
Abstract
Background
Limited data are available on the survival and causes of death in pediatric patients with chronic kidney disease (CKD) stage 5 receiving kidney replacement therapy (KRT) in Asia.
Methods
Data were obtained from the Japanese nationwide cross-sectional CKD stage 5 survey on pediatric patients (<20 years of age) who started KRT from 2006 to 2013. The cohort was divided into three groups according to age at the start of KRT: <1, 1–5, and 6–19 years.
Results
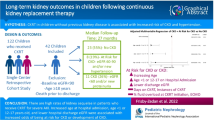
Among the 701 children who were included, 59.3% were boys. Peritoneal dialysis was the most common initial modality of KRT (60.3%). Median age at KRT initiation was 10.2 years. Infants (<1 year old) accounted for 16.0% of the total cohort. Overall survival at 1 and 5 years was 97.2% and 92.5%, respectively. Infants had significantly lower survival rates than the other groups (hazard ratio, 5.35; 95% CI, 2.60–11.03; P < 0.001). In contrast, after the age of 1 year, the survival rate improved and did not differ from that of other age groups. The most common causes of death were infection (35.9%) and sudden death (15.4%).
Conclusions
The overall survival rate of pediatric patients with CKD stage 5 in Japan is like that in other high-income countries. Age at initiation of KRT is an important factor affecting survival since the poorest survival rate was observed in infants. Further improvement in infant dialysis therapy is still needed to improve survival of the youngest children.
Graphical Abstract
A higher resolution version of the Graphical abstract is available as Supplementary information.

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Survival in the pediatric chronic kidney disease (CKD) stage 5 population has improved markedly over the last several decades due to advances in dialysis and transplantation techniques that are applicable to children [1,2,3,4,5,6,7,8]. Recent data from the North American Pediatric Renal Transplant Cooperative Study (NAPRTCS) showed that the 3-year survival rate of pediatric patients on chronic dialysis improved from 90% in the 1990s to 95% in the 2000s [9]. Similarly, in more recent years, longitudinal data from the Australia and New Zealand Dialysis and Transplant (ANZDATA) Registry revealed a strong effect with improved survival in pediatric patients with CKD stage 5 [10]. In addition, a 36% reduction in the 5-year mortality risk between 1980–1984 and 1995–2000 has been reported in European dialysis patients [11].
However, despite substantial advances in dialysis technology and clinical expertise over the past few decades and data showing improved survival and transplantation outcomes in children with CKD stage 5, the management of infants (<1 year old) requiring KRT remains a significant challenge for pediatric nephrologists. This age group has a variety of disadvantages, including difficulties in feeding and maintaining fluid balance, impaired growth, increased risk of infection, and presence of comorbidities. In addition, infants cannot undergo transplantation immediately. Infants are usually not referred for transplantation until they weigh 10 kg [12, 13] because kidney transplantation is technically more difficult due to the infant’s smaller body size and smaller vessel diameter compared to those of the relatively larger donor [14]. Several studies on infants have shown that this group has a significantly lower survival rate than those of children from other age groups [15, 16].
As noted, the survival rates of children with KRT have been reported in detail, mainly in Western countries. However, detailed information on the outcomes of KRT in children in Asian countries is lacking. In addition, there is a limited number of studies that have subdivided the younger age groups, especially infants. Therefore, we conducted a nationwide, retrospective cohort study to determine the survival rates and causes of death of Japanese pediatric patients with CKD stage 5 undergoing KRT, stratified by age.
Materials and methods
Study design and population
We conducted a nationwide cross-sectional survey in 2017 to update information on the incidence, primary kidney disease, initial treatment modalities, and survival in pediatric Japanese patients (<20 years of age) with CKD stage 5 during the period 2006–2013. This survey included 770 clinical departments in Japan, including all institutions that are members of the Japanese Society for Pediatric Nephrology (JSPN), the Japanese Society for Dialysis Therapy (JSDT), the Japanese Society for Clinical Renal Transplantation (JSCRT), and all university and children’s hospitals [17, 18]. CKD stage 5 was defined as an irreversible kidney function disorder requiring long-term dialysis of more than 3 months or transplantation.
