
Abstract
A variety of predictors of parent participation in prevention programming have been identified in past research, but few studies have investigated how those predictors may vary by implementation context. Patterns of parent participation were examined in the Early Risers Conduct Problems Prevention Program using two family-focused service delivery models: a community center model (Center) and an in-home outreach-based model (Outreach). An ethnically diverse sample of Kindergarten through second grade students (n = 246) displaying elevated levels of aggression were recruited for the study and randomly assigned to either the Center (n = 121) or Outreach (n = 125) models. In both delivery models, participants and their families completed an assortment of baseline measures and received family skills and child skills intervention components and family- and school-based case management. Parents in the Center model demonstrated greater overall participation in family-focused components of the intervention. Parent motivation with parent-focused expectancies for the intervention represented the strongest predictor of parent participation across both delivery models. Family income differentially predicted parent participation across the two models, with low income predicting greater participation in the Center model and lower participation in the Outreach model. A qualitative finding emerged showing that parents receiving parent skills in the Center model via groups preferred to learn skills related to facilitating overall family relationships, whereas parents receiving parent skills via individual Outreach meetings preferred to improve a child’s behavior and emotion skills. Implications are discussed for the design of prevention programming in order to maximize parent participation in high risk populations.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
When evidence-based prevention programs are delivered in “real world” settings, low rates of parent participation can jeopardize impact and replication (August et al. 2003, 2006; Garvey et al. 2006). Many participant characteristics have been investigated for their relationship to parent participation in prevention and treatment targeting children’s problem behavior. Family demographic variables such as minority status, lower socio-economic status, single parent status, and larger family size have been associated with indicators of lower parent participation rates (August et al. 2003; Coatsworth et al. 2006; Gorman-Smith et al. 2002; Kazdin et al. 1995; Lavigne et al. 2010; Scott et al. 2010). Several studies show lower parent participation is associated with higher severity of child behavior problems (August et al. 2003; Boxmeyer and Lochman 2006; Gorman-Smith et al. 2002; Watt et al. 2007), while one study showed that parents participate more when their child has more severe behavior problems (Dumas et al. 2007). Parents (primarily mothers) exhibiting high stress, distress, and/or mood difficulties are at risk for poor participation (Capage et al. 2001; Chronis et al. 2004; Kazdin et al. 1995; Werba et al. 2006), and one study showed that less participation was predicted by higher levels of parents’ frustration in the parent–child relationship (Bloomquist et al. 2009). The role of parents’ personality in participation is an area in need of further study. Perhaps parent personality characteristics associated with sociability such as extraversion, or traits that could impact help-seeking, such as neuroticism, might be associated with participation. Most of these variables reflect enduring characteristics and may not be amenable to change.
Researchers also have examined parent cognition as a participant characteristic predictive of parent participation. Parents’ perceptions of barriers associated with intervention, demands imposed by intervention, relevance of intervention, and relationship with the provider are predictive of their level of participation in outpatient treatment (Kazdin et al. 1997) and community-based prevention programming (Lee et al. 2006). In clinic-based parent training it was shown that parent motivation for treatment predicted parents’ perceived barriers to treatment participation, and this in turn predicted parents’ participation in treatment (Nock and Photos 2006). Finally, parents who identify an expectation that the intervention should be directed at the child were more likely to drop out of a parenting-focused intervention than those who endorsed an expectation for parenting skills (Miller and Prinz 2003). In a related manner, a daycare-based parenting intervention targeting low income, urban, minority families with young children produced high rates of participation when parents reported goals that matched the focus of the intervention (Gross et al. 2001). Such findings could lead to better understanding of parents’ views of intervention.
Another approach has been to investigate the role of program implementation context on predicting parents’ participation in parenting-focused programs. In one study evaluating parents’ intent to participate, program delivery methods (e.g., duration, format, and content) explained more variance (30%) in parent intent than all other factors combined (Matsumoto et al. 2009). In another study, parents were more inclined to attend group delivered behavioral parent training provided in a community setting than individual delivered training in a clinic setting (Cunningham et al. 1995). Finally, in a community prevention initiative, parent participation was predicted by the level of experience of the implementer, personality of the implementer (characteristics of high extraversion, low neuroticism, and low agreeableness), and if the implementer provided services in a quality manner (Bloomquist et al. 2009). Additional research is needed to examine the role of implementation context as a means to enhance parent participation.
Surprisingly, there has been little work investigating how participant characteristics interact with implementation context on parent participation in prevention programs. It may be instructive to determine which child, parent, and/or family characteristics predict greater participation in various implementation contexts. The current study explored these issues by evaluating rates and predictors of parent participation within a family-focused component of the Early Risers conduct problems program (August et al. 2001, 2003, 2006; Bernat et al. 2007) that was delivered in two distinct implementation contexts. A community center-based model (hereafter referred to as Center) offered services in local neighborhood centers that have many resources to assist and empower families (elaborated on below) as the primary program venue. In the Center model all parents were offered a standardized exposure of family-focused program services. A ‘Parent Skills’ subcomponent was provided in groups where parents were led by implementers to a consensus about which content skills strategies were a focus, and a ‘Family Support’ subcomponent emphasized center-based referrals to access services to assist the family. In an in-home outreach-based model (hereafter referred to as Outreach), services were provided primarily in the home. The parents in Outreach were offered individualized exposure for ‘Parent Skills’ and ‘Family Support’ programming based on need. Parent Skills was provided on a one-parent-at-a-time basis where parents were led by implementers to determine which content skills strategies were a focus for their family, and Family Support emphasized community-based referrals (outside of the center) to access services to assist the family. Although not the focus of this study, the same Early Risers ‘Child Skills’ and ‘Child School Support’ subcomponents were provided over an average of 16 months to children in local schools in both conditions (see August et al. 2007 for a detailed description of Early Risers program).
It was hypothesized that both models would yield variation in participation rates. It was further hypothesized that parent participation globally, and within each program delivery model specifically, would be predicted by baseline participant characteristic variables such as family demographics, parent report of child and parenting status, parent report of personal status, and parent report of pre-intervention cognitions about the intervention. We relied exclusively on parent report of predictors reasoning that parents’ perceptions on these variables had the most proximal impact on their subsequent participation. To avoid a selection bias we randomized families to Center or Outreach models. To our knowledge this randomized experimental design has not been previously used within a prevention context with elementary age children and their families. This study is therefore viewed as exploratory and no specific hypotheses are offered about which model would yielded higher parent participation rates or which variables would best predict global participation or context model-specific participation. It was anticipated, however, that the results from this research would yield informative data regarding the ‘fit’ between child/parent/family characteristics and implementation context.
