
Abstract
The objective was to examine the relationships of self-reported physical activity (PA) by domain (leisure, occupational, other) with PA and sedentary time as measured objectively by accelerometry. Subjects were adults with low habitual PA levels from a community in northern France. Among subjects in the lowest tertile of a PA score from a screening questionnaire, 160 (37% males, age: 41.0 ± 10.8 years, BMI: 25.1 ± 4.1 kg/m2, mean ± SD) completed a detailed instrument (Modifiable Activity Questionnaire), and wore an accelerometer (Actigraph) for seven consecutive days. Relationships between questionnaire domains (occupational, leisure, and “non-occupational non-leisure”) and accelerometry measures (total activity and sedentary time) were assessed using Spearman correlation coefficients. In this population, the highest contributor to total reported PA (h/week) was occupational PA. Time spent in non-occupational non-leisure PA ranked second in women and third in men. The most frequent non-occupational non-leisure PA were shopping and household chores. In women, non-occupational non-leisure PA contributed more than occupational or leisure-time PA to total PA energy expenditure (median: 18.0, 9.1, and 4.9 MET-h/week, respectively). Total PA by accelerometry (count/day) was correlated to leisure-time PA in women (r = 0.22, P < 0.05) and to occupational (r = 0.43, P < 0.01) and total reported PA (r = 0.39, P < 0.01) in men (all in MET-h/week). There was an inverse relationship between accelerometry sedentary time (h/day) and non-occupational non-leisure PA (MET-h/week, r = −0.30, P < 0.001). These findings indicate the importance of assessing non-occupational non-leisure PA for a better understanding of how individuals partition their time between active or sedentary occupations.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Insufficient daily physical activity (PA) is emerging as an important public health concern [1]. It is a modifiable risk factor for chronic diseases such as cardiovascular disease, type 2 diabetes mellitus, and certain types of cancer [2–4]. Public health recommendations stress the benefits of accumulating 30 min or more of at least moderate-intensity PA on most days of the week [2–4]. In countries from the European Union, data from the Eurobarometer 2002 survey suggest that as much as two thirds of the adult populations are insufficiently active for optimal health benefits [5]. In France, a 2005 telephone survey in 8,708 representative subjects (15–74 year), indicated a prevalence of sufficient PA for health benefits of 52.1% in men and 39.5% in women [6]. From a public health perspective, the most inactive segments of the population thus represent a large at-risk group.
Another important concept is the limitation of sedentary time [7]. Sedentary time represents the duration of occupations that expend very little energy above resting metabolic rate, e.g., sitting, TV viewing, playing video games, reading… Sedentary behavior and low PA levels represent complementary aspects of human movement behavior and are independent risk factors for major chronic diseases such as type 2 diabetes [8] or metabolic disease markers [9].
Public health recommendations emphasize the importance of PA accumulated in the various settings of daily living, including leisure and sports, work, transport, or home [2–4]. As indicated in a recent update [3], activity can be accumulated “from bouts lasting 10 or more min”, which should facilitate incorporation of PA in daily life. There is currently increasing interest in PA performed outside leisure and work [10–17]. Previous reports have shown that domestic PA can significantly contribute to the daily PA amount required to confer health benefits [6, 10, 14–18]. Higher domestic PA was found associated with lower levels of cardiovascular risk factors in post menopausal women [12]. “Non-leisure” PA such as household chores explained most of the associations between cardiovascular disease mortality and PA in Canadian women [17]. However, the contribution of non-occupational non-leisure PA to total PA in different settings and populations remains insufficiently defined.
Questionnaires, and increasingly motion sensors, are used for assessment of habitual PA and sedentary behavior at population level [19, 20]. Only questionnaires can provide contextual information on different PA domains such as occupational, leisure, transportation, and domestic PA. Motion sensors such as accelerometers provide objective data on PA intensity, frequency, and duration [19–22]. Accelerometers also give objective information at the lower end of the activity spectrum and specific cut-offs have been proposed as a measure of sedentary time [23]. Therefore, the combined use of self-report and objective methods allows for better understanding of the characteristics of PA and sedentary behaviors. The relation of non-occupational non-leisure PA to accelerometry recordings is, however, unknown.
