobacter pylori infection after 17 years: the Sorreisa gastrointestinal disorder study. Eur J Epidemiol. 2008;23(9):625–33.
Sandven I, Abdelnoor M, Wethe M, Nesheim BI, Vikanes A, Gjonnes H, et al. Helicobacter pylori infection and Hyperemesis gravidarum. An institution-based case-control study. Eur J Epidemiol. 2008;23(7):491–8.
Rours GI, Verkooyen RP, Willemse HF, van der Zwaan EA, van Belkum A, de Groot R, Verbrugh HA, Ossewaarde JM. Use of pooled urine samples and automated DNA isolation to achieve improved sensitivity and cost-effectiveness of large-scale testing for Chlamydia trachomatis in pregnant women. R J Clin Microbiol. 2005;43:4684–90.
Ye X, Pierik FH, Hauser R, Duty S, Angerer J, Park MM, Burdorf A, Hofman A, Jaddoe VW, Mackenbach JP, Steegers EA, Tiemeier H, Longnecker MP. Urinary metabolite concentrations of organophosphorous pesticides, bisphenol A, and phthalates among pregnant women in Rotterdam, the Netherlands: the Generation R Study. Environ Res. 2008;108:260–7.
Wang WY, Barratt BJ, Clayton DG, Todd JA. Genome-wide association studies: theoretical and practical concerns. Nat Rev Genet. 2005;6:109–18.
Hofman A, Breteler MM, van Duijn CM, Janssen HL, Krestin GP, Kuipers EJ, Stricker BH, Tiemeier H, Uitterlinden AG, Vingerling JR, Witteman JC. The Rotterdam study: 2010 objectives and design update. Eur J Epidemiol. 2009;24(9):553–72.
Huang L, Li Y, Singleton AB, Hardy JA, Abecasis G, Rosenberg NA, Scheet P. Genotype-imputation accuracy across worldwide human populations. Am J Hum Genet. 2009;84(2):235–50.
Freathy RM, Mook-Kanamori DO, Sovio U, Prokopenko I, Timpson NJ, Berry DJ, et al. Variants in ADCY5 and near CCNL1 are associated with fetal growth and birth weight. Nat Genet. 2010;42(5):430–5.
Thompson A. Thinking big: large-scale collaborative research in observational epidemiology. Eur J Epidemiol. 2009;24(12):727–31.
Isaacs A, Sayed-Tabatabaei FA, Aulchenko YS, Zillikens MC, Sijbrands EJ, Schut AF, et al. Heritabilities, apolipoprotein E, and effects of inbreeding on plasma lipids in a genetically isolated population: the Erasmus Rucphen family study. Eur J Epidemiol. 2007;22(2):99–105.
Collaboration CCG. Collaborative pooled analysis of data on C-reactive protein gene variants and coronary disease: judging causality by Mendelian randomisation. Eur J Epidemiol. 2008;23(8):531–40.
Little J, Higgins JP, Ioannidis JP, Moher D, Gagnon F, von Elm E, et al. Strengthening the reporting of genetic association studies (STREGA): an extension of the STROBE statement. Eur J Epidemiol. 2009;24(1):37–55.
Miettinen OS. Up from ‘false positives’ in genetic-and other-epidemiology. Eur J Epidemiol. 2009;24(1):1–5.
Thelle DS. STROBE and STREGA: instruments for improving transparency and quality of reporting scientific results. Eur J Epidemiol. 2009;24(1):7–8.
van Wieren-de Wijer DB, Maitland-van der Zee AH, de Boer A, Belitser SV, Kroon AA, de Leeuw PW, et al. Determinants of DNA yield and purity collected with buccal cell samples. Eur J Epidemiol. 2009;24(11):677–82.
Psaty BM, Hofman A. Genome-wide association studies and large-scale collaborations in epidemiology. Eur J Epidemiol. 2010;25(8):525–9.
Tan Q, Zhao JH, Li S, Kruse TA, Christensen K. Power assessment for genetic association study of human longevity using offspring of long-lived subjects. Eur J Epidemiol. 2010;25(7):501–6.
Janssens AC. Is the time right for translation research in genomics? Eur J Epidemiol. 2008;23(11):707–10.