The survey was administered via two questionnaires, one designed to record the presence and approximate number of children with CKD stage 5 in each institution, and a second consisting of detailed questions regarding the characteristics of each patient, including sex, age at initiation of KRT, primary kidney disease, initial treatment modality (i.e., peritoneal dialysis [PD], hemodialysis, or preemptive kidney transplantation), dates of treatment-related events, changes in treatment modality, serum creatinine level at the start of KRT, follow-up duration, and final outcome. Primary kidney disease, classified according to the European Renal Association and European Dialysis and Transplantation Association (ERA-EDTA) codes, was determined by the patients’ nephrologists [11].
Definitions of outcome variables
All-cause mortality is an outcome of interest. The observation period was defined as the period from the initiation of KRT until death or when the questionnaires were sent (August 18, 2017). The cause and time of death for each patient were individually reviewed and grouped into categories that are clinically relevant for pediatric patients, such as infection, cardiopulmonary, cerebrovascular, liver failure, pancreatitis, hemorrhagic shock, thrombotic microangiopathy, malignancy, primary disease, sudden death, and unknown/missing.
To describe in detail the outcomes of children with CKD stage 5 who started KRT during infancy, we categorized patients into the following three age groups at the start of KRT: <1, 1–5, and 6–19 years.
Ethics
This study was performed in accordance with the tenets of the Declaration of Helsinki. The study protocol was approved by the Central Ethics Board of the Tokyo Women’s Medical University (approval number: 2353). The requirement for informed consent was waived because of the retrospective nature of the study.
Statistical analysis
Baseline demographic and clinical characteristics are presented as the median (interquartile range [IQR]) or proportion, as appropriate. The Kaplan–Meier method of survival analysis was applied to calculate the probabilities of overall survival at 1–5 years after the initiation of KRT in each age group. Subsequently, to show the relationship more directly, we plotted the mortality risk across age as a continuous variable. In addition, Cox proportional hazards models were used to examine the hazard ratio (HR) for overall survival time according to age at the start of KRT, with the oldest age group (≥6 years) as the reference, and to adjust for variables such as initial KRT modality, primary kidney disease, and predictors of mortality identified in previous studies. Statistical analyses were performed using R version 4.1 (R Foundation for Statistical Computing, Vienna, Austria) (https://cran.r-project.org/), and P < 0.05 was considered statistically significant.
Results
Demographic characteristics
We identified 701 patients of <20 years of age who initiated KRT from January 1, 2006 to December 31, 2013. The demographic characteristics of these children are presented in detail in Tables 1 and 2 and Supplementary Table 1. The cohort consisted of 416 boys (59.3%) and 285 girls (40.7%). Congenital anomalies of the kidney and urinary tract were the most common etiologies of kidney disease in this cohort, accounting for 37.4% of patients with CKD stage 5. The most common initial KRT modality was PD, which was performed in 423 (60.3%) patients. Preemptive transplantation without prior dialysis was performed in 157 patients (22.4%), 90% of whom were in the 6–19-year-old group. The median age at KRT initiation was 10.2 years (IQR, 3.1–14.5 years). The most common age group was 6–19 years (67.0%). The youngest group, comprising those <1 year old, accounted for 16.0% of the total cohort.
Patient survival on kidney replacement therapy
The overall survival for the entire cohort at 1 and 5 years was 97.2% (95% CI, 95.6–98.2) and 92.5% (95% CI, 89.6–94.5), respectively. Figure 1 depicts the survival curves estimated by the Kaplan–Meier method stratified according to age at the initiation of KRT. Supplementary Fig. 1 illustrates this relationship more directly using a spline function. Patients younger than 1 year had significantly lower survival rates than those in the other groups (P < 0.001). Table 3 shows the survival rate by age of starting KRT. We found that the survival rate of the <1-year-old group was 92.4% (95% CI, 87.4–97.6) and 76.8% (95% CI, 67.7–87.0) at 1 and 5 years, respectively, which was lower than those of the other groups. On the other hand, after 1 year of age, the survival rate did not differ from that of other age groups.

