
Abstract
Purpose
The aim of this investigation was to determine the influence of endurance running on calcaneus bone stiffness in male and female runners.
Methods
A total of 122 marathoners (longer distance runners, men = 101; women = 21) and 81 half-marathon and 10-km runners (shorter distance runners; men = 48; women = 33), competing in an international running event, underwent an ultrasonographic assessment of the right and left calcaneus. Calcaneus bone stiffness was estimated using the measurements of the speed of sound (SOS) and broadband ultrasound attenuation (BUA). Seventy-five age-matched sedentary people served as the control group.
Results
Male and female longer distance runners and shorter distance runners presented higher values than sedentary counterparts in SOS (P < 0.05), and calcaneus stiffness (P < 0.05). Although there were no significant differences between longer distance and shorter distance runners in the ultrasonographic variables, longer distance runners presented greater effects size in SOS (1.00 vs 0.93 males; 1.10 vs 0.77 females), BUA (0.62 vs 0.25 males; 0.89 vs 0.20 females) and calcaneus stiffness (0.88 vs 0.66 males; 1.20 vs 0.60 females) than shorter distance endurance runners.
Conclusion
Calcaneus bone stiffness was higher in all endurance runners compared to a sedentary control population. The volume of ground reaction forces which occur during endurance running might induce the adaptation of the calcaneus bone.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
From a mechanical point of view, changes in bone mineral density and bone geometry are possible by inducing mechanical stimuli with external loadings and/or with loading forces during skeletal muscle contractions, although other non-mechanical factors also contribute to changes in bone density (Stabley et al. 2014). For this reason, exercise modalities requiring high muscular forces (such as resistance training) or generating high impacts (such as speed running and jumping) are regularly recommended to enhance bone mass and bone density (Schinkel-Ivy et al. 2014; Wilks et al. 2009). Nevertheless, not all exercise modalities have shown an osteogenic effect on healthy individuals.
Cross-sectional and longitudinal investigations indicate that weight-bearing exercise activities, that include the direct action of gravitational forces, produce greater bone adaptations (Guadalupe-Grau et al. 2009; Nikander et al. 2010; Tenforde and Fredericson 2011) than sports like swimming, water polo or rowing, that do not have measurable osteogenic benefits (Gomez-Bruton et al. 2014; Greene et al. 2012; Greenway et al. 2012). Moreover, sports with high ground reaction forces produce high muscle forces as the muscles lengthen at great speed during exercise actions and landing. Exercise activities that combine the mechanical stimulus from ground reaction forces and the tension produced by intense muscle contractions are considered better for bone stimulation (Ju et al. 2014). Since bone adaptation is limited to loaded regions (Guadalupe-Grau et al. 2009), the exercise modality has to be chosen to specifically act on the whole body or relevant sites (Kemmler et al. 2006). Based on these osteogenic criteria, running could be one of the most suitable exercise routines to preserve or to improve bone mineral stiffness and bone strength in healthy male and females. However, the outcomes of previous investigations on this topic are contradictory because either positive [e.g., increased bone mass and cross-sectional moments of inertia (Feldman et al. 2012)] or adverse bone adaptations [e.g., reduced bone mass and increased bone turnover (Hetland et al. 1993)] have been found when comparing endurance runners to healthy sedentary controls. Perhaps, the anatomical location of the bone adaptation assessment in these previous investigations is responsible for this inconsistency because the positive outcomes were found on tibia structure (loaded region during endurance running) while the negative bone adaptations were found on the lumbar spine and proximal femurs (less loaded region during running).
The study of bone mineral density in runners is an ideal scenario to investigate bone adaptations because the differences in training volume, running pace and stride length between sprinters and endurance runners provide different mechanical environments using the same exercise activity (e.g., running). Evidence suggests that sprinters typically present higher values of bone mineral density than endurance runners in both adult (Magkos et al. 2007) and master categories (Nowak et al. 2010; Wilks et al. 2009) probably due to higher impact loading protocols in sprinters versus endurance athletes. Recently, it has been suggested that bone mineral density depends on running distance because participants in short-distance disciplines presented higher values of bone mineral density than long-distance athletes (Gast et al. 2013). Specifically, the differences in bone density between short-distance runners and endurance runners were most marked at loaded-bearing regions (legs, hips and spine). However, all previous investigations (Gast et al. 2013; Nowak et al. 2010; Wilks et al. 2009) typically grouped endurance runners in the same category despite the differences in training volumes and running pace between shorter distance runners (e.g., 10-km runners) and longer distance runners (e.g., marathoners).