Amin N, van Duijn CM, Janssens AC. Genetic scoring analysis: a way forward in genome wide association studies? Eur J Epidemiol. 2009;24(10):585–7.
Mook-Kanamori DO, Miranda Geelhoed JJ, Steegers EA, Witteman JC, Hofman A, Moll HA, et al. Insulin gene variable number of tandem repeats is not associated with weight from fetal life until infancy: the Generation R Study. Eur J Endocrinol. 2007;157(6):741–8.
Geelhoed JJ, Mook-Kanamori DO, Witteman JC, Hofman A, van Duijn CM, Moll HA, et al. Variation in the IGF1 gene and growth in foetal life and infancy. The Generation R Study. Clin Endocrinol (Oxf). 2008;68(3):382–9.
van Houten VA, Mook-Kanamori DO, van Osch-Gevers L, Steegers EA, Hofman A, Moll HA, et al. A variant of the IGF-I gene is associated with blood pressure but not with left heart dimensions at the age of 2 years: the Generation R Study. Eur J Endocrinol. 2008;159(3):209–16.
Duijts L, Bakker-Jonges LE, Mook-Kanamori DO, Labout JA, Hofman A, van Duijn CM, et al. Variation in the IGF-1 gene is associated with lymphocyte subset counts in neonates: the Generation R Study. Clin Endocrinol (Oxf). 2009;70(1):53–9.
Maas JA, Mook-Kanamori DO, Ay L, Steegers EA, van Duijn CM, Hofman A, et al. Insulin VNTR and IGF-1 promoter region polymorphisms are not associated with body composition in early childhood: the Generation R Study. Horm Res Paediatr. 2010;73(2):120–7.
Mook-Kanamori DO, Steegers EA, Uitterlinden AG, Moll HA, van Duijn CM, Hofman A, et al. Breast-feeding modifies the association of PPARgamma2 polymorphism Pro12Ala with growth in early life: the Generation R Study. Diabetes. 2009;58(4):992–8.
Mook-Kanamori DO, de Kort SW, van Duijn CM, Uitterlinden AG, Hofman A, Moll HA, et al. Type 2 diabetes gene TCF7L2 polymorphism is not associated with fetal and postnatal growth in two birth cohort studies. BMC Med Genet. 2009;10:67.
Geelhoed MJ, Steegers EA, Koper JW, van Rossum EF, Moll HA, Raat H, et al. Glucocorticoid receptor gene polymorphisms do not affect growth in fetal and early postnatal life. The Generation R Study. BMC Med Genet. 2010;11:39.
Mook-Kanamori DO, Ay L, Hofman A, van Duijn CM, Moll HA, Raat H, et al. No association of obesity gene FTO with body composition at the age of 6 months. The Generation R Study. J Endocrinol Invest. 2010 (in press).
Luijk MP, Velders FP, Tharner A, van Ijzendoorn MH, Bakermans-Kranenburg MJ, Jaddoe VW, et al. FKBP5 and resistant attachment predict cortisol reactivity in infants: gene-environment interaction. Psychoneuroendocrinology. 2010. doi:10.1016/j.psyneuen.2010.04.012.
van Batenburg-Eddes T, de Groot L, Arends L, de Vries A, Moll HA, Steegers EA, Hofman A, Jaddoe VW, Verhulst FC, Tiemeier H. Does gestational duration within the normal range predict infant neuromotor development? Early Hum Dev. 2008;84:659–65.
van Batenburg-Eddes T, de Groot L, Steegers EA, Hofman A, Jaddoe VW, Verhulst FC, et al. Fetal programming of infant neuromotor development: the Generation R Study. Pediatr Res. 2010;67(2):132–7.
van Batenburg-Eddes T, de Groot L, Huizink AC, Steegers EA, Hofman A, Jaddoe VW, et al. Maternal symptoms of anxiety during pregnancy affect infant neuromotor development: the Generation R Study. Dev Neuropsychol. 2009;34(4):476–93.
Burgmeijer RJF, Merkx JAM. Pakket.En hoe pakt het uit: Ouder en Kindzorg tussen wetenschap en praktijk. Nederlands Congres Ouder en Kindzorg. Assen, the Netherlands: van Gorcum; 1999.
Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF- 36). I. Conceptual framework and item selection. Med Care. 1992;30:473–83.