Kaplan–Meier survival curves in children with CKD stage 5 stratified according to age at the commencement of KRT. Kaplan–Meier survival analysis showed that the younger age group (<1 year) had a significantly lower survival rate compared to that of the other age groups (hazard ratio [HR], 5.35; 95% CI, 2.60–11.03; P < 0.001). CKD, chronic kidney disease; KRT, kidney replacement therapy
In addition, Table 4 shows the adjusted HR of the association between age group and all-cause mortality. The adjusted HR for death was higher in the <1-year-old group compared to that of any group that started KRT at 1 year or older and was 5.35 (95% CI, 2.60–11.03; P < 0.001) when compared to the 6–19-year group.
Description of 39 cases of death during the observation period
Table 5 presents the demographic characteristics of the 39 children who died during the observation period. The median age of patients at the time of death was 3.6 years, and the median time from the introduction of KRT to death was 1.3 years. There was no difference in the number of deaths between male and female patients, and the main primary kidney diseases were cystic kidney disease and hereditary nephropathy. Among the deaths, there were fewer transplants for the initial modality of KRT.
Details of the time from the start of KRT to death and the causes of death for each age group are shown in Fig. 2. During the observation period, the highest number of patients (18/39, 46.2%) died within 1 year after the start of KRT. However, in the <1-year-old group, we found that there were constant deaths until about 3 years after the start of KRT. Of the 18 patients who died within 1 year, the most common causes of death were infection (8/18, 44.4%) and cardiopulmonary disease (5/18, 27.8%). Table 6 shows the causes and proportions of deaths according to age. Infection was the most common cause of death, accounting for 35.9% of all patients, followed by sudden death, with a rate of 15.4%. Furthermore, we found that both occurred in all age groups.

Detailed description of the deceased, including primary kidney disease and time from KRT initiation to death. (a) < 1 year old, (b) 1–5 years old, (c) 6–19 years old. CNS, congenital nephrotic syndrome; HDK, hypo/dysplastic kidney; ARPKD, autosomal recessive polycystic kidney disease; ADPKD, autosomal dominant polycystic kidney disease; AKI, acute kidney injury; ARB, angiotensin-II receptor blocker; FSGS, focal segmental glomerulonephritis; TMA, thrombotic microangiopathy; MELAS, mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes; KRT, kidney replacement therapy
Discussion
The cumulative 5-year survival rate for the entire cohort was 92.5%, which was excellent and like other high-income countries [8, 19]. However, the youngest age group, which started KRT before 1 year of age, had the worst mortality, which was five times higher than that in the older age group (≥6 years). Interestingly, after the age of 1 year, the survival rate clearly improved and did not differ from that of other age groups.
Until the early 1980s, chronic maintenance dialysis was not available for infants with CKD stage 5. Nowadays, however, most infants can be treated with dialysis due to remarkable advances in medical technology. The number of infants who started chronic PD and were registered in the United States Renal Data System (USRDS) increased from 543 during 1990–1999 to 1180 during 2000–2014 [20]. A similar trend was also observed in data from the NAPRTCS. The proportion of infants initiating chronic dialysis increased from 13.4% during 1992–2001 to 14.9% during 2002–2011 [9]. In the present study, the proportion of patients who started KRT during infancy was also high, at 16.0% of the entire cohort. This is approximately ten times higher than that in low-income countries, where medical resources are scarce [21]. Despite the high proportion of difficult-to-manage infants in this cohort, a high 5-year survival rate was achieved for the entire cohort.
