
Abstract
The aim of our study was to compare long distance runners to body mass index (BMI)- and age-matched healthy controls with respect to bone parameters at all relevant loaded and nonloaded skeletal sites. Furthermore, we assessed the effect of running volume on bone parameters. Twenty elite male runners (21.1 km<1:15 h; volume >75 km/week/year) participated in the study (RG), 11 age- and BMI-matched male subjects (28±5 years) served as nontraining controls (CG). Subjects with any medication or illness affecting bone metabolism or with a family history of osteoporosis were not included. Bone parameters at various sites (total body, lumbar spine, femoral neck/hip, calcaneus) were measured by dual energy X-ray (DXA), quantitative computed tomography and quantitative ultrasound. Body composition was assessed via DXA and bioimpedance analysis; nutritional parameters were determined by 5-day dietary protocols. Training variables were assessed by questionnaires. Compared with nontraining controls runners had significantly higher BMD at all loaded sites (calcaneus, lower limbs, femoral neck, pelvis, and trabecular lumbar spine). BMD at nonloaded sites (ribs, upper limbs, and skull) was slightly but not significantly higher in the runners. We observed a low (r=0.30), nonsignificant association between training volume (km/week/year) and trabecular BMD of the femoral neck, which disappeared after adjusting for age, BMI, and body fat in this group of highly trained male runners. The effect of long distance running per se on bone parameters is not deleterious.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The popularity of recreational and competitive long distance running has increased over the last decades. Its positive impact on the cardiovascular system is generally accepted; however, its effect on bone parameters at loaded and nonloaded sites is still under discussion because endurance exercises may affect bones by anabolic and catabolic pathways.
Studies comparing male long-distance runners with “untrained” controls showed rather heterogeneous effects on BMD. Potential reasons are the major differences in recruitment, exclusion criteria, measurement techniques, and sample sizes. For example, exercise and physical activity of the study subjects varied widely; often the sedentary status of the control group was questionable (Bennell et al. 1997). Further, the majority of the studies with male runners (Bennell et al. 1997, Bilanin et al. 1989, Brahm et al. 1997, Goodpaster et al. 1996, Greene et al. 2004, Hetland et al. 1993, MacDougall et al. 1992, Michel et al. 1992, Nevill et al. 2003, Stewart and Hannan 2000) did not match regarding anthropometric parameters. Since age, weight, body mass index (BMI), or lean body mass (LBM) are significant predictors of BMD in males (Douchi et al. 2003) this deficit may have resulted in a severe bias. Thus, it is difficult to judge whether differences in bone parameters could predominantly be attributed to the exercise status.
Furthermore, most studies (Brahm et al. 1997, Hetland et al. 1993, MacDougall et al. 1992) reported negative associations between the running volume (i.e., min/week or km/week) and BMD. However, these studies included subjects with rather low running volume (i.e., joggers). Taking into account that these subjects may participate in other fitness activities with higher osteoanabolic impact (i.e., games, resistance exercise), the negative effect of running volume on BMD will be overestimated.
In this study we wanted to determine the isolated effect of long distance running on bone parameters at different mechanically loaded or nonloaded sites. We hypothesized that for runners, bone parameters at loaded sites were significantly higher compared with age- and BMI-matched untrained controls. Furthermore, we speculate that running volume did not relevantly affect bone parameters in this homogeneous group of sub-elite runners. In order to verify our hypothesis, two groups, one of elite runners and the other of nontraining controls were matched for parameters known to affect bone (Douchi et al. 2003). Bone parameters were assessed at all skeletal sites using different techniques.
Materials and methods
Subjects
Twenty endurance trained male runners and 11 age- and BMI-matched controls (age: 20–35 years) participated in the study. The runners were recruited by the Bavarian record list. Inclusion criteria were a running history of at least 5 years, a running volume of more than 75 km per week (>46.6 miles/week) during the complete year, and a time of less than 1.15 h for a semi-marathon (or <32:30 min for 10,000 m). Inclusion criteria for the controls were low sportive activity (≤2 h exercise/week) during the last 5 years, no sport activities with moderate or high osteoanabolic impact (Kemmler et al. 2004) during lifetime, and an energy intake ≥130 kJ/kg body weight. All participants were free of past or present diseases and medications affecting bone metabolism. No subject showed a family history of osteoporosis. Four controls were cigarette smokers, while none of the runners had ever smoked.