In this study, we used a population-based dataset on PA behavior and sedentary time obtained with both questionnaire and accelerometer in French adults with low habitual PA levels. First, we describe in these subjects the contribution of non-occupational non-leisure PA to total PA. Second, we report the cross-sectional relationships of the different PA domains (occupational, leisure, and non-occupational non-leisure) as assessed by questionnaire with objective measures of total PA and sedentary time as provided by accelerometry.
Methods
Setting
The present study is part of a PA intervention project in insufficiently active adults (the ETAP study, French acronym for “Action-study for promotion of physical activity”) developed in the framework of a larger ongoing research project, the Fleurbaix-Laventie Ville-Santé (FLVS) study [24]. The study included in 2002 a detailed assessment of health status and lifestyle of about 1,500 adults living in two towns in northern France, Fleurbaix and Laventie.
Participants
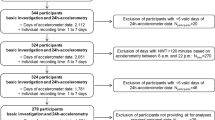
Adults (n = 1,421), aged 18–74 year, from Fleurbaix and Laventie (about 20% of the total population), volunteered to be screened for health status after a call in the local medias. Data collected included self-reported habitual PA. We used the short last-7 day recall International Physical Activity Questionnaire (IPAQ) [25, 26] as a screening tool to identify the least physically active subjects. This instrument consists of seven questions assessing vigorous, moderate-intensity, and walking activity in everyday life. We used the sum of [(vigorous PA min/week * 2) + (moderate PA min/week) + (walking min/week)] as an indicator of total PA [25]. Subjects classified in the lowest tertile of this total PA score were considered eligible for the study (n = 443). Subjects medically unfit for a PA promotion intervention (i.e., reporting either personal history of coronary artery disease, chest pain, peripheral artery disease, respiratory insufficiency, dyspnea at rest, joint pain, or any disease limiting mobility) were not included (n = 103). Research assistants then met 340 subjects at their home for additional query and 160 agreed to participate in the study. There was no significant difference in age, sex ratio, BMI, and IPAQ-derived data between included subjects and those who refused (data not shown).
Data collection
The study protocol was approved by the regional ethics committee (Lille, France) and all participants gave written informed consent. On the day of inclusion, trained staff administered a detailed PA questionnaire during a face-to-face interview and provided subjects with an accelerometer. The following data had been collected during an earlier visit at home in the framework of the FLVS project: body weight in light clothes to the nearest 0.1 kg using a bipedal bio-electrical impedance device (Tanita TBF 310 model, Tanita, Courbevoie, France), standing height (without shoes) to the nearest cm using a portable stadiometer, educational level (three categories: (1) primary school level, ≤9 years of education (low); (2) completed ≥2 years of high school, 10–11 years of education (intermediate); and (3) university studies (high), >11 years of education), and smoking status (former, current, or non smoker).
