
Abstract
Chromium(III) is long regarded as essential trace element but the biochemical function and even basic transport ways in the body are still unclear. For a more rational discussion on beneficial as well as toxic effects of Cr(III), we re-investigated the bioavailability of the most important oral Cr supplements by using radiolabeled compounds and whole-body-counting in rats and in the first time also in humans. The apparent absorption of 51Cr(III) from Cr-picolinate, Cr-nicotinate, Cr-phenylalaninate, Cr-proprionate, or Cr-chloride was generally low (0.04–0.24 %) in rats with slightly higher values for Cr-chloride and -phenylalaninate. Taking a fast urine excretion into account, the true absorption of 51Cr was clearly higher for CrPic3 (0.99 %), probably indicating a different uptake mechanism of this rather stable organic Cr complex. The bioavailability of CrPic3 and Cr(d-Phen)3, the leading compounds in actual investigations, was analysed also in human volunteer by intraindividual comparison. The apparent absorption (=Cr bioavailability) of 51Cr from both compounds was substantially higher in humans (0.8–1 %) than in rats. Again, most of freshly absorbed CrPic3 was excreted into the urine resulting in the same low whole-body retention after 7 days for both compounds. In summary, the bioavailability of Cr from pharmaceutical Cr compound is lower than hitherto assumed. Importantly, humans absorb Cr(III) clearly better than rats. The absorption mechanism of CrPic3 seems to be different from ionic Cr(III) but, as only the same low amount of Cr is retained from this compound, it is also not more bioavailable than other Cr compounds.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Previous research has suggested that chromium in its trivalent form (Cr3+) is involved in the regulation of carbohydrate, lipid, and protein metabolism via an enhancement of insulin action (Schwarz and Mertz 1957; Mertz 1969; Cefalu and Hu 2004; Jeejeebhoy et al. 1977; Vincent 2000; Nair et al. 2008). This function could be of general interest because diabetes mellitus is an increasing health concern in many countries (Zimmet et al. 2001). Insulin resistance, an impaired biological response to normal or elevated serum insulin concentration, appears to be an early step in transforming normal glucose metabolism into diabetes. There is an important need for the development of new antihyperglycemic agents to improve insulin sensitivity and provide long-term benefit in the management of diabetes mellitus (Broadhurst and Domenico 2006).
Since the early work of Schwarz and Mertz (1957), Cr3+ is regarded as an essential nutrient for humans that potentiate the action of insulin in glucose uptake. An oligopeptide, Chromodulin, isolated from various liver tissues, is believed to function as part of a unique autoamplification mechanism for insulin signaling (Davis et al. 1997; Hatfield et al. 2006). After calcium and before iron, chromium is second in mineral supplements in US. 2.2 % of adults from the National Health and Nutrition Examination Survey 1999–2000 were taking supplements containing chromium, reflecting the US dietary supplement industry with a business market of 20.3-billion $ in 2005 (Radimer et al. 2004).
However, despite the many publications on chromium as a physiologic or therapeutic factor, many questions are open and it is even not clear whether Cr is an essential trace element or not. Some practical issues hinder the advancement in this field, for example the low intestinal absorption of chromium and the very low (nM) concentrations in body fluids and tissues which make the analytical determinations arduous to perform against the background of ubiquitous Cr. Since dietary chromium is poorly absorbed, there has been a surge of interest in the use of more bioavailable formulations. Picolinic acid, a natural derivative of the amino acid tryptophan, is thought to facilitate chromium absorption (Evans 1982a). The bioavailability of CrPic3 is reported to be higher (2–5 %) compared to all other chromium compounds in rats and humans and this has been the leading argument in the marketing of this product (Evans 1982b). However, as the picolinic moiety may raise also some toxic questions (Vincent 2003), also other Cr compounds are favoured at the moment in animal and human studies such as Cr-nicotinate, Cr-d-phenylalaninate, or Cr-proprionate (Olin et al. 1996; Lau et al. 2007; Dong et al. 2007; Dong et al. 2008; Clodfelder et al. 2005; Stanieka and Krejpcioa 2009).
Regarding the widespread use of various chromium compounds in humans, there are surprisingly little experimental data available concerning the pharmacokinetic of these drugs. The aim of the present study was therefore to compare the bioavailability of chromium from different Cr supplements in rats and for the first time also in humans using 51Cr-labelled compounds and whole body counting which together allows a comprehensive and quantitative characterisation of chromium absorption in comparison. Preliminary results with CrPic3 in a small group of rats were already published (Kottwitz et al. 2009).