The study was approved by the ethics committee of the University of Erlangen (Ethik Antrag 2691), the Bundesamt für Strahlenschutz (Z 2.1.2-22462/2-2002-005), and the Bayerisches Landesamt für Arbeitsschutz (13B/3443-4/5/02). All study participants gave written informed consent.
Anthropometric data
We measured height, weight, BMI, and body composition. BMI was calculated from weight and height (kg/m2).
Bone densitometry and body composition
Dual energy X-ray absorptiometry
Total and regional body composition was determined by whole body dual energy X-ray absorptiometry (DXA, QDR 4500A Hologic, Bedford, MA, USA). For DXA the following subregions of the total body scan were included in the analysis: skull, arms, thoracic and lumbar spine, ribs, pelvis, and legs. DXA was also used to measure whole body BMD. Coefficient of variation (CV) for the total body BMD scan was 0.9%.
Quantitative computed tomography
Quantitative computed tomography (QCT) was performed at the lumbar spine (L1–L3) and the proximal femur (Somatom Volume Zoom, Siemens, Erlangen, Germany). At the spine, BMD was determined in 10-mm thick slices of L1 to L3 each using the OsteoCT protocol (Kalender et al. 1987). CV for the LS-QCT scan was 2.1%. The CT images were also used to determine the width of the vertebral body in anterior–posterior and in lateral direction. At the hip a spiral scan and 3D analysis protocol recently developed in our Institute (Kang 2003) was used to measure the cross-sectional area, BMD, and cortical thickness of the femoral neck (Fig. 1).

QCT of the proximal femur. The figures show three orthogonal views (axial, sagittal, transversal) of the 3D volume. Periosteal and endosteal bone surfaces are outlined. The neck VOI is indicated by the black bold border. The direction of the neck axis is indicated by the arrow. The image on the lower right is a cut perpendicular to the neck axis through the femoral head
Quantitative ultrasound
Broadband ultrasound attenuation (BUA) and speed of sound (SOS) were measured with quantitative ultrasound (QUS) at the calcaneus (Sahara, Hologic). In vivo precision (CV) was 0.4% for SOS and 3.6% for BUA.
Questionnaires
A detailed questionnaire completed by all study subjects combined several parts: (1) osteoporotic risk factors, including diseases, medications, and family history of osteoporosis. (2) recent (last 5 years) and present physical activity and exercise levels (Kemmler 2000, Kemmler et al. 2004); (3) nutritional behavior.
In addition, for the runners’ group specific exercise parameters such as years of exercising, running volume, average running speed, and records on various distances were asked.
Nutritional analysis
The individual dietary intake was assessed by a 5-day protocol completed by the participants after being carefully instructed. For precise weighing of the consumed food, participants were given identical digital household scales. The analysis of the protocols was performed in collaboration with the University of Bayreuth, using Prodi-4,5/03 Expert software. This program extracts a total of 1,500 different basic nutritional ingredients. The precision of the analysis for energy, fat, carbohydrate, protein, calcium, phosphorous, and vitamin D intake was high, demonstrated by coefficients of variance smaller than 5% (Kemmler 2003). In this contribution we predominately focused on parameters relevant for bone.
Statistical analysis
All measured values are reported as means and standard deviations. The Kolgomorov–Smirnov test was used to check for normal distribution. Homogeneity of variance was investigated using Levine’s F test. For normally distributed variables, differences between groups were assessed with independent t tests, otherwise the Mann–Whitney U test was used. Simple and stepwise multiple linear regression analyses were performed to determine the association between bone and independent parameters. All tests were two-tailed, a 5% probability level was considered significant (*). We used SPSS 12.0 (SPSS Inc, Chicago, IL, USA) for our statistical analysis.
Results
Table 1 shows the physical and training characteristics of the study subjects. As a result of matching no significant differences for age, height, weight, and BMI could be observed between the groups. Although BMI was slightly lower in the control group (CG), body-fat (%) analyzed by DXA was significantly higher in the controls compared with the runners (12.7 vs. 10.9%). Average annual running volume in the athletes group was 555 min/week; average speed was 13.2 km/h resulting in a weekly distance of ≈120 km. All the athletes used periodized regimes with distinct variations of running volume and speed during the course of a year. In contrast four participants of the control group did not exercise at all during the last 5 years. Five subjects exercised in sports with low osteoanabolic impact (cycling, swimming, inline skating) for 30–120 min/week during this period and two controllers started recreational sport activities (inline skating) during the last 5 years. No subject of the control group has a history of competitive exercise.