Modifiable activity questionnaire
We used the French version [27] of the Modifiable Activity Questionnaire [28] to obtain detailed data about habitual PA and sedentary behaviors. The MAQ designed by Kriska et al. [28] assesses past-year PA during leisure-time and at work as well as time spent viewing TV/video as a proxy for sedentary behavior. Criterion validity of the MAQ has been assessed against doubly labelled water [29]. Eighteen individuals (12 employed) had total energy expenditure (TEE) measured with the doubly labelled water technique and also answered the MAQ. Leisure activity (MET-h/week) correlated with the ratio TEE/resting metabolic rate (r = 0.56, P = 0.01). Occupational activity (MET-h/week) correlated with the ratio TEE/sleeping metabolic rate (r = 0.52, P = 0.03). Test–retest properties have also been assessed by Kriska et al. [28]. Twenty-nine subjects aged 21–36 year completed the MAQ twice, 1–3 weeks apart. Correlations coefficients (Spearman) ranged from 0.62 to 0.96 for leisure and occupational activity [28]. The questionnaire has been described elsewhere [9, 27, 28, 30]. Briefly, for leisure-time PA, subjects were asked to report all activities that had been performed at least 10 times for 10 min each session over the past 12 months. Then, detailed information was collected about the frequency and duration of each activity reported. After multiplying the number of h/week of each leisure by its estimated metabolic cost (in MET), an energy-expenditure indicator was obtained, expressed in MET-h/week of leisure-time PA. A MET is the ratio of the working metabolic rate of an activity divided by the resting metabolic rate [2]. MET values were drawn from the compendium published by Ainsworth et al. [31]. The assessment of occupational PA was based on the number of hours that the individual participated in physically demanding activities during an average workday, for each job held over the past year. The number of hours in each of three categories of occupational PA (light, moderate, and hard) was multiplied by an average group MET value (2, 4, and 7 METs, respectively) and then summed, resulting in a final occupational activity estimate expressed in MET-h/week. The questionnaire also enquired about the time spent daily at home watching TV/video, playing video games, using a computer, or reading (for leisure). Time spent watching TV/video or playing video games and time spent using a computer were summed in an indicator termed “screen viewing” expressed in h/week.
The original version of the MAQ only explored PA during leisure-time and at work. To also take into account PA unrelated to occupation or leisure and that was carried in, around, or afar the household, subjects were asked to report all “non-occupational non-leisure” PA that had been performed at least 10 times for 10 min each session over the past 12 months. This PA category included mainly shopping, household chores, and work for non-profit association. To collect these additional data, we used the same format as used for the questions in the occupational section of the MAQ.
Accelerometry
Physical activity was objectively assessed using the Actigraph accelerometer (model 7164, Manufacturing Technology, Inc., FL, USA) [32]. The Actigraph measures integrated accelerations associated with movement in the vertical plane. The recorded signal is amplified and filtered and results in a subsequent signal that is scored as an “activity count” over a user specified time interval (epoch). Here, 60 s epochs were used. The Actigraph was worn in a nylon pouch secured to a belt at the waistline. Participants were instructed to wear the Actigraph for seven consecutive days during all waking hours except during water-based activities.
In order to analyse meaningful information, only days with at least 8 h of recording time were considered valid. Only participants who had at least 4 days of valid recordings were included in this analysis. The Actigraph data were reduced with custom software developed in-house on SAS program (SAS, version 9.1, SAS Institute Inc., Cary, NC) for this and similar on-going PA research projects [33]. Based on previous literature [23, 25, 32], cut-points below 100 counts/min, over 1,952 counts/min, and over 5,724 counts/min, were used to quantify sedentary time, time spent in moderate PA, and time spent in vigorous PA, respectively. The software also identified “bouts” of PA, defined by duration of at least ten consecutive minutes spent in moderate or vigorous PA. As there were missing data due to malfunctioning accelerometers or non-compliance of participants, 141 accelerometer recordings (88%) were included in the present analyses.
Statistical analysis
Data are reported as mean value ± standard deviation or median ± inter-quartile range (1st–3rd quartiles: Q1–Q3) for normally and non-normally distributed variables, respectively. Relationships between habitual PA data obtained with the MAQ and the Actigraph were assessed using Spearman correlation coefficients. All analyses were performed using SAS software (SAS, version 9.1, SAS Institute Inc., Cary, NC).
Results
Table 1 shows the characteristics of the study population. Subjects were aged 19–63 years. Employed subjects represented 74.7% of the population (83.3% of men and 69.8% of women). Occupations included “assistant non-manual employees” (36.4%), “higher civil servants and executives” (29.5%), “non-manual employees” (26.1%), and “employed and self-employed professionals” (4.5%), “manual workers” (2.3%), “farmers” (1.1%). The “not employed” group (23.1%) included “students” (40.5%), “housewives” (29.7%), “retired” subjects (16.2%), those currently unemployed (5.4%), and those who could not be classified (8.1%).