Carver DJ, Chapman CA, Thomas VS, Stadnyk KJ, Rockwood K. Validity and reliability of the medical outcomes study short form-20 questionnaire as a measure of quality of life in elderly people living at home. Age Ageing. 1999;28:169–74.
De Brock AJLL, Vermulst AA, Gerris JRM, Abidin RR. Nijmeegse Ouderlijke Stress Index. Lisse: Swets en Zeitlinger b.v.; 1992.
Gerris JR, Boxtel DA, Vermulst AA, Janssens JM, van Zuthpen RA, Felling AJ. Parenting in Dutch families. Nijmegen, The Netherlands: University of Nijmegen, Institute of Family Studies; 1993.
Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry. 1987;150:782–6.
Derogatis LR, Melisaratos N. The brief symptom inventory: an introductory report. Psychol Med. 1983;13:595–605.
Duijts L, Jaddoe VW, Hofman A, Moll HA. Prolonged and exclusive breastfeeding reduces the risk of infectious diseases in infancy. Pediatrics. 2010;126(1):e18–25.
Wardle J, Guthrie CA, Sanderson S, Rapoport LJ. Development of the children’s eating behaviour questionnaire. Child Psychol Psychiatry. 2001;42:963–70.
Raat H, Botterweck AM, Landgraf JM, Hoogeveen WC, Essink-Bot ML. Reliability and validity of the short form of the child health questionnaire for parents (CHQ-PF28) in large random school based and general population samples. J Epidemiol Community Health. 2005;59:75–82.
Duijts L, Jaddoe VW, Hofman A, Steegers EA, Mackenbach JP, de Jongste JC, Moll HA. Maternal smoking in prenatal and early postnatal life and the risk of respiratory tract infections in infancy. The Generation R Study. Eur J Epidemiol. 2008;23(8):547–55.
Taylor JC, Law GR, Boyle PJ, Feng Z, Gilthorpe MS, Parslow RC, et al. Does population mixing measure infectious exposure in children at the community level? Eur J Epidemiol. 2008;23(9):593–600.
Raoult D. Recent and future developments in the epidemiology of the infectious diseases. Eur J Epidemiol. 2009;24(8):393–5.
Jenkins MA, Clarke JR. Validation of a questionnaire and bronchial hyper-responsiveness against respiratory physician assessment in the diagnosis of asthma. Int J Epidemiol. 1996;25:609–16.
Gabriele C, Asgarali R, Jaddoe VW, Hofman A, Moll HA, de Jongste JC. Smoke exposure, airway symptoms and exhaled nitric oxide in infants: the Generation R Study. Eur Respir J. 2008;32(2):307–13.
Mohangoo AD, de Koning HJ, Hafkamp-de Groen E, van der Wouden JC, Jaddoe VW, Moll HA, et al. A comparison of parent-reported wheezing or shortness of breath among infants as assessed by questionnaire and physician-interview: The Generation R Study. Pediatr Pulmonol. 2010;45(5):500–7.
Kompauer I, Demmelmair H, Koletzko B, Bolte G, Linseisen J, Heinrich J. Association of fatty acids in serum phospholipids with lung function and bronchial hyperresponsiveness in adults. Eur J Epidemiol. 2008;23(3):175–90.
Rzehak P, Schoefer Y, Wichmann HE, Heinrich J. A prospective study on the association between hay fever among children and incidence of asthma in East Germany. Eur J Epidemiol. 2008;23(1):17–22.
Behrens T. Current trends in aetiological asthma research. Eur J Epidemiol. 2009;24(3):115–8.
Visser AM, Jaddoe VW, Arends LR, Tiemeier H, Hofman A, Moll HA, et al. Paroxysmal disorders in infancy and their risk factors in a population-based cohort: the Generation R Study. Dev Med Child Neurol. 2010. doi:10.1111/j.1469-8749.2010.03689.x.
Kiefte-de Jong JC, Escher JC, Arends LR, Jaddoe VW, Hofman A, Raat H, et al. Infant nutritional factors and functional constipation in childhood: the Generation R Study. Am J Gastroenterol. 2010;105(4):940–5.