Table 2 shows the results of the 5-day dietary intake analysis. All values were higher in the runners group although not all differences reached significance. Regarding high running, the volume of fluid intake was rather low in the runners group. Except for vitamin D intake, which was below the NIH recommendation (Standing committee on the Scientific Evaluation of Dietary Reference Intakes 1997) of 5 μg/day (200 IU/D), the intake of nutritional parameters relevant to bone was in the range of present recommendations for both groups (Clarkson et al. 1995; Standing committee on the Scientific Evaluation of Dietary Reference Intakes 1997).
Table 3 shows the DXA total body measurements. In accordance with Nevill et al. (2003) we did not observe a difference between the dominant and nondominant sides in the extremities, thus the BMD of these regions was averaged based on BMC/area values. Total-body (TB) BMD was significantly higher in the runners´ group. The TB mean T score of the athletes was 0.9±0.8 SD compared with a T score of −0.2±0.7 SD in the controls (P<0.01). However, regarding the various regions of interest (ROI), the differences between the runners and controls were rather heterogeneous. Although BMD at all skeletal sites was higher in the runners´ group, significant results could be demonstrated only for the pelvis and the lower extremities (Table 3).
The QCT results of the lumbar spine assessment are presented in Fig. 2. Trabecular BMD of the lumbar spine was significantly higher in the runners compared with the nontraining controls (Fig. 2a; 162.7 vs. 140.0 g/cm3). Correspondingly the trabecular LS T score of the runners (0.2±0.7 SD) was significantly higher (P<0.05) compared with the controls (-0.5±0.8 SD). No further significant differences could be observed for the cortical BMD of the LS (Fig. 2b; 318.1 vs. 319.6 g/cm3) and the anthropometrical dimensions (Fig. 2c; width and Fig. 2d; depth) of the lumbar spine.

BMD (upper panels) and geometry (lower panels) of the lumbar spine measured by QCT
Cross sectional area (CSA), BMD, and cortical thickness of the femoral neck as assessed by QCT are given in Fig. 3a–c. Significant differences could be demonstrated for total (Fig. 3 a, 448.5 vs. 370.1 g/cm3) and trabecular (Fig. 3b; 310.6 vs. 226.2 g/cm3) BMD of the femoral neck. Differences for cortical BMD (Fig. 3c; 713.4 vs. 669.1 g/cm3) and minimum CSA (877.3 vs. 845.3 mm2) did not reach statistical significance. Cortical thickness of the femoral neck did not differ (2.64 mm) between both groups.

BMD of the femoral neck measured by QCT
Figure 4 shows the ultrasound results at the calcaneus. Differences between the runners and controls were significantly for both parameters: SOS (Fig. 4a; 1605 vs. 1536 m/sec) and BUA (Fig 4b; 100.2 vs. 67.9 dB/mHz).

SOS (left panel) and BUA (right panel) measured by QUS at the calcaneus
In the runners group the relationship between the running volume and BMD was determined at various skeletal sites using simple and multivariate regression analysis. Results from simple regression analysis were all nonsignificant ranging from negligible to small (|r|<0.15 for US, QCT-LS, and DXA; r=0.34, for cortical thickness of the femoral neck; r=- 0.30 for trabecular BMD of the femoral neck) and further decreased after adjusting for age, BMI, and total body fat in the multiple regression models.
Discussion
The main objective of our study was to determine whether in young males long distance running has a negative effect on bones. We recruited a cohort of young male runners with high training volume and compared this group with healthy age- and BMI-matched nontraining controls. We performed bone densitometry at various loaded and nonloaded skeletal sites but did not detect any decrease of BMD or other important bone parameters. On the contrary, BMD as measured by total body DXA was higher in the runners group in the pelvis and the legs. Also trabecular BMD of the spine and femoral neck measured by QCT and SOS and BUA at the calcaneus measured by QUS were higher in the runners than in the control group. Thus, our study clearly shows that in young males, long distance running does not have a detrimental effect on bone.