Table 2 displays past-year habitual PA data as assessed by the MAQ. When expressed in h/week, occupational PA ranked first in both genders. It was followed, in men, by leisure-time PA and, in women, by non-occupational non-leisure PA. When expressed in MET-h/week, non-occupational non-leisure PA ranked first in women, whereas, in men, occupational PA remained the highest contributor to total PA. Leisure-time PA of moderate intensity represented the major part of total leisure PA in both genders. The most frequently reported leisure-time PA were gardening (reported by 60.3% of men and 37.4% of women), do-it-yourself activities (e.g., interior wall painting, furniture repair…; 58.6% of men and 18.2% of women), walking (51.7% of men and 59.6% of women), swimming (31% of men and 27.3% of women), and cycling (27.6% of men and 25.3% of women). In men, leisure-time PA with the highest durations were do-it-yourself activities, gardening, and walking. In women, leisure-time PA with the highest durations were walking, gardening, and do-it-yourself activities. The most frequently reported non-occupational non-leisure PA were shopping (27.6% of men and 22.4% of women) and household chores (22.4% of men and 59.6% of women).
Table 3 shows daily PA data as measured by the Actigraph. Sedentary time averaged 7 h and 17 min, accounting for about 52.8% of the total daily recording duration. There was only little PA that was registered as being moderate or vigorous. These values were especially low when the criterion for bout PA, i.e., ten consecutive minutes above the threshold for a given intensity of PA, was used. Time spent in moderate PA was similar in men and women. Time spent in vigorous PA, as well as sedentary time, was higher in men than women.
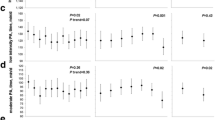
Table 4 lists the correlations between questionnaire domains (occupational, leisure, and “non-occupational non-leisure” PA and “screen viewing” time) and accelerometry (total activity and sedentary time). In women, total PA (in counts/day) was positively associated with total leisure-time PA (in h/week) and moderate intensity leisure-time PA (in MET-h/week). In men, total PA (in counts/day) was positively associated with occupational and total PA (in MET-h/week). In all subjects combined, total accelerometry-assessed PA (in counts/day) was also positively associated with total reported PA (in MET-h/week). In all subjects combined, and in women, accelerometry-measured sedentary time was inversely related with non-occupational non-leisure PA and with total PA (both in MET-h/week). Accelerometry-measured sedentary time was not significantly related to the reported screen viewing time (P < 0.1).
Discussion
In this study, we used both self-reported (questionnaire) and objectively measured (accelerometry) data to assess PA and sedentary patterns in an adult population characterized by low activity levels. Our aim was to assess the contribution of different PA domains to total PA and their relationships with accelerometry-measured total PA and sedentary time. In men and women combined, self-reported past-year non-occupational non-leisure PA contributed more to total reported PA than leisure-time PA. Non-occupational non-leisure PA was inversely correlated with sedentary time as assessed by accelerometry. The accelerometry counts correlated with moderate intensity leisure-time PA in women, and with occupational PA in men. Of note is the fact that occupational PA was twofold higher in men than in women in this population with low overall and leisure PA levels.
Both counts data and reported time spent in each PA domain confirmed our subjects had low habitual PA level. Field studies of one-week duration with the Actigraph found higher PA levels than those reported herein. In a population of similar age and BMI (n = 185), Ekelund et al. [23] reported total activity of 443 ± 153 and 473 ± 151 counts/min versus 338 ± 139 and 336 ± 100 counts/min in our study, in men and women, respectively. In another population of similar age and BMI, Cooper et al. [34] also reported higher counts data than those reported herein. Similarly, previous studies of past-year PA using the MAQ in adults reported higher levels of PA. Participants in the Diabetes Prevention Program [35], who were older and more obese than our study subjects, reported a mean of 16.3 MET-h/week of leisure-time PA versus 6.1 MET-h/week in our study. In data derived from the cohort of the French SU.VI.MAX study, obtained from a middle-aged population, leisure-time PA was 12 MET-h/week and occupational PA was 41.5 MET-h/week versus 6.1 and 15.4 MET-h/week in the present study, respectively [27].
