
Abstract
While chromium was proposed to be an essential trace element over 40 years ago and if essential should possess a specific transport and distribution mechanism, the details of its transport from the bloodstream to the urine have not been elucidated. However, chromium is known to be maintained in the bloodstream bound to transferrin and to be excreted in the urine bound to the oligopeptide chromodulin or a similar chromodulin-like species. Injection of 51Cr-labeled transferrin into the bloodstream resulted in a rapid and insulin-sensitive movement of chromium into the tissues as Cr transferrin; greater than 50% of the Cr is transported to the tissues within 30 min. Tissue levels of Cr are maximal 30 min after injection; decreases in tissue Cr with time are mirrored by increases in urine Cr. Approximately 50% of the 51Cr appears in the urine within 360 min of injection in the absence of added insulin; insulin treatment concurrent with injection of 51Cr-labeled transferrin results in approximately 80% of the label appearing in the urine within 180 min. The removal of 51Cr from the blood is faster than the appearance of 51Cr in the urine; the lag in time indicates that the Cr transferrin in the blood and Cr in the urine are not in direct equilibrium and that intermediates in the transport of Cr must be involved. This establishes a clear pathway of transport of Cr starting from transport by transferrin from the bloodstream into the tissues, followed by release and processing in the tissues to form chromodulin, excretion into the bloodstream, rapid clearance of chromodulin or a similar species into the urine, and ultimately excretion as this species. Insulin stimulates the processing of Cr in the tissues.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In the last decade, major advances have been made towards understanding the transport and “trafficking” of transition metals in biological systems. The progress has been especially notable for iron [1], copper [2], zinc [3], and nickel [4], and recent reports on manganese [5] suggest that major advances in understanding this system are underway. However, work on chromium lags far behind. This is not surprising as its status as a trace nutrient and its potential role in insulin-dependent carbohydrate and lipid metabolism in mammals, while generally accepted, is actively debated [6–8].
Cr(III) is a component of the diet; Cr is absorbed and transported throughout the body, and ultimately eliminated in the urine and bile. Enough data exist to outline the movement of Cr through the body. Absorption of dietary Cr is very small, 0.5–2%, and is inversely proportional to the level of intake in humans [9]. In the bloodstream, Cr is bound primarily to the ferric iron transport protein transferrin. Greater than 99% of Cr in the blood when given by a stomach tube as CrCl3 to rats is associated with noncellular components. About 90% of Cr in the serum is associated with the β-globulin fractions, while 80% immunoprecipitates with transferrin [10]. A similar percentage of serum Cr is associated with transferrin after an intravenous injection of CrCl3 [11]. The similar charge and ionic radii of chromic and ferric ions suggests that chromic ions should bind relatively tightly to transferrin. In fact, Cr(III) readily binds to the two ferric ion-binding sites, resulting in intense changes to the protein’s UV spectrum [12–18]. The two binding sites can be distinguished by electron paramagnetic resonance spectroscopy, and only chromic ions at the C-lobe site can be displaced by Fe(III) at near-neutral pH [14, 15]. Below pH 6, only the N-lobe site binds Cr [16]. The binding constants for chromic ions at the two sites have been shown to differ by 5 orders of magnitude, consistent with this site-selective binding [19]. Despite these data, a major role for transferrin in the transport rather than the storage of Cr was not proposed until recently [20], although Dowling et al. [21] suggested in 1990 that transferrin is important for Cr transport from the intestines.
When rats are injected with 51Cr-labeled transferrin rather than given Cr orally or injected with 51CrCl3 to guarantee that all the radiolabel is initially associated with transferrin, the transferrin serves as a transport agent for Cr [22]. The labeled molecule can be followed from the bloodstream into tissues, notably the liver and kidney; however, only one time point (2 h after injection) has been examined. This migration of transferrin is insulin-sensitive; coadministration of insulin leads to an appreciable increase in Cr transport from the bloodstream to the tissues [22]. 51Cr is ultimately lost in the urine as part of a low molar mass complex, assigned as the oligopeptide chromodulin (vide infra) [22]; urinary Cr loss is stimulated by insulin.