Our study possesses several strengths. (1) In contrast to most other studies, with the exception of body fat, runners and control were well matched for anthropometric variables (Table 1) known to significantly affect bone (Douchi et al. 2003). Regarding anthropometric factors, we decided to match for BMI and not for body fat. As expected, this procedure leads to a significantly higher body fat content in the CG. However, as stated by Douchi et al. (2003) body fat is a negligible BMD determinant in males. Thus, the significance between group differences for body fat (%) should not relevantly affect our results. Controls with inadequate energy intake (<130 kJ/kg body weight) were not included in the analysis. Thus differences for bone parameters could largely be attributed to the exercise status of the subjects. (2) Subjects with a history of diseases and medications with an impact on bone metabolism or a family history of osteoporosis were excluded. (3) Further, subjects who had exercised more than 2 h/week during the 5 years preceding the study or had carried out activities with moderate to high osteoanabolic impact (Kemmler et al. 2004) were not included in the control group. Five controls exercised in disciplines that were known to be associated with low BMD (swimming, cycling) (Morel et al. 2001). However, in contrast to athletes the volume of these activities was rather low (30 to <120 min/week), thus we do not expect exercise-induced negative effects in our controls. Although the accuracy of activity recall questionnaires per se may be limited, the recall of vigorous activities is adequately accurate (Blair et al. 1991) to classify our controls. (4) The runners group was very homogeneous: it consisted of ambitious sub-elite long distance runners with training volumes >75 km/week/year (5) Nutritional intake was assessed by 5-day dietary protocols. Regarding parameters with impact on bone, both groups were in the range of current recommendations (Clarkson et al. 1995, Standing committee on the Scientific Evaluation of Dietary Reference Intakes 1997). Furthermore, except in two parameters (carbohydrates and magnesium intake), we could not demonstrate significant differences between runners and controls. However, four smokers were identified in the control group. Although we do not think our results were affected by this, smoking may account for some reduction of BMD in the controls. (6) Bone densitometry was carried out at various skeletal sites and with three different techniques: QCT, DXA, and ultrasound. Thus, different facets of bone strength could be determined.
A limitation of the study is its relatively small sample size of the control group. Indeed, it was difficult to recruit a large amount of subjects with low BMI, who were healthy, without medication and eating disorders, and sedentary but willing to participate in a study assessing body composition by X-ray densitometry. However, as mentioned above, we think it is essential for both groups to be highly comparable for confounding factors.
Due to the cross-sectional nature of the study it is difficult to judge whether selection bias (i.e., subjects with “genetically” higher BMD may be predisposed for elite running due to lower injury rates) may affect our results. However, regarding the skull as a reference for a region that is most unlikely to be affected by running, BMD did not differ between both groups.
Comparing our results with those from the other studies in male runners (Aloia et al. 1978, Bennell et al. 1997, Bilanin et al. 1989, Brahm et al. 1997, Chae et al. 1994, Dalen et al. 1974, Greene et al. 2004, Hamdy et al. 1994, Hetland et al. 1993, MacDougall et al. 1992, Mussolino et al. 2001, Nevill et al. 2003, Nilsson and Westlin 1971, Stewart and Hannan 2000) is not easy due to variations in age, running volume, anthropometric variables, exercise status of the control group, and measurement techniques.
Results across studies (Bennell et al. 1997, Brahm et al. 1997, Dalen et al. 1974) are rather homogenous regarding feet, a site substantially affected by running. Indeed, independent of the measurement technique, bone parameters in runners were always significantly higher than those of the controls. Similarly, in the lower limbs (tibia, femur) and the proximal femur, with one exception (Hetland et al. 1993), existing studies (Bennell et al. 1997, Bilanin et al. 1989, Brahm et al. 1997, Chae et al. 1994, Dalen et al. 1974, MacDougall et al. 1992, Nevill et al. 2003, Nilsson and Westlin 1971, Stewart and Hannan 2000) reported higher BMD values in runners that were most often significant. For example, BMD in the femoral neck as measured by DXA was 3–13% higher than in controls.
