
Abstract
Objectives To investigate the association between occupational social class and cardiovascular disease (CVD) incidence, and the extent to which classical and lifestyle risk factors explain such relationships, and if any differences persist after 65 years of age. Design, Setting and Participants Prospective population study of 22,478 men and women aged 39–79 years living in the general community in Norfolk, United Kingdom, recruited using general practice age-sex registers in 1993–1997 and followed up for total mortality to 2006. Main results In both men and women an inverse relationship was observed between social class and CVD incidence, with a relative risk of social class V compared to I of 1.90 in men (95% CI 1.47 to 2.47, P < 0.001) and 1.90 in women (95% CI 1.45 to 2.49, P < 0.001). Adjusting for classical and lifestyle risk factors (age, smoking, BMI, systolic blood pressure, total blood cholesterol, history of diabetes, physical activity, weekly alcohol intake and plasma vitamin C levels) had little effect in men; the relative risk of social class V compared to I of 1.70 (95% CI 1.31 to 2.22, P < 0.001), while there was some attenuation seen in women, relative risk of social class V compared to I of 1.56 (95% CI 1.18 to 2.05, P = 0.011). The association persisted in men and women aged ≥65 years. Conclusions Some but not all of the socioeconomic differential in CVD incidence can be explained by potentially modifiable classical and lifestyle risk factors. Low social class remains a risk factor for CVD after age 65 years. Further understanding of the mechanisms underlying the association is needed if we are to reduce inequalities in health.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cardiovascular disease (CVD) is the main cause of death in the UK, accounting for over 208,000 deaths each year [1]. Death rates have been falling since the 1970s, however rates have fallen faster in the higher social classes so that the relative difference between those at the top and those at the bottom of the social scale has widened. Social inequalities in CVD in the UK are well documented [2–8]. However the majority of previous research focuses on younger men. The relationship between social class and cardiovascular risk factors differs between individuals depending on their age and sex [9]; it follows that the association between social class and CVD itself may also vary with age and sex, and should thus be explored within both sexes and over a larger age range that includes individuals who have retired. We have previously examined the relationship with total mortality in this cohort [10]. Since CVD mortality showed the greatest social gradient, we wished to focus on cardiovascular disease incidence to examine this question in more detail. We studied the relations between social class and CVD incidence, asking whether any socioeconomic differentials could be explained by classical and lifestyle CVD risk factors, and whether the associations were independent of educational attainment. Social class is a measure based upon occupation: we asked whether any associations with CVD incidence persist after 65 years of age.
Methods
Participants and measurements
The participants were part of a prospective population study of men and women aged 39–79 years, 99.5% white (as self-defined on questionnaire), resident in Norfolk, United Kingdom. Norfolk is a county in the UK encompassing a wide socioeconomic and urban–rural distribution. The cohort was recruited between 1993 and 1997 from age-sex registers of general practices as part of the Norfolk component of the European Prospective Investigation of Cancer (EPIC-Norfolk). All individuals in the age range in each General Practice database were invited to participate, except those marked as unsuitable by their General Practitioner. As virtually 100% of people in the UK are registered with general practitioners through the National Health Service, the age-sex registers form a population-based sampling frame. Detailed descriptions of the study methodology have been reported previously [11]. Approval for the study was obtained from the Norfolk Local Research Ethics Committee. Altogether 77,630 participants were invited, and 30,445 gave informed signed consent and completed a detailed health and lifestyle questionnaire. Of these, 25,639 agreed to attend a health examination. Because we required participants who were willing to provide detailed information and participate in a long term follow-up study, we only had a population response rate of about 45%, so participants were not a random population sample. Nevertheless, they were comparable to national samples with respect to many characteristics, but with a slightly lower prevalence of smokers.
Social class was classified according to the Registrar General’s occupation based classification scheme [12, 13]. Social class I consists of professionals, class II includes managerial and technical occupations, class III is subdivided into non-manual and manual skilled workers (IIInm and IIIm), class IV consists of partly skilled workers, and class V comprises unskilled manual workers (the detailed classification is described elsewhere [13]). For descriptive purposes, the variable was also grouped into non manual classes (classes I, II and IIInm) and manual classes (IIIm, IV and V). For men, social class was coded using their current occupation at the time of survey except when they were unemployed in which case their partner’s social class was used. Last employment was used for men who were retired. Unemployed men without partners were unclassified. Social class in women was based on their partner’s except when the partner’s social class was unclassified, missing, or they had no partner in which case social class was based on their own occupation. An unemployed woman without a partner was coded as unclassified.