Methods
51Cr-compounds
A solution of 51CrCl3, typical specific activity, 846 mCi/mg in 0.5 M HCl, was purchased from PerkinElmer Life and Analytical Sciences, Boston, USA. The 5 mCi-51Cr-activity of one delivered plastic flask was diluted with 500 μl of water.
Synthesis of 51Cr(trispicolinate)
51CrPic3·H2O was synthesized in a modified version according to Evans and Pouchnick (1993). Into a centrifugal filter device (Ultrafree-MC, 10.000 NMWL filter unit, low binding regenerated cellulose, Millipore) were pipetted 50 μl of an aqueous solution of picolinic acid (0.114 mM) and 240 μl of the diluted 51CrCl3-tracer solution. After mixing, 50 μl of an aqueous solution of CrCl3 (37 μM) were added and stirred. The mixture was incubated at 50 °C over night. After centrifugation at 5,000×g for 20 min, the reddish crystals remaining on the filter membrane were washed 3 times with 50 μl of ice-cold water. For the rat experiments, saturated aqueous solutions of 51CrPic3 (0.6 mM) were freshly prepared by adding 400 μl of water to the filter unit, incubation at 50 °C for 30 min, followed by centrifugation at 5,000×g for 20 min.
Synthesis of 51Cr-nicotinate
Into a centrifugal filter device (Ultrafree-MC, 10.000 NMWL filter unit, low binding regenerated cellulose, Millipore) were dissolved 14 mg of nicotinic acid in 50 μl 0.1 mM NaOH. 240 μl of the diluted 51CrCl3-tracer and 40 μMol CrCl3 (=10 mg) in 50 μl of H2O were added. The tube was heated in a block thermostat at 57 °C over night. After centrifugation at room temperature at 5,000×g for 20 min, the blue-gray solid on the filter membrane was washed 3 times with 100 μl of ice-cold water.
Synthesis of 51Cr-(d(or l)-phenylalaninate)3
(Modified procedure according to Yang et al. 2005). 10 mg (38 μmol) CrCl3·6H2O were dissolved in 200 μl of water in a 1.5 ml Eppendorf tubes. A 200 aliquot of a 51CrCl3-tracer solution (74 MBq) was added. 18.5 mg (=112 μMol) l or d-phenylalanine (M = 165.19 g/mol), respectively, was weighted in another Eppendorf tube and dissolved in 200 μl of water by heating to 80 °C in a thermo block. The 51CrCl3-solution was added and the mixture remained heated for 4 h. After freeze-drying, the green-violet solid obtained was washed with 2 × 400 μl of acetone. UV-spectroscopy in water showed identical absorption curves of both substances with peaks at 416 and 568 nm.
Radiochemical purity
The radiochemical purity of the synthesized 51Cr-compounds was tested by reverse phase HPLC (column Nucleosil C18 5U; eluent water/methanol, UV detection at 262 nM) using a method described by Olin et al. (1996). Following injection of CrPic3, the 51Cr-activity, found in peak at 4.14 min retention time, accounted for 95 % of the injected 51Cr-activity (Fig. 1). From all other radiolabel chromium compounds, including Cr-Nic2, the 51Cr activity was found outside detectable peaks or was tightly bound to the column material and could eluated by a EDTA-buffer. This indicated that these more labile Cr-complexes disintegrated under the experimental conditions.

HPLC chromatogram of 51Cr-picolinate. 95 % of the 51Cr activity was found in the main peak at 4.14 min retention time
Animal experiments
All experiments were approved by the local committee for animal experiments (37/04 and 21/08). Female Wistar rats (200–300 g, Charles River Germany), kept on a standard food in pellet diet (Altromin 1328) were used for all experiments. Rats had free access to tap water ad libitum.
The rats were fasted 4–6 h before and 1 h after the respective administration of labelled 51Cr-compounds. Aqueous solutions were administered by gastric intubation, intraperitoneal or intravenous (tail vein) injections. After administration, rats were kept in cages of 3–4 rats except some experiments in which some rats were kept in individual metabolic cages over 2 days for a quantitative collection of urine and faeces. The activity, measured immediately after administration of 51Cr, in the whole body was taken as the 100 % reference value. The 51Cr whole body retention were measured at given time points in the centre of a 200 cm long 4π-geometry whole body radioactivity detector with liquid organic scintillator in the energy range from 980 to 3,000 keV (Braunsfurth et al. 1977). The biological half-life of 51Cr was calculated from a triple term exponential fit algorithm to the measured whole body retention of 51Cr values in a period of 1–100 days after the administration of 51Cr. The rats were sacrificed by exsanguination from the abdominal aorta while under narcosis with Ketanest/Rompun. 51Cr activity in the excrements and tissues of rats was measured in the whole body counter or for longer sensitivity in a 3″ × 3″ NaJ detector (autogamma 5260, Canberra-Packard, Frankfurt, Germany.
