
Abstract
Purpose
Since herniotomy is one of the most frequent surgical procedures, the socioeconomical impact of guidelines for convalescence is substantial; at the same time, the introduction of mesh techniques as standard procedure has led to a marked decrease in recurrence rates. Therefore, a reappraisal of guidelines concerning convalescence is warranted.
Methods
This study is a comprehensive review of the literature including all levels of evidence.
Results
If an inguinal hernia is repaired with an appropriate technique in a surgically and technically faultless contemporary procedure, it is fully stable immediately after surgery. Therefore, pain is the only rational limiting factor for physical activities after the intervention. If a patient wishes to go back to work or other activities early, there is no reason to not facilitate this via a generous prescription of analgesics. Even hard physical work can technically be resumed after complete healing of the skin wound, and prolonged sick leave is neither necessary nor beneficial. No interrelation between physical activity after herniotomy and recurrence rate has yet been demonstrated; a randomized controlled trial might finally clarify this question, but at a substantial effort.
Conclusions
The periods of inactivity practiced by patients and recommended by GPs are widely arbitrary and basically much too long, leading to unnecessary expenditures with an estimated order of magnitude of several hundred million € per year in Germany. To reduce this surplus, guidelines should be implemented by the surgical professional associations and communicated intensively towards GPs and patients.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Inguinal hernia repair is one of the most frequently performed surgical procedures with a total annual volume of more than 600,000 procedures in the USA [1, 2], approximately 100,000 in the UK [3] and more than 200,000 in Germany [4]. Consequently, the economical impact of the procedure itself as well as the required absence from work after the operation is substantial, and time to resumption of work is one of the key parameters in surgical outcome assessment [5–8].
From a technical point of view, there are several procedures with a well-proven efficacy and excellent results; mesh-repair techniques, as the last substantial technical breakthrough, have evolved as the current gold standard [9]. Laparoscopic repair shows some relevant advantages in terms of postoperative pain (acute and chronic) as well as return to usual activities without inevitably compromising the surgical success [10–12]. However, all contemporary techniques require knowledge, diligence, and dexterity from the surgeon to be successful, and the open (Liechtenstein) repair is technically less demanding and therefore less dependent on the surgeon’s experience than laparoscopic procedures [13]. Therefore, the recently observed trend towards laparoscopic procedures [14] may promote substandard success rates during the learning curve. Indeed, the impact of a single surgeon’s inferior performance on a center’s results has been demonstrated empirically [15], and for several decades, lackluster surgical technique is assumed to be the main reason for inguinal hernia recurrence [16].
Since intra-abdominal pressure plays a triggering—albeit not causative—role in inguinal hernia development, the avoidance of physical strain has been traditionally recommended after surgical repair. However, there is no indication that intra-abdominal pressure—the putative link between physical strain and recurrence—is related to the latter in any way [17].
There is a wide variety of recommendations that are mostly just expert opinions rather than the result of systematic research, and available guidelines are based on cohort or case–control studies of low evidence [9]. There are a precious few reports of clinical trials on this issue [18], and reliable, evidence-based recommendations for a requirement of physical inactivity after hernia repair are notably absent [19, 20]. Since the most current guideline [9] recommends some caution in patients doing heavy lifting (“Probably a limitation on heavy weight lifting for 2–3 weeks is enough”) without specifying either the probability or the threshold of “heavy”, physicians may decide to err on the side of caution rather than recommend a too-early return to work.
Therefore, one of the key outcome parameters of hernia surgery is based on arbitrary decisions rather than representing an objective feature of procedural quality, diminishing the informative value of the published results. Moreover, there is insufficient evidence to support the surgeon while making a decision of quite substantial impact: False recommendations may lead to unnecessary recurrences with potentially hazardous consequences for the patient [21, 22] on the one or economical penalties for patient and/or society due to unnecessary occupational downtime on the other hand.
The present review therefore attempts to gather and analyze all available evidence on a possible relationship between physical activity after surgical hernia repair and hernia recurrence.