In addition to total body DXA in the femoral neck we used QCT to further differentiate trabecular and cortical BMD and to determine geometrical parameters such as the minimum cross-sectional neck area (CSA) and the cortical thickness. Total BMD of the femoral neck was 22% (P<.001) higher in the runners group. This difference is predominantly caused by a difference in trabecular BMD (37%, P<.001) which is more sensitive to the compressive type of strain induced by running, but in our opinion the difference in cortical BMD (7%, P=.07), although not significant, is also relevant. Interestingly, there was no difference in cortical thickness or in diameter. In contrast, in tennis players the increase in bone strength at the dominant compared to the nondominant side is induced by geometric adaptation and not by higher density (Ashizawa et al. 1999, Haapasalo et al. 2000). Obviously, here two sites within subjects were compared and almost all the subjects included in these studies started playing during childhood or early adolescence, whereas the majority of our subjects started exercising after the growth spurt. However, it is well known that the mechanism of bone adaptation differs between young and mature bone (Haapasalo et al. 1996). In childhood and during adolescence, loading results in larger bone size due to periosteal and endosteal expansion while in mature bones the increment of bone density may be the primary mechanism to strengthen the bone (Haapasalo et al. 2000).
Interestingly, the majority of studies with male runners focuses on the lumbar spine (Bennell et al. 1997, Bilanin et al. 1989, Brahm et al. 1997, Chae et al. 1994, Dalen et al. 1974, Goodpaster et al. 1996, Hamdy et al. 1994, Hetland et al. 1993, Lane et al. 1986, MacDougall et al. 1992, Michel et al. 1992, Stewart and Hannan 2000). The results are extremely heterogeneous, differences between runners and controls varied from significantly higher (QCT, BMD L1: +44% (Lane et al. 1986)) to significantly lower (DXA, BMC L2-L4: -19% (Hetland et al. 1993)) values. However, a closer inspection of these studies (Bilanin et al. 1989, Goodpaster et al. 1996, Hetland et al. 1993) which showed lower results in the runners` groups reveales that the control groups were not adequately matched because the controls had significantly higher values for weight, BMI and/or body fat. Furthermore the sedentary status of the control group in the studies of Goodpaster et al. (1996) and Hetland et al. (1993) is not ensured. Although participating less in weight lifting and ball games, controls of Hetland et al. (1993) spent on average 4.4 h/week on nonrunning sports activity.
Our results at the spine measured by total body DXA were slightly but not significantly higher (+7%) in the runners group. A more differential assessment again by using QCT showed a significant higher value of 15% trabecular BMD but no differences in cortical BMD or vertebral dimensions. Thus the mechanical impact of the running exercise still affects the lumbar spine. The relative contribution of axial gravitational forces impacting directly on the bone and muscle tension which stabilized the spine while running still needs to be determined although our results indicate some contribution of the muscle system. In the runners` group we found positive correlations between LBM and osteodensitometric parameters of the lumbar and thoracic spine ranging from r=0.34 (n.s., trabecular BMD, QCT) to r=0.63 (P<.001; thoracic spine, total body DXA) whereas we found no correlations in the control group.
For other non- or less mechanically stimulated skeletal sites (ribs, skull, humerus, and arms), that we analyzed using total body DXA, we found slight but nonsignificant higher BMD values in the runners group (see Table 3). Thus we do not confirm the hypothesis of catabolic effects at nonloaded skeletal sites (“steal effects”) caused by a negative hormonal milieu (Haapasalo et al. 2000).
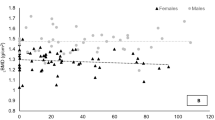
For reasons extensively discussed we do not compare the runner group with normative values of young “normal” adults. However, using the T score of the total body BMD measurement, all but three subjects were above the mean of an age-matched reference population supplied by the DXA manufacturer (white males, 25 years; mean: 1.15 g/cm2; 1 SD±0.094 g/cm2). At the spine trabecular BMD of all but one runner was within or above the ±1 SD range of the normal population (white males, 25 years; 160±26 mg/cm3, (Kalender et al. 1989)).