The insulin-sensitivity of Cr transport by transferrin is potentially quite significant as this has been proposed to be related to chromium’s potential role in carbohydrate and lipid metabolism [7, 20]. Morris et al. [23] have shown that increases in blood insulin concentrations following an oral glucose load result in significant decreases in plasma Cr levels; a subsequent infusion of insulin in these human euglycemic hyperinsulinemic clamp studies led to further Cr losses. Within 60–90 min, blood Cr levels start to recover. Patients also displayed increased urinary Cr losses during the course of the experiments, with the amount of Cr lost approximately corresponding to the amount of Cr lost from the intravascular space [23]. Increased urinary Cr loss within 90 min of a dietary stress such as high sugar intake (which results in increased insulin release) has been demonstrated in several other studies [24–29]. Repeated application of carbohydrate stress results in a decrease in glucose tolerance and decreased mobilization and subsequent loss of Cr [26]. A role for transferrin in this insulin-sensitive Cr migration from the blood to tissues and ultimately to the urine is consistent with recent reports that indicate that recycling of transferrin receptors is insulin-sensitive; increases in insulin result in a stimulation of the movement of transferrin receptor (and glucose transporter GLUT-4) from vesicles to the plasma membrane [30].
In 1981 Wu and Wada [31] identified a low molar mass species in human and rat urine that bound Cr; the material appeared to be similar to a compound isolated from mammalian liver with an approximate molecular mass of 1,500 Da that they had previously given the name low molecular weight chromium-binding substance (LMWCr) (LWMCr has subsequently been renamed chromodulin [6]). Chromodulin was subsequently first isolated and purified from rabbit liver and found to be an oligopeptide composed of glutamate, aspartate, cysteine, and glycine and capable of binding 4 equivalents of chromic ions [32]. The compound has a large acute intraperitoneal LD50 value (134.9 mg/kg body mass), probably because of its rapid clearance in the urine (mean tubular reabsorption rate 23.5%) [33]. Chromodulin was found to occur in a variety of tissues, although the levels were greatest in liver of the tissues examined, and in blood plasma, in addition to the urine [34]. Several research groups have confirmed that Cr is excreted in the urine exclusively as a low molar mass species [11, 22, 35–38], including when Cr is administered intravenously as Cr transferrin [22, 36]. Wada et al. assumed on the basis of the similar apparent molecular weight of chromodulin and the low molar mass species from size-exclusion chromatography that these species were identical, an assumption, which has generally been followed by subsequent investigators. However, the species from urine has not been isolated and characterized to date. Hence, Wada and coworkers [31–34] and subsequent researchers [20, 22] have proposed that chromodulin carries chromic ions from tissues to the bloodstream and then ultimately into the urine for excretion from the body.
Thus, the basic mechanism behind the movement of Cr from the blood to tissues and then ultimately to the urine appears to have begun to be elucidated, although the movement of Cr from the bloodstream to the urine has not been examined in detail as a function of time. Herein are described studies designed to follow the form of bound Cr(III) in the blood, tissues, and urine as a function of time after the introduction of Cr transferrin into the bloodstream to test this proposed mechanism of Cr transfer.
Materials and methods
Transferrin and miscellaneous
51CrCl3 in 1.0 M HCl, rat transferrin, and rabbit antiserum to rat transferrin were obtained from ICN. A 51Cr2 transferrin was prepared as previously described [18]. In short, apotransferrin was prepared by treatment of the diferric form with EDTA-containing buffer as described in Ref. [39]. 51CrCl3 was added to solutions of apotransferrin; these solutions were slowly stirred overnight to allow equilibrium to be achieved. The samples were loaded onto a Sephadex G-15 column to separate any uncombined metal. Insulin (bovine, zinc) was obtained from Calbiochem. Bovine liver chromodulin was isolated as described previously [40]. All procedures were performed using doubly deionized water unless otherwise noted and were performed with plasticware whenever possible.
Rats
Adult male Sprague Dawley rats (500–650 g) were obtained from Charles River Laboratories. Use of the adult rats allows for sufficient tissue to be obtained for hepatocyte subcellular distribution studies. The rats were injected in the tail vein with 130 μL of an aqueous solution containing 0.83 mg 51Cr2 transferrin corresponding to approximately 0.5 μg Cr and were placed into metabolic cages for collection of urine. The rats received 2.46×106 cpm 51Cr. Rats receiving insulin were injected with 150 μL of an aqueous solution containing the same quantity of labeled transferrin plus insulin (25 USP insulin units). After the appropriate time interval, blood was collected from tail snips into polypropylene tubes containing heparin and NaF. The rats were then sacrificed by carbon dioxide asphyxiation, and tissue samples were harvested and weighed. Muscle (muscolus triceps surae) samples were taken from a hind leg. Each data point represents the average of three rats. The total 51Cr content of blood and muscle was calculated assuming that the blood constituted 6% of the rats’ body mass and muscle constituted 30% of the body mass. The University of Alabama Institutional Animal Use and Care Committee approved all procedures involving the use of rats.