In this study we investigated PA that was neither occupational nor leisure-time related, a PA domain which we termed “non-occupational non-leisure” PA. This terminology may prevent overlap between PA domains. Indeed some “domestic” activities (e.g., do-it-yourself, gardening) are also considered as “leisure-time” PA. Whereas domestic PA is usually defined as activities carried out only in and around the household [16], the non-occupational non-leisure PA domain encompasses activities that can also be performed away from the household. An example of such activities is shopping, found here to be an important contributor to this PA domain. However, the contribution of non-occupational non-leisure PA to total reported PA appeared modest, especially in men. It has been previously reported that household PA contributes more to total energy expenditure in women than in men [11]. Non-occupational non-leisure PA did not correlate significantly with the objective measure of total PA. In women, although time spent in non-occupational non-leisure PA was much higher than the time spent in leisure-time PA, only the latter correlated with the accelerometry measure of total PA. Therefore, these activities could only contribute in a minor way to the total counts despite their prolonged duration. We might have overestimated the true metabolic cost associated with the non-occupational non-leisure PA. In line with this hypothesis, Brooks et al. [18] showed that the intensity of self-paced household chores performed by women was lower at home than in a laboratory environment.
We observed that total reported PA correlated with total daily activity counts recorded by the accelerometer. This association was significant in the whole sample population but was more apparent in men. Such a relationship is in line with early validation data by Kriska et al. [28] comparing total PA assessed with the MAQ to the Caltrac accelerometer output in Pima Indians. The fact that our population was relatively homogeneous and recruited to have low PA levels may explain in part that the correlation found here was low (Spearman r = 0.18 for total reported PA in MET-h/week). Considering PA domains separately, the correlations found by Kriska et al. [28] were higher than those reported here (in MET-h/week, Spearman r = 0.44 vs. r = 0.09 for leisure-time PA, and r = 0.41 vs. r = 0.22 for occupational PA, respectively). The persistent engagement of the Pima population in physically demanding occupations at the time of the study by Kriska et al. [28] may account for the higher correlations observed in this domain.
There was also a consistent pattern of negative relationships between total reported PA and sedentary time as assessed by the accelerometer. This is not in agreement with the notion that subjects with higher PA levels may compensate by increased sedentary periods in other parts of their day [36]. More specifically, this relationship appeared to be linked to the non-occupational non-leisure PA domain, as neither leisure-time nor occupational PA were significantly correlated with sedentary time. This suggests the importance of considering PA performed in this context when targeting a decrease in sedentary behavior. Public health recommendations insist on daily living PA as a starting point to exchange sedentary behaviors for active ones [2–4].
Using accelerometry as an objective measure of PA allowed us to analyze bouts of PA. Based on public health PA recommendations [3, 21], we used a ten consecutive minutes accumulation criteria to define such bouts. Applying this criterion resulted in a tenfold decrease in the mean number of hours spent in moderate or vigorous PA. A change of this magnitude is likely to have a very strong impact in analyses of PA categories and of relationships with health outcomes in future studies. It may therefore be questioned whether such a 10 min criterion is appropriate when analyzing accelerometry data. To our knowledge, there is, however, no consensus on how to extract bouts of PA from the raw activity count data. There are also very few data to which we can compare our results.
Another finding was the discrepancy between self-reported and measured PA duration. Noticeably, the duration of reported moderate leisure-time PA was longer than measured moderate intensity bout PA. Although it is specified with the MAQ that only activities performed for at least 10 min are to be reported, it appears that the notion of PA bout derived from self-report and from motion sensors such as accelerometers is very different. Of note, the MAQ in total captured less than half of the time that the accelerometers were worn. Indeed, PA questionnaires appear better suited to investigate moderate and vigorous volitional activities than light intensity activities [20, 37]. Since our subjects had low habitual PA levels, this could partly explain the low correlation coefficients observed.