Educational status was based on the highest qualification attained and was categorised into four groups: degree or equivalent, A-level or equivalent, O-level or equivalent, and less than O-level or no qualifications. O-level indicates educational attainment to the equivalent of completion of schooling to the age of 15 years and A-level indicates educational attainment to the equivalent of completion of schooling to the age of 17 years. For descriptive purposes educational status was also regrouped into those who finished school (degree or equivalent, A-level or equivalent, O-level or equivalent) and those who did not (less than O-level or no qualifications).
Personal medical history was assessed using the question in the Health and Lifestyle Questionnaire, “Has the doctor ever told you that you have any of the following?” followed by a checklist of diseases including myocardial infarction, stroke, cancer and diabetes mellitus. Yes/no responses to the questions “Have you ever smoked as much as one cigarette a day for as long as a year?” and “Do you smoke cigarettes now?” were used to derive smoking history [14, 15]. Height and weight were measured by trained nurses with participants dressed in light clothing and with their shoes removed [16]. A stadiometer was used to measure height to the nearest 0.1 cm. Salter scales were used to measure weight to the nearest 100 g. Body mass index (BMI) was then calculated as weight (kg)/height2 (m2). Blood and urine testing were performed by trained nurses using standard protocols. Blood pressure was recorded as the mean of two measurements taken in the right arm with the subject seated for 5 min, with the use of an Accutorr sphygmomanometer (Datascope, Huntingdon, UK). Levels of total cholesterol in nonfasted serum samples were measured by colorimetry (RA 100, Bayer Diagnostics, Basingstoke, UK).
Habitual physical activity was assessed using two questions referring to activity during the past year. The first question asked about usual physical activity at work, classified as four categories: sedentary, standing (e.g. hairdresser, guard), physical work (e.g. plumber, nurse) and heavy manual work (e.g. construction worker). The second question asked about the amount of time spent in hours per week in winter and summer in other physical activity. A simple index allocated individuals to four ordered categories: inactive (sedentary job and no recreational activity); moderately inactive (sedentary job with <0.5 h recreational activity per day, or standing job with no recreational activity); moderately active (sedentary job with 0.5–1 h recreational activity per day or standing job with <0.5 h recreational activity per day or physical job with no recreational activity); and active (sedentary job with >1 h recreational activity per day or standing job with >1 h recreational activity per day or physical job with at least some recreational activity or heavy manual job). This index was validated against heart rate monitoring with individual calibration in independent studies [17, 18]. We have also previously reported that this four point index is inversely related to all cause mortality and cardiovascular disease incidence in the EPIC-Norfolk population in men and women across a wide age and social class range [19].
Endpoint ascertainment
Incident CVD cases were defined using two methods: death certificate data and hospital record linkage. All individuals have been flagged for death at the UK Office of National Statistics (ONS), which is virtually complete. Death certificates are coded by trained nosologists using International Classification of Disease (ICD), revisions 9 and 10. Participants are also linked to hospital information systems so that hospital admissions anywhere in the United Kingdom are communicated to EPIC-Norfolk. Records are updated annually. The present study is based on follow-up to 31st July 2006. An incident cardiovascular disease event was defined as death with ICD-9 codes 401 to 448 or ICD-10 codes I10 to I79 anywhere on the death certificate and/or hospital admission with the same codes. A validation study was conducted of coronary artery disease cases ascertained from death certificates and hospital admissions in 1996 in EPIC-Norfolk [20]. The results indicated that this is a valid method for ascertaining events.
Statistical analysis
Descriptive statistics including means and percentages are used to show the characteristics of the study sample. Two sample t-tests were used to compare differences in mean values. The assumption of equal variances was verified. Differences in percentages were compared using χ2-tests. Analysis of variance was used to obtain mean values of each descriptive variable for each category of SES. Differences in mean total values across the groups were evaluated using F-tests.