Methods
Intervention Sites and Personnel
This study was executed within a collaborative effort that included Pillsbury United Communities family services agency in Minneapolis, Minneapolis Public Schools, and University of Minnesota Early Risers prevention team (see Bloomquist et al. 2008 for more information on this community-university partnership). Pillsbury United Communities is a longstanding family service agency that provides safety net and practical family services to low-income families through six affiliated neighborhood centers throughout Minneapolis. The agency operates numerous programs within each affiliated neighborhood center that focus on basic needs (food, housing, accessing county services), employment and economic development (job counseling, promotion of small business ventures), community-building (neighborhood meetings, arts festivals, community plays, cultural celebrations, after school programming), and health/wellness services (exercise classes, nutritional information, primary care health provision). All implementation staff, known as Family Advocates (FAs), was employed by Pillsbury United Communities, and was housed at two of the neighborhood centers (one on the near north side and the other on the near south side of Minneapolis). They worked with children enrolled in nine nearby demographically equivalent K-6th grade elementary schools.
The responsibilities of the FAs included recruitment of at-risk children eligible for participation in Early Risers and delivery of all programming. FAs provided co-located Child Skill and Child School Support programming in school settings. They delivered the family-focused components of Parent Skills and Family Support interventions primarily in the neighborhood family centers in the Center model and primarily in the home in the Outreach model. All FAs spoke English, but several of them were also fluent in Spanish, and they were assigned to schools that had the largest Spanish-speaking populations. During the first 2 years of this 4-year project there were eight full time equivalent (FTE) FA positions and two half-time program supervisory positions. For the last 2 years of the program, the number of FA positions was reduced to three FTE and there was only one program supervisor.
Identification, Assignment, and Recruitment of Subjects
A University of Minnesota IRB approved, multi-stage protocol was used to enroll children and families in the Early Risers program, and subsequently to recruit them to participate in a research study to evaluate the program. A refer and screen method was used to identify subjects eligible for enrollment in the Early Risers program offered at their school. Teachers nominated students who were demonstrating high levels of disruptive behavior in their classrooms and then screened those children on the standardized 25-item Aggression scale of the Child Behavior Checklist—Teacher Rating Form (CBC-TRF; Achenbach 1991). Children were eligible for the program and research study if they obtained a T-score ≥ 57 on the CBC-TRF Aggression scale. Children were excluded, however, if the child had IQ ≤ 70 or a pervasive developmental disorder and/or if school officials reported that the parents did not have at least rudimentary proficiency in either English or Spanish.
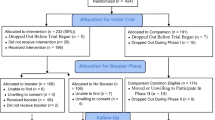
If a child met eligibility criteria for the study, his/her de-identified data were sent to Pillsbury United Communities agency. Next, his/her family was randomly assigned, via a stratified randomization procedure at the subject level, to Center or Outreach family-focused conditions, by a program supervisor at Pillsbury United Communities. The sample was stratified by gender (boy/girl), grade (K, first, second), and neighborhood center (one of two geographically based centers). At the same time the families of children meeting criteria were asked by a school liaison worker if they would be interested in participating in the Early Risers program offered at their school and explained the partnership between Pillsbury United Communities, Minneapolis Public Schools, and University of Minnesota. If the family was agreeable, the child and family were then recruited by the FA for Early Risers family-focused programming based on prior randomization. If parents agreed to enroll their child in the program, they were offered the voluntary opportunity to participate in the research study. Parents were informed of the requirements associated with participating in the research study including annual assessments conducted by the University of Minnesota research team, and they were informed there would be a compensation of $50 for each parent-completed assessment. Parents were further informed their family could receive Early Risers without consenting to serve as research participants if they should so choose. If parents were interested in the program and the research project, the FAs (who were fully trained in University of Minnesota IRB approved recruitment process) obtained consent from the primary parent/guardian and assent from the child.
Participant Characteristics
Participants in this study were 246 children in Kindergarten through second grade living in economically disadvantaged areas of Minneapolis, Minnesota, and their families. Initially, the recruitment and consent process yielded 261 families (131 = Center and 130 = Outreach). Ninety-four percent participated in parent baseline assessment (n = 246; 121 = Center and 125 = Outreach). The sample included 60% males and the average child age at study enrollment was 6.7 (SD = 1.0) years. Approximately 52% of the children were African American, 13% Hispanic, 9% multiracial, 8% Caucasian, and 18% other ethnicity. Approximately 41% of the children resided in single-parent households. The mean CBC-TRF Aggression score was 61.41 (SD = 12.45) for children in the Center model and 60.34 (SD = 15.50) for children in the Outreach model, a different that was not statistically different (t = .60, p = .55). Descriptive characteristics of the participants in the Center and Outreach models are presented in Table 1. There were no significant group differences in any of the demographic variables.
Interventions
In the prototype Early Risers program, aggressive/disruptive elementary-age children receive ‘Child Skills’ training and ‘Child School Support’ case management component interventions, and the family is offered ‘Parent Skills’ and ‘Family’ Support’ case management interventions. All interventions are delivered in a coordinated manner by a trained implementer. In this study, the child-focused components were identical in both Center and Outreach, and this included continuous fixed-prescription Child Skills subcomponent consisting of (1) small-group social-emotional skills training, (2) literature appreciation, and (3) creative/recreational activities delivered during the school year and over one summer (6–8 weeks) and a variable-prescription Child School Support subcomponent that included monitoring and mentoring of child at school, facilitation of communication between school and home, and informal consultation with the teacher (see August et al. 2007 for details).
Similarities Across Family-Focused Program Delivery Models
Several engagement strategies were used by FAs to promote parent participation in both program delivery models. Parent participants assigned to the Center or Outreach models received up to two prescribed engagement-oriented meetings that were delivered by FAs at the home or school. In the Center condition, however, there was an expressed goal of transitioning families to receive direct services (Parent Skills and Family Support) at the center. During these initial engagement meetings, the FAs fully informed the parents of family-focused interventions and used a semi-structured interview to elicit information regarding their strengths and concerns with respect to the child and parent/family. This information was used to identify areas of focus, set goals, and to inform the family how their goals might be facilitated by participating in the family-focused components. In addition, once programming began, parents in both conditions were paid $20 for each completed “Success Plan” used within Parent Skills (described below).
The content offered in Parent Skills and Family Support was identical in both Center and Outreach programming. Using principles of evidence-based practice (American Psychological Association 2006); a Parent Skills curriculum was developed by the Early Risers team which presented parenting-specific content via 19 Success Plans. These Success Plans covered topics relevant to parenting children with behavior challenges and was organized into six modules for promoting (1) behavior, (2) social, (3) emotional, and (4) academic child development, as well as (5) parent and (6) family well-being (see Table 5 for more information). The Success Plans are each about two to six pages (including illustrations and charts) and are available in English and Spanish. The Success Plans were read jointly by the implementer and the parent(s). If a parent had limited reading ability the FAs verbally summarized the content and focused on presenting the illustrations and/or charts. The FAs modeled the skills and engaged the parents in role play practice if the parents were comfortable doing so. Parents were asked comprehension questions (that are specified in the accompanying implementer manual) and were also asked to set goals to use the parenting strategies. In subsequent meetings the FAs inquired with parents about whether or not they were attaining their goal(s) and problem-solved with parents who had difficulty meeting them. The Family Support intervention addressed family needs through individualized case management, personal goal setting/attainment, and referrals to access services outside of Early Risers to address basic needs of the family and/or physical/mental health issues of the child/parents.
