
Abstract
This paper reviews the available research on the predictors of parental engagement in preventive and therapeutic psychological interventions that target mental health problems in children. Based on previous literature, seven predictors concerning parental motivation to engage are considered: perceived child problems, perceived parenting, attributions of problems, self-efficacy, expectations about treatment, perceived obstacles and global motivation to engage. PRISMA guidelines for systematic review were used to conduct the literature search. Thirty-seven studies that examined prospective relations between parental cognitions evaluated at the beginning of the intervention and parental engagement during the intervention were included. Most studies focused on the parents’ perception of the child’s problems and of parenting, with fewer studies examining the role of the other parental cognitions. The results suggest that the psychological dimensions proposed in motivational models may play an important role in understanding parental engagement in preventive and therapeutic psychological interventions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The impact of preventive and treatment programs that address children’s mental health problems depends on some level of parental engagement. Whether they aim to modify child behavior and emotional problems by intervening directly with the child (child-centered interventions) or indirectly through parenting behaviors and practices (parent-centered interventions), in these programs parents can assume different levels of involvement and different roles.
Some interventions focus on the central role of parents on the child’s psychological (mal)adaptation through different mechanisms, such as socio-learning processes, attachment, and emotional processes [1, 2]. In these interventions, parents are encouraged to modify their own behavior [3] to reduce parental risk factors (e.g., coercive behavior) and increase protective factors (e.g., sensitive and responsive behavior).
Several evidence-based parenting interventions are now available [4, 5], showing positive results in the promotion of positive parenting and in preventing the development of children’s mental health problems. However, epidemiological surveys show that few parents participate in any form of parent education (approx. 25%) [6], and among those involved in preventive parenting programs, a high attrition rate is observed (up to 60%) [7].
Parents can also perform other roles in the treatment of children with psychological disorders. These roles include not only the modification of their own behavior but also being consultants (providing information about the child), collaborators or co-therapists (helping the child in learning, training or generalizing specific skills) or co-clients (managing their own mental health problems that would impact children’s adjustment) [8].
Children also depend on the motivation of parents to seek professional help and to bring them to therapy. Although there are several evidence-based treatments for children’s mental health problems [9], there are many children and parents who might need but do not seek professional help. For example, an Australian national mental health survey indicated that only 25% of children aged between 4 and 17 years old with a diagnosable mental disorder had used any health services in the previous 6 months [10]. On the other hand, approximately half of the families who initiate psychological interventions drop out prematurely [11]. A recent review [12] shows that 51% of individuals who would benefit from parent training do not complete treatment.
Problems with missing consultations, premature termination and low engagement have a significant impact, limiting the reach of children’s mental health interventions and its efficacy, and compromising the effectiveness of mental health services [13]. Therefore, the study of parental engagement in psychological interventions and its predictors should be a priority [13].
Parental engagement in psychological interventions has been defined in the literature as a broad construct that includes several components [14, 15]. Behavioral parental engagement refers to parents’ actions that are required to carry out the intervention and to achieve desired outcomes [15]. These actions involve parental attendance and completion of the program and also parents’ participation engagement during the intervention process. Parents’ participation engagement consists in “parents’ active, independent, and responsive contributions to treatment” [p. 134, 16], such as sharing one’s point of view, asking questions, and participating in therapeutic activities, both within and between the sessions (e.g., serving as a co-therapist to reinforce the child’s use of the strategies learned during the sessions, or following the therapist’s or facilitator’s orientations when interacting with the child).
Despite the evidence supporting the importance of the parents’ participation in the outcomes of interventions targeting children’s mental health problems [8, 17, 18], most studies usually limit their definition of behavioral engagement to attendance/dropout [19]. For example, in a review examining engagement data across 262 studies of behavioral parent training, only 10% of the studies provided data on within-sessions engagement and even fewer reported on between-sessions engagement [12].
Sociodemographic factors related to parents’ engagement have been widely studied. A meta-analysis of studies conducted by Reyno and McGrath [20] showed that treatment dropout was associated with low socioeconomic status, single-parent status, and minority-group status, all with small effect sizes. These results suggest that the research on determinants of parental engagement must go beyond demographic characteristics. In addition, sociodemographic determinants cannot be easily changed and therefore have little utility for interventions addressing the promotion of parental engagement [21].
The seminal works of Spoth [22, 23] and Kazdin [24,25,26] have contributed greatly to a more theoretical approach to the study of parental engagement. Spoth and Redmond [22], informed by the Health Belief Models [27], proposed four main determinants of parents’ inclination to enroll in parenting programs: perceived child susceptibility to future problems, perceived severity of those problems, program benefits and program barriers. In the same line, the Barriers-to-Treatment Model [26] was developed to guide the research on premature treatment termination in child therapy. This model points to the influence of stress and obstacles that compete with treatment, including practical barriers to participation, perception of the treatment as demanding and as having little relevance to the child’s problem, and poor relationship or alliance with the therapist.
Taken together, these theoretical frameworks emphasize the importance of parental cognitions related to parents’ motivation to engage in parenting preventive or therapeutic interventions or to change their parenting behavior. Motivation to engage/change requires a number of factors: the desire to engage/change, i.e., the perception that engagement/change is important to accomplish parenting objectives; the perceived ability to engage/change, i.e., the sense of competence or efficacy to implement the necessary changes and the expectation that the therapy or the action will be effective in effecting those changes; and readiness to engage/change, i.e., change should be a priority to the parent at that moment [28].
The aim of the current study is to conduct a systematic review to analyze the role of parents’ motivation to engage in psychological interventions directed to preventing and/or reducing behavioral or emotional problems in children (child-centered, with a component of parent involvement; and/or parent-centered). In the current review, we will focus on parents’ behavioral engagement, including parents’ attendance and completion of the program and parents’ participation engagement within and between sessions. We will examine the role of the following parental cognitions: (a) perception of the child’s problem (including its severity and impact on the child’s development), (b) perception of their own parenting behavior, (c) attributions regarding the problem (e.g. internal/external locus), (d) self-efficacy, (e) expectations about treatment and perception of the intervention benefits, and (f) perceived obstacles/barriers to participation. We will also examine the role of more global motivational dimensions, including parents’ desire, willingness, and readiness to change.
The current study explores what research has been done and what is known about the influence of parental cognitions on parents’ engagement in interventions targeting children’s mental health problems. The specific questions to be addressed by the review are as follows: (1) How are parental cognitions and parental engagement measured in the studies? (2) Considering the different parental cognitions, what are the predictors of the two main aspects of behavioral engagement, i.e., attendance/dropout and participation engagement?