Rates of CVD hospital admissions and deaths stratified by social class were calculated using χ2-tests for linear trend to assess statistical significance. Cox’s proportional hazards regression [21] was used to examine the relationship between social class and CVD incidence, adjusting for cardiovascular risk factors. The proportionality assumption was assessed using Nelson-Aalen plots and by testing for evidence of a statistical interaction with the time scale of the models. There was no evidence of any violation of the proportionality assumption in any models. Wald tests were used to examine the effect of social class in each model. For the purpose of this study, follow-up for an individual began at the date of the first health check. Results will be presented for incidence up to 31st July 2006, about 10 years average follow-up time from the first health check.
All statistical analyses were performed separately for men and women using Stata version 8.0.
Results
Of the 25,639 participants who attended the health check, 570 with no details of their last occupation, one who had died but had no date of death was available, and 13 who were admitted to hospital between agreeing to participate and attending the health check, were excluded. A further 2,362 participants who reported prevalent heart attack, stroke, and cancer at baseline were excluded to avoid reverse causality. Another 215 participants with missing data for the covariates BMI and smoking were also excluded, leaving a total of 22,478 men and women in the current analyses. There were 5,192 cardiovascular deaths and hospital admissions during the follow up period (225,537 Person-years), 27% of these were deaths.
Descriptive characteristics of the cohort by sex are displayed in Table 1. Men were on average slightly older, taller and had higher BMIs than women. The proportion of current smokers in each sex was similar, a greater proportion of men were former smokers, while a greater proportion of women have never smoked. A greater proportion of men finished school, and a greater proportion had a history of diabetes. Mean blood pressure was greater in men, while total mean cholesterol and plasma vitamin C levels were greater in women. Levels of physical inactivity were similar in men and women; more women were classed as moderately inactive, while more men were considered active. On average men drank over twice as many units of alcohol per week as women.
Table 2 shows the descriptive characteristics of the cohort by social class in men and women. Similar patterns were seen in both sexes. The proportion of current smokers increased with decreasing social class. Plasma vitamin C levels and the proportion of participants who finished school decreased with decreasing social class. There was some suggestion that mean age, BMI and systolic blood pressure increased with decreasing social class but the range of values was minimal. Diabetes prevalence and total cholesterol did not vary linearly with social class. In women mean weekly intake of alcohol decreased with decreasing social class.
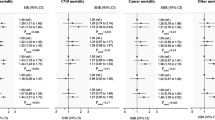
Table 3 shows the rates and adjusted relative risks for CVD incidence by social class in men and women. There was strong evidence of an inverse association between risk of CVD and social class in both men and women. In men the association was somewhat attenuated by adjustment for smoking and classical risk factors. Further adjustment for lifestyle covariates had little effect. The association was independent of education. In women adjustment for smoking somewhat attenuated the association, while there was little effect of adjusting for classical cardiovascular risk factors, and some attenuation after further adjustment for lifestyle factors. After adjustment for educational level women in social class V were still at an increased risk of CVD incidence compared to those in class I.
Adjusted relative risks for cardiovascular incidence by social class stratified by retirement age are shown in Table 4 for men and women. There is evidence of a strong social class effect on CVD in both men and women aged ≥65 years. This association is somewhat attenuated by adjustment for classical and lifestyle risk factors, and for education, but remains highly significant. Point estimates show an apparent gradient in younger men and women, although this is non-significant.
Discussion
In men we found an inverse association between risk of CVD and social class that was not explained by classical or lifestyle risk factors, despite socioeconomic differentials in these risk factors. There was some attenuation after adjustment for smoking, however consistent with previous research [4, 22–24] a socioeconomic gradient remained unexplained. The association was also independent of education.
In women risk of CVD increased with decreasing social class, some of this association was explained by classical and lifestyle risk factors. After full adjustment the effect was smaller than that seen in men. The smaller effect might be due to the smaller number of events meaning a lack of power, or this may partly reflect more difficulty in classifying social class in women. Some controversy exists over whether a woman’s social class should be graded using her own occupation or that of her husband [25–28]. Arguments for grading according to a woman’s own occupation are that the standard of living in the household may be influenced by a woman’s earnings, or her job may expose her to health hazards [29]. However, no clear difference between the two measures has been shown in women aged >60, and a stronger association was seen with husband’s social class in women aged 20–59 years [25, 27, 30]. Thus husband’s social class was considered an appropriate classification in this cohort. A weaker socioeconomic mortality gradient in women is consistent with much of the literature [31–36].