Some limitations to this work may be considered. First, accelerometry did not assess the same time period as recalled by the MAQ. However, both tools aim to assess “habitual PA” and accelerometer recordings in this study spanned over several days, including weekdays and weekends, as recommended [38, 39]. Second, as pointed out in a recent review about PA questionnaires validity [40], correlation coefficients may be imprecise if based on few observations and will depend on the degree of between-subject variability in a given population. However, as our population (n = 141) was relatively homogenous and recruited to have low PA levels, it is unlikely that the correlations found are exaggerated by high between-subject variability. Third, althought waist mounted accelerometers adequately detect dynamic activities (e.g., walking, running), they are less suitable for activities with a more important static component [41] and their validity may vary depending on the population studied. Conversely, recall bias is inherent to self-reported questionnaires and it is known that self-reported measures of PA are likely to contain errors of overreporting [20, 26]. In this study, questionnaires were interviewer-administered which may minimize this bias. Finally, study subjects were middle-aged men and women, with low PA levels, living in a semi-urban environment, which may limit the generalization of the findings to other populations or settings.
In conclusion, our results indicate that non-occupational non-leisure PA makes a more important quantitative contribution to total PA in women compared to men, in adults with low habitual PA levels. The non-occupational non-leisure PA domain is inversely correlated to sedentary time. This gives support to the notion that assessment of non-occupational non-leisure PA will help in understanding how individuals partition their time between active or sedentary behaviors. Such knowledge is much needed in the development of public health initiatives that aim to increase PA while reducing sedentary behaviors.
Abbreviations
- FLVS:
-
Fleurbaix-Laventie Ville-Santé
- IPAQ:
-
International physical activity questionnaire
- MAQ:
-
Modifiable activity questionnaire
- PA:
-
Physical activity
References
World Health Organization. World Health Report 2002: reducing risks promoting healthy life. Geneva: World Health Organization; 2002.
U.S. Department of Health and Human Services. Physical activity and health: a report of the surgeon general. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, S/N 017-023-00196-5; 1996.
Haskell WL, Lee IM, Pate RR, Powell KE, Blair SN, Franklin BA, et al. Physical activity and public health: updated recommendation for adults from the American college of sports medicine and the American heart association. Med Sci Sports Exerc. 2007;39:1423–34. doi:10.1249/mss.0b013e3180616b27.
Pate RR, Pratt M, Blair SN, Haskell WL, Macera CA, Bouchard C, et al. Physical activity and public health. A recommendation from the centers for disease control and prevention and the American college of sports medicine. JAMA. 1995;273:402–7. doi:10.1001/jama.273.5.402.
Sjöström M, Oja P, Hagströmer M, Smith BJ, Bauman A. Health-enhancing physical activity across European Union countries: the Eurobarometer study. J Public Health. 2006;14:291–300.
Escalon H, Vuillemin A, Erpalding ML, Oppert JM. Physical activity: between sports and sedentary behavior [in French]; Baromètre Santé 2005. Paris: Editions INPES; 2008.
Hamilton MT, Hamilton DG, Zderic TW. Role of low energy expenditure and sitting in obesity, metabolic syndrome, type 2 diabetes, and cardiovascular disease. Diabetes. 2007;56:2655–67. doi:10.2337/db07-0882.
Hu FB, Li TY, Colditz GA, Willett WC, Manson JE. Television watching and other sedentary behaviors in relation to risk of obesity and type 2 diabetes mellitus in women. JAMA. 2003;289:1785–91. doi:10.1001/jama.289.14.1785.
Bertrais S, Beyeme-Ondoua JP, Czernichow S, Galan P, Hercberg S, Oppert JM. Sedentary behaviors, physical activity, and metabolic syndrome in middle-aged French subjects. Obes Res. 2005;13:936–44. doi:10.1038/oby.2005.108.
Abu-Omar K, Rutten A. Relation of leisure time, occupational, domestic, and commuting physical activity to health indicators in Europe. Prev Med. 2008;47:319–23. doi:10.1016/j.ypmed.2008.03.012.