We also detected only nonsignificant to weak correlations between training volume and bone parameters in this elite runners` group but we must point out that our study has the limitation that only highly trained male athletes with training volumes exceeding 75 km/week/year were included. Other studies investigating the effect included male runners with more heterogeneous training volume: 0–160 km/week (Hetland et al. 1993), 2–12 h/week (Brahm et al. 1997), and 8–120 km/week (MacDougall et al. 1992). All these studies found negative relationships between training volume and BMD at least at one skeletal site. For example, MacDougall et al. (1992) reported that leg, but not total body, spine, or trunk BMD “tended to decrease” with mileages >32 km/week.
Again it must be remembered that results must be properly adjusted for anthropometric parameters such as weight, BMI, and LBM. This is particularly important if BMC instead of BMD is used as the dependent variable. For example the significant correlations between BMC determined by total body DXA and training volume reported by Hetland et al. (1993) became nonsignificant after adjustment for age and BMI. Even in our runners` group with a rather low variance of BMI or weight, the correlation between BMI or weight and BMD (TB-DXA, LS-QCT, LS-DXA) was significant, ranging between r=0.44 and 0.62.
In summary, our results show that in male runners bone parameters at loaded sites were higher compared to healthy age- and BMI-matched nontraining controls. Furthermore, we could not observe negative effects at nonloaded sites. Variation of running volume at high training levels did not correlate with bone parameters.
However, we do not suggest that our results are transferable to female long distance runners. We speculate that there are sex-specific differences concerning the sensibility of the reproductive system to stress and bones sensitivity to hormonal disturbances.
References
Aloia JF, Cohn SH, Bab T, et al (1978) Skeletal mass and body composition in marathon runners. Metabolism 27:1793–1796
Ashizawa N, Nonaka K, Michikami S, Mizuki T, Amagai H, Tokuyama K, Suzuki M (1999) Tomographical description of tennis-loaded radius: reciprocal relation between bone size and volumetric BMD. J Appl Physiol 86:1347–1351
Bennell KL, Malcolm SA, Khan KM, Thomas SA, Reid SJ, Brukner PD, Ebeling PR, Wark JD (1997) Bone mass and bone turnover in power athletes, endurance athletes, and controls: a 12-month longitudinal study. Bone 20:477–484
Bilanin JE, Blanchard MS, Russek-Cohen E (1989) Lower vertebral bone density in male long distance runners. Med Sci Sports Exerc 21:66–70
Blair SN, Dowda M, Pate RR, Kronenfeld J, Howe HG Jr., Parker G, Blair A, Fridinger F (1991) Reliability of long-term recall of participation in physical activity by middle-aged men and women. Am J Epidemiol 133:266–275
Brahm H, Strom H, Piehl-Aulin K, Mallmin H, Ljunghall S (1997) Bone metabolism in endurance trained athletes: a comparison to population-based controls based on DXA, SXA, quantitative ultrasound, and biochemical markers. Calcif Tissue Int 61:448–454
Chae AE, Platen P, Antz R, Kühlmorgen J, Allolio B, Lehmann H, Schuhmann S, Kannenberg J (1994) Knochendichte bei Leistungssportler/innen aus verschiedenen Sportarten im Vergleich zu Sportstudent/innen und untrainierten Kontrollpersonen. In: Liesen H, Weiß M, Baum M (eds) Regulations- und Repaimechanismen. Springer, Paderborn, Germany
Clarkson PM, Hayes EM (1995) Exercise and mineral status of athletes: calcium, magnesium, phosphorus, and iron. Med Sci Sports Exerc 27:831–843
Dalen N, Olsson KE (1974) Bone mineral content and physical activity. Acta Orthop Scand 45:170–174
Douchi T, Kuwahata R, Matsuo T, Uto H, Oki TYN (2003) Relative contribution of lean and fat mass component to bone mineral density in males. J Bone Miner Metab 21:17–21
Goodpaster BH, Costill DL, Trappe SW, Hughes GM (1996) The relationship of sustained exercise training and bone mineral density in aging male runners. Scand J Med Sci Sports 6:216–221
Greene DA, Naughton GA, Briody JN, Kemp A, Woodhead H, Farpour-Lambert N (2004) Musculoskeletal health in elite male adolescent middle-distance runners. J Sci Med Sport 7:373–383