Methods of Systematic Review
Eligibility Criteria
Inclusion criteria required for each study are as follows: (1) include measures of parents’ motivation to change and/or related dimensions (parents’ perception of children’s and parenting problems; parents’ self-efficacy; parents’ attributions; parents’ expectations about intervention; parents’ perception of benefits and obstacles) as predictors; (2) report outcomes related to some form of engagement in psychological interventions (engagement, involvement, participation, adherence, dropout); (3) include psychological interventions with a parenting component; (4) include a sample of parents of children 12 years old or younger; (5) present a prospective design and inferential statistics; (6) have been published in English in a peer reviewed journal; and (7) have been published after 1990. This last criterion was set because this was the decade when the seminal studies of parental engagement conducted by Spoth [22] and Kazdin [24,25,26] were published.
We excluded parenting interventions that were directed to specific health problems (e.g., preventing obesity, adaptation to chronic conditions) or educational problems (e.g., promoting readiness for school). When the articles included data retrieved from the same sample, and the outcomes of the studies overlapped substantially, we only retained one of the articles. The limitation to samples of parents of children up to 12 years old was based on the recognition that most parenting interventions to prevent or treat mental health problems are directed at this age range [29] and that most parenting programs to promote mental health of adolescents are directed at specific domains of behavior (prevention of substance abuse, early/risky sexual activity) [30].
Information Sources
A literature search was conducted for studies published in English from January 1990 through to 30 October 2017. Databases used were PsycINFO, Academic Search Complete, Education Source, Psychology and Behavioral Sciences Collection, ERIC, PsycARTICLES. The reference list of the studies included in the current systematic review and other reviews related to the subject were analyzed with the purpose of identifying any further potentially relevant papers.
Search Strategy and Study Selection
The following search terms and Boolean operators were used: (“child* problem” OR “child* behavior” OR “child* psychopathology” OR “parenting problems” OR “parenting practices” OR “parenting behavior” OR “parent* problem recognition” OR “parent* problem identification” OR “parent* perceived need” OR “parent* needs” OR “parent* attributions” OR “parent* control” OR “parent* beliefs” OR “parent* self-efficacy” OR “parent* efficacy” OR “parent* competence” OR “parent* confidence” OR “parent* expecta*” OR “parent* treatment beliefs” OR “perceived benefits” “parent* motivation” OR “parent* readiness” OR “parent* preparedness” OR “parent* receptiveness” OR “parent* willingness” OR “perceived obstacles”) AND (retention OR adherence OR attendance OR compliance OR engagement OR involvement OR participation OR drop-out OR dropout OR “drop out” OR completion OR attrition OR “premature termination”) AND (“mental health” OR “preventative intervention” OR “preventative program” OR “parent* intervention” OR “family intervention” OR “parent* program” OR “family program” OR “parent* training” OR “parent* management” OR “psychological intervention” OR “family therapy” OR “child* therapy” OR “psychotherapy”). Only Scholarly (Peer Reviewed) Journals were considered.
Methodological Quality of the Studies
To assess the methodological quality of the studies, we followed an adaptation of selected guidelines from the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. The following criteria were used: (a) description of relevant sample characteristics (child’s sex; child’s age mean and range; who is the participating parent, i.e. father/mother; socio economic status or parents’ education levels; parents’ ethnicity; if clinical sample: child’s diagnostic status): 1—all or all but one characteristics described; 0—more than one of the characteristics not described; (b) recruitment procedures adequately described: 1—description of the recruitment procedures (how the sample was recruited, percentage of individuals enrolled in the study, inclusion/exclusion criteria), 0—description absent for more than one element; (c) reliable measures of predictors: 1—reliability score for each measure reported and adequate, 0—reliability score not reported or not adequate for at least one of the measures; (d) reliable measures of parents’ engagement: 1—At least internal consistency for parents’ engagement measure reported and adequate or detailed description if objective measure (e.g., number of sessions attended), 0—reliability score not reported or not adequate; (e) power calculation reported and study adequately powered to detect hypothesized relations: 1—power calculation reported, 0—power calculation not reported; and (f) relevant confounders adjusted for in analyses: 1—family adversity (SES, single mother, parental psychopathology) adjusted for in analysis, 0—relevant confounders not adjusted for in analysis.
Results
Results of the Search
The Preferred Reporting Items for Systematic Reviews (PRISMA) flow diagram is presented in Fig. 1. The search produced 3280 papers. Studies were de-duplicated and screened by title and abstract, resulting in the exclusion of 2521 articles that did not meet the inclusion criteria.

PRISMA flow diagram of the article search and selection process
From the 68 full texts examined, 35 studies were eliminated because they: did not included predictors or outcomes of interest (15 studies); included other kinds of interventions in an undifferentiated way (e.g., mental health services, etc.) (nine studies); included adolescents samples (four studies); were retrieved from the same database (three studies); included small samples preventing the use of inferential statistics (two studies); and used qualitative or cross-sectional methodologies (two studies). The resulting database of 33 papers was supplemented by four studies selected by manual review of the references from included studies.
In total, 37 eligible articles were identified (Table 1). Most studies were from the USA (26) and a minority from Europe (six), Asia (two), Australia (two), and Canada (one). Table 1 describes the main characteristics of the studies included in the review.
The majority of the studies were conducted using clinical samples, with externalizing problems as the main reason for referral (only two samples included children with internalizing problems). From the community studies, five were conducted using high-risk samples (e.g., children screened in the community for externalizing problems). In most community studies participants received a financial compensation for their participation. Most of the studies included families with pre-school and school-aged children. Sample dimension was highly variable, and the large majority of participants were mothers. In addition, most studies included manualized (35 studies; e.g., Parent–Child Interaction Therapy, Triple P; Incredible Years Parenting Training Program; Coping Power) and face-to-face interventions, with a highly variable duration (3–28 sessions). Most of the studies addressed the modification of parents’ behavior and only two studies, with parents of children with internalizing problems, involved parents as “co-therapists.”
Methodological Quality of the Studies
The methodological quality of each study is displayed in the supplementary material file. In general, the studies presented good methodological quality. Only five studies met less than 50% of the criteria. The least fulfilled criteria were power analysis and sample size estimation (only one study presented sample size estimation). In more than one-third of the studies, no internal consistency data was presented for the scales measuring the predictors in the study sample, and the effects of the predictors of engagement were not controlled for important socio-demographic characteristics.