Reducing health inequalities is currently a key priority in the UK, however the appropriate focus for policies is less clear. Although changing individual health behaviours is an important public health goal, research implies that socioeconomic differentials are due to a wider range of factors and thus would persist even with improved health behaviour among the disadvantaged. Social class reflects experiences and exposures in adult life. It represents the material resources relevant for health and status, as well as aspects relevant to job characteristics, for example psychosocial aspects such as the degree of control over work, or physical risks such as occupational injury, or exposure to toxic substances [37, 38]. Current social class is also strongly related to childhood and parental social class and may well also reflect early life influences.
Retirement
Further stratification showed that in both men and women the social class association persisted and even appeared stronger in individuals aged 65 years and over. Point estimates show an apparent gradient in younger men and women that might be non-significant due to small numbers. Social class is a measure based upon occupation, thus its strong effect on CVD risk among those aged 65 years and older, the majority of whom would have retired, is of interest. It suggests that the pathways through which social class influences risk of CVD persist beyond an individual’s working life.
Comparison to other UK studies
Our study shows a much smaller social class gradient in risk of CVD than others based on specific occupational groups such as the British Army [39], or the Whitehall studies, based on British civil servants working in London [6, 40–42]. Both Whitehall studies show a steep gradient across employment grade, with established risk factors only accounting for a small proportion of this risk gradient. The authors suggest that employment grade provides a more accurate classification of social class that produces more homogenous groups than national statistics [6, 24]. However the Whitehall populations were not representative of the general population, containing a more polarized social class distribution that may have contributed to the greater gradients observed [4, 24]. Our estimates of social class differences are slightly lower than those observed in national coronary heart disease and stroke mortality statistics [43]. However, they are similar to those from the British Regional Heart Study [4, 24] which had comparable social class distribution to the national population of males at that time, and to the Scottish Heart Health Study [7].
Strengths and limitations
There are a number of limitations to this study. Prevalent severe illness, such as coronary heart disease, stroke or cancer is associated with a higher risk of mortality and may also cause a downward drift in social class, or individuals may be less likely to be upwardly mobile. While individuals with medical conditions that could potentially have confounded the relationship between SES and CVD incidence were excluded from the analyses, we cannot exclude the possible effect of prevalent subclinical disease that may explain some of the association. Although we examined how far a number of classical and lifestyle risk factors might account for some of the socioeconomic differential, we did not examine the roles of all potential factors, such as psychosocial factors that might explain some of the differences. We recognise the importance of such factors in explaining the socioeconomic differential, but wished to confine our analyses to examining the influence of the main classical and lifestyle risk factors.
Mortality and morbidity were ascertained using a regular record linkage system with national deaths registration. This method is one of the most frequently used in epidemiological studies [44]. While this may have missed some cardiovascular events, the specificity of events identified using this method is high [20]. Occupation details were obtained at the baseline survey between 1993 and 1997. Some degree of inaccuracy in reporting or recording this information is inevitable, however it seems unlikely that misclassifications would be non-random, and normally random measurement error is likely only to attenuate any relationships, not produce spurious relationships [45]. Although it has been shown that situations exist where random misclassification can bias odds ratios for categories at intermediate levels of risk away from or beyond the null [46], these examples largely relate to case–control studies which have recognised issues in estimating odds ratios. The misclassification patterns that produce this effect are more extreme than those found in most epidemiological studies, particularly cohort studies, so we do not think this is likely.
The socioeconomic differentials in CVD incidence are not as wide as have been reported in some other studies. This may reflect attenuation due to misclassification of social class as discussed. Alternatively, it is possible that in Norfolk the socioeconomic differentials may reflect less variation in lifestyles such as diet and physical activity than in more urban environments.