Hepatocyte fractionation
Subcellular liver fractions were obtained by differential centrifugation according to established procedures [22, 41, 42]. Tissues were diced, and the pieces were rinsed with 0.25 M sucrose solution. All subsequent steps were performed using the same solution. The pieces were ground in a tissue grinder. The nuclear, mitochondrial, lysosomal, and microsomal fractions were obtained as pellets from centrifugation at 30g, 3,300g, 25,000g, and 100,000g, respectively.
Chromatography and electrophoresis
Urine, blood plasma and subcellular fractions were rapidly frozen after collection and were stored at −20°C; samples were thawed immediately before subsequent use. S-200 column chromatography or Shodex OH-PAK high-performance liquid chromatography (HPLC) was used to separate components of the urine, blood plasma, and subcellular hepatocyte fractions. Chromatography columns were run with 50 mM NH4OAc buffer, pH 6.5; 0.1 M NaCl was used as the mobile phase for HPLC experiments. For Western blotting experiments, 4–20% tris(hydroxymethyl)aminomethane–HCl Ready Gels (Bio-Rad) were utilized. The 51Cr chromium content of the bands was determined by excising the bands from the polyacrylamide gels, followed by gamma counting.
Instrumentation
UV/vis measurements were made with a Hewlett-Packard 8453 spectrophotometer. Gamma counting was performed with a Packard Cobra II auto-gamma counter.
Statistical analysis
Numerical values in the tables and the text are presented as means ± the standard deviation. Curve-fitting was performed using Sigmaplot 8.0.2.
Results
Urine Cr
As noted previously with young [36] and adult [22] rats, 51Cr appears rapidly in the urine (within 120 min) after being introduced into the bloodstream as 51Cr transferrin. A 51Cr transferrin was injected to get a suitable quantity of 51Cr into the body for the desired studies; intravenous administration of other forms of 51Cr, such as 51CrCl3, introduces no physiologically relevant forms of Cr into the bloodstream. As shown in Fig. 1, almost 30% of the injected 51Cr is lost in 30 min. Urinary 51Cr loss continues at reduced rates until 3 days after injection when urinary Cr loss is minimal and approximately 80% of the injected 51Cr has been lost. Injection of insulin with the 51Cr transferrin results in an increase in the extent of urinary 51Cr loss, especially at early time points. After 30 min, 58% of the injected 51Cr has been lost via the urine; by 1 day, 83% of the injected 51Cr has been lost.

Urinary total chromium loss for adult male rats as a function of time. Solid circles indicate rats that did not receive insulin; open circles indicate rats receiving insulin. The lines represent fits of the curves. The initial injection contained 2.46×106 cpm 51Cr transferrin. Each data point represents the average of three rats.
Close examination of the urinary excretion curves in Fig. 1 suggests that the 51Cr loss cannot be described by a simple exponential increase to a maximum over time; indeed satisfactory fitting of the curves requires a biphasic model, four-variable model,
where t is the time elapsed in minutes after injection of Cr transferrin, and b and d are rate constants from the appearance of Cr from pools a and c, respectively. In the absence of insulin, the fit gives a=9.81×105 (±7.9×104) cpm, b=0.0486 (±0.0153) min−1, c=1.20×106 (±1.8×105) cpm, and d=0.0005 (±0.0002) min−1, with R2=0.989. In the presence of insulin, the fit gives a=1.80×106 (±5.5×104) cpm, b=0.0493 (±0.0051) min−1, c=4.01×105 (±6.2×104) cpm, and d=0.0012 (±0.0005) min−1, with R2=0.997. In both cases the two phases have identical rate constants (within error), indicating the processes leading to urinary chromium loss do not change upon addition of insulin. [Note that the fit to the data in the absence of insulin is rather poor and suggests the need for a more complex pharmokinetic model (vide infra).] Thus, the major component of the urinary excretion during the first 24 h after injection in the absence of added insulin is the slower loss of chromium. Insulin treatment results in nearly doubling the magnitude of the rapid phase of 51Cr loss, making it the major contributor to urinary Cr content, and also in a decrease by two thirds in the amount of 51Cr loss in the slow phase.
The 51Cr in the urine of both the rats receiving and the rats not receiving insulin was found to elute as a single peak at all times examined upon G-25 size-exclusion chromatography (Fig. 2). The features migrate at the same position as isolated bovine liver chromodulin (molecular weight 1,438) when applied to the same column; this oligopeptide is the only small molar mass biomolecule known to bind chromium in vivo. Thus, the feature is tentatively assigned to chromodulin. [Given this is only tentative following the practice of Wada and coworkers based on only the apparently similar molecular weight and chromium-binding ability, the low-molecular-weight chromium-binding compound(s) in urine and tissues (vide infra) will be designated herein as chromodulin-like species.] This is consistent with previous studies using Cr transferrin [22, 36] and with studies using other forms of chromium that release chromium in vivo [31, 37, 38]. The identification of radiolabeled chromodulin by its elution profile is made necessary by an inability to detect similar levels of chromodulin presently by other techniques. The oligopeptide has proven not to be antigenic to date, making use of immunochemical techniques impossible. While mass spectra and post source decay spectra of chromodulin have recently been obtained by matrix-assisted laser desorption ionization time-of-flight mass spectrometry (m/z=1,439 for [M+nH]+; Y. Sun, J. Vincent, S. Webb, C. Cassady, unpublished results), attempts to use the technique to identify the oligopeptide in biological samples (even when spiked with the oligopeptide) have not been successful.