Haapasalo H, Kontulainen S, Sievanen H, Kannus P, Jarvinen M, Vuori I (2000) Exercise-induced bone gain is due to enlargement in bone size without a change in volumetric bone density: a peripheral quantitative computed tomography study of the upper arms of male tennis players. Bone 27:351–357
Haapasalo H, Sievanen H, Kannus P, Heinonen A, Oja P, Vuori I (1996) Dimensions and estimated mechanical characteristics of the humerus after long-term tennis loading. J Bone Miner Res 11:864–872
Hamdy RC, Anderson JS, Whalen KE, Harvill LM (1994) Regional differences in bone density of young men involved in different exercises. Med Sci Sports Exerc 26:884–888
Hetland ML, Haarbo J, Christiansen C (1993) Low bone mass and high bone turnover in male long distance runners. J Clin Endocrinol Metab 77:770–775
Hetland ML, Haarbo J, Christiansen C, Larsen T (1993) Running induces menstrual disturbances but bone mass is unaffected, except in amenorrheic women. Am J Med 95:53–60
Kalender WA, Felsenberg D, Louis O, Lopez P, Klotz E, Osteaux M, Fraga J (1989) Reference values for trabecular and cortical vertebral bone density in single and dual-energy quantitative computed tomography. Eur J Rad 9:75–80
Kalender WA, Klotz E, Süss C (1987) Vertebral bone mineral analysis: an integrated approach with CT. Radiology 164:419–423
Kang Y (2003) 3D Quantitative Computed Tomography (QCT) of the proximal femur. Doctoral-Thesis Institute of Medical Physics. Friedrich-Alexander Universität Erlangen-Nürnberg, Erlangen, pp 99
Kemmler W (2000) Körperliche Belastung und Osteoporose - Einfluss eines intensiven 9-monatigen körperlichen Trainings auf Knochendichte, Gesamtkalzium und Wirbelkörperbreite bei Frauen mit unterschiedlichem Belastungsniveau in der Vergangenheit. Osteologie 9:114–123
Kemmler W, Engelke K, Lauber D, Weineck J, Hensen J, Kalender WA (2003) The Erlangen Fitness Osteoporosis Prevention Study (EFOPS) - a controlled exercise trial in early postmenopausal women with low bone density: First year results. Arch Phys Med Rehabil 84:673–683
Kemmler W, Weineck J, Kalender WA, Engelke K (2004) The effect of habitual physical activity, nonathletic exercise, muscle strength, and VO2max on bone parameters is rather low in early osteopenic postmenopausal women. J Muskuloskel Neuron Interact 4:325–334
Lane NE, Bloch DA, Jones HH, Marshall WH, Wood PD, Fries JF (1986) Long-distance running, bone density and osteoarthritis. JAMA 255:1147–1151
MacDougall JD, Webber CE, Martin J (1992) Relationship among running mileage, bone density, and serum testosterone in male runners. J Appl Physiol 73:1165–1170
Michel BA, Lane NE, Björkengren A, Bloch DA, Fries JF (1992) Impact of Running on Lumbar Bone Density: a 5-year longitudinal study. Journal of Rheumatology 19:1759–1763
Morel J, Combe B, Francisco J, Bernard J (2001) Bone mineral density of 704 amateur sportsmen involved in different physical activities. Osteoporos Int 12:152–157
Mussolino ME, Looker AC, Orwoll ES (2001) Jogging and bone mineral density in men: results from NHANES III. Am J Public Health 91:1056–1059
Nevill AM, Holder RL, Stewart AD (2003) Modeling elite male athletes’ peripheral bone mass, assessed using regional dual x-ray absorptiometry. Bone 32:62–68
Nilsson BE, Westlin NE (1971) Bone density in athletes. Clin Orthop 77:179–182
Standing committee on the Scientific Evaluation of Dietary Reference Intakes IoM (1997) Dietary reference intakes:calcium, phosphorus,magnesium, Vitamin D, and flouride. Academic Press, Washington D.C
Stewart AD, Hannan J (2000) Total and regional bone density in male runners, cyclists, and controls. Med Sci Sports Exerc 32:1373–1377
Acknowledgement
The study was funded by the Bundesinstitut für Sportwissenschaften, Bonn, Germany (VF 0407/01/28/2002–2004)
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kemmler, W., Engelke, K., Baumann, H. et al. Bone status in elite male runners. Eur J Appl Physiol 96, 78–85 (2006). https://doi.org/10.1007/s00421-005-0060-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-005-0060-1