Predictors and Outcomes of Parental Engagement Examined
Table 2 includes information about the descriptives of the predictors and outcomes examined in the studies included in the review. A more detailed description of the studies and results is included in the supplementary material file.
Perceived child behavioral problems was the predictor of parental engagement most often studied, followed by parents’ perception of parenting. Fewer studies analyzed the role of inadequate attributions, parental self-efficacy, perceived intervention benefits or expectations about treatment, parental motivation and readiness to change/for treatment and parental perceived obstacles. A large majority of the studies examined only one or two predictors concerning parental cognitions, except for Bloomquist et al. [31], who examined several predictors simultaneously (i.e. perceived child problems, perceived parenting, anticipated barriers, motivation to engage in the intervention).
Most studies evaluated objective indicators of engagement (i.e., dropout or program completion and attendance) and only a minority evaluated parents’ participation engagement. In the case of program completion or dropout, a categorical measure was used to determine who completed the program or who dropped out. However, the criteria for dropout or completion was highly variable (e.g., in some cases completion required the completion of the entire program protocol, in other cases half of the sessions, and in other cases even less). Attendance was usually measured by the number or percentage of sessions attended. Lastly, parents’ participation engagement was measured using brief scales (1–13 items), usually filled by therapists or group facilitators and in one study by parents. These scales included items regarding homework completion, quality and quantity of participation within and between sessions, and quantity or/and quality of parent adherence to treatment procedures.
Study Results by Domain
Table 3 presents study results by predictors and outcomes. Although sometimes the studies included more predictors, we only report the variables and results related to the objective of this review.
Parents’ Perception of the Child’s Problems
The intensity, frequency and severity of internalizing and/or externalizing problems were measured by scales administered to parents (e.g., Eyberg Child Behavior Inventory) in most studies. One study also resorted to a parent daily report to evaluate externalizing problems (Oppositional and Aggressive Behavior Scale of the Parent Daily Report) and another study used an interview (Risk Factor Interview). Results concerning observational measures or other’s report of child problems (e.g. teacher) were not included in the analysis because they do not represent parent’s perception of child’s problems.
Twenty studies (72.4%) reported non-significant associations between parents’ perception of the child’s externalizing and/or internalizing problems and parents’ attendance (five studies [32,33,34,35,36]), completion/dropout (fifteen studies [35, 37,38,39,40,41,42,43,44,45,46,47,48,49,50,51]) and parents’ participation engagement (five studies [18, 32,33,34, 42]), and these results were observed for parenting interventions in clinical or community samples.
On the other hand, eight studies (27.6%) found significant associations between parents’ perception of the child’s problems and parents’ attendance (four studies [17, 31, 52, 53]), completion/dropout (three studies [54,55,56]) or parents’ participation engagement (one study [57]) in studies with clinical and community samples. All these significant associations occurred for externalizing problems, with the exception of the study by Wells et al. [53], who also found positive significant associations between child internalizing problems evaluated by fathers and attendance.
The parents’ attendance in four community samples was predicted by a higher perception of externalizing problems [17, 31, 52, 53]. By contrast, in three studies, parents’ dropout from a parenting intervention, involving clinical samples and one court-ordered sample, was predicted by more perceived externalizing problems [54,55,56]. Lastly, in one study, the parents’ perception of more externalizing problems was significantly associated with a higher parental participation engagement in the therapy [57].
Parents’ Perception of Parenting
In ten studies, the parents’ perception of their own parenting was evaluated by self-report scales. These scales measured discipline styles or positive/negative parenting practices (e.g., Parenting Scale). In one study, parents’ perceptions of parenting were collected through the Risk Factor Interview to evaluate adverse child-rearing practices. Results concerning observational measures were not included because they do not represent parent’s perception of parenting problems.
The results suggest that parents’ perception of parenting predicted parents’ engagement in seven studies (63.6%) [31, 52,53,54,55, 58, 59] and had no effect on parental engagement in four studies (36.4%) [38, 42, 51, 60]. More negative and adverse parenting was associated with parents’ non-completion of the treatment in one study conducted using a clinical sample [54] and in one study where parents were court-ordered to participate in the treatment [55]. On the other hand, in community studies, parents’ attendance was predicted by higher levels of consistent or positive discipline [31, 52, 59]; more over-reactive behavior [53] and higher parental participation engagement was predicted by higher levels of negative parenting and by higher levels of supportive/positive parenting [58]. Nevertheless, the parents’ perception of their own parenting did not predict completion of the program [38, 42, 51, 60] or adherence to the techniques learned during the program [42] in studies using community samples.
Parents’ Attributions
Parents’ attributions were evaluated through interviews (Leeds Attributional Coding System) and by a self-report scale (Children’s Attribution Style Questionnaire-Parent Version). All the three studies that explored parents’ attributions as a predictor of engagement reported significant effects of some dimensions of parents’ attributions. In one study [35], mothers’ child-centered attributions were not significantly associated with the outcomes, suggesting that attributing the responsibility of the problem to the child is not a barrier to attending therapy. However, in this same study, mothers who attributed more responsibility to themselves attended more sessions and were more likely to complete therapy (e.g., ‘he behaves like this because I’m not strict enough’). In another study [61], mothers who never attended therapy were more likely to have higher inadequate child-centered attributions (a composite resulting from the difference between the score of adequate attributions for positive events, i.e., more external, situational, specific, and the score for inadequate attributions for negative events, i.e., more internal, stable, global), compared to parents who dropped out of therapy and those who completed therapy.
Lastly, the results of a study by Miller and Prinz [47] showed that parents’ engagement in the therapy was predicted by the match between parents’ incoming motivation, evaluated through an interview, and the assignment to a treatment condition (parent-only treatment or child-only treatment). The assignment to a treatment condition that did not match the parents’ attributions regarding the child’s externalizing problems (internal to the parent or external to the parent) predicted dropout from therapy. However, the effect of a mismatched treatment condition was only significant when families entered treatment with external motivations (parents focused on changing the child) and were offered a parent-only treatment approach. The same effect was not significant for mismatched families with internal motivations (parents focused on changing their behavior that were offered a child-only treatment).
Parents’ Self-Efficacy
Parents’ self-efficacy was evaluated by brief self-report scales (e.g., Parenting Sense of Competence Scale). In one study, the Parenting Sense of Competence Scale was adapted to be administered by interview.
Four studies, one conducted with a community sample and three with a clinical sample, showed no significant associations between parents’ self-efficacy and engagement (66.7%) [34, 46, 50, 62]. On the other hand, two studies (33.3%) found a significant association between parents’ self-efficacy and engagement [17, 61]. In a study with a clinical sample [61], single mothers who never attended therapy were more likely to have lower parental efficacy, and in another study, with a community sample of parents of preschoolers [17], higher attendance was associated with lower parenting self-efficacy.