Differences Between Family-Focused Program Delivery Models
Participants in the Center model were offered the majority of programming in a Pillsbury United Communities neighborhood center and referrals for additional supports were made principally within the center (FAs used an agency published “Pillsbury United Communities Resource Guide” as a referral source). All participants in the Center model were offered 10 sixty-minute sessions of the Parent Skills group which were delivered via Family Nights at the center. The Family Nights included brief parent–child bonding activities before or after the Parent Skills groups, and while the parents met in their Parent Skills group, the children were engaged in recreational activities with other center staff. In Parent Skills groups the parents were led by the FA to consensually choose from a menu of Success Plans (see Table 5) to reflect the preferences of what the group wanted to cover over 10 sessions (this was flexible and could be revised at any time). The location of Family Support contacts was primarily at the center and was delivered via one-to-one meetings with the FAs. The Family Support contacts often occurred before or after Parent Skills meetings, but were also conducted at times convenient to the parents. The protocol called for each family to receive a minimum of three Family Support contacts to check in and assess potential needs, but could be as many as indicated depending on level of need. There was no specified amount of time prescribed for Family Support.
Participants in the Outreach model were offered services mostly in their home and referrals within the Family Support emphasized accessing community resources (FAs used a community published “Minneapolis Handbook of the Streets” as a referral source). There was explicit instruction to not guide families to the Pillsbury United Communities agency unless the family directly asked for such referral information. Participants in this condition received individualized Parent Skills integrated with Family Support during each meeting (i.e., sessions combined both Parent Skills and Family Support activities). The parents were led by the FA to choose from a menu of Success Plans (see Table 5) to reflect the parent’s preferences of what he or she wanted to cover during the meetings (this was flexible and could be revised at any time). The frequency of family-focused meetings in Outreach was based on a level of need that was determined by the child’s severity of behavior problems and the parent’s expressed concerns about the family that were ascertained via the above noted semi-structured interview used during the engagement meetings. The implementer manual included an algorithm to assist FAs in categorizing families as Level 1—low child severity/low family severity; Level 2—high child severity/low family severity or low child severity/high family severity; and Level 3—high child severity/high family severity. The protocol called for each family to receive the following amount of family-focused services depending on assessed need: Level 1—minimum of 3 contacts, Level 2—approximately 10 contacts, and Level 3—10 + contacts (whatever was needed).
Implementation Support
Training
Each FA and program supervisor was provided a personal copy of the project manual and related materials. Initial three-day training was provided for each FA and program supervisor by the program developers. It included an overview of the study, a complete review of the project manual, modeling of intervention skills, and role-play activities. Since FAs were assigned to work with all of the children referred in a school, and each child’s parent/family was randomly assigned to a treatment condition, they were trained to deliver both the Center and Outreach models of family-focused service delivery. A significant portion of the training included differentiation of procedures between the two models and the importance of implementing them as specified by the manual. The research staff provided a half-day booster training session to the FAs and program supervisors each fall to promote continued adherence to the research protocol. Whenever staff turnover occurred, new FAs completed an abbreviated one-day training of all interventions provided by program developer staff, and they shadowed/assisted an existing FA in providing all child-focused and family-focused services (in Center and Outreach models) to families for several weeks before working independently.
Site Supervision
Each FA was supervised by a program supervisor employed by Pillsbury United Communities agency. The FAs reported directly to the program supervisor and had weekly group and individual supervision meetings with them. FAs were also expected to consult with the program supervisor in the event of an emergency or deviation from study protocol.
Program Oversight and Technical Assistance
Pillsbury United Communities agency was responsible for day-to-day management and oversight of the program. The Early Risers program developers and/or a highly trained/experienced Early Risers program manager met with and/or had phone contacts with program supervisors on a weekly basis throughout the project. These meetings/phone contacts focused on technical assistance, review of program progress, and resolution of any emerging concerns/problems. In addition, the Early Risers program developers and/or a highly trained/experienced Early Risers program manager met directly with the FAs approximately monthly to check in, troubleshoot any implementation obstacles/problems, and review service delivery specifications.
Adherence of Service Delivery Model
Weekly logs were completed by FAs to document adherence to Center and Outreach delivery models. Table 2 summarizes Type of Contact frequency data. As expected the Center model had significantly more contacts at the center than Outreach [Center, n = 61 (50%) vs. Outreach, n = 16 (14%), χ2(1) = 40.45, p < .001] and Outreach had significantly more contacts in homes than Center [Center, n = 66 (55%) vs. Outreach, n = 85 (68%), χ2(1) = 9.36, p = .030]. It can be seen, however, that both Center and Outreach family services were sometimes delivered in the other models preferred setting. When FAs delivered the Center model they also used some home contacts to deliver the above described engagement meetings and these contacts are included in Table 2 data. For the Center model the FAs were supposed to transition to having subsequent service delivery contacts at the center, but apparently in some cases additional contacts were used in the home that went past the two engagement home visits. FAs reported in supervision and technical assistance meetings that it was hard to engage some families exclusively in the Center model and once services began they felt ethically obligated to work with them which sometimes necessitated more home visits than specified in the manual. FAs delivering Outreach also had some center visits with Outreach families, but only a small number (n = 16). FAs reported in supervision and technical assistance meetings that some of the Outreach families were already consumers of the center and/or lived in close proximity to it and came in on their own accord. Table 2 also shows that the Center model had more contacts in school/other settings and more phone contacts than Outreach. Since both models involved school-based child-focused programming (described earlier) it is to be expected that some contacts with the parents might occur in school within both Center and Outreach models. Other settings for Family Support-related contacts might be at a clinic or social services agency which could be used in either Center or Outreach models on occasion. Phone contact was also encouraged in both Center and Outreach models to engage families, coordinate appointments, and check-in on progress. On balance, when considering the all of the above information, we conclude that adherence to the Center and Outreach models was acceptable and satisfactory in terms of type of contact because a majority of contact within each model was as specified in the manual with justifiable reasons noted for exceptions.
Indicators of Parent Participation in the Family-Focused Programming
Frequency of Family-Focused Contacts and Number of Minutes
Since Parent Skills and Family Support were delivered simultaneously in Outreach the participation data for both of these interventions was combined for both Center and Outreach so they could be compared as an overall indication of family-focused participation. For Center model, parents’ participation was measured by contacts and minutes of services received in Parent Skills and also Family Support, and these scores were combined into number of contacts and number of minutes as indicators for family-focused participation. For Outreach model parents’ participation was measured by their contacts and minutes of services received each meeting with the FA (which typically combined Parent Skills and Family Support strategies) thus providing number of contacts and number of minutes as indicators for family-focused participation.