EPIC-Norfolk is composed of participants willing to complete detailed questionnaires and attend health checks, and the response rate was quite low at about 45% [47], thus selection bias may be a problem if non response was associated with social class or with cardiovascular health status given a certain social class. It is possible that we may have selected a health conscious study cohort, particularly in the lower social classes, and thus there may be some attenuation of the socioeconomic differential in our results. However the range of socioeconomic circumstances of the participants was wide [12, 48], and in terms of anthropometric variables, serum lipids and blood pressure [11] and of physical and mental functional health [49], the cohort was similar to the general resident population in England, although there were fewer current smokers. Selection of a more health conscious cohort would mean that the external generalisability of the study results may be affected, but the internal validity of the study results should not be affected. Excluding those with unclassified or missing data for SES or CVD incidence could cause bias, but only if these people differed from those included in the study with respect to the relation between SES and morbidity, which seems unlikely.
Conclusions
Some but not all of the socioeconomic differential in CVD incidence can be explained by potentially modifiable classical and lifestyle risk factors. Low social class remains a risk factor for CVD after age 65 years. Further understanding of the mechanisms underlying the association is needed if we are to reduce inequalities in health.
Abbreviations
- BMI:
-
Body mass index
- CVD:
-
Cardiovascular disease
- EPIC-Norfolk:
-
European Prospective Investigation of Cancer and Nutrition
- ICD:
-
International Classification of Disease
- SES:
-
Socioeconomic status
References
British Heart Foundation. 2007 Coronary Heart Disease Statistics. British Heart Foundation. 2007.
Marmot MG, Adelstein AM, Robinson N, Rose GA. Changing social-class distribution of heart disease. Br Med J. 1978;2(6145):1109–12.
Heller R, Williams H, Sittampalam Y. Social class and ischaemic heart disease: use of the male:female ratio to identify possible occupational hazards. J Epidemiol Community Health. 1984;38(3):198–202.
Emberson JR, Whincup PH, Morris RW, Walker M. Social class differences in coronary heart disease in middle-aged British men: implications for prevention. Int J Epidemiol. 2004;33(2):289–96.
Coulthard M, Chow Y, Dattani N, White C, Baker A, Johnson B. Health. In: Babb Penny, Martin Jean, Haezewindt P, editors. Focus on social inequalities. London: Office for National Statistics; 2004. p. 69–84.
Rose G, Marmot MG. Social class and coronary heart disease. Br Heart J. 1981;45(1):13–9.
Woodward M, Shewry MC, Cairns S, Smith W, Tunstall-Pedoe H. Social status and coronary heart disease: results from the Scottish heart health study. Prev Med. 1992;21(1):136–48.
Kaplan GA, Keil JE. Socioeconomic factors and cardiovascular disease: a review of the literature. Circulation. 1993;88(4 pt 1):1973–98.
Myint PK, Luben RN, Welch AA, Bingham SA, Wareham NJ, Khaw KT. Effect of age on the relationship of occupational social class with prevalence of modifiable cardiovascular risk factors and cardiovascular diseases. A population-based cross-sectional study from European Prospective Investigation into Cancer—Norfolk (EPIC-Norfolk). Gerontology 2006;52(1):51–8.
McFadden EC, Luben RN, Wareham NJ, Bingham SA, Khaw KT. Occupational social class, educational level, smoking and body mass index, and cause-specific mortality in men and women: a prospective study in the European Prospective Investigation of Cancer and Nutrition in Norfolk (EPIC-Norfolk) cohort. In press 2008.
Day N, Oakes S, Luben R, Khaw KT, Bingham S, Welch A, et al. EPIC-Norfolk: study design and characteristics of the cohort. European Prospective Investigation of Cancer. Br J Cancer. 1999;80(1):95–103.
Shohaimi S, Luben R, Wareham N, Day N, Bingham S, Welch A, et al. Residential area deprivation predicts smoking habit independently of individual educational level and occupational social class. A cross sectional study in the Norfolk cohort of the European Investigation into Cancer (EPIC-Norfolk). J Epidemiol Community Health. 2003;57(4):270–6.
Elias P, Halstead K, Prandy K. CASOC: Computer-Assisted Standard Occupational Coding. London: HMSO; 1993.