Parents’ Expectations About Intervention or Intervention-Perceived Benefits
In four studies, parents’ expectations about treatment were evaluated by self-report scales. The content of these self-report scales was heterogeneous, including: parents’ beliefs about the credibility of treatment; parents’ expectations of improvement with treatment; beliefs about the child’s current need for medication and therapy; beliefs about the use and prescription of medication in general; beliefs about whether treatment is worthwhile; parents’ perception of their understanding of treatment/possible side effects; and feelings of trust in providers and the feeling of inclusion in treatment planning.
The studies show mixed results concerning the role of parents’ expectations about the intervention: two found a significant association between parents’ expectations and parents’ engagement (50%) [63, 64], while two found no significant association (50%) [18, 41].
The two studies that did not find any association share some methodological constraints. Using a small clinical sample (n = 29) of families with a child with a primary mood disorder, Davidson et al.’s [41] study found no significant association between positive attitudes about treatment and parents’ participation engagement for the main caretaker (although this association was found for a secondary caretaker). In this study, there was also no significant relationship between positive beliefs about treatment and attendance. In a study that included a community sample (n = 50) of children with high levels of internalizing problems and their parents [18], positive expectations about treatment did not predict parental participation engagement. This study also resorted to a small sample and to a one-item measure of parents’ expectations, and this may result in a less sensitive evaluation of expectations.
On the other hand, Nock et al.’s [63] study using a clinical sample of families with a child with behavioral problems showed significant effects for parents’ expectations, but in opposite ways for different outcomes (attendance, quantity of adherence to treatment procedures, and quality of adherence to treatment procedures). More positive expectations were associated simultaneously with higher adherence to treatment procedures (but not with the quality of the parents’ adherence) and with lower attendance.
In another study [64], using a clinical sample of families with a child presenting behavioral problems, the results support a curvilinear relationship between parents’ expectations about therapy, treatment attendance and premature termination in an intervention that involved parent management training and children’s cognitive problem-solving. More attendance and fewer dropouts were associated with very high or very low parental expectations.
Parents’ Perceived Obstacles
The two studies [31, 32] that examined the role of perceived obstacles to participation at pre-intervention resorted to self-report measures to evaluate this predictor (e.g., Obstacles to engagement Scales). Bloomquist et al. [31] found no significant association between parents’ attendance and parents’ anticipated barriers, but Dumas et al. [32] observed that parents who reported fewer time and scheduling demands attended more sessions than parents who reported more demands on their time. In this study, participation engagement was not predicted by perceived obstacles.
Parents’ Motivation to Change
Four studies conducted with clinical samples explored the effect of parents’ motivation to change or to engage in treatment [31, 57, 63, 65]. These studies resorted to three self-report scales that measured desire for the child to change, readiness to change and perceived ability to change (e.g., parent motivation inventory), or that evaluated parents’ pre-contemplation, contemplation, and action dimensions (Parent Readiness for Change Scale). Three of these studies [31, 57, 63, 65] found significant effects of parents’ motivation to change. In Wade and Andrade’s [65] and Bloomquist et al.’s [31] studies, parents reporting higher levels of readiness and motivation attended mores sessions. Stadnick et al.’s [57] study observed that motivation to participate in therapy, more specifically perceived ability, was positively and significantly associated with the observed parental engagement during sessions. Only one study [63], conducted using a sample of low-income parents, found no association between parents’ motivation and quality and quantity of treatment adherence and attendance.
Discussion
This study examined the predictors of parental engagement in psychological interventions. Low parental engagement is a major problem because it limits the positive impact of interventions addressing children’s mental health problems, especially in populations most in need (e.g., families and children exposed to more psychosocial risks). Identifying the psychological predictors of parental engagement is crucial to improving the reach and effectiveness of psychological interventions with parents and children.
We identified 37 papers reporting prospective studies that examined parental psychological predictors (evaluated at the beginning of the intervention) of parental engagement during a psychological intervention. The samples studied were very diverse in terms of the level of risk/disorders, recruitment and socio-economic composition. 19 studies included clinical samples, 17 included community samples and only one study used a court-ordered sample. Most clinical samples consisted of children with externalizing problems as the main reason for referral. This is consistent with the fact that parents play a more central role in both the conceptualization and the treatment of children’s externalizing disorders compared to children’s internalizing problems [3].
The majority of the studies examined parental dropout, completions and parental attendance, and fewer studies analyzed parents’ participation engagement in the intervention. This is in line with previous literature on parental engagement that usually equates engagement with attendance or dropout, excluding a more qualitative dimension of parents’ participation [19], although some studies suggest this type of involvement is a better predictor of positive outcomes for interventions [17].
Departing from previous empirical literature [66] and theoretical models of psychological determinants of parental engagement [15, 23,24,25], we examined, as predictors of parental engagement in psychological interventions, parental motivation to change or to engage in the intervention and six related cognitions: perceived child problems, perceived parenting, parents’ attributions, parents’ self-efficacy, parents’ expectation about the treatment, and parents’ perceived obstacles.
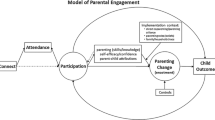
These six parental cognitions can be organized in two dimensions that are central to motivation to change: need or desire to change and the perception that change is possible (Fig. 2). According to motivational models, parents are more likely to attend and participate in therapy if they perceive that there is a need for change, recognizing the existence of a problem with their child or with their own parenting behavior (Need or Desire to Change). Additionally, parents will be more likely to engage in therapy if they endorse adaptive attributions concerning their child’s and their own behavior, believe that they can conduct the needed changes (self-efficacy), expect the intervention to be effective in changing the problematic behavior and perceive that the benefits of participation will outweigh the costs (Possibility of Change).

Parental motivation to engage in therapy or parenting programs
In the current review, parents’ perception of the child and the parents’ problems were the predictors of parental engagement more extensively researched. Far fewer studies examined the role of perceived intervention benefits and obstacles, parental self-efficacy, attributions, parental motivation and readiness to change/for treatments. Therefore, the evidence concerning some important potential cognitive predictors of parental engagement is very limited and a more global test of the role of the different dimensions on parental engagement is even scarcer.