St James-Roberts I, Halil T. Infant crying patterns in the first year: normal community and clinical findings. J Child Psychol Psychiatry. 1991;32:951–68.
van den Berg MP, van der Ende J, Crijnen AA, Jaddoe VW, Moll HA, Mackenbach JP, Hofman A, Hengeveld MW, Tiemeier H, Verhulst FC. Paternal depressive symptoms during pregnancy are related to excessive infant crying. Pediatrics. 2009;124(1):e96–103.
Gartstein MA, Rothbart MK. Studying infant temperament via the revised infant behavior questionnaire. Infant Behav Dev. 2003;26:64–86.
Ireton H, Glascoe FP. Assessing children’s development using parents’ reports. The child development inventory. Clin Pediatr. 1995;34:248–55.
St James-Roberts I, Wolke D. Differences between maternal and objective ratings of difficult neonatal behavioural style: implications for temperament research and clinical perspectives. J Reprod Infant Psychol. 1983;1:53–60.
St James-Roberts I, Wolke D. Convergences and discrepancies, among mothers’ and professionals’ assessments of difficult neonatal behaviour. J Child Psychol Psych All Discipl. 1989;29:21–42.
Achenbach TM. Manual for the child behavior checklist/4–18 and 1991 profile. Burlington: University of Vermont Department of Psychiatry; 1991.
Verhulst FC, Van der Ende J, Koot HM. Manual for the CBCL/4-18. Rotterdam, the Netherlands: Erasmus Universiteit/Deptartment of Child and Adolescent Psychiatry, Sophia Children’s Hospital; 1996.
Cents RA, Tiemeier H, Luijk MP, Jaddoe VW, Hofman A, Verhulst FC, et al. Grandparental anxiety and depression predict young children’s internalizing and externalizing problems The Generation R Study. J Affect Disord. 2010. doi:10.1016/j.jad.2010.06.020.
Roza SJ, van Batenburg-Eddes T, Steegers EA, Jaddoe VW, Mackenbach JP, Hofman A, et al. Maternal folic acid supplement use in early pregnancy and child behavioural problems: the Generation R Study. Br J Nutr. 2010;103(3):445–52.
Roza SJ, Verhulst FC, Jaddoe VW, Steegers EA, Mackenbach JP, Hofman A, et al. Maternal smoking during pregnancy and child behaviour problems: the Generation R Study. Int J Epidemiol. 2009;38(3):680–9.
Walker LS, Garber SJ, van Slyke DA. Development and validation of the pain response inventory for children. Psychol Assess. 1997;9:392–405.
Wolff NJ, Darlington AS, Hunfeld JA, Verhulst FC, Jaddoe VW, Moll HA, Hofman A, Passchier J, Tiemeier H. The association of parent behaviors, chronic pain, and psychological problems with venipuncture distress in infants: the Generation R Study. Health Psychol. 2009;28(5):605–13.
Wolff N, Darlington AS, Hunfeld J, Verhulst F, Jaddoe V, Hofman A, et al. Determinants of somatic complaints in 18-month-old children: the Generation R Study. J Pediatr Psychol. 2010;35(3):306–16.
Fenson L, Dale PS, Reznick JS, Thal D, Bates E, Hartung JP. MacArthur communicative development inventories; user’s guide and technical manual. San Diego: Singular Publishing Group, Inc; 1983.
Saudino KJ, Dale PS, Oliver B, Petrill SA, Richardson V, Rutter M, Simonoff E, Stevenson J, Plomin R. The validity of parent-based assessment of cognitive abilities of 2-year-olds. Br J Develop Psychol. 1998;16:349–63.
Isquith PK, Gioia GA, Espy KA. Executive function in preschool children: examination through everyday behavior. Dev Neuropsychol. 2004;26:403–22.
Ay L, Hokken-Koelega AC, Mook-Kanamori DO, Hofman A, Moll HA, Mackenbach JP, et al. Tracking and determinants of subcutaneous fat mass in early childhood: the Generation R Study. Int J Obes (Lond). 2008;32(7):1050–9.
Holzhauer S, Hokken Koelega AC, Ridder M, Hofman A, Moll HA, Steegers EA, et al. Effect of birth weight and postnatal weight gain on body composition in early infancy: The Generation R Study. Early Hum Dev. 2009;85(5):285–90.
Roza SJ, Govaert PP, Vrooman HA, Lequin MH, Hofman A, Steegers EA, et al. Foetal growth determines cerebral ventricular volume in infants The Generation R Study. Neuroimage. 2008;39(4):1491–8.