Elution profiles of urine from adult male rats from a G-25 column as a function of time. a Rats not receiving insulin; b rats receiving insulin
Both the slower and faster phases of urinary 51Cr loss both arise from chromodulin-like-species loss. Several studies have shown that Cr is lost in the urine within 90 min of a dietary stress such as high sugar intake [23–29]. This Cr increase in response to sugar is actually the result of the increases in blood insulin concentration associated with the increased sugar concentrations [23], consistent with the results of this study. Thus, as suggested previously [6–8], a direct link appears to relate urinary chromodulin loss and carbohydrate metabolism.
Blood plasma Cr
Examination of the labeled Cr content of the blood plasma in the absence of added insulin (Fig. 3) as a function of time reveals a rapid loss of plasma 51Cr for the first 30 min, followed by a more gradual loss of 51Cr. The removal of 51Cr from the blood is faster than the appearance of 51Cr in the urine. The lag in time indicates that the major forms of Cr in the blood and urine are not in direct equilibrium; intermediates in the transport of Cr must be involved. Previously, blood plasma levels after intravenous injection of CrCl3 as a function of time have been fit to the sum of three exponential decays [43–45]. These decays have been interpreted in terms of the existence of three pools of tissue chromium exchangeable with the plasma Cr, which is ultimately lost in the urine. The pools have varying half-lives on the order of 0.5–12 h, 1–14 days, and 3–12 months. Attempts to fit the loss of plasma Cr in the absence of insulin to the sum of three exponential decays failed as the data underdetermined the fit. Given that one of the decays in the previous fits was a slow decay on the order of months, which would essentially contribute a constant background over the time frame of the current study, attempts were made to fit the data to the sum of two exponential decays and a constant background level of labeled Cr; these also failed.

Blood plasma total chromium for adult male rats as a function of time. Solid circles indicate rats that did not receive insulin; open circles indicate rats receiving insulin. The lines represent fits of the curves. The initial injection contained 2.46×106 cpm 51Cr transferrin. Each data point represents the average of three rats.
One reason for this failure is apparent from the behavior in the presence of insulin (Fig. 2). In this case, the rapid loss of plasma 51Cr is followed by a small increase in the 51Cr content. Thus, the behavior appears to be more complex than rate-limiting exchanges of Cr and rapid loss of Cr in the urine. The behavior of the plasma 51Cr levels in both the presence and the absence of insulin can be fit reasonably well over the time scale of this experiment to the sum of a constant 51Cr background and an exponential loss of 51Cr:
In the absence of added insulin, a=2.71×105 (±2.9×104) cpm, b=2.19×106 (±7.6×104) cpm, and c=0.0838 (±0.0143) min−1 (R2=0.994). In the presence of insulin, a=1.76×105 (±1.3×104) cpm, b=2.28×106 (±3.5×104) cpm, and c=0.102 (±0.0109) min−1 (R2=0.999). (The determination of the rate constant for the exponential loss of plasma Cr is limited by the lack of data points at earlier times. Given that 10–15 min is required to guarantee distribution of the injected transferrin throughout the bloodstream and that time is required to collect a blood sample, reliably obtaining data points at times appreciably earlier than 30 min after injection unfortunately is not feasible.)