Regarding the first component of the motivational model, parents’ perceived need to change, the effects of perceived child problems and perceived parenting as predictors were examined. The relationship between parents’ perception of the frequency/intensity of the child’s problems at the beginning of the intervention and different outcomes of parental engagement during the intervention was non-significant in most studies. It is important to take into account that the child’s problems are an indirect measure of the perceived need to change, and for that reason its relation with engagement may not be straightforward. For example, if parents report a high level of externalizing problems, this does not necessarily imply that they recognize it as a problem, or that they see themselves as part of the problem or as part of the solution to that problem. On the other hand, the relations between parents’ perception of their own parenting and parents’ engagement showed more significant effects, especially when the studies included clinical samples.
The significant associations between the perception of child and parenting problems and parental engagement revealed a different picture for community and clinical samples. In community samples, a higher perception of the child’s externalizing problems and higher levels of both positive and negative parenting predicted more engagement [17, 31, 52, 53]. On the other hand, different results were observed in clinical and court ordered studies, showing that parents’ perception of externalizing problems in their children and their perception of more negative and adverse parenting was predictive of parents’ non-completion [54,55,56]. We may hypothesize that extreme levels of a child’s externalizing problems and more negative parenting practices may place too much of a burden on families in clinical samples, leading them to feeling hopeless and resulting in therapy dropout. Parents most in need may have more difficulties in maintaining motivation to remain in the intervention due to various factors (e.g., parents who are more stressed by the child’s behavior and feeling more hopeless and parents with more difficulties to self-regulate). Interestingly, the only study with a clinical sample that evaluated the association between perceived child externalizing problems and parents’ participation engagement found a positive significant association [57]. This result may indicate that, when parents have children with higher levels of child problems and are retained in the therapy, they show a higher commitment and participation in the therapy sessions than parents who perceive lower levels of externalizing problems.
In conclusion, the relation between parents’ engagement and parents’ perceived need to change (because of perceived child or parenting problems) may not be linear. The predisposition to engage in the interventions may be hampered when parents from community samples recognize only a few problems in the child or in their own parenting behavior, thus not justifying an effort to be engaged in a parenting program. On the other hand, engagement can also be hindered when parents from clinical samples perceive too many problems in the child and in their parenting behavior, which can lead them to feel hopeless and unable to implement the needed changes.
These apparently disparate results emphasize the importance of the second component of the motivational model: parents’ perceived possibility of change. Several parental cognitions related to this component were examined: parents’ attributions and self-efficacy consistent with the belief that the child’s and the parents’ behavior change is possible; parents’ beliefs and expectation that the intervention will be effective in changing the problematic behavior; and parents’ perception of obstacles to their engagement. As previously pointed out, parental cognitions related to this component have been far less examined by the empirical literature.
The three studies with clinical samples that investigated the role of parents’ attributions of the child’s problems found significant effects [35, 47, 61]. Engagement in therapy was more likely when mothers attributed more responsibility to themselves. On the other hand, mothers who never attended therapy were more likely to have higher inadequate child-centered attributions. These results show that parents are more likely to engage in the therapy when they show some internal locus of control instead of merely attributing control to the child (e.g., “I have some responsibility for my child’s behavior, it is not just because of her/his temperament”) and when they believe that the child’s and their own behavior is, to some extent, changeable.
In addition, the study by Miller and Prinz [47] indicates the importance of considering conjointly the parents’ attributions and the type of therapy offered to the parents. The mismatch between parents’ attributions regarding the child’s aggressive problems (internal to the parent or external to the parent) and the type of therapy parents received (child-centered or parent-centered) predicted parents’ dropout, but only for families entering treatment with external motivations (parents focused on changing the child) and that were offered a parent-only treatment approach. This study suggests that parents’ incoming expectations about who should receive therapy might be a factor to address when planning that therapy.
In relation to parents’ self-efficacy, only two [17, 61] of the six studies found significant effects in parents’ engagement. Concerning the absence of effects in four of the six studies, it is important to note that perceived self-efficacy or competence in parenting is only a proxy of the perceived capacity of parents to make the appropriate changes, which would be more directly related to the proposed role of self-efficacy in motivational models of change [67]. The two studies that found significant effects indicate different effects for clinical and community samples: in a clinical sample, lower parental efficacy was more common in single mothers who never attended therapy [61] but was associated with higher attendance in a community sample [17]. This suggests that parents’ low-efficacy can compromise their involvement in therapy in samples with high levels of externalizing problems, and this may be especially true in more disadvantaged samples, once this study was conducted with a sample of single mothers. However, low parental self-efficacy can mobilize parents of children with normative levels of behavioral problems to engage in a universal parenting intervention. It might be easier to accept one’s role in problem maintenance and the need to be involved in intervention when the child’s problems are perceived as moderate and part of normal development.
The results of the four studies that examined the role of parents’ expectations about treatment are mixed. One shows a positive relation between positive expectations about treatment and parents’ participation engagement [63], two suggest a significant relation between parents’ expectations and attendance [63, 64], and two studies found no relation at all [18, 41]. Some methodological limitations of these last two studies may explain the absence of results, since one of them used only one item to measure expectations and both of them resorted to small sample sizes that may have lacked the power to detected significant results.
Concerning the relation between parents’ expectations and attendance, the results of Nock et al. [63] were somewhat surprising. In this study, more positive expectations were associated with less parental attendance. The authors hypothesized that positive expectations about treatment were related to shorter treatment attendance because parents with more positive expectations demonstrated a greater improvement and required a smaller dose of treatment to obtain the therapeutic objectives. These findings are consistent with Nock and Kazdin’s [64] study, which found that parents with the lowest expectations were also those with the greatest attendance; although this study found a curvilinear relation between expectations and attendance, indicating that parents who attended more sessions and who were least likely to drop out from treatment presented either very high or very low expectations concerning therapy. On the other hand, those parents with moderate expectations attended the fewest sessions and were most likely to drop out from treatment. The fact that Nock et al.’s [63] study did not find the same curvilinear relation may be due to the shorter duration of the treatment, which possibly contributed to diminishing the variability within the sample.
Although several theoretical models emphasize the role of perceived obstacles to the participation in the treatment, one of the only two studies that examined this predictor found no significant effects [31]. One possible explanation for the absence of effects in this study was that the intervention provided support to families, such as delivering the interventions in the family home or in a community center at night, thus significantly decreasing practical obstacles.