Frequency of Success Plans
The number of Success Plans that parents received during Parent Skills was also tabulated. Since any number of Success Plans could be presented and trained at any one contact in both Center and Outreach, a simple frequency was calculated. This entails the number of Success Plans presented and trained on with the parents irrespective of contact and/or minutes of participation.
Predictor Measures Administered at Baseline
Family Demographics
A Biographical Questionnaire was use to obtain information pertaining to single parent status, mothers’ education level, minority status, and household income.
Parent Report on Child and Parenting
The Behavioral Assessment System for Children, Parent Rating Scales (BASC-2-PRS; Reynolds and Kamphaus 2004) is a broadband behavioral rating instrument with good reliability and validity (α = .77 to .94). Gender-specific T-scores are provided with a mean of 50 and a standard deviation of 10. Scores on the Externalizing Composite scale (α = .92) were used to assess parent perceptions of the child’s global behavioral functioning from the parent’s perspective.
The Parenting Relationship Questionnaire (PRQ; Kamphaus and Reynolds 2006) is a 71-item self report measure that assesses a parent’s perspective of the parent–child relationship. Gender-specific T-scores are provided with a mean of 50 and a standard deviation of 10. In this study, the Discipline Practices (α = .86) and Relational Frustration (α = .81) were examined.
Parent Report on Self
The Brief Symptom Inventory 18 (BSI 18; Derogatis and Melisaratos 1983) is a self-report symptom inventory designed to measure psychological distress in the parent. The instrument has 18 items that can be aggregated to form the Global Severity Index (GSI) score (α = .87). Gender specific normative scores are provided in the form of T-scores with a mean of 50 and a standard deviation of 10.
The NEO-Five Factor Inventory (NEO-FFI; Costa and McCrae 1992) is a 60-item self-report inventory designed to assess domains of personality. The NEO-FFI was developed by a combination of rational methods and factor analytic research on the structure of personality and has been the subject of extensive research. Considerable evidence of validity and reliability is available for this measure (Caruso 2000; Costa and McCrae 1992). In this study, scales of Neuroticism (α = .74) and Extraversion (α = .60) were examined.
Parent Report on Intervention
The Parent Views of Intervention Questionnaire (PVIQ) was created by the researchers specifically for this study. The PVIQ is a 23-item self-report measure of parent’s a priori perceptions and thoughts related to participating in the Early Risers program. The PVIQ was constructed by adapting items from the Parent Motivation Inventory (Nock and Photos 2006), Barriers to Treatment Participation Scale (Kazdin et al. 1997), and the Credibility/Expectancies Questionnaire-Parent Version (Nock et al. 2007) to fit a prevention context within Early Risers. Prior to intervention (at baseline) the research technician reiterated the intervention methods and goals within the Early Risers program to parents. The parent then answered questions on the PVIQ to reflect their views of the Early Risers program. PVIQ items are answered using a five-point scale (1 = strongly disagree; 5 = strongly agree).
A principal components analysis (PCA) was conducted on an original 24-item pool to examine the internal structure of the PVIQ (n = 237). Varimax rotation was used because we expected the three components to be orthogonal based on prior evaluation in the treatment literature (e.g., Kazdin et al. 1997; Miller and Prinz 2003; Nock and Photos 2006). Three factors emerged from this analysis including (i) Parent Motivation and Parent-Focused Expectancies (10 items), (ii) Anticipated Barriers and Obstacles (8 items), and (iii) Child-Focused Expectancies (5 items; see the "Appendix"). The resulting eigenvalues and scree plot from the PCA supported a three component solution, in which the three components accounted for approximately 44% of the variance in scores (see Table 3). Using a cut of .40 factor loading, one item did not load on any factor. Each scale obtained adequate internal validity (Parent Motivation and Parent-Focused Expectancies scale: α = .87; Anticipated Barriers and Obstacles: α = .79; Child-Focused Expectancies scale: α = .78) The Parent Motivation and Parent-Focused Expectancies scale was not significantly correlated with the Anticipated Barriers and Obstacles scale (r = −.08), but was positively associated with the Child-Focused Expectancies scale (r = .27, p < .001). The Anticipated Barriers and Obstacles was not associated with the Child-Focused Expectancies scale (r = .01).
Results
Parent Participation Rates in Family-Focused Programming
We examined the number of parents who received services within Center and Outreach. Data in Table 4 shows that a total of 114 parents from the Center model (94% of those enrolled) and 111 parents from the Outreach model (89% of those enrolled) participated in at least one contact of any type and there were no significant between group differences [χ2(1) = 2.31, p = .13]. Next, we looked at the total dosage of services received by parents in the Center and Outreach models for those who had any type of contact (see Table 4). The average participation for parents was approximately 21 contacts and 418 min for Center and approximately 15 contacts and 270 min for Outreach. Negative binomial regressions showed that there was a significant intervention model difference in the participation rates for the family-focused component. The result indicated that parents in the Center model received a significantly higher dosage as indicated by more contacts and more minutes of intervention compared to those in the Outreach model.
There was no significant model difference in number of Success Plans received or in the number of parents who received them [Center, n = 39 (32%) vs. Outreach, n = 39 (31%), χ2 (1) = .03, p = .86] (see Table 4). The frequency of each Success Plan preferred by parents was calculated for Combined (representing the whole sample), Center, and Outreach models (see Table 5). Overall, when looking at the combined sample, “Improving Parent Stress Management Skills” and “Noticing a Child’s Positive Behavior” were the most preferred Success Plans. Chi-square tests were conducted to examine Center and Outreach model differences in parent’s preferences for each Success Plan. Group comparisons showed that significantly more parents in the Center model preferred “Managing Sibling and Family Conflicts” and there was a trend for them preferring “Developing Family Routines and Rituals” more than parents in Outreach. On the other hand, compared to parents in Center, more parents in the Outreach model preferred the “Noticing a Child’s Positive Behavior,” “Teaching a Child to Obey,” and “Teaching a Child to Understand and Express Feelings.”
Predictors of Participation in Family-Focused Programming
The associations between predictor measures and total number of minutes of parent participation in family-focused programming were examined. Zero-order correlations were first calculated in order to evaluate any direct associations between predictors and family-focused programming participation. Next, a series of hierarchical multiple regression analyses were conducted in order to examine the ability of predictors to explain variance in family-focused programming participation while controlling for demographic variables and other groups of predictors. Due to a significant amount of positive skew in the distribution of the number of minutes of family-focused programming participation, a log transformation was used on this variable for the following analyses.