Human studies
In a pilot study, CrPic3 and 4 weeks later Cr(d-Phen)3 (400 μg Cr with 16 and 11 μCi 51Cr-activity) were administered orally as aqueous solution (100 ml) in three male volunteers (three of the authors, subject 1, 58 years, 87 kg, subject 2, 65 years, 65 kg, subject 3, 56 years, 91 kg). The retained 51Cr activities were measured after 7 days in the whole-body counter. Urine was collected quantitatively for 48 h and the 51Cr activities were measured in the whole body counter. The additional radiation burden from orally administered 51Cr (50 years equivalent dose) was between 0.01 and 0.02 mSv, which reflects <1 % of the natural radiation burden of 2.4 mSv/year of a subject in Germany.
Data analysis
The mean 51Cr retention data R(t) from the whole-body counting were fitted by a compartment model with the condition A1 + A2 + A3 = 100 % for the 3 compartments (Eq. 1).
As start values for the fit software (Slide Write Plus 7.0, Advanced Graphics Software Inc., Encinitas, USA), the data of Mertz et al. (1965) for the retention of 51CrCl3 in rats were used. For the long-term half-life, only a lower and upper threshold could be fitted within the limited observation period. The lower threshold for the long half-life was found from a 2-compartment fit, while the upper threshold of T 31/2 results from a 3-term fit with fixed parameters T 11/2 and T 21/2 from the 2-term fit and 5.9 days, respectively. With this upper threshold for T 31/2 , the final 3-compartment fit resulted in the 3 pool sizes and their half-lives of 51Cr-retention (Table 2).
For comparison of whole-body-retention data between groups of rats, the Student t test was used. Differences between their mean values were regarded as significant at p < 0.05.
Results
A variety of Cr(III) compounds were labelled with 51Cr and their basic pharmacokinetic parameters were studied in rats after oral and parenteral application. The bioavailability of CrPic3 and Cr(d-Phen)3, as the most relevant preparations used in nutritional supplements, were measured and compared also in human volunteers. After oral administration of 51Cr-labelled Cr-compounds, the whole-body-retention 7 days after administration was generally low between 0.04 and 0.24 % of the dose (Fig. 2).

51Cr whole body retention 7 days after oral application after different chromium compounds in rats (6–12 μg Cr/rat) (=apparent absorption of 51Cr). Box-whisker-Plots with mean values
This parameter reflects the apparent intestinal absorption and the storage of chromium in tissue and organs and could also be a reasonable measure of the bioavailability of chromium from a given drug. In detail, the comparison between different Cr compounds did show some differences. The rather ionic and water soluble compounds such as Cr-d/l-(Phen)3 and CrCl3 were significantly better absorbed and retained than the more organic, poorly soluble complexes, such as CrPic3, CrNic2, and CrProp, which all showed very low values. However, it should be pointed out that the true intestinal Cr absorption of most Cr-compounds was remarkably different from the retention values due to a substantial and fast urine excretion of freshly absorbed 51Cr. This effect is most relevant for 51CrPic3 because most of the absorbed Cr was excreted directly into the urine within the first two days after administration (Table 1).
As the amount of absorbed 51Cr was very low from all compounds under study, precise long-term measurements of retained 51Cr was only possible after i.p. or i.v. injection. However, no fundamental differences in the biodistribution of Cr(III) were found so far in earlier studies. In keeping with this view, the range of compound specific urine excretion seen after oral application was found also after i.p. injection (Table 1). In addition, also a substantial faecal excretion occurs which is low after CrCl3 and higher following CrPhen3 application.
In the dose range from 0.01 to 5 μg Cr/rat, there was found no dose effect on the whole-body-retention after i.v. administration (data not shown).
Following the 51Cr-whole-body-retention for up to 7 weeks, almost identical retention curves were obtained for all chromium compounds under study, again except for CrPic3 (Fig. 3). For this drug, a fast drop of the whole body retention occurs due to the excretion of 51Cr by the kidney. For all compounds, the respective retention data fitted well to a three-compartment model (Fig. 3; Table 2).