Lastly, four studies examined the relationship between parents’ global motivation to change and parents’ engagement in treatment. Consistent with motivational models of parents’ engagement, the results of three studies suggest that highly motivated parents were more likely to engage in the psychological intervention [31, 57, 65]. The only study that did not find a significant association between parents’ motivation to change and engagement in the treatment [63] was conducted with a low-income clinical sample. Parents from low SES are more likely to experience several stressors, such as financial, social, and psychological problems, and therefore the engagement of these families in a treatment that places an additional burden on families (in terms of time, transportation to the clinic, etc.) may not depend exclusively on parents’ motivation to engage.
Clinical Practice Implications
Interventions directed at the prevention of children’s mental health problems can positively impact the child and family life when families attend and actively participate in the interventions, especially those families most in need.
The results suggest that parental engagement in community preventive parenting programs is facilitated by parents’ perception of the child’s and parenting problems, low self-efficacy in managing educational situations, and increased parental motivation. Therefore, parents’ engagement in community interventions might be promoted by targeting these cognitions early in the intervention, so that parents can identify individual objectives for changes in parenting behavior in order to overcome the child’s problems. Additionally, it is important to target the reduction of practical barriers by offering the program at convenient hours and in accessible locations, and by providing childcare facilities during program hours.
On the other hand, parents from clinical samples who perceive more child externalizing problems, more negative parenting practices, lower self-efficacy, and who endorse more inadequate attributions of problems, have a higher risk of dropout. These families may be overwhelmed by the child’s externalizing problems. Therefore, in these situations, it may be useful for clinicians to let parents know they understand their difficulties, to reinforce their alliance with parents so that they can feel supported and to offer supplementary opportunities of contact (e.g., brief telephone calls or more frequent sessions). Simultaneously, to the support offered to these parents, it is important to promote more adequate attributions regarding the child’s behavior, so that parents can see themselves as part of the solution, hold more realistic expectations concerning the treatment, and perceive themselves as more capable of implementing needed changes.
Limitations of This Review and Future Research Directions
This review has some limitations. First, we only included studies published in peer-reviewed journals. This option offers, to some extent, a guarantee of the quality of the studies, but on the other hand can increase the bias of reporting studies that found significant effects. Second, the specific search terms included in this review to address our study objectives do not cover all possible equivalent search terms, and therefore this may have affected the articles selection. The strategy to look for additional articles not included in the initial selection was aimed to diminish the bias introduced by the specific search terms used, but still some articles may have been left out. Third, our operationalization of parents’ engagement did not include the earlier phases of enrollment. The study of the predictors of parents’ enrollment in preventive and treatment interventions is crucial to increasing the reach of these interventions and to guaranteeing that they target the parents most in need.
Research examining parental cognitive predictors of parents’ engagement in psychological interventions remains limited and shares some limitations that are important to address in future research. In most studies reviewed, engagement is equated with attendance and dropout or retention. Parents’ participation engagement is rarely reported. Although the different dimensions of engagement are related, they represent different aspects of parental engagement that can be influenced by various factors and differently contribute to the efficacy and effectiveness of interventions. Piotrowska et al.’s [68] model of parental engagement in parenting programs that proposes several interdependent stages of engagement (connecting, attending, participating and enacting) may be a useful framework to guide the operationalization of parents’ engagement in future studies.
In addition, in most studies, mothers formed the large majority of participants. Fathers are underrepresented in parenting intervention studies and those included in this review are no exception. Fathers’ low rate of participation in psychological interventions is critical. This is especially true if we consider that co-parenting is a determinant of treatment success [68]. A meta-analysis conducted by Lundahl et al. [69] that examined fathers’ involvement in parenting training showed that when fathers were included, more positive changes in children’s behaviors were observed immediately after the training. Future studies should pay attention to both the mother’s and father’s engagement in interventions.
Some methodological limitations of the studies reviewed should be mentioned. Only one study presented sample size estimations and some may have lacked the power to detect significant associations. On the other hand, although most studies resorted to valid and reliable measures, some studies did not present internal consistency indicators for some measures. Lastly, the effects of the predictors on engagement were not controlled for important socio-demographic characteristics in some of the studies.
In the studies reviewed, parental cognitions and motivation were only measured at the beginning of the therapy. Parents’ motivation to be involved in a psychological intervention is a dynamic process and can change during that process. Likewise, the potential predictors of parents’ engagement, such as parents’ attributions and parents’ self-efficacy, are targets for change in many parenting interventions and so may evolve during the process. Therefore, it would be interesting to examine how the change of these specific predictors during the treatment can relate to engagement at various points during the intervention.
Lastly, research on cognitions that determine parents’ motivation to engage in psychological interventions remains scarce. We have limited knowledge of the role of some dimensions of parents’ cognition and motivation (specifically, parents’ attributions of problems, parents’ perceived benefits and obstacles and more global parents’ motivation). Given the importance of this research, more studies are needed to identify the predictors of parents’ engagement. These will enable the identification of families at risk for dropout and low participation and encourage the work of modifying risk factors, such as inadequate attributions or lack of acknowledgment of a child’s and parenting problems, early in the intervention.
Summary
Parents’ low adherence and high dropout in interventions that address children’s mental health problems is a major problem, with impacts on health care costs. Identifying modifiable psychological determinants of parental engagement is essential to improving the reach and effect of parenting interventions. This work reviews the available research on the predictors of parental engagement (attendance, dropout and parental participation engagement) in psychological interventions to prevent and treat mental health problems in children (age < 12 years). Based on theoretical models of parental engagement, several predictors were identified: perceived child problems and perceived parenting (perceived need for the intervention), attributions of problems, self-efficacy, expectations about treatment, perceived obstacles (perceived possibility of change), and global motivation to change.
PRISMA guidelines for systematic review oriented the search in PsycINFO, Academic Search Complete, Education Source, Psychology and Behavioral Sciences Collection, ERIC and the PsycARTICLES databases. 37 studies that evaluated parental cognitions at the beginning of the intervention and examined them as predictors of parental engagement during a psychological intervention were included in the review.
The results show that parents’ perception of children’s problems and of their own parenting are the most studied cognitive predictors of parents’ engagement in psychological interventions. Nevertheless, available research shows that other dimensions, such as parents’ attribution of problems and parents’ readiness to change, may play an important role in the prediction of parental engagement. These results support the motivational models that emphasize the importance of parents’ perceived need to change and their perceived ability to conduct these changes.
Further studies are needed to identify parental cognitions that promote parents’ engagement in child mental health interventions and that can be targeted in these interventions.