Roza SJ, Govaert PP, Lequin MH, Jaddoe VW, Moll HA, Steegers EA, et al. Cerebral ventricular volume and temperamental difficulties in infancy The Generation R Study. J Psychiatry Neurosci. 2008;33(5):431–9.
Geelhoed MJ, Snijders SP, Kleyburg-Linkers VE, Steegers EA, van Osch-Gevers L, Jaddoe VW. Reliability of echocardiographic measurements of left cardiac structures in healthy children. Cardiol Young. 2009;19(5):494–500.
Geelhoed JJ, Steegers EA, van Osch-Gevers L, Verburg BO, Hofman A, Witteman JC, et al. Cardiac structures track during the first 2 years of life and are associated with fetal growth and hemodynamics: the Generation R Study. Am Heart J. 2009;158(1):71–7.
Geelhoed JJ, VANO-G L, Verburg BO, Steegers EA, Hofman A, Helbing W, et al. Maternal anthropometrics in pregnancy are associated with left ventricular mass in infancy. The Generation R Study. Pediatr Res. 2008;63(1):62–6.
de Jonge LL, van Osch-Gevers L, Geelhoed JJ, Hofman A, Steegers EA, Helbing WA, et al. Breastfeeding is not associated with left cardiac structures and blood pressure during the first two years of life. The Generation R Study. Early Hum Dev. 2010;86(8):463–8.
Geelhoed JJ, Kleyburg-Linkers VE, Snijders SP, Lequin M, Nauta J, Steegers EA, et al. Reliability of renal ultrasound measurements in children. Pediatr Nephrol. 2009;24(7):1345–53.
Geelhoed JJ, Taal HR, Steegers EA, Arends LR, Lequin M, Moll HA, et al. Kidney growth curves in healthy children from the third trimester of pregnancy until the age of two years. The Generation R Study. Pediatr Nephrol. 2010;25(2):289–98.
Geelhoed JJ, Verburg BO, Nauta J, Lequin M, Hofman A, Moll HA, et al. Tracking and determinants of kidney size from fetal life until the age of 2 years: the Generation R Study. Am J Kidney Dis. 2009;53(2):248–58.
Mook-Kanamori DO, Holzhauer S, Hollestein LM, Durmus B, Manniesing R, Koek M, et al. Abdominal fat in children measured by ultrasound and computed tomography. Ultrasound Med Biol. 2009;35(12):1938–46.
Durmus B, Mook-Kanamori DO, Holzhauer S, Hofman A, van der Beek EM, Boehm G, et al. Growth in foetal life and infancy is associated with abdominal adiposity at the age of 2 years: the Generation R Study. Clin Endocrinol (Oxf). 2010;72(5):633–40.
Holzhauer S, Zwijsen RM, Jaddoe VW, Boehm G, Moll HA, Mulder PG, et al. Sonographic assessment of abdominal fat distribution in infancy. Eur J Epidemiol. 2009;24(9):521–9.
Ay L, Van Houten VA, Steegers EA, Hofman A, Witteman JC, Jaddoe VW, et al. Fetal and postnatal growth and body composition at 6 months of age. J Clin Endocrinol Metab. 2009;94(6):2023–30.
van Houten VA, Steegers EA, Witteman JC, Moll HA, Hofman A, Jaddoe VW. Fetal and postnatal growth and blood pressure at the age of 2 years. The Generation R Study. J Hypertens. 2009;27(6):1152–7.
Dierckx B, Tulen JH, van den Berg MP, Tharner A, Jaddoe VW, Moll HA, et al. Maternal psychopathology influences infant heart rate variability: Generation R Study. Psychosom Med. 2009;71(3):313–21.
Dierckx B, Tulen JH, Tharner A, Jaddoe VW, Hofman A, Verhulst FC, et al. Low autonomic arousal as vulnerability to externalising behaviour in infants with hostile mothers. Psychiatry Res. 2010. doi:10.1016/j.psychres.2009.09.014.
Labout JA, Duijts L, Arends LR, Jaddoe VW, Hofman A, de Groot R, et al. Factors associated with pneumococcal carriage in healthy Dutch infants: the Generation R Study. J Pediatr. 2008;153(6):771–6.