Smith MR, Kinmonth A-L, Luben RN, Bingham S, Day NE, Wareham NJ, et al. Smoking status and differential white cell count in men and women in the EPIC-Norfolk population. Atherosclerosis 2003;169(2):331–7.
Sargeant L, Wareham N, Bingham S, Day N, Luben R, Oakes S, et al. Vitamin C and hyperglycemia in the European Prospective Investigation into Cancer–Norfolk (EPIC-Norfolk) study: a population-based study. Diabetes Care. 2000;23(6):726–32.
Sargeant LA, Khaw K-T, Bingham S, Day NE, Luben RN, Oakes S, et al. Cigarette smoking and glycaemia: the EPIC-Norfolk study. Int J Epidemiol. 2001;30(3):547–54.
Wareham NJ, Jakes RW, Rennie KL, Mitchell J, Hennings S, Day NE. Validity and repeatability of the EPIC-Norfolk physical activity questionnaire. Int J Epidemiol. 2002;31(1):168–74.
Wareham NJ, Jakes RW, Rennie KL, Schuit J, Mitchell J, Hennings S, et al. Validity and repeatability of a simple index derived from the short physical activity questionnaire used in the European Prospective Investigation into Cancer and Nutrition (EPIC) study. Public Health Nutr. 2003;6(4):407–13.
Khaw K-T, Jakes R, Bingham S, Welch A, Luben R, Day N, et al. Work and leisure time physical activity assessed using a simple, pragmatic, validated questionnaire and incident cardiovascular disease and all-cause mortality in men and women: The European Prospective Investigation into Cancer in Norfolk prospective population study. Int J Epidemiol. 2006;35(4):1034–43.
Boekholdt SM, Ron JGP, Nicholas ED, Robert L, Sheila AB, Nicholas JW, et al. Macrophage migration inhibitory factor and the risk of myocardial infarction or death due to coronary artery disease in adults without prior myocardial infarction or stroke: the EPIC-Norfolk prospective population study. Am J Med. 2004;117(6):390–7.
Cox DR. Regression models and life tables. J R Stat Soc (B). 1972;34:187–220.
Steenland K, Henley J, Thun M. All-cause and cause-specific death rates by educational status for two million people in two American Cancer Society cohorts, 1959–1996. Am J Epidemiol. 2002;156(1):11–21.
Bucher HC, Ragland DR. Socioeconomic indicators and mortality from coronary heart disease and cancer: a 22-year follow-up of middle-aged men. Am J Public Health. 1995;85(9):1231–6.
Pocock SJ, Shaper AG, Cook DG, Phillips AN, Walker M. Social class differences in ischaemic heart disease in British men. Lancet. 1987;2(8552):197–201.
Arber S, Ginn J. Gender and inequalities in health in later life. Soc Sci Med. 1993;36(1):33–46.
Arber S, Lahelma E. Inequalities in women’s and men’s ill-health: Britain and Finland compared. Soc Sci Med. 1993;37(8):1055–68.
Martikainen P, Kauppinen TM, Valkonen T. Effects of the characteristics of neighbourhoods and the characteristics of people on cause specific mortality: a register based follow up study of 252,000 men. J Epidemiol Community Health. 2003;57(3):210–7.
Krieger N, Chen J, Selby J. Comparing individual-based and household-based measures of social class to assess class inequalities in women’s health: a methodological study of 684 US women. J Epidemiol Community Health. 1999;53(10):612–23.
Fein O. The influence of social class on health status: American and British research on health inequalities. J Gen Intern Med. 1995;10(10):577–86.
Arber S. Class, paid employment and family roles: Making sense of structural disadvantage, gender and health status. Soc Sci Med. 1991;32(4):425–36.
Gregorio DI, Walsh SJ, Paturzo D. The effects of occupation-based social position on mortality in a large American cohort. Am J Public Health. 1997;87(9):1472–5.
Bopp M, Minder CE. Mortality by education in German speaking Switzerland, 1990–1997: results from the Swiss National Cohort. Int J Epidemiol. 2003;32(3):346–54.
Koskinen S, Martelin T. Why are socioeconomic mortality differences smaller among women than among men? Soc Sci Med. 1994;38(10):1385–96.