References
Bögels SM, Brechman-Toussaint ML (2006) Family issues in child anxiety: attachment, family functioning, parental rearing and beliefs. Clin Psychol Rev 26:834–856
Dishion TJ, Patterson GR (2006) The development and ecology of antisocial behavior in children and adolescents. In Cicchetti D, Cohen DJ (eds), Developmental psychopathology. Risk, disorder, and adaptation, vol 3 (pp 503–541). Wiley, New York
Forehand R, Jones DJ, Parent J (2013) Behavioral parenting interventions for child disruptive behaviors and anxiety: What’s different and what’s the same. Clin Psychol Rev 33:133–145
Tully LA, Hunt C (2016) Brief parenting interventions for children at risk of externalizing behavior problems: A systematic review. J Child Fam Stud 25:705–719
Finan SJ, Swierzbiolek B, Priest N, Warren N, Yap M (2018) Parental engagement in preventive parenting programs for child mental health: a systematic review of predictors and strategies to increase engagement. PeerJ 6:e4676
Sanders MR, Markie-Dadds C, Rinaldis M, Firman D, Baig N (2007) Using household survey data to inform policy decisions regarding the delivery of evidence-based parenting interventions. Child Care Health Dev 33:768–783
Nowak C, Heinrichs N (2008) A comprehensive meta-analysis of Triple P-Positive Parenting Program using Hierarchical Linear Modeling: effectiveness and moderating Variables. Clin Child Fam Psychol Rev 11:114
Podell JL, Kendall PC (2011) Mothers and fathers in family cognitive-behavioral therapy for anxious youth. J Child Fam Stud 20:182–195
Thomas R, Zimmer-Gembeck MJ (2007) Behavioral outcomes of Parent-Child Interaction Therapy and Triple P-Positive Parenting Program: a review and meta-analysis. J Abnorm Child Psychol 35:475–495
Sawyer MG, Arney FM, Baghurst PA, Clark JJ, Graetz BW, Kosky RJ et al (2001) The mental health of young people in Australia: key findings from the child and adolescent component of the National Survey of Mental Health and well-being. Aust N Z J Psychiatry 35:806–814
Nock MK, Ferriter C (2005) Parent management of attendance and adherence in child and adolescent therapy: a conceptual and empirical review. Clin Child Fam Psychol Rev 8:149–166
Chacko A, Jenden SA, Lowry LS, Cornwell M, Chimklis A, Chan E et al (2016) Engagement in behavioral parent training: review of the literature and implications for practice. Clin Child Fam Psychol Rev 19:204–215
Ingoldsby EM (2010) Review of interventions to improve family engagement and retention in parent and child mental health programs. J Child Fam Stud 19:629–645
Lindsey MA, Brandt NE, Becker KD, Lee BR, Barth RP, Daleiden EL et al (2014) Identifying the common elements of treatment engagement interventions in children’s mental health services. Clin Child Fam Psychol Rev 17:283–298
Staudt M (2007) Treatment engagement with caregivers of at-risk children: gaps in research and conceptualization. J Child Fam Stud 16:183–196
Haine-Schlagel R, Walsh NE (2015) A review of parent participation engagement in child and family mental health treatment. Clin Child Fam Psychol Rev 18:133–150
Garvey C, Julion W, Fogg L, Kratovil A, Gross D (2006) Measuring participation in a prevention trial with parents of young children. Res Nurs Health 29:212–222
Pereira AI, Muris P, Mendonça D, Barros L, Goes AR, Marques T (2016) Parental involvement in cognitive-behavioral intervention for anxious children: parents’ in-session and out-session activities and their relationship with treatment outcome. Child Psychiatry Hum Dev 47:113–123
Dumas JE, Moreland AD, Gitter AH, Pearl AM, Nordstrom AH (2008) Engaging parents in preventive parenting groups: do ethnic, socioeconomic, and belief match between parents and group leaders matter? Health Educ Behav 35:619–633
Reyno SM, McGrath PJ (2006) Predictors of parent training efficacy for child externalizing behavior problems—a meta-analytic review. J Child Psychol Psychiatry 47:99–111
Morawska A, Sanders M (2006) A review of parental engagement in parenting interventions and strategies to promote it. J Child Serv 1:29–40
Spoth R, Redmond C, Haggerty K, Ward T (1995) A controlled parenting skills outcome study examining individual difference and attendance effects. J Marriage Fam 57:449–464
Spoth R, Redmond C, Shin C (2000) Modeling factors influencing enrollment in family-focused preventive intervention research. Prev Sci 1:213–225
Alan EK (1996) Dropping out of child psychotherapy: issues for research and implications for practice. Clin Child Psychol Psychiatry 1:133–156
Kazdin AE, Holland L, Crowley M, Breton S (1997) Barriers to treatment participation scale: evaluation and validation in the context of child outpatient treatment. J Child Psychol Psychiatry 38:1051–1062
Kazdin AE, Holland L.,Crowley M (1997) Family experience of barriers to treatment and premature termination from child therapy. J Consult Clin Psychol 65:453–463
Janz NK, Becker MH (1984) The health belief model: a decade later. Health Educ Q 11:1–47
Miller WR, Rollnick S (2002) Motivational interviewing: preparing people for change, 2nd edn. Guilford Press, New York
Stewart-Brown SL, Schrader-Mcmillan A (2011) Parenting for mental health: what does the evidence say we need to do? Report of workpackage 2 of the dataprev project. Health Promot Int 26:i10–i28
Ruiz-Casares M, Drummond JD, Beeman I, Lach LM (2016) Parenting for the promotion of adolescent mental health: a scoping review of programmes targeting ethnoculturally diverse families. Health Soc Care Community 25:743–757
Bloomquist ML, August GJ, Lee SS, Piehler TF, Jensen M (2012) Parent participation within community center or in-home outreach delivery models of the Early Risers Conduct Problems Prevention Program. J Child Fam Stud 21:368–383
Dumas JE, Nissley-Tsiopinis J, Moreland AD (2007) From intent to enrollment, attendance, and participation in preventive parenting groups. J Child Fam Stud 16:1–26
Nix RL, Bierman KL, McMahon RJ, Conduct Problems Prevention Research Group (2009) How attendance and quality of participation affect treatment response to parent management training. J Cons Clin Psychol 77:429–438
Orrell-Valente JK, Pinderhughes EE, Valente E Jr, Laird RD, Bierman KL, Coie JD et al (1999) If it’s offered, will they come? Influences on parents’ participation in a community-based conduct problems prevention program. Am J Community Psychol 27:753–783
Peters S, Calam R, Harrington R (2005) Maternal attributions and expressed emotion as predictors of attendance at parent management training. J Child Psychol Psychiatry 46:436–448