Lebon A, Labout JA, Verbrugh HA, Jaddoe VW, Hofman A, van Wamel W, et al. Dynamics and determinants of Staphylococcus aureus carriage in infancy: the Generation R Study. J Clin Microbiol. 2008;46(10):3517–21.
Lebon A, Moll HA, Tavakol M, van Wamel WJ, Jaddoe VW, Hofman A, et al. Correlation of bacterial colonization status between mother and child: the Generation R Study. J Clin Microbiol. 2010;48(3):960–2.
Verkaik NJ, Lebon A, de Vogel CP, Hooijkaas H, Verbrugh HA, Jaddoe VW, et al. Induction of antibodies by Staphylococcus aureus nasal colonization in young children. Clin Microbiol Infect. 2010;16(8):1312–7.
Verhaegh SJ, Lebon A, Saarloos JA, Verbrugh HA, Jaddoe VW, Hofman A, et al. Determinants of Moraxella catarrhalis colonization in healthy Dutch children during the first 14 months of life. Clin Microbiol Infect. 2009. doi:10.1111/j.1469-0691.2009.03008.x.
Lebon A, Labout JA, Verbrugh HA, Jaddoe VW, Hofman A, van Wamel WJ, et al. Role of Staphylococcus aureus nasal colonization in atopic dermatitis in infants: the Generation R Study. Arch Pediatr Adolesc Med. 2009;163(8):745–9.
Saridjan NS, Huizink AC, Koetsier JA, Jaddoe VW, Mackenbach JP, Hofman A, Kirschbaum C, Verhulst FC, Tiemeier H. Do social disadvantage and early family adversity affect the diurnal cortisol rhythm in infants? The Generation R Study. Horm Behav. 2010;57(2):247–54.
Luijk MP, Saridjan N, Tharner A, van Ijzendoorn MH, Bakermans-Kranenburg MJ, Jaddoe VW, et al. Attachment, depression, and cortisol: deviant patterns in insecure-resistant and disorganized infants. Dev Psychobiol. 2010;52(5):441–52.
Duijts L, Bakker-Jonges LE, Labout JA, Jaddoe VW, Hofman A, Steegers EA, et al. Perinatal stress influences lymphocyte subset counts in neonates. The Generation R Study. Pediatr Res. 2008;63(3):292–8.
Duijts L, Bakker-Jonges LE, Labout JA, Jaddoe VW, Hofman A, Steegers EA, et al. Fetal growth influences lymphocyte subset counts at birth: the Generation R Study. Neonatology. 2009;95(2):149–56.
Alonso A, de Irala J, Martinez-Gonzalez MA. Representativeness, losses to follow-up and validity in cohort studies. Eur J Epidemiol. 2007;22(7):481–2.
Richiardi L, Baussano I, Vizzini L, Douwes J, Pearce N, Merletti F, et al. Feasibility of recruiting a birth cohort through the Internet: the experience of the NINFEA cohort. Eur J Epidemiol. 2007;22(12):831–7.
Cardis E, Richardson L, Deltour I, Armstrong B, Feychting M, Johansen C, et al. The INTERPHONE study: design, epidemiological methods, and description of the study population. Eur J Epidemiol. 2007;22(9):647–64.
Pitrou I, Dauchet L, Bailly L, Koubi SE, Tavolacci MP, Ladner J. Mobile phone follow-up of subjects included in a prospective cohort study: unexpected difficulties. Eur J Epidemiol. 2007;22(6):411–2.
Ekman A, Klint A, Dickman PW, Adami HO, Litton JE. Optimizing the design of web-based questionnaires—experience from a population-based study among 50, 000 women. Eur J Epidemiol. 2007;22(5):293–300.
Touvier M, Mejean C, Kesse-Guyot E, Pollet C, Malon A, Castetbon K, et al. Comparison between web-based and paper versions of a self-administered anthropometric questionnaire. Eur J Epidemiol. 2010;25(5):287–96.
Barakat-Haddad CP, Elliott SJ, Eyles J, Pengelly D. Predictors of locating children participants in epidemiological studies 20 years after last contact: internet resources and longitudinal research. Eur J Epidemiol. 2009;24(8):397–405.