51Cr-whole-body retention from 51CrPic3 as well as other chromium compounds in rats after i.p. injection. The respective half-lives were calculated from a 3-compartment model
The three compartments are described by different pool sizes (A1–A3), the whole body retention curve follows three different half-lives in the range of minutes to hours (T 11/2 ), 5 days (T 2)1/2 , and a long half-live of 100 days which can only be estimated from the retention data (T 31/2 ) (Table 2). The striking difference is the pool size for a central compartment (A1) representing presumably the blood volume. Only for CrPic3, this pool size is close to 100 %, indicating that in a short period after injection the entire compound is present in this pool.
However, despite the different urinary excretion rate, the long-term distribution of 51Cr into organs from different compounds was similar from three different Cr compounds, including CrPic3. After 7 days, most of the 51Cr activities were found in liver, kidney and bone. The bone values in Fig. 4 represent the 51Cr activity in a single femur indicating that the high activity in carcass mainly expresses a large storage pool in bone.

51Cr organ distribution from different Cr compounds 7 days after i.p. injection. GIT gastrointestinal tract. Mean ± SD values of 3 rats
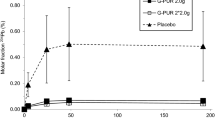
The intestinal absorption and urine excretion of 51Cr following oral administration of CrPic3 and Cr(d-Phen)3, the most promising compounds used in many studies, were tested also in three human volunteers at a dose of 400 μg Cr. Overall, the 7 days-whole-body-retention of Cr was significantly higher in humans than in rats (CrPic3: 0.75 ± 0.04 %; Cr(d-Phen)3: 0.95 ± 0.13 %), but with no significant differences between both compounds (p < 0.064). However, a clear difference was found in the urine excretion (3.4 ± 0.85 % vs. 0.33 ± 0.06 %), which goes parallel to the situation in rats. Most of the absorbed Cr from CrPic3 was excreted directly into the urine within 48 h after application (Fig. 5).

7 days whole-body retention (WBR) and 2 days urine excretion of 51Cr after oral application of 400 μg Cr in form of CrPic3 or Cr(d-Phen)3 in three male volunteers
Discussion
In the present study the most relevant chromium compounds used for nutritional supplements were labeled with 51Cr and their absorption, retention, excretion and tissue distribution were compared in rats and for the first time also in humans. 51Cr-chromium chloride was used as reference because this is the only compound for which pharmacokinetic data have already been measured in earlier studies by Mertz and others using the same analytical techniques, in particular, 51Cr-whole-body-counting (Mertz et al. 1965; Onkelinx 1977). This technique is rarely used today because it needs special equipment which is no longer available in most scientific centers. However, it remains by far the most reliable technique to measure the bioavailability of a trace element such as chromium for which an appropriate isotope is available. All other techniques (e.g., measuring post absorptive Cr concentration in blood or urine samples) are less sensitive, hard to quantify, and always face the problem with high background Cr in tissues and body fluids.
As judged by the 7 days-whole body retention (7d-WBR), the apparent absorption of Cr from all chromium compounds was found to be very low in rats between 0.04 and 0.24 % from the administered dose. These values are 2–10 times lower than described earlier (Anderson et al. 1996). The 7d-WBR represents also a good measure for the bioavailability of a given chromium compound. “Bioavailability”, in its pharmacological meaning, denotes the extent to which a substance is reaching its site of action in the body by way of systemic circulation. For chromium, the believed site of action is the insulin receptor on the cell surface of insulin dependent cells, e.g., in fat and muscle tissue. It is therefore unlikely that the fraction of absorbed but directly excreted Cr can have metabolic function in vivo. Following this argumentation, the true absorption (7d-WBR plus urine and feces excretion) overestimates the bioavailability of chromium. As a consequence, rather simple and cheap compounds such as CrCl3 do provide the same or even higher amounts of Cr than CrPic3 or CrNic2, the two marked leader in chromium supplementation.
This view is in contrast to the literature, because so far a high urine excretion is thought to be an offset by increases in chromium absorption (Rhodes et al. 2010). Especially, the high urinary excretion of Cr from CrPic3 was an argument for an assumed improved bioavailability. In humans, a higher excretion of Cr in urine was noted after supplementation with CrPic3 in volunteers (Clancy et al. 1994). A model calculation even predicted that Cr3+ from oral CrPic3 can accumulate in human tissue (Stearns et al. 1995). More recently, a comparison of acute absorption of commercially available chromium supplements was made in volunteers by following the 24 h urinary excretion of chromium after 200 μg Cr dosage DiSilvestro and Dy (2007). CrPic3 always showed the highest urine excretion reinforcing the concept that CrPic3 is absorbed best.