Therefore, the aim of this study was to assess bone ultrasonographic variables in different types of endurance runners to determine whether prolonged running constitutes an effective “mechanical stimulus” to produce measurable bone adaptations in a loaded region, e.g., calcaneus. A second aim was to determine whether endurance running training and calcaneus bone adaptations are related in a dose–response manner. For this purpose, we measured calcaneus bone stiffness in male and female runners of different endurance running disciplines. We hypothesized that longer distance runners (e.g., marathoners) would have increased calcaneus bone stiffness compared to shorter distance runners (e.g., 10-km and half-marathon runners).
Methods
Ethics statement
All participants were fully informed of any risks and discomforts associated with the experiments before giving their informed written consent to participate. The study was approved by the Camilo Jose Cela Ethics Committee in accordance with the latest version of the Declaration of Helsinki.
Participants
A total of 203 trained endurance runners and 75 healthy controls volunteered to participate in this investigation. The sample of endurance runners was recruited from the competitors in the Rock ‘n’ Roll Madrid Marathon & ½ Marathon while the control participants were recruited from the population of students and staff of the Camilo José Cela University. Endurance runner participants were divided into two groups according to their habitual competition distance: longer distance endurance runners (e.g., marathoners; men = 101, 41.0 ± 9.1 years; women = 21, 40.5 ± 8.0 years) and shorter distance endurance runners (e.g., ½ marathon and 10-km endurance runners; men = 48, 38.2 ± 10.4 years; women = 33, 37.1 ± 8.8 years; Table 1). Control participants (e.g., sedentary counterparts) were specially chosen to match age and sex of the endurance runners (men = 43, 38.6 ± 8.6 years; women = 32, 37.6 ± 7.6 years). Inclusion criteria for the control group included being mentally active, as evidenced by occupation or educational participation and sedentary behavior, and sedentary, as evidenced by <1 h of exercise per week. To determine the physical activity of the sedentary controls, participants filled out a questionnaire about daily physical activity routines and exercise. All the participants were healthy and were free of any musculoskeletal and metabolic disorders known to affect the bones. In the female population, pregnant participants, participants currently breastfeeding or with signs of amenorrhea were excluded from the study sample. Only Caucasian individuals were included in the study because the amount of data obtained from other races was insufficient to include race as a variable for the analysis. Participants’ information was obtained using personal interviews and questionnaires. Subjects were questioned regarding date of birth, training habits (including the type of shoe and whether they predominantly trained over soil, asphalt or track), previous medical conditions and injuries, and self-rated their habitual endurance discipline according to their routine training. Subjects unable to give a single self-rated best discipline were excluded from the study. Participants were then assigned to the longer distance runners group (e.g., marathoners), shorter distance runners group (half-marathon and 10 km) or sedentary counterparts according to their habitual competition distance. Information about their physical characteristics, training habits and running experience is shown in Table 1.
Experimental protocol
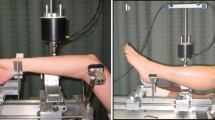
All the experimental procedures were performed 1–3 days before the participation in the running races. Participants’ height (Seca 213, Germany) and body mass were measured (Radwag, Poland) and the questionnaire was individually filled out to assess medical conditions, medication, previous injuries in the lower limbs, training habits and gynecological status (only in females). Once the inclusion criteria were fulfilled, participants underwent an ultrasonographic assessment of the calcaneus in the right and left feet using a bone scanner (Achilles, General Electric Health Care-Lunar, WI, USA). This scanner consisted of a control box, a heel waterbath and two transducers placed opposite each other at each side of the waterbath. A known ultrasound signal was sent from one fixed transducer throughout the waterbath with the heel in it and the ultrasound signal was subsequently received by the opposing fixed transducer. Signal parameters were digitized and sent to a computer for automated analysis. For this measurement, participants remained comfortably seated and their bare foot was placed in the waterbath. Expandable membranes were filled with warm water and isopropyl alcohol was used to provide coupling between the heel and the membranes, eliminating spaces with air.