Dong L, Block G, Mandel S. Activities contributing to total energy expenditure in the United States: results from the NHAPS Study. Int J Behav Nutr Phys Act. 2004;1:4. doi:10.1186/1479-5868-1-4.
Greendale GA, Bodin-Dunn L, Ingles S, Haile R, Barrett-Connor E. Leisure, home, and occupational physical activity and cardiovascular risk factors in postmenopausal women. The Postmenopausal estrogens/progestins intervention (PEPI) Study. Arch Intern Med. 1996;156:418–24. doi:10.1001/archinte.156.4.418.
Lawlor DA, Taylor M, Bedford C, Ebrahim S. Is housework good for health? Levels of physical activity and factors associated with activity in elderly women. Results from the British women’s heart and health study. J Epidemiol Community Health. 2002;56:473–8. doi:10.1136/jech.56.6.473.
Salmon J, Owen N, Bauman A, Schmitz MK, Booth M. Leisure-time, occupational, and household physical activity among professional, skilled, and less-skilled workers and homemakers. Prev Med. 2000;30:191–9. doi:10.1006/pmed.1999.0619.
Stamatakis E, Ekelund U, Wareham NJ. Temporal trends in physical activity in England: the health survey for England 1991 to 2004. Prev Med. 2007;45:416–23.
Stamatakis E, Hillsdon M, Primatesta P. Domestic physical activity in relationship to multiple CVD risk factors. Am J Prev Med. 2007;32:320–7. doi:10.1016/j.amepre.2006.12.020.
Weller I, Corey P. The impact of excluding non-leisure energy expenditure on the relation between physical activity and mortality in women. Epidemiology. 1998;9:632–5. doi:10.1097/00001648-199811000-00012.
Brooks AG, Withers RT, Gore CJ, Vogler AJ, Plummer J, Cormack J. Measurement and prediction of METs during household activities in 35- to 45-year-old females. Eur J Appl Physiol. 2004;91:638–48. doi:10.1007/s00421-003-1018-9.
Corder K, Brage S, Ekelund U. Accelerometers and pedometers: methodology and clinical application. Curr Opin Clin Nutr Metab Care. 2007;10:597–603. doi:10.1097/MCO.0b013e328285d883.
Lagerros YT, Lagiou P. Assessment of physical activity and energy expenditure in epidemiological research of chronic diseases. Eur J Epidemiol. 2007;22:353–62. doi:10.1007/s10654-007-9154-x.
Centers for Disease Control and Prevention. Actigraph National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey Data. Actigraph. Available at: http://www.cdc.gov/nchs/data/nhanes/nhanes_03_04/paxraw_c.pdf.
Jacobi D, Perrin AE, Grosman N, Dore MF, Normand S, Oppert JM, et al. Physical activity-related energy expenditure with the RT3 and TriTrac accelerometers in overweight adults. Obesity (Silver Spring). 2007;15:950–6. doi:10.1038/oby.2007.605.
Ekelund U, Griffin SJ, Wareham NJ. Physical activity and metabolic risk in individuals with a family history of type 2 diabetes. Diabetes Care. 2007;30:337–42. doi:10.2337/dc06-1883.
Kettaneh A, Oppert JM, Heude B, Deschamps V, Borys JM, Lommez A, et al. Changes in physical activity explain paradoxical relationship between baseline physical activity and adiposity changes in adolescent girls: the FLVS II study. Int J Obes Lond. 2005;29:586–93. doi:10.1038/sj.ijo.0802992.
Craig CL, Marshall AL, Sjostrom M, Bauman AE, Booth ML, Ainsworth BE, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35:1381–95. doi:10.1249/01.MSS.0000078924.61453.FB.
Tehard B, Saris WH, Astrup A, Martinez JA, Taylor MA, Barbe P, et al. Comparison of two physical activity questionnaires in obese subjects: the NUGENOB study. Med Sci Sports Exerc. 2005;37:1535–41. doi:10.1249/01.mss.0000177464.68521.3b.