However, the management of infants and <5-year-old children remains one of the greatest challenges for pediatric nephrologists [22,23,24,25]. It has already been reported that the survival rate of infants and <5-year-old children with CKD stage 5 is low. USRDS 2019 Annual Data revealed that the 5-year survival rate (83.0%) in children of 0–4 years of age who started chronic PD was significantly lower than that in the 5–17-year-old group (93.3%–96.0%) [19]. Similarly, data from the Italian Registry of Pediatric Chronic Dialysis (IRPCD) also showed that children <5 years of age at the start of dialysis had significantly lower survival rates than children who started dialysis at the age of 5–15 years [26]. Although the only available Asian data are from Taiwan, it was reported that the mortality rate of children aged 0–4 who started chronic PD was significantly higher than that of children aged 15–19 years [23]. In recent years, there has been a move to further stratify the children of the <5-year-old group: the <1-year-old group and the ≥1-year-old group. It has been found that the survival rate of the <1-year-old group remains quite low in Western countries [9]. However, detailed information in Asian countries is scarce. Therefore, in this study, the <1-year-old group was stratified for examination. The results showed that the survival rate of infants was significantly lower than that of other age groups, as reported in previous studies. However, the survival rate of children ≥1 year of age did not differ from that of other age groups and was clearly superior to that of infants. These results are consistent with the longitudinal data from the ANZDATA Registry, published in 2021 [10]. The reasons for the lower survival of infants on KRT have been reported to be related to the higher frequency of infections, including peritonitis on PD, primary kidney disease, including autosomal recessive polycystic kidney disease (ARPKD), and the presence of comorbidities [27,28,29,30,31,32]. In the present cohort, PKD was the most common primary kidney disease among infants. Infections were the most common cause of death within 1 year of KRT initiation.
The strength of this study is that we have described a detailed cohort of Asian children with CKD stage 5, with stratification of infants and <5-year-old children. However, this study has several limitations. First, since reporting to the Japanese Society for Pediatric Nephrology CKD stage 5 Survey is voluntary and at the discretion of the reporting physicians, it is reasonable to assume that some institutions would report only successful cases. However, as the mortality results in the survey seem to be consistent with the literature and other registries [23, 32,33,34], it remains a valid tool for investigating the outcomes of long-term dialysis initiated during childhood in Japan. Second, several institutions did not provide information on the causes of death, which would have resulted in a higher percentage of deaths reported as unknown, thus making comparisons more difficult. However, as these were considered to occur randomly, they were unlikely to affect the ranking of causes of death in this study. Third, patients who were on dialysis for CKD stage 5 but died before discharge may not have been included in the cohort. Thus, the number of deaths may have been underestimated. Fourth, since the number of events in this study is very small (39 cases), we may not have adjusted for all confounders. However, this is a common occurrence in this research field. Therefore, future studies with the establishment of a global registry are necessary.
Conclusion
The overall survival rate of pediatric patients with CKD stage 5 in Japan is like that in other high-income countries. The age at initiation of KRT is an important factor affecting survival since the poorest survival rate was observed in infants. Further improvement in infant dialysis therapy is warranted to improve the survival rate of infants.