Bexelius C, Merk H, Sandin S, Ekman A, Nyren O, Kuhlmann-Berenzon S, et al. SMS versus telephone interviews for epidemiological data collection: feasibility study estimating influenza vaccination coverage in the Swedish population. Eur J Epidemiol. 2009;24(2):73–81.
Clarisse B, Nikasinovic L, Poinsard R, Just J, Momas I. The Paris prospective birth cohort study: which design and who participates? Eur J Epidemiol. 2007;22(3):203–10.
Stolk RP, Rosmalen JG, Postma DS, de Boer RA, Navis G, Slaets JP, et al. Universal risk factors for multifactorial diseases: LifeLines: a three-generation population-based study. Eur J Epidemiol. 2008;23(1):67–74.
Kim BM, Ha M, Park HS, Lee BE, Kim YJ, Hong YC, et al. The mothers and children’s environmental health (MOCEH) study. Eur J Epidemiol. 2009;24(9):573–83.
Nur U, Longford NT, Cade JE, Greenwood DC. The impact of handling missing data on alcohol consumption estimates in the UK women cohort study. Eur J Epidemiol. 2009;24(10):589–95.
Delaney JA, Platt RW, Suissa S. The impact of unmeasured baseline effect modification on estimates from an inverse probability of treatment weighted logistic model. Eur J Epidemiol. 2009;24(7):343–9.
Foraita R. A conditional synergy index to assess biological interaction. Eur J Epidemiol. 2009;24(9):485–94.
Goodman A, Gatward R. Who are we missing? Area deprivation and survey participation. Eur J Epidemiol. 2008;23(6):379–87.
Lundbye-Christensen S, Dethlefsen C, Gorst-Rasmussen A, Fischer T, Schonheyder HC, Rothman KJ, et al. Examining secular trends and seasonality in count data using dynamic generalized linear modelling: a new methodological approach illustrated with hospital discharge data on myocardial infarction. Eur J Epidemiol. 2009;24(5):225–30.
Hafeman DM. A sufficient cause based approach to the assessment of mediation. Eur J Epidemiol. 2008;23(11):711–21.
Miettinen OS. Survival analysis: up from Kaplan–Meier-Greenwood. Eur J Epidemiol. 2008;23(9):585–92.
Pekkanen J, Sunyer J. Problems in using incidence to analyze risk factors in follow-up studies. Eur J Epidemiol. 2008;23(9):581.
Stang A. Appropriate epidemiologic methods as a prerequisite for valid study results. Eur J Epidemiol. 2008;23(12):761–5.
Stromberg U. Empirical bayes and semi-bayes adjustments for a vast number of estimations. Eur J Epidemiol. 2009;24(12):737–41.
VanderWeele TJ. Mediation and mechanism. Eur J Epidemiol. 2009;24(5):217–24.
Walter S, Tiemeier H. Variable selection: current practice in epidemiological studies. Eur J Epidemiol. 2009;24(12):733–6.
Acknowledgments
The Generation R Study is conducted by the Erasmus Medical Center in close collaboration with the School of Law and Faculty of Social Sciences of the Erasmus University Rotterdam, the Municipal Health Service Rotterdam area, Rotterdam, the Rotterdam Homecare Foundation, Rotterdam and the Stichting Trombosedienst & Artsenlaboratorium Rijnmond (STAR-MDC), Rotterdam. We gratefully acknowledge the contribution of children and parents, general practitioners, hospitals, midwives and pharmacies in Rotterdam. We thank Rachel Bakker, Claudia Kruithof and Dr. Fernando Rivadeneira for their study coordination, data management, and GWAS analyses. The general design of Generation R Study is made possible by financial support from the Erasmus Medical Center, Rotterdam, the Erasmus University Rotterdam, the Netherlands Organization for Health Research and Development (ZonMw), the Netherlands Organisation for Scientific Research (NWO), the Ministry of Health, Welfare and Sport and the Ministry of Youth and Families. Vincent Jaddoe received an additional grant from the Netherlands Organization for Health Research and Development (ZonMw 90700303, 916.10159).
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Jaddoe, V.W.V., van Duijn, C.M., van der Heijden, A.J. et al. The Generation R Study: design and cohort update 2010. Eur J Epidemiol 25, 823–841 (2010). https://doi.org/10.1007/s10654-010-9516-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10654-010-9516-7