Vuillemin A, Oppert JM, Guillemin F, Essermeant L, Fontvieille AM, Galan P, et al. Self-administered questionnaire compared with interview to assess past-year physical activity. Med Sci Sports Exerc. 2000;32:1119–24. doi:10.1097/00005768-200006000-00013.
Kriska AM, Knowler WC, LaPorte RE, Drash AL, Wing RR, Blair SN, et al. Development of questionnaire to examine relationship of physical activity and diabetes in Pima Indians. Diabetes Care. 1990;13:401–11. doi:10.2337/diacare.13.4.401.
Schulz LO, Harper IT, Smith CJ, Kriska AM, Ravussin E. Energy intake and physical activity in Pima indians: comparison with energy expenditure measured by doubly-labeled water. Obes Res. 1994;2:541–8.
Pereira MA, FitzerGerald SJ, Gregg EW, Joswiak ML, Ryan WJ, Suminski RR, et al. A collection of physical activity questionnaires for health-related research. Med Sci Sports Exerc. 1997;29:S1–205. doi:10.1097/00005768-199705001-01074.
Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, et al. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc. 2000;32:S498–504. doi:10.1097/00005768-200009001-00009.
Freedson PS, Melanson E, Sirard J. Calibration of the computer science and applications, inc. accelerometer. Med Sci Sports Exerc. 1998;30:777–81. doi:10.1097/00005768-199805000-00021.
Balkau B, Mhamdi L, Oppert JM, Nolan J, Golay A, Porcellati F, et al. EGIR-RISC study group. Physical activity and insulin sensitivity: the RISC study. Diabetes. 2008;57:2613–8. doi:10.2337/db07-1605.
Cooper AR, Page A, Fox KR, Misson J. Physical activity patterns in normal, overweight and obese individuals using minute-by-minute accelerometry. Eur J Clin Nutr. 2000;54:887–94. doi:10.1038/sj.ejcn.1601116.
Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346:393–403. doi:10.1056/NEJMoa012512.
Salmon J, Bauman A, Crawford D, Timperio A, Owen N. The association between television viewing and overweight among Australian adults participating in varying levels of leisure-time physical activity. Int J Obes Relat Metab Disord. 2000;24:600–6. doi:10.1038/sj.ijo.0801203.
Shephard RJ. Limits to the measurement of habitual physical activity by questionnaires. Br J Sports Med. 2003;37:197–206. doi:10.1136/bjsm.37.3.197.
Bassett DR Jr. Validity and reliability issues in objective monitoring of physical activity. Res Q Exerc Sport. 2000;71:S30–6.
Ward DS, Evenson KR, Vaughn A, Rodgers AB, Troiano RP. Accelerometer use in physical activity: best practices and research recommendations. Med Sci Sports Exerc. 2005;37:S582–8. doi:10.1249/01.mss.0000185292.71933.91.
Neilson HK, Robson PJ, Friedenreich CM, Csizmadi I. Estimating activity energy expenditure: how valid are physical activity questionnaires? Am J Clin Nutr. 2008;87:279–91.
Matthews CM. Calibration of accelerometer output for adults. Med Sci Sports Exerc. 2005;37:S512–22. doi:10.1249/01.mss.0000185659.11982.3d.
Acknowledgments
The authors gratefully thank Leila Mhamdi, PhD, for her assistance in data analysis. We thank Cedus, Go Sport, Fournier Pharma, Roche, Lesieur, and Nestlé France for their support to the Fleurbaix-Laventie Ville-Santé study. This project was supported by a research-action grant from the French Ministry of Health—National Nutrition and Health Program (PNNS-2002).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jacobi, D., Charles, MA., Tafflet, M. et al. Relationships of self-reported physical activity domains with accelerometry recordings in French adults. Eur J Epidemiol 24, 171–179 (2009). https://doi.org/10.1007/s10654-009-9329-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10654-009-9329-8