Materials and methods
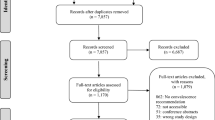
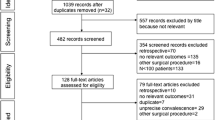
The analysis is based on a comprehensive literature search. Firstly, the reference database MEDLINE was searched for pertinent articles throughout its entire period of coverage (1966–2012); to create a pool of likely candidate trials for the review, the “Medical Subject Heading” (MeSH) “hernia, inguinal” was employed with “surgery” as a qualifying term and combined with “treatment outcome” or “recurrence”, respectively. Keywords for the specification of the search where “activities of daily living”, “work”, and “exercise” (MeSH); since there is no MeSH covering the subject of this article sufficiently, further keywords (weight, heavy, lifting, strain, and [return to] work) were also sought in titles and abstract, and articles were selected accordingly. The search was amended by the application of the “related articles” function on the PubMed web site to relevant sources e.g., [23–29], searches in other databases such as the Cochrane Library, and review of reference lists from the relevant identified articles.
Published material was weighed and analyzed according to the principles of evidence-based medicine. The usually employed in- and exclusion criteria for an evidence-based literature review were not applicable since only three articles would have qualified. Therefore, all available evidence was evaluated.
Results
RCTs concerning physical inactivity recommendations after herniotomy
Only three randomized controlled trials (RCTs)—all from the same center—concerning the main topic of this review were identified [23–25]. After an initial 3-week period of physical inactivity, patients received different recommendations for the ensuing time (immediate full occupational and recreational activity vs. activity according to the GP’s recommendation [23, 24] or reduced strain for an additional 3 months [25], respectively). GPs recommended extended periods of restrained activity, and immediate full workload had no adverse effects. On the contrary, the only recurrences observed by Taylor et al. [25] occurred after the extended reduced activity.
RCTs comparing various surgical procedures
There are a number of randomized controlled trials that have compared different surgical techniques and included resumption of work and/or daily activities as end points (data not shown). However, the explanatory power of these results is limited because resumption of work is profoundly influenced by socioeconomic circumstances, particularly sick leave compensations by employers and/or CIH or NHS [22]. Moreover, the periods of incapacitation for work or daily activities reflect the surgeons’ recommendations rather than the actual load capacity of the reconstruction, conveniently explaining the wide variety of inactivity periods reported in the literature. However, there appears to be a systematic trend towards shorter recovery periods and less postoperative pain after laparoscopic as opposed to open hernia repair [10–12].
Prospective cohort studies
Prospective clinical trials have denied a relationship between postoperative mobilization and hernia recurrence as early as in the 1940s [30]; nevertheless, extended periods of bed rest were part of the clinical routine for decades thereafter.
An American case–control comparison between patients covered by “worker’s compensation” or private health insurance, respectively [31], graphically corroborates the importance of socioeconomic circumstances: not only did the former group return much later to work (33.5 ± 4.6 vs. 12.6 ± 2.3 days) but it also reported persistent pain for a sixfold period (111.0 ± 42.2 vs. 17.8 ± 7.9 days).
In a subgroup of patients with recurrent hernia (n = 69), Chiofalo et al. [32] detected an equivalent time of return to work in comparison with patients without recurrence (n = 431).
Some studies indicate an earlier return to occupational and recreational activities after laparoscopic as compared to open repair [33, 34], but once again, this is more a function of the surgeons’ recommendations and the—often insufficiently treated—more intense pain after open surgery.
The only prospective comparison of different recommendations for convalescence was presented by Bay-Nielsen et al. [29]: Three groups of patients treated with the Liechtenstein procedure received the following advice:
-
1.
Immediate full activity without strain limits (n = 1,069)
-
2.
Reduced activity for 3–4 weeks (n = 1,306)
-
3.
No specific recommendations (8,297 reference patients from the Danish Hernia Database)
There were no significant differences between groups in terms of hernia recurrence, but alas, the recurrence rate in the first group was only half as high (0.7 %) as in the others (1.6 and 1.4 %, respectively). The single most important reason stated for extended periods of inactivity was pain under exertion.
Retrospective studies
In a number of retrospective studies, patients were advised to resume full physical activities early after the operation, and did so without any negative impact on the recurrence rates, which were well under 1 % [35, 36].
Questionnaires
Several published questionnaires show that the recommended periods of reduced activity after herniotomy vary substantially but are generally in excess of 4 weeks even for uncomplicated primary procedures [27, 37–45]; GPs typically recommend even longer periods of physical restraint than surgeons [26].