Prior to conducting correlation and regression analyses, difference in missing data status was examined for the two conditions. Of the 246 participants, complete data on all variables were available for 145 (Center n = 70 (48%) and Outreach n = 75 (52%), χ 2 = .12, p = .78). Comparisons between those who had complete data versus those who had one or more missing data showed that there were no significant differences between them on child’s age, gender, ethnicity, number of siblings living, and the initial TRF aggression score, and on mother’s age, education level, BSI global severity symptom index score, and number of moved in past year. There were significant differences in annual income level (χ 2 = 6.45, p = .04) and single parent status (χ 2 = 6.14, p = .01). Those who were from the lower income group and those who were from single parent households tended to have more participants with missing data.
Correlational Analyses
Table 6 displays the correlations between each predictor measure and the total number of minutes that parents participated in family-focused programming. Correlations were examined separately for Combined, Center, and Outreach models. In order to investigate if predictor measures differentially predicted participation between the two family-focused delivery models, Fisher’s Z transformations were used to examine significant differences between correlations in Center and Outreach.
A number of correlations between predictor variables and participation emerged as significant. Family income was negatively associated with parent participation in Center (r = −.19, p < .05) and higher income predicted greater participation in Outreach (r = .20, p < .05). These correlations were significantly different (p < .01), meaning that the two models reliably differ in their association between income and parent participation. In the Combined sample, increased parent-reported child externalizing symptoms on the BASC-2 PRS Externalizing Problems composite was associated with increased parent participation (r = .20, p < .01). Two scales from the PRQ—Discipline Practices and Relational Frustration—were both positively associated with higher levels of participation in the Combined sample showing that that parents who were more consistent with discipline and experienced higher levels of frustration in the parent–child relationship were more likely to participate (Discipline Practices: r = .17, p < .05; Relational Frustration: r = .14, p < .05). The Global Severity Index score from the BSI was positively associated with overall participation, reaching significance in the Combined model sample (r = .14, p < .05), thus demonstrating that parents with higher levels of psychological distress showed higher levels of participation. Higher scores on the Neuroticism scale of the NEO-FFI were positively associated with participation in the Center model (r = .27, p < .01), but not in the Outreach model. A Fisher’s Z transformation confirmed that parent Neuroticism showed a stronger positive association with parent participation in the Center model than in the Outreach model (p < .05). Finally, higher scores on the Parent Motivation and Parent-Focused Expectancies scale of the PVIQ were a strong predictor of parent participation, reaching significance in the Combined sample and within each treatment model (Combined: r = .26, p < .001; Center: r = .29, p < .01; Outreach: r = .26, p < .01).
Regression Analyses
A series of hierarchical multiple regression analyses were next analyzed in order to test the ability of the predictor variables in predicting participation while controlling for family demographic information, including family income, ethnicity (African American vs. other ethnicities), single parent status, and mother’s education level. Program delivery model (i.e., Center vs. Outreach) was also entered into each regression model as a second step. The regressions were organized by types of predictors, including Family Demographics, Parent Report of Child and Parenting, Parent Report of Self, and Parent Report of the Intervention. Using the demographic variables as the first step in each regression, and program delivery model as the second step, separate models were analyzed for each of these predictor groupings. Interaction terms between each predictor and program delivery model were then entered into each model to look for differential predictor effects by program model. All variables used in interaction terms were centered on their means. Additionally, a full regression model was analyzed, including each grouping of predictor variables along with significant interaction terms. Because listwise deletion procedures were used for missing data, the number of participants included in each regression model varied by the set of predictor variables examined.
In the base regression model (n = 218) including only the demographic variables (family income, ethnicity, single parent status, and mother’s education level), these variables together did not reliably predict participation in the sample. Program delivery model was a marginally significant predictor of participation when added as a second step to the regression model (Std. β = −.13, p = .06), with the Center model predicting greater participation. When interaction terms were added to the model, the individual interaction term between annual household income and program model was significant (Std. β = −.18, p < .05). Figure 1 shows that lower income predicted greater participation in the Center model, whereas higher income was associated with greater participation in the Outreach model. This interaction term was retained in subsequent regression models in order to control for the interaction effect.

The interaction between income and program delivery model in predicting parent participation in family-focused programming
A regression (n = 166) predicting participation using Parent Report of Child and Parenting variables was examined, including the Discipline Practices and Relational Frustration scales of the PRQ and the Externalizing scale from the BASC-2 PRS. The set of Parent Report of Child and Parenting variables and their interaction terms with delivery model did not aid in prediction of participation after controlling for demographic variables and delivery model.
A regression (n = 176) including Parent Report of Self variables was next examined in order to determine if these variables were predictive of participation while controlling for demographic information and program model. The set of Parent Report of Self variables, including the NEO Extraversion and Neuroticism scales and Global Severity Index score from the BSI and their interaction terms with delivery model did not aid in prediction of participation after controlling for demographic variables and delivery model.
A regression (n = 177) including Parent Report of Intervention variables was analyzed in predicting participation. The Parent Report of Intervention variables, including the PVIQ measures (Parent Motivation and Parent-Focused Expectancies, Anticipated Barriers, and Child-Focused Expectations), were again added in an additional step in order to examine their ability to predict participation while controlling for the demographic variables, program model, and the interaction between program model and income. The regression model including all steps reliably predicted participation (F(9, 167) = 3.90, p < .001). The addition of interaction terms did not significantly improve the model. Looking at individual predictors, the Parent Motivation and Parent-Focused Expectancies scale was a significant predictor of participation (Std. β = .28, p < .001) while controlling for all other factors in the model, with higher motivation and parent-focused expectancies predicting greater participation.
Finally, a full regression model (n = 166) was analyzed, entering each group of predictors described above as a block in a step-wise fashion. Following the demographic variables and program model, Parent Report of Child and Parenting, Parent Report of Self, and Parent Report of Intervention blocks were each entered sequentially. Only the significant interaction term of income by program model was retained and entered along with the demographic variables. All other non-significant interaction terms were not included in the full model. The full regression model including all predictors was a significant predictor of participation (F(15, 129) = 2.27, p = .01). Looking at blocks of predictors, only the Parent Report of Intervention block added significantly to the model following the entry of all other predictors (F Change(3, 129) = 3.29, p < .05). In examining individual predictors within the full regression model with all variables entered, the Parent Motivation and Parent-Focused Expectancies scale from the PVIQ remained a significant predictor of participation (β = .23, p < .05). The interaction term between income and program delivery also retained its significance in the presence of all other predictors (β = −.19, p < .05). Finally, the main effect of program model achieved significance within the context of the full regression model in predicting participation (β = .19, p < .05). It should be noted that program model only achieved marginal significance as a predictor in the larger sample size utilized in the previously described demographics regression model.