References
Goodman WG, Goldin J, Kuizon BD, Yoon C, Gales B, Sider D, Wang Y, Chung J, Emerick A, Greaser L, Elashoff RM, Salusky IB (2000) Coronary-artery calcification in young adults with end-stage renal disease who are undergoing dialysis. N Engl J Med 342:1478–1483. https://doi.org/10.1056/NEJM200005183422003
Johnstone LM, Jones CL, Grigg LE, Wilkinson JL, Walker RG, Powell HR (1996) Left ventricular abnormalities in children, adolescents and young adults with renal disease. Kidney Int 50:998–1006. https://doi.org/10.1038/ki.1996.401
Groothoff JW, Grootenhuis M, Dommerholt A, Gruppen MP, Offringa M, Heymans HS (2002) Impaired cognition and schooling in adults with end stage renal disease since childhood. Arch Dis Child 87:380–385. https://doi.org/10.1136/adc.87.5.380
Bartosh SM, Leverson G, Robillard D, Sollinger HW (2003) Long-term outcomes in pediatric renal transplant recipients who survive into adulthood. Transplantation 76:1195–1200. https://doi.org/10.1097/01.TP.0000092524.75807.84
Mitsnefes MM (2002) Pediatric end-stage renal disease: heart as a target. J Pediatr 141:162–164. https://doi.org/10.1067/mpd.2002.126921
Mitsnefes MM, Daniels SR, Schwartz SM, Meyer RA, Khoury P, Strife CF (2000) Severe left ventricular hypertrophy in pediatric dialysis: prevalence and predictors. Pediatr Nephrol 14:898–902. https://doi.org/10.1007/s004670000303
Broyer M, Le Bihan C, Charbit M, Guest G, Tete MJ, Gagnadoux MF, Niaudet P (2004) Long-term social outcome of children after kidney transplantation. Transplantation 77:1033–1037. https://doi.org/10.1097/01.tp.0000120947.75697.8b
Chesnaye NC, van Stralen KJ, Bonthuis M, Harambat J, Groothoff JW, Jager KJ (2018) Survival in children requiring chronic renal replacement therapy. Pediatr Nephrol 33:585–594. https://doi.org/10.1007/s00467-017-3681-9
Weaver DJ Jr, Somers MJG, Martz K, Mitsnefes MM (2017) Clinical outcomes and survival in pediatric patients initiating chronic dialysis: a report of the NAPRTCS registry. Pediatr Nephrol 32:2319–2330. https://doi.org/10.1007/s00467-017-3759-4
Larkins NG, Wong G, Alexander SI, McDonald S, Prestidge C, Francis A, Le Page AK, Lim WH (2021) Survival and transplant outcomes among young children requiring kidney replacement therapy. Pediatr Nephrol 36:2443–2452. https://doi.org/10.1007/s00467-021-04945-9
van der Heijden BJ, van Dijk PC, Verrier-Jones K, Jager KJ, Briggs JD (2004) Renal replacement therapy in children: data from 12 registries in Europe. Pediatr Nephrol 19:213–221. https://doi.org/10.1007/s00467-003-1376-x
van Heurn E, de Vries EE (2009) Kidney transplantation and donation in children. Pediatr Surg Int 25:385–393. https://doi.org/10.1007/s00383-009-2350-x
Salvatierra O Jr, Millan M, Concepcion W (2006) Pediatric renal transplantation with considerations for successful outcomes. Semin Pediatr Surg 15:208–217. https://doi.org/10.1053/j.sempedsurg.2006.03.007
Neipp M, Offner G, Lück R, Latta K, Strehlau J, Schlitt HJ, Ehrich JH, Klempnauer J, Nashan Br (2002) Kidney transplant in children weighing less than 15 kg: donor selection and technical considerations. Transplantation 73:409–416. https://doi.org/10.1097/00007890-200202150-00015
Vidal E, van Stralen KJ, Chesnaye NC, Bonthuis M, Holmberg C, Zurowska A, Trivelli A, Da Silva JEE, Herthelius M, Adams B, Bjerre A, Jankauskiene A, Miteva P, Emirova K, Bayazit AK, Mache CJ, Sánchez-Moreno A, Harambat J, Groothoff JW et al (2017) Infants requiring maintenance dialysis: outcomes of hemodialysis and peritoneal dialysis. Am J Kidney Dis 69:617–625. https://doi.org/10.1053/j.ajkd.2016.09.024