During each ultrasonographic assessment, the speed of sound (SOS) and the broadband ultrasound attenuation (BUA) were directly measured while the calcaneus stiffness index was calculated as follows:
while SOS is a variable that assesses the elastic resistance of the bone (and it correlates with mineral and protein contents), BUA measures the loss of ultrasound energy occurred by absorption or dispersion (and it correlated with bone density; Cepollaro et al. 1995). Stiffness is achieved through the combination of SOS and BUA related to patient age. Previous investigations have obtained good validity and reliability results when using this instrument to measure the bone mineral density of the calcaneus with a coefficient of variation of 0.47 % for SOS, 2.6 % for BUA and 1.6 % for stiffness (Cepollaro et al. 1992; Toyras et al. 2002). Besides, a recent meta-analysis has indicated that quantitative ultrasound has an excellent sensitivity to assess exercise-induced changes in bone status (Babatunde and Forsyth 2013). If right-to-left calcaneus stiffness differed by more than 10 %, the assessment was repeated in both feet. Those participants with right-to-left stiffness differences higher than 10 % were excluded from the analysis. In each ultrasonographic measurement, T scores and Z scores for calcaneus stiffness were calculated using the reference population included in the manufacturer’s software. The individual T score represents the difference between the participant’s value for calcaneus stiffness and the mean value for a population of young adults of the same sex with peak bone mass (Gast et al. 2013). The individual Z score represents the difference between the participant’s value for calcaneus stiffness and the value of a sex- and age-adjusted population (Gast et al. 2013).
Statistical analysis
Initially, all the variables measured in the calcaneus (speed of sound, broadband ultrasound attenuation, and stiffness) were compared between right and left feet using Student’s t test for paired samples. All variables were very comparable in both feet (<1 % of variation), and thus, mean values for both feet were used for statistical analysis. Comparison between the three groups of subjects (longer distance runners, shorter distance runners and sedentary counterparts) for age, height, body mass, body mass index and training status was made using a one-way analysis of variance (ANOVA). Between-group differences in calcaneus ultrasound properties were performed using an ANCOVA with age, body mass and body mass index as covariates. Tukey’s post-hoc analysis was then used to identify differences between groups in these variables. Besides, we calculated the effect size in pairwise comparisons in reference to the control group according to the formula proposed by Glass et al. (1981). The magnitude of the effect size was interpreted using the scale of Cohen (1988): an effect size lower than 0.2 was considered small, an effect size around 0.5 was considered medium and an effect size over 0.8 was considered large. Male and female populations were analyzed separately because this investigation did not aim to investigate sex differences. We also performed a preliminary analysis of the effects of the type of shoes and the most habitual training surface on the differences between longer distance runners and shorter distance runners. These variables did not influence calcaneus density and were excluded from the analysis. Data are expressed as mean values ± standard deviation (SD). The significance level was set at α = 0.05. This statistical analysis was performed using the SPSS v.18 software package (SPSS Inc., USA).
Results
In males, longer distance runners and shorter distance runners did not significantly differ in age and height from their sedentary counterparts (Table 1). However, both groups of runners (longer and shorter distance) presented lower body mass and body mass index than the sedentary controls (P < 0.05). Male longer distance runners had a significantly higher training volume than shorter distance runners (P < 0.05), but they had similar running experience. In females, only shorter distance runners presented lower values for body mass and body mass index than the sedentary controls (P < 0.05). Female longer distance runners had a significantly higher training volume than female shorter distance runners but similar running experience.
Table 2 depicts mean values for calcaneus ultrasound properties in all three groups of participants for both male and female participants. In males, longer distance runners presented higher values for speed of sound, broadband ultrasound attenuation and calcaneus stiffness (P < 0.05) than their sedentary counterparts. Shorter distance runners had higher values for speed of sound and calcaneus stiffness than the sedentary controls (P < 0.05). However, there were no significant differences between the two groups of runners in the aforementioned variables. In females, longer distance runners also presented higher values for all ultrasonographic parameters when compared to the female sedentary controls (Table 2; P < 0.05) while shorter distance runners differed only in speed of sound and calcaneus stiffness (P < 0.05). Again, there were no differences between the two groups of runners in the calcaneus ultrasound properties. Mean T score and Z score values are shown in Fig. 1. In males, Z scores and T scores of both longer distance and shorter distance runners were significantly higher than the sedentary controls (P < 0.05). The same differences were found in the female population with longer distance runners and shorter distance runners presenting higher Z scores and T scores than female sedentary controls (P < 0.05). Again, there were no statistically significant differences between longer and shorter distance runners.