Discussion
This study examined parent participation rates within the Early Risers family-focused intervention component delivered via a Center model or an Outreach model. The study sought to determine if parent participation would be greater in one model or the other and if unique participant characteristics would be associated with participation rates across and within Center and Outreach family-focused program delivery models (i.e., fit). Participation data were obtained for the family-focused component (Parent Skills and Family Support) and a select panel of child, parent, and family characteristic measures collected from parents prior to receiving program services, including a new measure to assess parent reported pre-intervention views of the intervention they were offered. The results showed significant differences in parent participation when comparing delivery models. Moreover, baseline measures of participant characteristics predicted participation across and within program models in informative ways.
Parent Participation Rates in Family-Focused Programming
It was hypothesized that there would be differences in parent participation rates for Center and Outreach models (no specific hypotheses were offered about which model might work best). The average total dosage for Center was significantly greater than Outreach (Center average of 21 contacts/418 min > Outreach average of 15 contacts/270 min). Regression analyses also confirmed that the Center model was a better predictor of parent participation than Outreach. There was no significant delivery model difference in number of Success Plans received or in the number of parents who received them. We conclude that Center was better than Outreach in terms of yielding a higher total dosage of participation. This is similar to another study where parent skills training provided in a community setting had better participation than the same services offered in a clinic setting (Cunningham et al. 1995). This finding is also important because research shows that better outcomes are obtained when parents receive a higher dosage (August et al. 2004, 2006).
There may be many reasons why Center had more average dosage in parent participation. Much of the explanation undoubtedly is accounted for by the way in which services are provided within each model (i.e., implementation context). First, service delivery is much more efficient in the Center model where parents are seen in mass for Parent Skills (additionally Center-based Family Support was often provided before and after Parent Skills). Second, in this study parents in Center also received some home contact (although significantly less than Outreach). Third, it’s also true that the Center model had more contacts and minutes in school/other settings and by phone than Outreach. Thus, it appears that Center resulted in more contacts of different types which increased overall participation. Fourth, the Center model may have allowed parents to access a broad array of the Pillsbury United Communities services above and beyond family-focused programming. Although not counted as part of participation, these center resources may have been highly valued by parents, and could have drawn them into the center in general. Fifth, the parents attending Parent Skills groups often socialized and emotionally supported/encouraged each other. This group cohesion may have been enjoyable and/or helpful to parents. Finally, parents attended Parent Skills that were provided within Family Nights and their children also came at the same time to partake in fun recreational activities. It could be that children in the Center model influenced their parents to show up for Family Nights (resulting in more parent participation in Parent Skills and an overall bonding to the center).
The resource-rich center that served as the program venue in the present study is similar to other efforts that have used dedicated resource-rich school space for parents that is designed to enhance parent and family participation in preventive services (Dishion and Kavanagh 2003). Thus, it appears as though providing services to families within a resource rich community or school setting is effective in engaging them in preventive services targeting high-risk children.
In addition to reporting rates of parent participation across delivery models, we also examined the manner in which parents participated within the Parent Skills subcomponent. In the Center model, parents attended groups and were led by FAs to reach a consensus about which Success Plans were preferred by parents for their group meetings, whereas in the Outreach model parents met individually with FAs and were led to pick and choose Success Plans that were uniquely preferred by them during that meeting. When the experimental conditions were combined, the data showed that the Success Plans most preferred by all parents centered on improving parent stress management and reinforcing children’s positive behavior. There was also statistical significance between conditions in preferences of Success Plans. The Center model elicited parent preferences that are more family-oriented to address sibling/family conflicts and enhance family routines/rituals, whereas the Outreach model elicited parent preferences that are more child-oriented to increase positive behavior, reduce disobedience, and enhance a child’s awareness/expression of feelings. These differences may reflect dynamics of group delivery in Center (tailoring by group consensus) and individual delivery in Outreach (tailoring by individual). Perhaps in Parent Skills groups that occurred in Center there was a tendency for parents to select family-oriented content that may be common to all parents. On the other hand, it may be preferred and/or easier to focus on children’s behavior-emotional challenges in a more private one-to-one meeting in an Outreach mode of service delivery. These findings have implication for delivery of parenting skills interventions. If the goal is to buttress overall family interactions then a Center-type parent group format may be most conducive, but if the goal is more on helping a parent manage a child’s behavior and promote child emotion skills then an individualized Outreach-type approach might be best.
Predictors of Parent Participation in Family-Focused Programming
It was hypothesized that child, parent, and family characteristic variables collected prior to start of the intervention would predict parents’ subsequent participation in family-focused programming (no hypotheses were offered about specific predictors of participation within service delivery models). One predictor emerged as highly salient irrespective of service delivery model. This was the strong finding that parents who were highly motivated with parent-focused expectancies for intervention at the outset were most likely to participate, and this reached significance within each family service delivery model and in the combined sample, even when controlling for all other predictors. These results are similar to previous research showing that parent motivation and expectancy of the intervention to focus on the parent is related to higher levels of parent participation (Miller and Prinz 2003; Nock and Photos 2006). This finding is particularly relevant in prevention work. For example, parents invited to participate with their children in the Early Risers program were not necessarily seeking help. If a parent is not motivated nor has parent-focused expectancies for intervention, he/she might require more intensive motivational enhancement efforts prior to intervention onset (e.g., Chaffin et al. 2009; Dishion et al. 2003; McCay et al. 1996; Nock and Kazdin 2005).
Family income status emerged as a unique predictor of participation in both Center and Outreach models. Parents of lower income families were more likely to participate in Center, whereas parents of higher income families exhibited greater participation in Outreach. These findings add to the body of research in the challenging area of engaging low-income parents and families in interventions. Previous research suggests that lower income predicts lower parent participation in parent skills interventions (Coatsworth et al. 2006; Gorman-Smith et al. 2002; Kazdin et al. 1995; Lavigne et al. 2010; Scott et al. 2010), but lower income predicts higher parent participation in a family support-oriented intervention (Bloomquist et al. 2009). In this study, Parent Skills and Family Support interventions were combined. Such an integrated intervention approach increases participation from lower income families who receive programming via a Center model. It is worth emphasizing that the entire sample was low income so those at the extreme of the lower end may be the most stressed and in need of basic living resources. The Center model could well be better for parents of very low income families because they may have benefited from the emotional support and encouragement received in Parent Skills groups, as well as from the assistance and resources offered via Family Support to address income-related basic needs. The Outreach model, on the other hand, may be a better match for relatively higher income families who may be less stressed and less in need of basic resources.