The whole body retention after oral, i.v., or i.p. application of chromium compounds in rats showed a typical tri-phasic curve for all compounds under study reflecting three different transport and storage compartments in the body (Fig. 3). This has been shown earlier so far only for CrCl3 in rats as well as in humans (Mertz et al. 1965; Onkelinx 1977; Doisy et al. 1971; Sargent et al. 1979). The retention curves were very similar to that for all other Cr-compounds, except CrPic3. Most of the absorbed or injected 51Cr from CrPic3 is found in urine and feces within 48 h after application (Table 1). It can be speculated that poorly water-soluble CrPic3-complex is bound to a lesser degree to plasma proteins compared to free Cr3+. It is well known that the iron transport protein transferrin does bind Cr3+ in vitro, like it binds many other metal ions, and is always assumed that transferrin is also the physiological transporter for Cr3+ (Vincent 2000; Sun et al. 2000). The best evident so far has been described by (Clodfelder and Vincent 2005) by i.v. injecting 51Cr-labeled transferrin into mice with or without co-injection of insulin. A rapid and insulin-sensitive movement from blood into tissue and finally into urine (80 % in 3 h was found). However, using a proteomic approach it was shown that Cr(III)Cl3 in culture cell media containing 5 % human serum do form complexes not only with transferrin but also with albumin and immunoglobulins, in the case of bovine serum in media only with albumin (Tkaczyk et al. 2010). At the moment, it must simply be pointed out that transferrin as the natural chromium transporter in blood has so far not definitely been proven in vivo. One could even argue that it seems unlikely that large amounts of unsaturated transferrin with its strong binding affinity for metals (Cr, effective binding constant = 3 × 1015 M−2 (Sun et al. 2000) circulating in blood would allow such a substantial Cr3+ loss into the urine as found again in this study.
The mechanism of Cr absorption is also not well understood. Cr is thought to be absorbed in the intestinal mucosa. Administered chromium compounds could be hydrolyzed at the acid pH in the stomach forming the hexa-aquo-ion [Cr(H2O)6]3+(aq) which reacts with OH-ions in the intestine to form rather insoluble Cr-hydroxide-oxides at neutral pH. However, it can only be speculated which chromium species is preferentially absorbed in the intestinal tract. For the case of manganese it is quite well known that Mn3+/2+ and Fe3+/2+ compete for the same transport system in blood (transferrin) and cellular metal importer (DMT1, divalent metal transporter 1 for example in enterocytes). All identified Nramp proteins such as DMT1 are thereby strictly limited to divalent metal ions, making a reduction Me3+ → Me2+ necessary. For chromium, chromium(II), “chromous” ions (Cr2+) are possible but are extremely instable and it is questionable if they can exists in biological systems and can act as substrates for DMT1. Interestingly, with Nrat1 a first transporter for a trivalent metal (aluminum) was found in plants but nothing is known on its Cr3+ transporting activity. Several authors believe that the absorption of trivalent chromium is a passive diffusion process, which cannot be saturated (Donaldson and Barreras 1966; Dowling et al. 1989). Dosing a wide range of Cr concentrations (0.02–20 μg/rat) in form of CrCl3 by gastric-gavage, we recently also found no saturation effect (Kottwitz et al. 2009) on Cr absorption.
Concerning the rather hydrophobic CrPic3, it has been discussed earlier that it may be absorbed as intact molecule by a different absorption mechanism that ionic Cr3+ Gammelgaard et al. (1999); Hepburn and Vincent (2002). A relevant point could be that Cr(Pic)3 represents a relative stable organic complex which is poorly water soluble. This stability could be demonstrated in our study to test the radiochemical purity in HPLC on a reverse phase column (Fig. 1). All other complexes, including Cr-nicotinate and Cr-(d,l-Phen)3 did not survive the HPLC condition as intact molecule what must have been overlooked in earlier HPLC results for example for CrNi2 (Olin et al. 1996). On the other hand, a recent review favored the view that little of the intact Cr(Pic)3 molecule is absorbed in the intestinal tract (Vincent 2010). This was based on experiments with CrPic3, in which the picolinic moiety was 14C-labeled (NIH Publication No. 08-5897 2008). Oral administration of a rather high dosage (15–17 mg/kg = 600 ug Cr/rat) in rats resulted in a high urinary excretion of Cr-free 14C activity (>50 % within 24 h), indicating that most of the picolinic acid moiety must have been absorbed independently from chromium. However, according to these data about 1 % of intact CrPic3 was isolated from the 8 h-urine samples what perfectly fits with the experiments described here. This would, however, demonstrate that the reason of the increased absorption rate of CrPic3 compared to ionic Cr is due to the absorption of the intact molecule. What remains unclear is if the retained Cr from Cr(Pic)3 is derived from absorbed CrPic3 or is obtained from the absorption of free Cr3+ which was released from the complex at low pH in the stomach. Our experiments show that a similar ratio between retained and excreted Cr is found after i.p., i.v. or oral application what could indicate that both fractions could be derived from intact CrPic3 entering the metabolic active compartments of the body. However, a final proof could only be derived from the use of double labeled 51Cr(14C-Pic)3.