Interestingly, in a much discussed study published by Rider et al. [46], patients typically felt that they could have resumed work earlier than their surgeons had recommended. On the other hand, the actual period of absence from work often exceeded the aforementioned recommendations [37, 47].
In contrast to recurrence, there are clues that chronic pain after herniotomy—a relatively frequent residuum [48]—is promoted by early resumption of physical activities [49]; therefore, sufficient analgesia in the postoperative period is a prerequisite of early mobilization.
Expert opinions
In an analysis including surgical textbooks currently used in German medical schools [20], recommendations were imprecise and/or arbitrary and generally tended towards rather long periods of inactivity, typically over 1 and up to 6 months.
Discussion
There are undeniable international differences in recommendations with respect to physical inactivity after herniotomy, but these reflect peculiarities of health care financing and absence compensation for workers more than rational considerations concerning healing and rehabilitation. Moreover, the recommendations in the current literature are somewhat more generous than in older studies and textbooks, likely as a result of replacement of the Bassini and Shouldice operations by mesh-based techniques as the gold standard. The issue of physical restraint after herniotomy has been seriously “under-researched” so far, and a careful and comprehensive review of the currently available external evidence yields absolutely no reliable clues for an endangerment of a technically feasible Mesh reconstruction—irrespective of its open vs. laparoscopic placement—by physical activity of any type, including heavy lifting. This statement presently only pertains to standard “heavy” mesh techniques, because the issue of early return to daily activities has not yet been investigated with regard to lightweight or large-pore mesh techniques. However, the fact that there are no differences in recurrence rates [50] suggests that return to physical strain might not be more harmful than after standard mesh repair.
Interestingly, the situation in other surgical specialties closely corresponds to our observations with regard to herniotomy. For frequent procedures like cholecystectomy or hysterectomy, there is ample evidence for the reduction of postoperative pain by laparoscopic access e.g., [51–53], a wide variety of largely arbitrary recommendations for postoperative convalescence e.g., [54, 55], and a complete lack of evidence for a relationship between early resumption of work and physical activities on the one and the incidence of incisional hernia on the other hand.
The key prerequisite for success in hernia surgery is surgical prowess [16, 56], and the superior immediate stability of mesh repair has not yet been recognized sufficiently as far as postoperative convalescence procedures and guidelines are concerned.
Essentially, modern hernia repair allows for recurrence rates of under 1 % [57], but it does not guarantee such a result because the required surgical quality cannot automatically be assumed. The relative variability of recurrence rates stated in the literature [9, 58] suggests procedure-related prognostic factors; therefore, quality control and assurance should be implemented where this benchmark is missed by a substantial margin (i.e., when recurrence rates are above 3 %). The German Quality Assurance Office [58] and the European Hernia Society [9] reported recurrence rates of up to 19 % in contemporary series survey, indicating much room for improvement in some institutions.
Obviously, the target of any change in policy must not endanger the 1 % recurrence threshold, but the incentive to revise the current typical period of occupational downtime of 4 weeks is immense: Based on a number of 200,000 procedures per year and an estimated gross expenditure of 150–300 € per sick leave day (estimated from data of CHI insurers, hospital operating companies, and Ekman et al. [59]) in Germany, the reduction of downtime from 4 to 1 week would gain 630 million–1.26 billion € per year.
The rejection of such a gain would require solid evidence in favor of longer periods of inactivity, which the present literature is far from providing; on the contrary, the relatively few studies allowing such conclusions fail to show any differences [27, 29, 36]. Furthermore, any clinically observed differences would have to be carefully analyzed with regard to technical errors because biomechanical analyses have proven that since the introduction of the Shouldice technique, the loading capacity of reconstructed hernias exceeds any demands occurring in vivo [60, 61].
The key factors influencing absence from work are physicians’ recommendations and sick leave compensation, and not the actual requirements for a recurrence-free convalescence. A possible exception may be the—comparatively rare—true traumatic (so-called sports-) hernias for which some authors recommend longer periods of reduced physical load [62], but these hardly matter in the greater scheme of things.