The correlational analyses are suggestive of other relationships between predictors and parent participation. Parents who rated higher levels of externalizing behavior problems in their child and who self-reported being more consistent with discipline and as experiencing higher levels of frustration in the parent–child relationship were more likely to participate. These results are consistent with earlier research showing the same pattern of associations (Bloomquist et al. 2009; Dumas et al. 2007). The finding of parents reporting better discipline methods also participating more seems inconsistent with the finding that highly frustrated parents also attend more. This may suggest; however, that effective parents with difficult children who frustrate them are more likely to attend parent-focused interventions. It is also noteworthy that parents with higher levels of personal distress showed higher levels of participation across service delivery models. This is in contrast with much of the literature showing higher levels on indicators of parent stress/distress is related to lower parent participation (Capage et al. 2001; Chronis et al. 2004; Kazdin et al. 1995; Miller and Prinz 2003; Werba et al. 2006). It should be noted; however, that much of the earlier research pertained to parent skills interventions, while the current results involved the Early Risers family-focused component in which Parent Skills and Family Support are combined. Perhaps combining skills and support strategies is the best way to facilitate the participation of stressed/distressed parents. It is also noteworthy that higher neuroticism in parents was positively associated with parent participation in the Center model but not the Outreach model. This may suggest that parents, who are prone to worry and ruminate, which is typical of more neurotic individuals, perhaps preferred the Center model. It stands to reason that the emotional and tangible support provided by the Center model alleviates some of these parents’ worries and concerns. These correlational results are preliminary given that regression analysis did not replicate them when controlling for demographic variables and other predictors (perhaps due to limited power) but they do suggest predictors of parent participation that merit further investigation.
Summary and Implications for Prevention Programming
Several findings emerged that have implications for providing family-focused prevention services for high risk children. An important result was that Center yielded higher dosage participation than Outreach. This is likely related to the resource-rich center itself which provided many intervention-related and other center-related opportunities to families. Offering parent-focused programming in such a resource-rich center appears to be effective in engaging parents of high-risk children in prevention activities. A qualitative finding was that parents in the Center-type parenting skills group preferred to learn skills related to facilitating overall family relationships, whereas parents participating in Outreach-type individual meetings preferred skills training designed to improve a child’s behavior and emotion skills. Depending on the implementers goals the two different delivery formats could be considered accordingly. There was a robust finding that highly motivated parents with parent-focused expectancies for intervention were more likely to participate regardless of delivery model. The obvious implication is that parents who are less motivated and have child-focused expectancies might profit from motivational enhancement efforts designed to motivate parents and/or alter expectancies to be more in line with a parent-focused intervention. Another key finding was that low income families participated more in Center, perhaps because it was better at meeting the needs of these very low income parents. If the goal is to engage very low income parents it is best to provide services within emotionally supportive parenting groups and to offer assistance and resources in a setting that can directly help families with income-related basic needs. Other correlational findings (as reviewed above) offer avenues for further research exploration.
References
Achenbach, T. M. (1991). Manual for child behavior checklist/4–18 and 1991 Profile. Burlington, VT: University of Vermont, Department of Psychiatry.
American Psychological Association Presidential Task Force on Evidence-Based Practice. (2006). Evidence-based practice in psychology. American Psychologist, 61, 271–285.
August, G. J., Bloomquist, M. L., Lee, S. S., Realmuto, G. M., & Hektner, J. M. (2006). Can evidence-based prevention programs be sustained in community systems-of-care? The Early Risers advanced-stage effectiveness trial. Prevention Science, 7, 151–165.
August, G. J., Bloomquist, M. L., Realmuto, G. M., & Hektner, J. M. (2007). The Early Risers ‘‘Skills for Success’’ Program: A targeted intervention for preventing conduct problems and substance abuse in aggressive elementary school children. In P. H. Tolan, J. Szapocznick, & S. Sambrano (Eds.), Preventing youth substance abuse: Science-based programs for children and adolescents (pp. 137–158). Washington, DC: American Psychological Association.
August, G. J., Lee, S. S., Bloomquist, M. L., Realmuto, G. M., & Hektner, J. M. (2003). Dissemination of an evidence-based prevention innovation for aggressive children living in culturally diverse, urban neighborhoods: The Early Risers effectiveness study. Prevention Science, 4, 271–286.
August, G. J., Lee, S. S., Bloomquist, M. L., Realmuto, G. M., & Hektner, J. M. (2004). Maintenance effects of an evidence-based prevention innovation for aggressive children living in culturally diverse, urban neighborhoods: The Early Risers effectiveness study. Journal of Emotional and Behavioral Disorders, 12, 194–205.
August, G. J., Realmuto, G. M., Hektner, J. M., & Bloomquist, M. L. (2001). An integrated components preventive intervention for aggressive elementary school children: The Early Risers program. Journal of Consulting and Clinical Psychology, 69, 614–626.
Bernat, D., August, G. J., Hektner, J. M., & Bloomquist, M. L. (2007). The Early Risers prevention intervention: Six year outcomes and mediational processes. Journal of Abnormal Child Psychology, 35, 605–617.
Bloomquist, M. L., August, G. J., Horowitz, J., Lee, S. S., & Jensen, C. (2008). Moving from science to practice: Transposing and sustaining the Early Risers conduct problems prevention program in a community service system. Journal of Primary Prevention, 29, 307–321.
Bloomquist, M. L., Horowitz, J. L., August, G. J., Lee, C.-Y. S., Realmuto, G. M., & Klimes-Dougan, B. (2009). Understanding parent participation in a going-to-scale implementation trial of the Early Risers conduct problems prevention program. Journal of Child and Family Studies, 18, 710–718.
Boxmeyer, C. L., & Lochman, J. E. (2006). Predictors of parent engagement in the Coping Power program. Paper presented at the 40th annual meeting of the Association for Behavioral and Cognitive Therapy, Chicago, IL.
Capage, L. C., Bennett, G. M., & McNeil, C. B. (2001). A comparison between African American and Caucasian children referred for treatment of disruptive behavior disorders. Child & Family Behavior Therapy, 23, 1–14.
Caruso, J. C. (2000). Reliability generalization of the NEO personality scales. Educational and Psychological Measurement, 60, 236–254.
Chaffin, M., Valle, L. A., Funderburk, B., Gurwitch, R., Silovsky, J., Bard, D., et al. (2009). A motivational intervention can improve retention in PCIT for low-motivation child welfare clients. Child Maltreatment, 14, 356–368.
Chronis, A. M., Chacko, A., Fabiano, G. A., Wymbs, B. T., & Pelham, W. E. (2004). Enhancements to the behavioral parent training paradigm for families of children with ADHD: Review and future directions. Clinical Child and Family Psychology Review, 7, 1–27.
Coatsworth, J. D., Duncan, L. G., Pantin, H., & Szapocznik, J. (2006). Differential predictors of African American and Hispanic parent retention in a family-focused preventive intervention. Family Relations, 55, 240–251.
Costa, P. T., Jr., & McCrae, R. R. (1992). Revised NEO Personality Inventory (NEO-PI-R) and the NEO Five Factor Inventory (NEO-FFI) Professional Manual. Odessa, FL: Psychological Assessment Resources.
Cunningham, C. E., Bremner, R. B., & Boyle, M. (1995). Large group community-based parenting programs for families of preschoolers at risk for disruptive behaviour disorders: Utilization, cost effectiveness, and outcome. Journal of Child Psychology and Psychiatry, 36, 1141–1159.