As the chromium metabolism in rats could be different to humans, we studied the oral chromium absorption from 51CrPic3 and 51Cr-(d-Phen)3 also in three human volunteers (Fig. 5). The apparent absorption of CrPic3 and Cr(d-Phen)3 was substantially higher (0.7–0.9 %) compared to rats, but also much lower (3–5 times) than so far recognized (Clancy et al. 1994; Gargas et al. 1995). Despite the absolute values, for both compounds the profile of absorption, urine excretion and retention seems to similar in rats and humans, an argument that the results from the other compounds in rats are representative also for the human situation. Our results explains the rather high urine excretion in studies with CrPic3 in humans and can be used for a better calculation of the effect of chromium but also for the widespread discussion on the potential toxic effect of CrPic3 in vivo.
Conclusions
Despite more than 50 years of research, the reputation of chromium as an essential trace element or antidiabetic drug is ambiguous at the moment (42). Studies in this field using different compounds, dosages, and biological system are hard to compare, results are often controversy and conflicting. Meta-analysis and official reports are thus more and more sceptical towards a role of Cr in evidence based medicine (Trumbo and Ellwood 2006; National Research Council 2002). On the other hand, very recent studies in patients, cell culture or animal models seem to show medical benefit or clear cellular effects or Cr (Phung et al. 2010; Dogukan et al. 2010; Jain et al. 2010; Wang et al. 2010; Tuzcu et al. 2011; Li et al. 2011). Chromium will have a future as an accepted essential trace element or as a medicament only if studies clarify definitely the mechanisms of chromium action on the molecular level. A prerequisite for carefully designed studies in the future would also be that the pharmacokinetics of Cr compounds must be known in full detail in order to provide appropriate and comparable preparations and dosages.
References
Anderson RA, Bryden NA, Polansky MM, Gautschi K (1996) Dietary chromium effects on tissue chromium concentrations and chromium absorption in rats. J Trace Elem Exp Med 9:11–25
Braunsfurth JS, Gabbe EE, Heinrich HC (1977) Performance parameters of the Hamburg 4π whole body radioactivity detector. Phys Med Biol 22:1–17
Broadhurst CL, Domenico P (2006) Clinical studies on chromium picolinate supplementation in diabetes mellitus-a review. Diabetes Technol Ther 8:677–687
Cefalu WT, Hu FB (2004) Role of chromium in human health and in diabetes. Diabetes Care 27:2741–2751
Clancy SP, Clarkson PM, DeCheke ME, Nosaka K, Freedson PS, Cunningham JJ, Valentine B (1994) Effects of chromium picolinate supplementation on body composition, strength, and urinary chromium loss in football players. Int J Sport Nutr 4:142–153
Clodfelder BJ, Vincent JB (2005) The time-dependent transport of chromium in adult rats from the bloodstream to the urine. J Biol Inorg Chem 10:383–393
Clodfelder BJ, Gullick BM, Lukaski HC, Neggers Y, Vincent JB (2005) Oral administration of the biomimetic [Cr3O(O2CCH2CH3)6(H2O)3]+ increases insulin sensitivity and improves blood plasma variables in healthy and type 2 diabetic rats. J Biol Inorg Chem 10:119–130
Davis CM, Royer AC, Vincent JB (1997) Synthetic multinuclear chromium assembly activates insulin receptor kinase activity: functional model for low-molecular-weight chromium-binding substance. Inorg Chem 36:5316–5320
DiSilvestro RA, Dy E (2007) Comparison of acute absorption of commercially available chromium supplements in humans. J Trace Elem Exp Med 21:274–275
Dogukan A, Tuzcu M, Juturu V, Cikim G, Ozercan I, Komorowski J, Sahin K (2010) Effects of chromium histidinate on renal function, oxidative stress, and heat-shock proteins in fat-fed and streptozotocin-treated rats. J Ren Nutr 20(2):112–120
Doisy RJ, Streeten DHP, Souma ML, Kalafer ME, Rekant SL, Dalakos TG (1971) Metabolism of 51chromium in human subjects. In: Mertz W, Cornatzer WE (eds) Newer trace elements in nutrition. Dekker, New York, pp 155–168