The problems with the fits can be explained by examining the S-200 size-exclusion elution profiles of the plasma as a function of time (Fig. 4a). In the absence of added insulin, the elution profile is dominated by the protein transferrin (which elutes approximately at fraction 45). (Authentic samples of rat transferrin elute at this position from the column; additionally sodium dodecyl sulfate–polyacrylamide gel electrophoresis followed by transfer to nitrocellulose and immunoblotting reveals that transferrin is a major component of this band and that 51Cr comigrates on the gel with transferrin.) More 51Cr is associated with transferrin than any other species for the first day after injection. In a bimodal fashion, 51Cr transferrin levels drop rapidly and then drop gradually. A 51Cr-containing species (eluting at approximately fraction 78) is maximal at 30 min, and its level declines gradually with time. The identity of this feature has not been established. It has been postulated to be a metabolism product of transferrin [22]; when CrCl3 is administered intravenously rather than Cr transferrin, this feature is not observed [11]. However, it does not react with polyclonal transferrin antibodies, indicating it is not a fragment of transferrin or it lacks the antigenic site(s) of transferrin. Another species, with a similar molecular weight to chromodulin (eluting at approximately fraction 118), is barely detectable after 30 min, but its level rises with time. Previously, this species on the basis of the molecular weight and its ability to bind Cr was postulated to be chromodulin [22, 36]; this, however, is not the case. Thus, the exponential decay component of the fit corresponds to the rapid mode of loss of transferrin from the plasma during the first hour after injection; the constant component probably is attributable to the gain of the low molecular weight species and the loss of the unidentified species that roughly cancel each other. In fact, the smallest molecular weight species appears to be derived from the larger species. The larger species appears rapidly (maximal concentration at the first time point after injection), followed by a drop in its concentration that closely matches the appearance of the smaller species. The appearance of low molecular weight Cr-containing species from the possible metabolism of transferrin has been noted previously in experiments with human plasma [46]. This pathway, the conversion of transferrin into the two unidentified species, accounts for less than 10% of the total injected Cr. Consequently the behavior of 51Cr in the plasma in the first few hours after injection is far more complex than can be explained by a fit to three exponential losses.

Elution profiles of blood plasma from adult male rats from a S-200 column as a function of time. a Rats not receiving insulin; b rats receiving insulin
Insulin has a dramatic effect on the 51Cr-containing species in the blood plasma as a function of time (Fig. 4b). Transferrin levels again drop rapidly. The larger unidentified species is still present 30 min after injection, and its level drops with time. The level of the smaller species strikingly rises with time during the first 720 min after injection such that most plasma 51Cr is in the form of this species, rather than transferrin. This is reflected in the maximum in the total blood plasma 51Cr as a function of time curve. In the simplistic fit to an exponential decrease and a constant background, the magnitude of the loss of 51Cr transferrin is identical in the presence and absence of insulin, as are the rate constants. The constant contribution after this time crudely corresponds to the sum of the levels of transferrin after the first 60 min and those of the two unidentified species. The amount of 51Cr bound to transferrin and to the chromodulin-like species as a function of time can be calculated from the data in Fig. 4 and is shown in Figs. 5 and 6. Comparison of the results in the presence and absence of insulin indicates that the extent of disappearance of 51Cr transferrin from the blood in the first 120 min after injection is greater in the animals receiving insulin. The disappearance of 51Cr transferrin for the insulin-treated animals can be fit reasonably well by a simple exponential loss:
where a=2.46×106 (±3.6×104) cpm and b=0.0790 (±0.0053) min−1 (R2=0.998). In the absence of insulin, the behavior of the 51Cr transferrin level as a function of time is clearly more complex than a single exponential loss; however, the data underdetermine attempts to fit the curve to two exponential losses. As can also be noted from Fig. 5, the appearance of the smaller unidentified species in the blood is actually slightly slower than the appearance of chromodulin-like species in the urine.

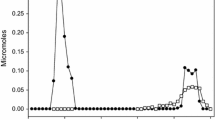
Content of injected chromium as Cr transferrin, chromodulin, tissue Cr, and urinary chromodulin as a function of time. a Rats not receiving insulin; b rats receiving insulin. The initial injection contained 2.46×106 cpm 51Cr transferrin. Each data point represents the average of three rats.

Tissue total chromium content for adult male rats not receiving insulin as a function of time. Each data point represents the average of three rats.