The limiting factor for activity after herniotomy from an objective point of view is not recurrence risk, but pain [29, 63–65]. Technically, a properly performed mesh reconstruction of an inguinal hernia has full loading strength immediately after wound closure, and there is no evidence for a relationship between intra-abdominal pressure and hernia recurrence [17]. Since laparoscopic hernia repair is associated with less postoperative pain [10–12], it may facilitate the early resumption of work and daily activities, and consequently current guidelines favor laparoscopic access especially in patients in whom quick recovery and return to work is particularly important [9, 10]. Therefore, there is no reason why a patient should not return to his regular activities—regardless of the physical strain involved—immediately after healing of the skin wound, assuming that sufficient analgesia is provided. Interestingly, this conclusion hearkens back to the first pertinent study published by Blodgett and Beattie in 1947 [30].
Conclusion
It is unacceptable that patients or their GPs are individually responsible for the decision concerning when to resume occupational and recreational activities after herniotomy, and international as well as national guidelines should incorporate pertinent recommendations immediately. Guidelines should include the postoperative convalescence and—irrespective of the surgical proceeding—recommend generous analgesia for the postoperative period and unlimited physical and occupational activities after wound healing without fear of recurrence, but only after careful consideration of the possible side effects of prescribed analgesics. This may imply the choice of laparoscopic over open repair, but this aspect is not in the actual scope of our review and requires in-depth consideration of physician- and institution-related confounding factors.
Possibly, but not necessarily, the results of the present review could be corroborated by a prospective RCT, but the required study design is rather demanding, and the likelihood for novel insights is low.
References
Holzheimer RG (2004) First results of Lichtenstein hernia repair with Ultrapro®-mesh as cost saving procedure—quality control combined with a modified quality of life questionnaire (SF-36) in a series of ambulatory operated patients. Eur J Med Res 9(6):323–327
Holzheimer RG (2005) Inguinal hernia: classification, diagnosis and treatment—classic, traumatic and Sportsman's hernia. Eur J Med Res 10(3):121–134
Kurzer M, Kark A, Hussain T (2007) Inguinal hernia repair. J Perioper Pract 17 (7):318–321, 323–316, 328–330
Schumpelick V, Stumpf M, Schwab R (2004) Leistenhernienchirurgie als ambulante und kurzzeitstationäre Chirurgie. Möglichkeiten und Grenzen. Chirurg 75(2):126–130. doi:10.1007/s00104-003-0777-5
Prieto-Díaz-Chávez E, Medina-Chávez JL, Anaya-Prado R (2009) A cost-effectiveness analysis of tension-free versus shouldice inguinal hernia repair: a randomized double-blind clinical trial. Hernia 13(3):233–238. doi:10.1007/s10029-008-0461-2
Gholghesaei M, Langeveld HR, Veldkamp R, Bonjer HJ (2005) Costs and quality of life after endoscopic repair of inguinal hernia vs open tension-free repair: a review. Surg Endosc 19(6):816–821. doi:10.1007/s00464-004-8949-z
Kuhry E, van Veen RN, Langeveld HR, Steyerberg EW, Jeekel J, Bonjer HJ (2007) Open or endoscopic total extraperitoneal inguinal hernia repair? A systematic review. Surg Endosc 21(2):161–166. doi:10.1007/s00464-006-0167-4
Subhas G, Bakston D, Gupta A, Jacobs MJ, Mittal VK, Silapaswan S (2010) Internal ring occlusion and floor support: a novel technique for inguinal hernia mesh repair. Am Surg 76(9):933–937