Mackenbach JP, Kunst AE, Groenhof F, Borgan JK, Costa G, Faggiano F, et al. Socioeconomic inequalities in mortality among women and among men: an international study. Am J Public Health. 1999;89(12):1800–6.
Manor O, Eisenbach Z, Israeli A, Friedlander Y. Mortality differentials among women: the Israel Longitudinal Mortality Study. Soc Sci Med. 2000;51(8):1175–88.
Stronks K, Van De Mheen H, Van Den Bos J, Mackenbach JP. Smaller socioeconomic inequalities in health among women: the role of employment status. Int J Epidemiol. 1995;24(3):559–68.
Martikainen P, Blomgren J, Valkonen T. Change in the total and independent effects of education and occupational social class on mortality: analyses of all Finnish men and women in the period 1971–2000. J Epidemiol Community Health. 2007;61(6):499–505.
Adler NE, Newman K. Socioeconomic disparities in health: pathways and policies. Health Aff. 2002;21(2):60–76.
Lynch P, Oelman BJ. Mortality from coronary heart disease in the British army compared with the civil population. Br Med J (Clin Res Ed). 1981;283(6288):405–7.
Marmot M, Rose G, Shipley M, Hamilton P. Employment grade and coronary heart disease in British civil servants. J Epidemiol Community Health. 1978;32(4):244–9.
Marmot MG, Smith GD, Stansfeld S, Patel C, North F, Head J, et al. Health inequalities among British civil servants: the Whitehall II study. Lancet. 1991;337(8754):1387–93.
Marmot M, Shipley M, Brunner E, Hemingway H. Relative contribution of early life and adult socioeconomic factors to adult morbidity in the Whitehall II study. J Epidemiol Community Health. 2001;55(5):301–7.
British Heart Foundation. Age-standardised death rates from CHD and stroke by sex and social class, 1976/81 to 1997/99, England and Wales. 2007 [updated 2007; cited 2007 15/10]; Available from: http://www.heartstats.org/temp/Tabsp1.8spweb07.xls.
Kunst AE, Mackenbach JP. Measuring socioeconomic inequalities in health; Copenhagen: World Health Organisation, 1995.
Flegal KM, Brownie C, Haas J. The effects of exposure misclassification on estimates of relative risk. Am J Epidemiol. 1986;123(4):736–51.
Dosemeci M, Wacholder S, Lubin JH. Does nondifferential misclassification of exposure always bias a true effect toward the null value? Am J Epidemiol. 1990;132(4):746–8.
Myint PK, Luben RN, Surtees PG, Wainwright NWJ, Welch AA, Bingham SA, et al. Relation between self-reported physical functional health and chronic disease mortality in men and women in the European Prospective Investigation Into Cancer (EPIC-Norfolk): a prospective population study. Ann Epidemiol. 2006;16(6):492–500.
Wainwright NWJ, Surtees PG. Places, people, and their physical and mental functional health. J Epidemiol Community Health. 2004;58(4):333–9.
Surtees PG, Wainwright NW, Khaw KT. Obesity, confidant support and functional health: cross-sectional evidence from the EPIC-Norfolk cohort. Int J Obes Relat Metab Disord. 2004;28(6):748–58.
Acknowledgments
We thank the participants and general practitioners who took part in the study and the staff of EPIC-Norfolk.
Funding
EPIC-Norfolk is supported by research programme grant funding from the Cancer Research Campaign and Medical Research Council with additional support from the Stroke Association, British Heart Foundation, and Research Into Ageing.
Competing interests
None declared.
Contributors
KTK, SB, and NW are principal investigators in the EPIC-Norfolk population study. SB is responsible for the dietary measurements and analyses. RL is responsible for data management and computing and data linkages for post coding. EM conducted the data analyses and wrote the paper with KTK with contributions from other co-authors.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
McFadden, E., Luben, R., Wareham, N. et al. Occupational social class, risk factors and cardiovascular disease incidence in men and women: a prospective study in the European Prospective Investigation of Cancer and Nutrition in Norfolk (EPIC-Norfolk) cohort. Eur J Epidemiol 23, 449–458 (2008). https://doi.org/10.1007/s10654-008-9262-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10654-008-9262-2