Derogatis, L. R., & Melisaratos, N. (1983). The brief symptom inventory: An introductory report. Psychological Medicine, 13, 596–605.
Dishion, T., & Kavanagh, K. (2003). Intervening in adolescent problem behavior: A family-centered approach. New York: Guilford Press.
Dishion, T. J., Nelson, S. E., & Kavanaugh, K. (2003). The family check-up with high-risk young adolescents: Preventing early-onset substance use by parent monitoring. Behavior Therapy, 34, 553–571.
Dumas, J. E., Nissley-Tsiopinis, J., & Moreland, A. D. (2007). From intent to enrollment, attendance, and participation in preventive parenting groups. Journal of Child and Family Studies, 16, 1–26.
Garvey, C., Julion, W., Fogg, L., Kratovil, A., & Gross, D. (2006). Measuring participation in a prevention trial with parents of young children. Nursing & Health, 29, 212–222.
Gorman-Smith, D., Tolan, P. H., Henry, D. B., Leventhal, A., Schoeny, M., Lutovsky, K., et al. (2002). Predictors of participation in a family focused preventive-intervention. Psychology of Addictive Behaviors, 16, S55–S64.
Gross, D., Julion, W., & Fogg, L. (2001). What motivates participation and drop-out among low-income urban families of color in a prevention intervention. Family Relations, 50, 246–254.
Kamphaus, R. W., & Reynolds, C. R. (2006). Parenting Relationship Questionnaire (PRQ). Bloomington, MN: Pearson Assessments.
Kazdin, A. E., Holland, L., Crowley, M., & Breton, S. (1997). Barriers to treatment participation scale: Evaluation and validation in the context of child outpatient treatment. Journal of Child Psychology and Psychiatry, 38, 1051–1062.
Kazdin, A. E., Stolar, M. J., & Marciano, P. L. (1995). Risk factors for dropping out of treatment among White and Black families. Journal of Family Psychology, 9, 402–417.
Lavigne, J. V., LeBailly, S. A., Gouze, K. R., Binns, H. J., Keller, K., & Pate, L. (2010). Predictors and correlates of completing behavioral parent training for the treatment of oppositional defiant disorder in pediatric primary care. Behavior Therapy, 41, 198–211.
Lee, S. L., August, G. J., Bloomquist, M. L., Mathy, R., & Realmuto, G. M. (2006). Implementing an evidence-based preventive intervention in Neighborhood Family Centers: Examination of perceived barriers to program participation. Journal of Primary Prevention, 27, 573–597.
Matsumoto, Y., Sofronoff, K., & Sanders, M. R. (2009). A socio-ecological predictor model of parental intention to participate in a Triple P Positive Parenting Program. Journal of Child and Family Studies, 18, 274–283.
McCay, M., Nudelman, R., McCadam, K., & Gonzales, J. (1996). Evaluating a social work engagement approach to involving inner-city children and their families in mental health care. Research on Social Work Practice, 6, 462–472.
Miller, G. E., & Prinz, R. J. (2003). Engagement of families in treatment for childhood conduct problems. Behavior Therapy, 34, 517–534.
Nock, M. K., Ferriter, C., & Holmberg, E. (2007). Parent beliefs about treatment credibility and effectiveness: Assessment and relation to subsequent treatment participation. Journal of Child and Family Studies, 16, 27–38.
Nock, M. K., & Kazdin, A. E. (2005). Randomized controlled trial of a brief intervention for increasing participation in parent management training. Journal of Consulting and Clinical Psychology, 73, 872–879.
Nock, M. K., & Photos, V. (2006). Parent motivation to participate in treatment: Assessment and prediction of subsequent participation. Journal of Child and Family Studies, 15, 345–358.
Reynolds, C. R., & Kamphaus, R. W. (2004). Behavior assessment system for children (2nd ed.). Circle Pines, MN: American Guidance Service.
Scott, S., O’Connor, T. G., Futh, A., Matias, C., Price, J., & Doolan, M. (2010). Impact of a parenting program in a high-risk, multi-ethnic community: The PALS trial. Journal of Child Psychology and Psychiatry, 51, 1331–1341.
Watt, B. D., Hoyland, M., Best, D., & Dadds, M. R. (2007). Treatment participation among children with conduct Problems and the role of telephone reminders. Journal of Child and Family Studies, 16, 522–530.
Werba, B., Eyberg, S. M., Boggs, S. R., & Algina, J. (2006). Predicting the outcome of parent–child interaction therapy: Success and Attrition. Behavior Modification, 30, 618–646.
Author information
Authors and Affiliations
Corresponding author
Appendix: Factors of Parent Views of Intervention Questionnaire and Corresponding Items
Appendix: Factors of Parent Views of Intervention Questionnaire and Corresponding Items
Component 1: Parent Motivation and Parent-Focused Expectancies (10 items)
-
1.
My child’s behavior has to improve soon.
-
2.
I am willing to work on changing my own behavior as it related to managing my child.
-
3.
It is very important for the well-being of my family that my child changes his or her behavior.
-
4.
Although the main problem is my child’s behavior, I believe I should be involved in making positive change.
-
5.
I am willing to change my current parenting techniques and try new ones.
-
6.
My child will experience many negative things in life if his or her behavior does not change.
-
7.
I believe that changing my own behavior can cause my child’s behavior to change.
-
8.
I look forward to learning new techniques for managing my child’s behavior and helping his or her development.
-
9.
It is important for me to learn how to be a better parent.
-
10.
Learning to be a better parent should be a major focus of the program.
Component 2: Anticipated Barriers and Obstacles (8 items)
-
1.
It will be hard to find transportation.
-
2.
I will likely have scheduling problems due to other events or activities.
-
3.
I have too many things to do and this will interfere with my participating in this program.
-
4.
The program seems too long.
-
5.
The focus of the program seems of no use for my cultural or ethnic group.
-
6.
I have too much stress in my life making it hard to do anything extra like Early Risers.
-
7.
I do not like sharing my personal life with others.
-
8.
The parent-focused part of the program does not seem interesting or necessary for me.
Component 3: Child-Focused Expectations (5 items)
-
1.
This program should focus on children, not parents.
-
2.
The most important thing is that someone is working with my child.
-
3.
In Early Risers, I want my child to work on academic schoolwork, more than social skills or behavior.
-
4.
In Early Risers, I want my child to work on social skills, more than academic schoolwork or behavior.
-
5.
In Early Risers, I want my child to work on behavior, more than academic schoolwork or social skills.
Rights and permissions
About this article
Cite this article
Bloomquist, M.L., August, G.J., Lee, S.S. et al. Parent Participation Within Community Center or In-Home Outreach Delivery Models of the Early Risers Conduct Problems Prevention Program. J Child Fam Stud 21, 368–383 (2012). https://doi.org/10.1007/s10826-011-9488-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-011-9488-6