Wedekin M, Ehrich JH, Offner G, Pape L (2010) Renal replacement therapy in infants with chronic renal failure in the first year of life. Clin J Am Soc Nephrol 5:18–23. https://doi.org/10.2215/CJN.03670609
Hattori M, Sako M, Kaneko T, Ashida A, Matsunaga A, Igarashi T, Itami N, Ohta T, Gotoh Y, Satomura K, Honda M, Igarashi T (2015) End-stage renal disease in Japanese children: a nationwide survey during 2006–2011. Clin Exp Nephrol 19:933–938. https://doi.org/10.1007/s10157-014-1077-8
Hirano D, Inoue E, Sako M, Ashida A, Honda M, Takahashi S, Iijima K, Hattori M, Japanese Society of Pediatric Nephrology (2020) Clinical characteristics at the renal replacement therapy initiation of Japanese pediatric patients: a nationwide cross-sectional study. Clin Exp Nephrol 24:82–87. https://doi.org/10.1007/s10157-019-01788-5
United States Renal Data System (2019) 2019 USRDS Annual Data Report: Epidemiology of kidney disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD. https://www.usrds.org/annual-data-report/. Accessed 30 June 2021
Sanderson KR, Yu Y, Dai H, Willig LK, Warady BA (2019) Outcomes of infants receiving chronic peritoneal dialysis: an analysis of the USRDS registry. Pediatr Nephrol 34:155–162. https://doi.org/10.1007/s00467-018-4056-6
Lalji R, Francis A, Johnson DW, McCulloch M (2020) Health disparities in access to kidney replacement therapy amongst children and adolescents with end-stage kidney disease in low- and lower-middle-income countries. Kidney Int 97:463–465. https://doi.org/10.1016/j.kint.2019.11.030
Rees L, Hattori M, Borzych-Dużałka D (2021) Infant dialysis. In: Emma F, Goldstein S, Bagga A, Bates CM, Shroff R (eds) Pediatric nephrology. Springer, Heidelberg, pp 1–14
Lin HH, Tsai CW, Lin PH, Cheng KF, Wu HD, Wang IK, Lin CY, Chen W, Huang CC (2012) Survival analysis of pediatric dialysis patients in Taiwan. Nephrology (Carlton) 17:621–627. https://doi.org/10.1111/j.1440-1797.2012.01613.x
Chavers BM, Molony JT, Solid CA, Rheault MN, Collins AJ (2015) One-year mortality rates in US children with end-stage renal disease. Am J Nephrol 41:121–128. https://doi.org/10.1159/000380828
Chesnaye NC, Schaefer F, Bonthuis M, Holman R, Baiko S, Baskın E, Bjerre A, Cloarec S, Cornelissen EAM, Espinosa L, Heaf J, Stone R, Shtiza D, Zagozdzon I, Harambat J, Jager KJ, Groothoff JW, van Stralen KJ, ESPN/ERA-EDTA Registry Committee (2017) Mortality risk disparities in children receiving chronic renal replacement therapy for the treatment of end-stage renal disease across Europe: an ESPN-ERA/EDTA registry analysis. Lancet 389:2128–2137. https://doi.org/10.1016/S0140-6736(17)30063-6
Rinaldi S, Sera F, Verrina E, Edefonti A, Gianoglio B, Perfumo F, Sorino P, Zacchello G, Cutaia I, Lavoratti G, Leozappa G, Pecoraro C, Rizzoni G, Italian Registry of Pediatric Chronic Peritoneal Dialysis (2004) Chronic peritoneal dialysis catheters in children: a fifteen-year experience of the Italian Registry of Pediatric Chronic Peritoneal Dialysis. Perit Dial Int 24:481–486. https://doi.org/10.1177/089686080402400515
Sanderson KR, Warady BA (2020) End-stage kidney disease in infancy: an educational review. Pediatr Nephrol 35:229–240. https://doi.org/10.1007/s00467-018-4151-8
Zaritsky JJ, Hanevold C, Quigley R, Richardson T, Wong C, Ehrlich J, Lawlor J, Rodean J, Neu A, Warady BA, SCOPE Investigators (2018) Epidemiology of peritonitis following maintenance peritoneal dialysis catheter placement during infancy: a report of the SCOPE collaborative. Pediatr Nephrol 33:713–722. https://doi.org/10.1007/s00467-017-3839-5