Calcaneus’ stiffness expressed as age- and sex-adjusted Z scores or peak bone mass sex-adjusted T scores in male and female shorter distance runners, longer distance runners and sedentary counterparts. *Significantly different from sedentary counterparts at P < 0.05
Discussion
The main purpose of this investigation was to assess bone adaptations induced by different types of endurance running, as measured by cross-sectional comparisons in calcaneus ultrasound properties between male and female runners of different endurance running disciplines (from 10 km to marathoners). The main results of our investigation were (a) both, longer distance and shorter distance endurance runners presented higher values for calcaneus stiffness than their sedentary counterparts (Table 2); (b) the adaptations in the calcaneus ultrasound properties produced by endurance training were of similar magnitude in men and women; (c) longer distance runners presented the highest values for calcaneus stiffness according to Z and T scores (Fig. 1) while these endurance runners had also the highest training volume per week (Table 1). All these results suggest that prolonged running produces a significant and positive bone adaptation in the calcaneus of endurance runners. Besides, it is likely that the higher volume of running per week present in long-distance runners is responsible for a greater calcaneus adaptation in this type of endurance runners.
Previous investigations have been geared to determine the influence of the mechanical stimuli produced during running on bone mineral density and bone strength (Bennell et al. 1997; Gast et al. 2013; Nowak et al. 2010; Wilks et al. 2009) because of the suitability of running to produce bone adaptations in young and adult individuals. In brief, these investigations have evidenced that sprint-type runners presented higher total body bone mineral density, especially in weight-bearing zones such as the legs, hip, lumbar spine and trunk, than endurance-trained runners (Gast et al. 2013). However, endurance running disciplines include races from 5-km to ultraendurance events of 100 km. Thus, the mechanical stimuli for bone adaptation can be very different among endurance runners.
In the present investigation, we compared calcaneus bone stiffness in male and female long-distance runners (marathoners) to short-distance endurance runners (half-marathoners and 10 km). Participants in these groups had comparable age, anthropometric characteristics and running experience, but long-distance runners presented higher values of training volume, as measured by running distance per week (Table 1). Interestingly, both groups of runners presented higher speed of sound, broadband ultrasound attenuation and calcaneus stiffness than age- and sex-matched sedentary controls (Table 2; Fig. 1). These data suggest that endurance running training promotes bone adaptation in the calcaneus inducing a higher stiffness and strength, as previously found for the tibia (Feldman et al. 2012).
Although there were no statistically significant differences between longer distance and shorter distance runners in the ultrasonographic variables studied, the effect size obtained by longer distance training was always superior to the effect size for shorter distance endurance training. When compared to sex- and age-matched sedentary controls, male longer distance runners presented greater effect sizes in SOS (1.00 vs 0.93), BUA (0.62 vs 0.25) and calcaneus stiffness (0.88 vs 0.66) than shorter distance endurance runners. In female participants, longer distance runners also presented greater effect sizes in SOS (1.10 vs 0.77), BUA (0.89 vs 0.20) and calcaneus stiffness (1.20 vs 0.60) than shorter distance runners. These results indicate that the volume of endurance training might exert a progressive adaptation in calcaneus bone stiffness. Furthermore, these results are in concordance with the traditional mechanostat theory proposed by Frost (1987) since a higher volume of mechanical stimuli during running tended to produce superior bone adaptations (Nikander et al. 2010).
The Z and T scores provide a unique insight into investigating the impact of different sport types compared to a reference population (Tveit et al. 2014). These scales provide a fair comparison of an individual’s bone mineral density to his/her sex-matched young reference of peak bone mass (T score) and his/her expected age-adjusted value (Z score). Because the group of longer distance runners reported higher training volumes of weight-bearing physical activity (e.g., running), as measured per km week−1, it might be expected that they would show a slightly better calcaneus bone density than the general population and runners with lower training volumes. The data presented in Fig. 1 indicate that endurance running training increases calcaneus stiffness when compared to a population at peak bone mass age (T score) and to an age-matched population (Z score). Moreover, the effect size also suggests that the higher the training volume, the higher the increases over Z and T scores in both male and female individuals.