Total tissue Cr
Taking into consideration the amount of radiolabel in the urine and blood, a large quantity of 51Cr is absorbed into the tissues. Figure 5 displays the amount of 51Cr injected minus the amounts of urinary and plasma 51Cr; this is an approximation of the amount of 51Cr absorbed and retained in the tissues as a function of time. Fecal Cr losses have not been included. Fecal losses correspond to Cr from the bile and, thus, reflect absorbed chromium, although even when using metabolic cages contamination from the urine also occurs. Fecal Cr losses over 1 day should correspond to only about 2% of the injected Cr [43, 45]. Retained 51Cr is maximal at 30 min, the first time point examined after the injection (note that 10–15 min is required to guarantee distribution of the injected transferrin throughout the bloodstream). Thus, transfer of 51Cr from 51Cr transferrin in the blood to tissues is very rapid. The loss of 51Cr from transferrin, thus, occurs simultaneously with the rise of tissue 51Cr; the tissue 51Cr levels subsequently decrease with the increase of urine 51Cr levels. This indicates a net movement of 51Cr from 51Cr transferrin to the tissues to the urine. Interestingly insulin injection has the effect of lowering retained 51Cr at all times, yet 51Cr disappeared from the transferrin in the blood plasma to a greater extent at early time points in the rats given insulin. This is readily explained by the greater urinary loss of 51Cr in rats receiving insulin. Insulin not only increases the transfer of 51Cr from transferrin to the tissues but also results in much greater movement of 51Cr into chromodulin-like species, resulting in its loss in the urine. Thus, while 51Cr moves to a greater extent from the blood to the tissues, tissue 51Cr levels are lower as this is more than offset by an increase in the generation of chromodulin-like species and its loss in the urine. Thus, insulin appears to accelerate the processing of 51Cr by the tissues. Also of significance is that while the effect of insulin on transferrin movement can account for increased movement of Cr from the bloodstream into the tissues, this cannot account for the increased flux of Cr through the tissues and into the urine. Also, Fe(III) released from transferrin is reduced in endosomes to Fe(II), which is transported into the cytosol by divalent metal ion transporters [47]; this route is probably not available to Cr(III). The potentials for the reduction of Cr(III) complexes with biological ligands generally are too negative for reduction of the Cr(III) by biological reductants. Thus, insulin must have a separate action on chromium metabolism.
Tissue Cr distribution
The distribution of 51Cr in selected tissues as a function of time is shown in Figs. 6 and 7 for rats receiving insulin. For all tissues examined in the absence of added insulin, the 51Cr content of every tissue or organ except the heart reached a maximum level or a plateau within 120 min of the injection. Liver and muscle had by far the greatest quantities of 51Cr. In the presence of insulin, the 51Cr content of every tissue also reached a maximum level or a plateau within 120 min of the injection. Liver and muscle again possessed the greatest quantities of 51Cr at all times. However, insulin administration results in an accelerated rate of loss of 51Cr from each of these tissues. This is consistent with the more rapid loss of 51Cr from the tissues observed with insulin treatment as shown in Fig. 5.

Tissue total chromium content for adult male rats receiving insulin as a function of time. Each data point represents the average of three rats.
Hepatoctye subcellular Cr distribution
Because of the large 51Cr content of the liver, the subcellular distribution of 51Cr in hepatocytes was investigated (Figs. 8, 9). In both rats receiving and rats not receiving insulin, the greatest quantity of 51Cr is in the nuclei, with the maximum quantity reached 120 min after injection. The contents of the other subcellular components follow similar time courses within experimental error. These results, as well as the other results described before, are consistent with previous studies using 51Cr transferrin that only looked at 51Cr distribution 120 min after injection (with and without administration of insulin) [22, 36]. After 120 min, insulin treatment results in a more rapid loss of 51Cr from the nuclear fraction than in the absence of insulin. Thus, insulin has little or no effect on the distribution of Cr between compartments; the effects of the hormone are primarily on the rate that Cr is cleared from the compartments.

Subcellular distribution of chromium in hepatocytes of adult male rats not receiving insulin as a function of time. Each data point represents the average of three rats.

Subcellular distribution of chromium in hepatocytes of adult male rats receiving insulin as a function of time. Each data point represents the average of three rats.
The components of the cytosol at each time point were separated by S-200 chromatography to attempt to identify the 51Cr-containing species (Fig. 10). In the elution profiles, two major 51Cr features are present: a large molecular weight feature corresponding to transferrin (established again by comparison of the elution profile with that of authentic transferrin and immunoblotting) and a smaller molecular weight feature that elutes at the same position as chromodulin. In addition, small amounts of very large molecular weight species which elute with the solvent front and of species with molecular weights lower than chromodulin are observable. The appearance of transferrin in the cytosol probably results from the very low density transferrin-containing endosomes, which fail to precipitate with the microsomal fraction; rupture of endosomes from freezing and thawing releases the Cr transferrin. In the presence and absence of added insulin, the amount of transferrin rises with time for the first 120 min and then steadily decreases. Without added insulin, the amount of chromodulin-like species present rises for the first 120 min and then decreases steadily. When insulin is administered, the amount of chromodulin-like species in the cytosol rises for the first 360 min and then decreases. One result of this is that, for example, 120 min after the injection that rats not receiving insulin have more 51Cr in the form of chromodulin-like species than in the form of 51Cr transferrin and this is reversed in the presence of insulin (as noted previously [22, 36]). One interesting effect of insulin is a change in the relative time for levels of Cr transferrin and chromodulin-like species to become maximal. In the absence of insulin, both levels rise almost simultaneously; while in the presence of insulin, Cr-transferrin levels peak first (in the same time required in the absence of insulin). Yet, the peak chromodulin-like-species level appears at an appreciably delayed time, suggesting that insulin effects the processing of Cr during or between removal from transferrin and binding to chromodulin-like species. The appearance and reasonably rapid disappearance of transferrin in hepatocytes with the concomitant or subsequent appearance of another form of bound Cr provides additional evidence that transferrin is the primary Cr transport agent from the blood to the tissues. Consistent with this conclusion is the work of Sayato et al. [11], who followed the fate of 51Cr given as 51CrCl3. Components of the hepatocyte cytosol (120 min after treatment) were separated by G-200 size-exclusion chromatography. Comparison of their results with those presented in Fig. 10a suggests that these authors observed Cr transferrin in the cytosol of the liver cells.