Hijazi R, Abitbol CL, Chandar J, Seeherunvong W, Freundlich M, Zilleruelo G (2009) Twenty-five years of infant dialysis: a single center experience. J Pediatr 155:111–117. https://doi.org/10.1016/j.jpeds.2009.01.007
Vidal E, Edefonti A, Murer L, Gianoglio B, Maringhini S, Pecoraro C, Sorino P, Leozappa G, Lavoratti G, Ratsch IM, Chimenz R, Verrina E, Italian Registry of Paediatric Chronic Dialysis (2012) Peritoneal dialysis in infants: the experience of the Italian Registry of Paediatric Chronic Dialysis. Nephrol Dial Transplant 27:388–395. https://doi.org/10.1093/ndt/gfr322
Carey WA, Martz KL, Warady BA (2015) Outcome of patients initiating chronic peritoneal dialysis during the first year of life. Pediatrics 136:e615–e622. https://doi.org/10.1542/peds.2015-0980
Galiyeva DB, Jackson CA, Wild SH, Burns S, Hughes D, Traynor JP, Metcalfe W, Halbesma N (2020) Long-term all-cause mortality and cardiovascular outcomes in Scottish children after initiation of renal replacement therapy: a national cohort study. Pediatr Nephrol 35:677–685. https://doi.org/10.1007/s00467-019-04430-4
Verrina E, Edefonti A, Gianoglio B, Rinaldi S, Sorino P, Zacchello G, Lavoratti G, Maringhini S, Pecoraro C, Calevo MG, Turrini Dertenois L, Perfumo F (2004) A multicenter experience on patient and technique survival in children on chronic dialysis. Pediatr Nephrol 19:82–90. https://doi.org/10.1007/s00467-003-1270-6
Groothoff JW, Gruppen MP, Offringa M, Hutten J, Lilien MR, Van De Kar NJ, Wolff ED, Davin JC, Heymans HS (2002) Mortality and causes of death of end-stage renal disease in children: a Dutch cohort study. Kidney Int 61:621–629. https://doi.org/10.1046/j.1523-1755.2002.00156.x
Acknowledgements
The authors thank all the patients, families, physicians, and institutes who contributed to the JSPN CKD Stage 5 Survey. The authors also thank doctors Akira Matsunaga, Toru Igarashi, Toshiyuki Ota, Takao Konomoto, Naoko Ito, Ryoko Harada, Takuya Fujimaru, and Kenichi Satomura; members of the JSPN CKD Stage 5 Survey Committee; doctors Yuko Akioka, Kenji Ishikura, Yuko Hamasaki, Yoshitomo Itami, Yoshimitsu Goto, Yoshihiko Ueda, Misako Hiramatsu, Shuich Ito, Osamu Uemura, Satoshi Sasaki, Ken Hatae, Hiroshi Hataya, Mikiya Fujieda, and Hiroshi Yoshimura; and members of the JSPN, the Japanese Society for Dialysis Therapy (JSDT), and the Japanese Society for Clinical Renal Transplantation (JSCRT) for their contributions to data collection.
Funding
This work was funded by the Japanese Society for Pediatric Nephrology (JSPN).
Author information
Authors and Affiliations
Consortia
Contributions
D. H., A. A., and M. H. conceived and designed the study; D.H. and E.I. performed statistical analyses; D.H., E. I., and M.H. developed the figures; D.H. and M.H. drafted and revised the paper; all authors interpreted the data, provided intellectual content, and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information

Supplementary Fig. 1
The hazard ratio for a unit increase of age using spline function. To show the relationship more directly, we have plotted the hazard ratio for a unit increase of age using a spline function. (PNG 146 kb)
Supplementary Table 1
(DOCX 13 kb)
Graphical Abstract
(PPTX 1589 kb)
Rights and permissions
About this article

{kind=link}
Cite this article
Hirano, D., Inoue, E., Sako, M. et al. Survival analysis among pediatric patients receiving kidney replacement therapy: a Japanese nationwide cohort study. Pediatr Nephrol 38, 1–7 (2023). https://doi.org/10.1007/s00467-022-05568-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-022-05568-4