The current experimental design presents some limitations and they should be summarized to improve the comprehension of the main outcomes found in this investigation. First, this is a cross-sectional study that investigates the effects of endurance training disciplines on calcaneus bone stiffness. Cross-sectional investigations have less validity than longitudinal studies because there still remains the possibility that greater calcaneus bone density in longer distance runners could be the result of factors not associated with this investigation. Second, this investigation is focused on the calcaneus while it is likely that endurance running training induces bone adaptation in legs and trunks. Thus, the examination of bone changes induced by endurance running training should be expanded to other body areas using dual-energy X-ray absorptiometry. Third, we did not control the diet or the nutritional status of the participants in this investigation. Thus, it remains the possibility that some of the differences found in this investigation are related to the diet of the runners versus their sedentary controls (Welch and Rosen 2005). In the authors’ opinion, these limitations do not hinder the main outcomes and applicability of the investigation.
In the current investigation, several ultrasonographic variables measured in the calcaneus presented greater values in endurance runners when compared to sedentary counterparts (Welch and Rosen 2005). Thus, it can be suggested that prolonged running produces a significant bone adaptation in the calcaneus of endurance runners (Kemmler et al. 2006). Besides, the effect size in calcaneus bone stiffness, speed of sound and broadband ultrasound attenuation in longer distance runners (marathoners) was superior to endurance runners of shorter disciplines such as 10 km and half-marathon. It is likely that the higher volume of running per week present in marathoners induced an enhanced calcaneus adaptation when compared to the remaining endurance runners. Endurance running might be used to improve areal bone mineral density and the higher the distance covered per week the better the bone adaptations. Finally, improvements in bone mineral stiffness with endurance running were of similar magnitude in male and female runners.
Abbreviations
- ANOVA:
-
Analysis of variance
- ANCOVA:
-
Analysis of covariance
- BUA:
-
Broadband ultrasound attenuation
- SD:
-
Standard deviation
- SOS:
-
Speed of sound
References
Babatunde OO, Forsyth JJ (2013) Quantitative ultrasound and bone’s response to exercise: a meta analysis. Bone 53:311–318
Bennell KL, Malcolm SA, Khan KM, Thomas SA, Reid SJ, Brukner PD, Ebeling PR, Wark JD (1997) Bone mass and bone turnover in power athletes, endurance athletes, and controls: a 12-month longitudinal study. Bone 20:477–484
Cepollaro C, Zacchei F, Borracelli D (1992) Precision of new ultrasound bone densitometers: correlation with absorptiometry methods. In: Proceedings of ultrasonic assessment of bone II, symposium. Harwell Biomedical Research, Bath England
Cepollaro C, Agnusdei D, Gonnelli S, Martini G, Pondrelli C, Borracelli D, Palmieri R, Parisi G, Gennari C (1995) Ultrasonographic assessment of bone in normal Italian males and females. Br J Radiol 68:910–914
Cohen J (1988) Statistical power analysis for the behavioral sciences. Lawrence Erlbaum Associates, Hillsdale
Feldman S, Capozza RF, Mortarino PA, Reina PS, Ferretti JL, Rittweger J, Cointry GR (2012) Site and sex effects on tibia structure in distance runners and untrained people. Med Sci Sports Exerc 44:1580–1588
Frost HM (1987) Bone “mass” and the “mechanostat”: a proposal. Anat Rec 219:1–9
Gast U, Belavy DL, Armbrecht G, Kusy K, Lexy H, Rawer R, Rittweger J, Winwood K, Zielinski J, Felsenberg D (2013) Bone density and neuromuscular function in older competitive athletes depend on running distance. Osteoporos Int 24:2033–2042
Glass G, McGaw B, Smith M (1981) Meta-analysis in social research. Sage, Newbury Park