Donaldson RM, Barreras RF (1966) Intestinal absorption of trace quantities of chromium. J Lab Clin Med 68:484–493
Dong F, Xiaoping MR, Nair S, Ren J (2007) Chromium (d-phenylalanine)3 improves obesity-induced cardiac contractile defect in ob/ob mice. Obesity 15:2699–2711
Dong F, Kandadi MR, Ren R, Sreejayan N (2008) Chromium (d-phenylalanine)3 supplementation alters glucose disposal, insulin signaling, and glucose transporter-4 membrane translocation in insulin-resistant mice. J Nutr 138:1846–1851
Dowling HJ, Offenbacher EG, Pi-Sunyer FX (1989) Absorption of inorganic, trivalent chromium from the vascularly perfused rat small intestine. J Nutr 119:1138–1145
Evans GW (1982a) The role of picolinic acid in metal metabolism. Life Chem Rep 1:57–67
Evans GW (1982b) Dietary supplementation with essential metal picolinates. US Patent 4,315,927, 1982
Evans GW, Pouchnick DJ (1993) Composition and biological activity of chromium-pyridine carboxylate complexes. J Inorg Biochem 49:177–187
Gammelgaard B, Jensen K, Steffansen BJ (1999) In vitro metabolism and permeation studies in rat jejunum: organic chromium compared to inorganic chromium. J Trace Elem Med Biol 13:82–88
Gargas ML, Norton RL, Paustenbach DJ, Finley BL (1995) Urinary excretion of chromium by humans following ingestion of chromium picolinate. Implications for biomonitoring. Drug Metab Dispos 23:607–609
Hatfield MJ, Gillespie S, Chen Y, Li Z, Cassady CJ, Vincent JB (2006) Low-molecular-weight chromium-binding substance from chicken liver and American alligator liver. Comp Biochem Physiol 144:423–431
Hepburn DD, Vincent JB (2002) In vivo distribution of chromium picolinate in rats and implications for the safety of the dietary supplement. Chem Res Toxicol 15:93–100
Jain SK, Croad JL, Velusamy T, Rains JL, Bull R (2010) Chromium dinicocysteinate supplementation can lower blood glucose, CRP, MCP-1, ICAM-1, creatinine, apparently mediated by elevated blood vitamin C and adiponectin and inhibition of NFkappaB, Akt, and Glut-2 in livers of zucker diabetic fatty rats. Mol Nutr Food Res 54(9):1371–1380
Jeejeebhoy KN, Chu RC, Marliss EB, Greenberg GR, Bruce-Robertson A (1977) Chromium deficiency, glucose intolerance, and neuropathy reversed by chromium supplementation, in a patient receiving long-term total parenteral nutrition. Am J Clin Nutr 30:531–538
Kottwitz K, Laschinsky N, Fischer R, Nielsen P (2009) Absorption, excretion and retention of 51Cr from labelled Cr-(III)-picolinate in rats. Biometals 22:289–295
Lau FC, Bagchi M, Bagchi D (2007) Letter to the editor: comparison of acute absorption of chromium(III) supplements. J Trace Elem Med Biol 21:274–276
Li F, Wu X, Zhao T, Zhang M, Zhao J, Mao G, Yang L (2011) Anti-diabetic properties of chromium citrate complex in alloxan-induced diabetic rats. J Trace Elem Med Biol 25(4):218–224
Mertz W (1969) Chromium occurrence and function in biological systems. Physiol Rev 49:163–239
Mertz W, Roginski EE, Reba RC (1965) Biological activity and fate of trace quantities of intravenous chromium(III) in the rat. Am J Physiol 209:489–494
National Research Council (2002) Dietary reference intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc. A Report of the Panel on Micronutrients, Subcommittees on Upper Reference Levels of Nutrients and of Interpretation and Uses of Dietary Reference Intakes, and the Standing Committee on the Scientific Evaluation of Dietary Reference Intakes Food and Nutrition Board Institute of Medicine. National Academy Press, Washington
NIH Publication No. 08-5897 (2008) NTP technical report on the toxicology and carcinogenesis. Studies of chromium picolinate monohydrate (CAS NO. 27882-76-4) in F344/N rats and B6C3F1 mice Scheduled Peer Review Date: February 27–28
Olin KL, Stearns DM, Armstrong WH, Keen CL (1996) Comparative retention/absorption of 51chromium from 51Cr chloride, 51Cr nicotinate and 51Cr picolinate in a rat model. Trace Elem Electrolytes 11:182–186
Onkelinx C (1977) Compartment analysis of metabolism of chromium(III) in rats of various ages. Am J Physiol 232(5):E478–E484