Elution profiles of soluble fraction of hepatocytes from adult male rats from a S-200 column as a function of time. a Rats not receiving insulin; b rats receiving insulin
Discussion
On the basis of these results, a kinetic model for the movement of Cr from transferrin in the blood to chromodulin-like species in the urine has been proposed (Scheme 1). The model assumes the presence of five major types of chromium: Cr transferrin in the blood plasma (A), Cr in the tissues (B), chromodulin-like species in the plasma (C), the smaller unidentified species in the plasma (F), the larger unidentified species in the plasma (E), and chromodulin-like species in the urine (D). Because of the varying rates of Cr absorption and excretion by the tissues, tissue chromium is used to express the average Cr content of tissues. Two pathways are required to fit the movement of Cr from transferrin to the urine and species in the bloodstream. The first involves the transport of Cr by transferrin to the tissues (k1), followed by the release of Cr and production and release of chromodulin-like species into the blood (k2), and the movement of chromium as chromodulin-like species from the blood to the urine (k3). The presence of chromodulin-like species in the tissues (vide infra) and in the urine necessitates the presence of chromodulin-like species in the blood plasma, although its presence appears to be masked by the smaller unidentified species. Hence, chromodulin-like species is assumed to be kept at low steady-state levels in the blood, and k3 is assumed to be much larger than k1 and k2. The second pathway includes the appearance of the larger unidentified species (k4), which in turn is either metabolized to generate the smaller unidentified species or gives up its Cr to the smaller species (k5). This kinetic model fits the experimental data well at the early time points but fails to simulate the gradual loss of Cr from the tissues to the urine. This failure arises because the model does not incorporate the processing and loss of chromium from the various tissues occurring at different rates, as is obvious from Figs. 6 and 7. This manifests itself, for example, in the requirement for at least a biphasic function to fit to the appearance of chromodulin-like species in the urine as a function of time. Although the quantity of Cr distributed in several tissues as a function of time was determined in the present work, additional experiments are necessary and are under way to determine the Cr-containing species and rates of conversion in different tissues so that a more sophisticated pharmokinetic model of chromium transport can be developed.

Proposed mechanism of distribution of chromium from Cr transferrin
Conclusion
If Cr is an essential trace element, a specific transport and distribution mechanism should exist. Injection of 51Cr-labeled transferrin into the bloodstream resulted in a rapid and insulin-sensitive movement of Cr into the tissues as Cr transferrin. Tissue levels of Cr were maximal 30 min after injection; decreases in tissue Cr with time were mirrored by increases in urine Cr. The removal of Cr from the blood was faster than the appearance of Cr in the urine; the lag in time indicates that the Cr transferrin in the blood and the Cr in the urine are not in direct equilibrium and that intermediates in the transport of Cr must be involved. This establishes a clear pathway of transport of Cr starting from transport by transferrin from the bloodstream into the tissues, followed by release and processing in the tissues to form chromodulin-like species, excretion of chromodulin-like species into the bloodstream, rapid clearance of chromodulin-like species into the urine, and ultimately excretion as chromodulin-like species. Insulin stimulates the processing of Cr in the tissues, such that the insulin-dependence of Cr transport is only explained in part by insulin-sensitive transferrin movement. The data are consistent with an association between Cr and insulin signaling.