Simons MP, Aufenacker T, Bay-Nielsen M, Bouillot JL, Campanelli G, Conze J, de Lange D, Fortelny R, Heikkinen T, Kingsnorth A, Kukleta J, Morales-Conde S, Nordin P, Schumpelick V, Smedberg S, Smietanski M, Weber G, Miserez M (2009) European Hernia Society guidelines on the treatment of inguinal hernia in adult patients. Hernia 13(4):343–403. doi:10.1007/s10029-009-0529-7
Bittner R, Arregui ME, Bisgaard T, Dudai M, Ferzli GS, Fitzgibbons RJ, Fortelny RH, Klinge U, Kockerling F, Kuhry E, Kukleta J, Lomanto D, Misra MC, Montgomery A, Morales-Conde S, Reinpold W, Rosenberg J, Sauerland S, Schug-Pass C, Singh K, Timoney M, Weyhe D, Chowbey P (2011) Guidelines for laparoscopic (TAPP) and endoscopic (TEP) treatment of inguinal hernia [International Endohernia Society (IEHS)]. Surg Endosc 25(9):2773–2843. doi:10.1007/s00464-011-1799-6
Aasvang EK, Gmaehle E, Hansen JB, Gmaehle B, Forman JL, Schwarz J, Bittner R, Kehlet H (2010) Predictive risk factors for persistent postherniotomy pain. Anesthesiology 112(4):957–969. doi:10.1097/ALN.0b013e3181d31ff8
Schmedt CG, Sauerland S, Bittner R (2005) Comparison of endoscopic procedures vs Lichtenstein and other open mesh techniques for inguinal hernia repair: a meta-analysis of randomized controlled trials. Surg Endosc 19(2):188–199. doi:10.1007/s00464-004-9126-0
Reuben B, Neumayer L (2006) Surgical management of inguinal hernia. Adv Surg 40:299–317
Alkhoury F, Martin JT, Contessa J, Zuckerman R, Nadzam G (2010) The impact of laparoscopy on the volume of open cases in general surgery training. J Surg Educ 67(5):316–319. doi:10.1016/j.jsurg.2010.08.001
Eklund AS, Montgomery AK, Rasmussen IC, Sandbue RP, Bergkvist LA, Rudberg CR (2009) Low recurrence rate after laparoscopic (TEP) and open (Lichtenstein) inguinal hernia repair: a randomized, multicenter trial with 5-year follow-up. Ann Surg 249(1):33–38. doi:10.1097/SLA.0b013e31819255d0
Nyhus LM (1989) The recurrent groin hernia: therapeutic solutions. World J Surg 13(5):541–544
Hendry PO, Paterson-Brown S, de Beaux A (2008) Work related aspects of inguinal hernia: a literature review. Surgeon 6(6):361–365
McIntosh A, Hutchinson A, Roberts A, Withers H (2000) Evidence-based management of groin hernia in primary care—a systematic review. Fam Pract 17(5):442–447
Bay-Nielsen M, Bisgaard T (2009) Rekonvalescens og sygemelding efter operation for lyskebrok. [Convalescence and sick leave following inguinal hernia repair]. Ugeskr Laeger 171(40):2899–2901
Lucht M (2008) Gesicherte Erkenntnisse zur Notwendigkeit einer körperlichen Schonung nach Leistenhernienoperation—Eine Evidenzbasierte Literaturstudie. Doctoral Thesis, Johann Wolfgang Goethe-Universität, Frankfurt/Main
Kavic MS (2005) Hernia repair: 2005. A reflection. Hernia 9(4):308–309. doi:10.1007/s10029-005-0001-2
McCormack K, Wake B, Perez J, Fraser C, Cook J, McIntosh E, Vale L, Grant A (2005) Laparoscopic surgery for inguinal hernia repair: systematic review of effectiveness and economic evaluation. Health Technol Assess 9(14):1–203, Ii–iv
Bourke JB, Taylor M (1978) The clinical and economic effects of early return to work after elective inguinal hernia repair. Br J Surg 65(10):728–731
Bourke JB, Lear PA, Taylor M (1981) Effect of early return to work after elective repair of inguinal hernia: clinical and financial consequences at one year and three years. Lancet 2(8247):623–625
Taylor EW, Dewar EP (1983) Early return to work after repair of a unilateral inguinal hernia. Br J Surg 70(10):599–600
Baker DM, Rider MA, Locker A, Fawcett AN (1993) How long do patients convalesce after inguinal herniorrhaphy? Current principles and practice. Ann R Coll Surg Engl 75(3):216
Baker DM, Rider MA, Fawcett AN (1994) When to return to work following a routine inguinal hernia repair: are doctors giving the correct advice? J R Coll Surg Edinb 39(1):31–33