Gomez-Bruton A, Gonzalez-Aguero A, Gomez-Cabello A, Matute-Llorente A, Casajus JA, Vicente-Rodriguez G (2014) The effects of swimming training on bone tissue in adolescence. Scand J Med Sci sports. doi:10.1111/sms.12378
Greene DA, Naughton GA, Bradshaw E, Moresi M, Ducher G (2012) Mechanical loading with or without weight-bearing activity: influence on bone strength index in elite female adolescent athletes engaged in water polo, gymnastics, and track-and-field. J Bone Miner Metab 30:580–587
Greenway KG, Walkley JW, Rich PA (2012) Does long-term swimming participation have a deleterious effect on the adult female skeleton? Eur J Appl Physiol 112:3217–3225
Guadalupe-Grau A, Fuentes T, Guerra B, Calbet JA (2009) Exercise and bone mass in adults. Sports Med 39:439–468
Hetland ML, Haarbo J, Christiansen C (1993) Low bone mass and high bone turnover in male long distance runners. J Clin Endocrinol Metab 77:770–775
Ju YI, Sone T, Ohnaru K, Tanaka K, Yamaguchi H, Fukunaga M (2014) Effects of different types of jump impact on trabecular bone mass and microarchitecture in growing rats. PLoS One 9:e107953
Kemmler W, Engelke K, Baumann H, Beeskow C, von Stengel S, Weineck J, Kalender WA (2006) Bone status in elite male runners. Eur J Appl Physiol 96:78–85
Magkos F, Yannakoulia M, Kavouras SA, Sidossis LS (2007) The type and intensity of exercise have independent and additive effects on bone mineral density. Int J Sports Med 28:773–779
Nikander R, Kannus P, Rantalainen T, Uusi-Rasi K, Heinonen A, Sievanen H (2010) Cross-sectional geometry of weight-bearing tibia in female athletes subjected to different exercise loadings. Osteoporos Int 21:1687–1694
Nowak A, Straburzynska-Lupa A, Kusy K, Zielinski J, Felsenberg D, Rittweger J, Karolkiewicz J, Straburzynska-Migaj E, Pilaczynska-Szczesniak L (2010) Bone mineral density and bone turnover in male masters athletes aged 40–64. Aging Male 13:133–141
Schinkel-Ivy A, Burkhart TA, Andrews DM (2014) Differences in distal lower extremity tissue masses and mass ratios exist in athletes of sports involving repetitive impacts. J Sports Sci 32:533–541
Stabley JN, Moningka NC, Behnke BJ, Delp MD (2014) Exercise training augments regional bone and marrow blood flow during exercise. Med Sci Sports Exerc 46:2107–2112
Tenforde AS, Fredericson M (2011) Influence of sports participation on bone health in the young athlete: a review of the literature. PM & R J injury Funct Rehabil 3:861–867
Toyras J, Nieminen MT, Kroger H, Jurvelin JS (2002) Bone mineral density, ultrasound velocity, and broadband attenuation predict mechanical properties of trabecular bone differently. Bone 31:503–507
Tveit M, Rosengren BE, Nilsson JÅ, Karlsson MK (2014) Exercise in youth: high bone mass, large bone size, and low fracture risk in old age. Scand J Med Sci Sports 25(4):453–461
Welch JM, Rosen CJ (2005) Older women track and field athletes have enhanced calcaneal stiffness. Osteoporos Int 16:871–878
Wilks DC, Winwood K, Gilliver SF, Kwiet A, Chatfield M, Michaelis I, Sun LW, Ferretti JL, Sargeant AJ, Felsenberg D, Rittweger J (2009) Bone mass and geometry of the tibia and the radius of master sprinters, middle and long distance runners, race-walkers and sedentary control participants: a pQCT study. Bone 45:91–97
Acknowledgments
The authors wish to thank the subjects for their invaluable contribution to the study. In addition, we are very grateful to the Organization of the Rock ‘n’ Roll Madrid Marathon & ½ Marathon for their contribution to the study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest derived from the outcomes of this study.
Additional information
Communicated by Olivier Seynnes.
Rights and permissions
About this article

Cite this article
Lara, B., Salinero, J.J., Gutiérrez, J. et al. Influence of endurance running on calcaneal bone stiffness in male and female runners. Eur J Appl Physiol 116, 327–333 (2016). https://doi.org/10.1007/s00421-015-3285-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-015-3285-7