Phung OJ, Quercia RA, Keating K, Baker WL, Bell JL, White CM, Coleman CI (2010) Improved glucose control associated with i.v. chromium administration in two patients receiving enteral nutrition. Am J Health Syst Pharm 67(7):535–541
Radimer K, Bindewald B, Hughes J, Ervin B, Swanson C, Picciano MF (2004) Dietary supplement use by US adults: data from the national health and nutrition examination survey, 1999–2000. Am J Epidemiol 160:339–349
Rhodes NR, McAdory D, Love S, Di Bona KR, Chen Y, Ansorge K, Hira J, Kern J, Kent J, Lara P, Rasco JF, Vincent JB (2010) Urinary chromium loss associated with diabetes is offset by increases in absorption. J Inorg Biochem 104:790–797
Sargent T, Lim TH, Jenson RL (1979) Reduced chromium retention in patients with hemochromatosis, a possible basis of hemochromatotic diabetes. Metabolism 28:70–79
Schwarz K, Mertz W (1957) A glucose tolerance factor and its differentiation from factor 3. Arch Biochem Biophys 72(2):515–518
Sreejayan N, Dong F, Kandadi MR, Yang X, Ren J (2008) Chromium alleviates glucose intolerance, insulin resistance, and hepatic er stress in obese mice. Obesity 16:1331–1337
Stanieka H, Krejpcioa Z (2009) The effects of tricentric chromium(III) propionate complex supplementation on pregnancy outcome and maternal and foetal mineral status in rat. Food Chem Toxicol 47:2673–2678
Stearns DM, Belbruno JJ, Wetterhahn KE (1995) A prediction of chromium(III) accumulation in humans from chromium dietary supplements. FASEB J 9:1650–1657
Sun Y, Ramirez J, Woski SA, Vincent JR (2000) The binding of trivalent chromium to low-molecular-weight chromium-binding substance (LMWCr) and the transfer of chromium from transferrin and chromium picolinate to LMWCr. J Biol Inorg Chem 5:129–136
Tkaczyk C, Huk OL, Mwale F, Antoniou J, Zukor DJ, Petit A, Tabrizian M (2010) Investigation of the binding of Cr(III) complexes to bovine and human serum proteins: a proteomic approach. J Biomed Mater Res A 94:214–222
Trumbo PR, Ellwood KC (2006) Chromium picolinate intake and risk in type 2 diabetes: an evidence-based review by the United States food and drug administration. Nutr Rev 64:357–363
Tuzcu M, Sahin N, Orhan C, Agca CA, Akdemir F, Tuzcu Z, Komorowski J, Sahin K (2011) Impact of chromium histidinate on high fat diet induced obesity in rats. Nutr Metab 8:28. doi:10.1186/1743-7075-8-28
Vincent J (2000) The biochemistry of chromium. J Nutr 130:715–718
Vincent JB (2003) The potential value and toxicity of chromium picolinate as a nutritional supplement, weight loss agent and muscle development agent. Sports Med 33(3):213–230
Vincent JB (2010) Chromium: celebrating 50 years as an essential element? Dalton Trans 39:3787–3794
Wang Y, vanOort MM, Yao M, van der Horst DJ, Rodenburg KW (2010) Insulin and chromium picolinat induce translocation of CD36 to plasma membrane trough different signiling pathways in 3T3-L1 adipocytes and with differential functionality of the CD36. Biol Trace Elem Res. doi:10.1007/s12011-010-8809-8
Yang X, Palanichamy K, Ontko AC, Rao MN, Fang CX, Ren J, Sreejayan N (2005) A newly synthetic chromium complex-chromium(phenylalanine)3 improves insulin responsiveness and reduces whole body glucose tolerance. FEBS Lett 579:1458–1464
Zimmet P, Alberti KG, Shaw J (2001) Global and societal implications of the diabetes epidemic. Nature 414:782–787
Acknowledgments
The technical assistance of Angelika Schmidt is grateful acknowledged. Parts of the data are including in the medical thesis of N.L., N.F., and G.C. at the University Hamburg, Germany. N.L., K.K., P.N. designed research; N.L., K.K., B.F., B.D., P.N. conducted research; R.F. analyzed data; B.F. and P.N. wrote the paper; all authors read and approved the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Laschinsky, N., Kottwitz, K., Freund, B. et al. Bioavailability of chromium(III)-supplements in rats and humans. Biometals 25, 1051–1060 (2012). https://doi.org/10.1007/s10534-012-9571-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10534-012-9571-5