Thorup J, Jørgensen T, Kjaergaard J, Billesbølle P (1994) Convalescence after inguinal herniorrhaphy. Scand J Gastroenterol 29(12):1150–1152
Bay-Nielsen M, Thomsen H, Andersen FH, Bendix JH, Sørensen OK, Skovgaard N, Kehlet H (2004) Convalescence after inguinal herniorrhaphy. Br J Surg 91(3):362–367. doi:10.1002/bjs.4437[doi]
Blodgett JB, Beattie EJ (1947) The effect of early postoperative rising on the recurrence rate of hernia. Surg Gynecol Obstet 84:716–718
Salcedo-Wasicek MC, Thirlby RC (1995) Postoperative course after inguinal herniorrhaphy. A case-controlled comparison of patients receiving workers' compensation vs patients with commercial insurance. Arch Surg 130(1):29–32
Chiofalo R, Holzinger F, Klaiber C (2001) Total endoskopische präperitoneale Netzplastik bei primären und Rezidivleistenhernien. Gibt es Unterschiede? Chirurg 72(12):1485–1491
Savarise MT, Simpson JP, Moore JM, Leis VM (2001) Improved functional outcome and more rapid return to normal activity following laparoscopic hernia repair. Surg Endosc 15(6):574–578. doi:10.1007/s004640080039[doi]
Pavlidis TE, Atmatzidis KS, Lazaridis CN, Papaziogas BT, Makris JG, Papaziogas TB (2002) Comparison between modern mesh and conventional non-mesh methods of inguinal hernia repair. Minerva Chir 57(1):7–12
Amid PK, Lichtenstein IL (1998) Long-term result and current status of the Lichtenstein open tension-free hernioplasty. Hernia 2:89–94
Quilici PJ, Greaney EM Jr, Quilici J, Anderson S (2000) Laparoscopic inguinal hernia repair: optimal technical variations and results in 1700 cases. Am Surg 66(9):848–852
Robertson GS, Burton PR, Haynes IG (1993) How long do patients convalescence after inguinal herniorrhaphy? Current principles and practice. Ann R Coll Surg Engl 75(1):30–33
Töns C, Muck-Töns A, Schumpelick V (1993) Leistenhernienchirurgie in Deutschland 1992: Eine Umfrage an 1656 deutschen Kliniken. Chirurg 64(8):635–641
Bachoo P, Duncan JL (1995) Prolonged convalescence following inguinal hernia repair: an unnecessary trend. Health Bull (Edinb) 53(4):209–212
Herzog U, Kocher T (1996) Leistenhernienchirurgie in der Schweiz 1994. Eine Umfrage an 142 Ausbildungskliniken in der Schweiz. Chirurg 67(9):921–926
van den Oever R, Debbaut B (1996) Kostenanalyse der Leistenhernienchirurgie bei ambulanter und stationärer Versorgung. Zentralbl Chir 121(10):836–840
Ciampolini J, Boyce DE, Shandall AA (1998) Adult hernia surgery in Wales revisited: impact of the guidelines of The Royal College of Surgeons of England. Ann R Coll Surg Engl 80(5):335–338
Kehlet H, Callesen T (1998) Recommendations for convalescence after hernia surgery. A questionnaire study. Ugeskr Laeger 160(7):1008–1009
Ismail W, Taylor SJ, Beddow E (2000) Advice on driving after groin hernia surgery in the United Kingdom: questionnaire survey. BMJ 321(7268):1056
Metzger J, Lutz N, Laidlaw I (2001) Guidelines for inguinal hernia repair in everyday practice. Ann R Coll Surg Engl 83(3):209–214
Rider MA, Baker DM, Locker A, Fawcett AN (1993) Return to work after inguinal hernia repair. Br J Surg 80(6):745–746
Callesen T, Klarskov B, Bech K, Kehlet H (1999) Short convalescence after inguinal herniorrhaphy with standardised recommendations: duration and reasons for delayed return to work. Eur J Surg 165(3):236–241. doi:10.1080/110241599750007108[doi]
Bay-Nielsen M, Perkins FM, Kehlet H (2001) Pain and functional impairment 1 year after inguinal herniorrhaphy: a nationwide questionnaire study. Ann Surg 233(1):1–7
Kumar S, Wilson RG, Nixon SJ, Macintyre IM (2002) Chronic pain after laparoscopic and open mesh repair of groin hernia. Br J Surg 89(11):1476–1479. doi:10.1046/j.1365-2168.2002.02260.x