Topham GL, Wampler KS (2008) Predicting dropout in a filial therapy program for parents and young children. Am J Fam Ther 36:60–78
Abrahamse ME, Niec LN, Junger M, Boer F, Lindauer RJL (2016) Risk factors for attrition from an evidence-based parenting program: findings from the Netherlands. Child Youth Serv Rev 64:42–50
Baker S, Sanders MR (2017) Predictors of program use and child and parent outcomes of a brief online parenting intervention. Child Psychiatry Hum Dev 48:807–817
Chen YC, Fortson BL (2015) Predictors of treatment attrition and treatment length in Parent-Child Interaction Therapy in Taiwanese families. Child Youth Serv Rev 56:28–37
Danko CM, Garbacz LL, Budd KS (2016) Outcomes of Parent–Child Interaction Therapy in an urban community clinic: a comparison of treatment completers and dropouts. Child Youth Serv Rev 60:42–51
Davidson KH, Fristad MA (2006) The Treatment Beliefs Questionnaire (TBQ): an instrument to assess beliefs about children’s mood disorders and concomitant treatment needs. Psychol Serv 3:1–15
Eisner M, Meidert U (2011) Stages of parental engagement in a universal parent training program. J Prim Prev 32:83–93
Kazdin AE (1990) Premature termination from treatment among children referred for antisocial behavior. J Child Psychol Psychiatry 31:415–425
Lanier P, Kohl PL, Benz J, Swinger D, Moussette P, Drake B (2011) Parent–child interaction therapy in a community setting: examining outcomes, attrition, and treatment setting. Res Soc Work Pract 1:689–698
Lavigne JV, Lebailly SA, Gouze KR, Binns HJ, Keller J, Pate L (2010) Predictors and correlates of completing behavioral parent training for the treatment of oppositional defiant disorder in pediatric primary care. Behav Ther 41:198–211
Leung C, Sanders M, Ip F, Lau J (2006) Implementation of triple P-positive parenting program in Hong Kong: predictors of programme completion and clinical outcomes. J Child Serv 1:4–17
Miller GE, Prinz RJ (2003) Engagement of families in treatment for childhood conduct problems. Behav Ther 34:517–534
Plueck J, Freund-Braier I, Hautmann C, Beckers G, Wieczorrek E, Doepfner M (2010) Recruitment in an indicated prevention program for externalizing behavior—parental participation decisions. Child Adolesc Psychiatry Ment Health 4:15–15
Prinz RJ, Miller GE (1994) Family-based treatment for childhood antisocial behavior: experimental influences on dropout and engagement. J Consult Clin Psychol 62:645–650
Werba BE, Eyberg SM, Boggs SR, Algina J (2006) Predicting outcome in parent-child interaction therapy: success and attrition. Behav Modif 30:618–646
Winslow EB, Bonds D, Wolchik S, Sandler I, Brayer S (2008) Predictors of enrollment and retention in a preventive parenting intervention for divorced families. J Prim Prev 30:151–172
Calam R, Sanders MR, Miller C, Sadhnani V, Carmont SA (2008) Can technology and the media help reduce dysfunctional parenting and increase engagement with preventative parenting interventions? Child Malt 13:347–361
Michael BW, Anna S, Raziye S (2015) Mothers’ and fathers’ attendance in a community-based universally offered parenting program in Sweden. Scand J Public Health 44:274–280
Kazdin AE, Mazurick JL (1994) Dropping out of child psychotherapy: distinguishing early and late dropouts over the course of treatment. J Consult Clin Psychol 62:1069–1074
McWey LM, Holtrpo K, Wojciak AS, Claridge AM (2015) Retention in a parenting intervention among parents involved with the child welfare system. J Child Fam Stud 24:1073–1087
Schneider BW, Gerdes AC, Haak LM, Lawton KE (2013) Predicting treatment dropout in parent training interventions for families of school-aged children with ADHD. Child Fam Behav Ther 35:144–169
Stadnick NA, Haine-Schlagel R, Martinez JI (2016) Using observational assessment to help identify factors associated with parent participation engagement in community-based child mental health services. Child Youth Care Forum 45:745–758
Baydar N, Reid MJ, Webster-Stratton C (2003) The role of mental health factors and program engagement in the effectiveness of a preventive parenting program for Head Start mothers. Child Dev 74:1433–1453
Ryan SM, Boxmeyer CL, Lochman JE (2009) Influence of risk factors for child disruptive behavior on parent attendance at a preventive intervention. Behav Disord 35:41–52
Knox M, Burkhart K (2014) A multi-site study of the ACT Raising Safe Kids program: predictors of outcomes and attrition. Child Youth Serv Rev 39:20–24
Chacko A, Wymbs BT, Rajwan E, Wymbs F, Feirsen N (2017) Characteristics of parents of children with ADHD who never attend, drop out, and complete behavioral parent training. J Child Fam Stud 26:950–960
Roberts MW, Joe VC, Rowe-Hallbert A (1992) Oppositional child behavior and parental locus of control. J Clin Child Psychol 21:170–177
Nock MK, Ferriter C, Holmberg E (2007) Parent beliefs about treatment credibility and effectiveness: assessment and relation to subsequent treatment participation. J Child Fam Stud 16:27–38
Nock MK, Kazdin AE (2001) Parent expectancies for child therapy: assessment and relation to participation in treatment. J Child Fam Stud 10:155–180
Wade M, Andrade BF (2015) Validation of a measure of parental readiness for treatment in a clinical sample of children with disruptive behavior. J Psychopathol Behav Assess 37:184–195
Morrissey-Kane E, Prinz R (1999) Engagement in child and adolescent treatment: the role of parental cognitions and attributions. Clin Child Fam Psychol Rev 2:183–198
Schwarzer R, Renner B (2000) Social-cognitive predictors of health behavior: action self-efficacy and coping self-efficacy. Health Psychol 19:487–495
Piotrowska PJ, Tully LA, Lenroot R, Kimonis E, Hawes D, Moul C et al (2017) Mothers, fathers, and parental systems: a conceptual model of parental engagement in programmes for child mental health—connect, attend, participate, enact (CAPE). Clinic Child Fam Psychol Rev 20:146–161
Lundahl BW, Tollefson D, Risser H, Lovejoy MC (2007) A meta-analysis of father involvement in parent training. Res Soc Work Pract 18:97–106
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Pereira, A.I., Barros, L. Parental Cognitions and Motivation to Engage in Psychological Interventions: A Systematic Review. Child Psychiatry Hum Dev 50, 347–361 (2019). https://doi.org/10.1007/s10578-018-0852-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10578-018-0852-2