References
Boccio J, Salgueiro J, Lysionek A, Zubillaga M, Weill R, Goldman C, Caro R (2003) Biol Trace Elem Res 92:189–212
O’Halloran TV, Culotta VC (2000) J Biol Chem 275:25057–25060
Outten CE, O’Halloran TV (2001) Science 292:2488–2492
Carrington PE, Chivers PT, Al-Mjeni F, Sauer RT, Maroney MJ (2003) Nat Struct Biol 10:126–130
Luk E, Jensen LT, Culotta VC (2003) JBIC 8:803–809
Vincent JB (2000) Acc Chem Res 33:503–510
Vincent JB (2001) Polyhedron 20:1–26
Vincent JB (2004) Biol Trace Elem Res 99:1–16
Anderson RA, Kozlovsky AS (1985) Am J Clin Nutr 41:1177–1183
Hopkins LL Jr, Schwarz K (1964) Biochim Biophys Acta 90:484–491
Sayato Y, Nakamuro K, Matsui S, Ando M (1980) J Pharm Dyn 3:17–23
Aisen P, Aasa R, Redfield AG (1969) J Biol Chem 244:4628–4633
Tan AT, Woodworth RC (1969) Biochemistry 8:3711–3716
Harris DC (1977) Biochemistry 16:560–564
Ainscough EW, Brodie AM, Plowman JE, Bloor SJ, Sanders-Loehr J, Loehr TM (1980) Biochemistry 19:4072–4079
Ainscough EW, Brodie AM, Plowman JE (1979) Inorg Chim Acta 33:149–153
Moshtaghie AA, Ani M, Bazrafshan MR (1992) Biol Trace Elem Res 32:39–46
Ani M, Moshtaghie AA (1992) Biol Trace Elem Res 32:57–64
Sun Y, Ramirez J, Woski SA, Vincent JB (2000) JBIC 5:126–136
Vincent JB (1999) J Nutr 130:715–718
Dowling HJ, Offenbacher EG, Pi-Sunyer FX (1990) Nutr Res 10:1251–1260
Clodfelder BJ, Emamaullee J, Hepburn DD, Chakov NE, Nettles HS, Vincent JB (2001) JBIC 6:608–617
Morris BW, MacNeil S, Stanley K, Gray TA, Fraser R (1993) J Endocrinol 139:339–345
Anderson RA, Polansky MM, Bryden NA, Roginski EE, Patterson KY, Veillon C, Glinsmann W (1982) Am J Clin Nutr 36:1184–1193
Anderson RA, Polansky MM, Bryden NA, Roginski EE, Patterson KY, Reamer DC (1982) Diabetes 31:212–216
Anderson RA, Bryden NA, Polansky MM, Reiser S (1990) Am J Clin Nutr 51:864–868
Kozlovsky AS, Moser PB, Reisner S, Anderson RA (1986) Metabolism 35:515–518
Morris BW, Blumsohn A, MacNeil S, Gray TA (1992) Am J Clin Nutr 55:989–991
Morris BW, Griffiths H, Kemp GJ (1988) Clin Chem 34:1114–1116
Kandror KV (1999) J Biol Chem 274:25210–25217
Wu GY, Wada O (1981) Jpn J Ind Health 23:505–512
Yamamoto A, Wada O, Ono T (1987) Eur J Biochem 165:627–631
Wada O, Wu GY, Yamamoto A, Manabe S, Ono T (1983) Environ Res 32:228–239
Yamamoto A, Wada O, Ono T (1984) J Inorg Biochem 22:91–102
Feng WY, Qian QF, Ding WJ, Chai ZF (2000) J Radioanal Nucl Chem 244:321–325
Clodfelder BJ, Upchurch RG, Vincent JB (2004) J Inorg Biochem 98:522–533
Shute AA, Chakov NE, Vincent JB (2001) Polyhedron 20:2241–2252
Hepburn DDD, Vincent JB (2002) Chem Res Toxicol 15:93–100
Mazurier J, Spik G (1977) Biochim Biophys Acta 629:399–408
Davis CM, Vincent JB (1997) Biochim Biophys Acta 339:335–343
de Duve C, Pressman BC, Gianetto R, Wattiaux R, Appelmans F (1955) Biochem J 60:604–617
Rowin GL (1974) In: Methods in molecular biology. Marcel Dekker, New York, pp 90–109
Mertz W, Roginski EE, Reba RC (1965) Am J Physiol 209:489–494
Onkelinx C (1977) Am J Physiol 232:R478–R484
Lim TH, Sargent T III, Kusubov N (1983) Am J Physiol 244:R445–R454
Borguet F, Cornelis R, Lameire N (1990) Biol Trace Elem Res 26–27:449–460
Griffiths WJH, Kelley AL, Smith SJ, Cox TM (2000) Q J Med 93:575–587
Acknowledgements
Funding was provided by the National Institutes of Health (DK62094-01) and the American Diabetes Association to J.B.V. The authors wish to thank Bryan Gullick and Robert Upchurch for assistance with numerous experiments. J.B.V. is inventor or coinventor of four patents on the use of Cr oligopeptides and synthetic complexes as nutritional supplements and therapeutic agents.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Clodfelder, B.J., Vincent, J.B. The time-dependent transport of chromium in adult rats from the bloodstream to the urine. J Biol Inorg Chem 10, 383–393 (2005). https://doi.org/10.1007/s00775-005-0647-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00775-005-0647-3