Sajid MS, Leaver C, Baig MK, Sains P (2012) Systematic review and meta-analysis of the use of lightweight versus heavyweight mesh in open inguinal hernia repair. Br J Surg 99(1):29–37. doi:10.1002/bjs.7718
Kluivers KB, Hendriks JC, Mol BW, Bongers MY, Bremer GL, de Vet HC, Vierhout ME, Brolmann HA (2007) Quality of life and surgical outcome after total laparoscopic hysterectomy versus total abdominal hysterectomy for benign disease: a randomized, controlled trial. J Minim Invasive Gynecol 14(2):145–152. doi:10.1016/j.jmig.2006.08.009
Korolija D, Sauerland S, Wood-Dauphinee S, Abbou CC, Eypasch E, Caballero MG, Lumsden MA, Millat B, Monson JR, Nilsson G, Pointner R, Schwenk W, Shamiyeh A, Szold A, Targarona E, Ure B, Neugebauer E (2004) Evaluation of quality of life after laparoscopic surgery: evidence-based guidelines of the European Association for Endoscopic Surgery. Surg Endosc 18(6):879–897. doi:10.1007/s00464-003-9263-x
Le Blanc-Louvry I, Coquerel A, Koning E, Maillot C, Ducrotté P (2000) Operative stress response is reduced after laparoscopic compared to open cholecystectomy: the relationship with postoperative pain and ileus. Dig Dis Sci 45(9):1703–1713
McLauchlan GJ, Macintyre IM (1995) Return to work after laparoscopic cholecystectomy. Br J Surg 82(2):239–241
Ottesen M, Møller C, Kehlet H, Ottesen B (2001) Substantial variability in postoperative treatment, and convalescence recommendations following vaginal repair. A nationwide questionnaire study. Acta Obstet Gynecol Scand 80(11):1062–1068
Bokobza B (2002) Causes and mechanisms of recurrence after laparoscopic ventral hernia repair. In: Morales-Conde S (ed) Laparoscopic ventral hernia repair. Springer-Verlag, France, pp 451–461
Wara P, Bay-Nielsen M, Juul P, Bendix J, Kehlet H (2005) Prospective nationwide analysis of laparoscopic versus Lichtenstein repair of inguinal hernia. Br J Surg 92(10):1277–1281. doi:10.1002/bjs.5076[doi]
Bauer H, Fellmann E, Hermanek P, Hübner M, Jungnickel H, Kraas E, Ogasa J, Rückert K, Rümmelein D, Siefers H-F (2004) Leistenhernie. http://www.bqs-qualitaetsreport.de/2003/ergebnisse/leistungsbereiche/leistenhernie/. Accessed 28.12.2010
Ekman M, Johnell O, Lidgren L (2005) The economic cost of low back pain in Sweden in 2001. Acta Orthop 76(2):275–284
Hollinsky C, Göbl S (1999) Bursting strength evaluation after different types of mesh fixation in laparoscopic herniorrhaphy. Surg Endosc 13(10):958–961
Van’t Riet M, van Steenwijk De Vos PJ, Kleinrensink GJ, Steyerberg EW, Bonjer HJ (2002) Tensile strength of mesh fixation methods in laparoscopic incisional hernia repair. Surg Endosc 16(12):1713–1716. doi:10.1007/s00464-001-9202-7
Kumar A, Doran J, Batt ME, Nguyen-van-Tam JS, Beckingham IJ (2002) Results of inguinal canal repair in athletes with sports hernia. J R Coll Surg Edinb 47(3):561–565
Callesen T, Bech K, Nielsen R, Andersen J, Hesselfeldt P, Roikjaer O, Kehlet H (1998) Pain after groin hernia repair. Br J Surg 85(10):1412–1414. doi:10.1046/j.1365-2168.1998.00864.x[doi]
Gillion JF, Fagniez PL (1999) Chronic pain and cutaneous sensory changes after inguinal hernia repair: comparison between open and laparoscopic techniques. Hernia 3:75–80
Callesen T (2003) Inguinal hernia repair: anaesthesia, pain and convalescence. Dan Med Bull 50(3):203–218
Acknowledgments
The results were in part presented in the doctoral thesis of Mireille Untied (nee Lucht) at the University of Frankfurt in 2007 [20].
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Buhck, H., Untied, M. & Bechstein, W.O. Evidence-based assessment of the period of physical inactivity required after inguinal herniotomy. Langenbecks Arch Surg 397, 1209–1214 (2012). https://doi.org/10.1007/s00423-012-1008-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-012-1008-7