
Abstract
Objectives
This study investigated whether reductions in finger blood flow (FBF) during and after vibration are similarly dependent on the magnitude and duration of the vibration.
Methods
FBF on the left and right hand was measured every minute during, and for 1 h following, exposure of the right hand to one of three magnitudes of 125-Hz sinusoidal vibration (0, 22, or 88 ms−2 rms) for one of two durations (7.5 or 15 min). Each of five experimental sessions was comprised of five periods: (i) no force and no vibration (5 min), (ii) 2-N force and no vibration (5 min), (iii) 2-N force and vibration (7.5 or 15 min), (iv) 2-N force and no vibration (5 min), and (v) no force and no vibration (60 min).
Results
Vibration reduced FBF in the exposed and unexposed hands, both during and after vibration. With increased magnitude of vibration, there was increased vasoconstriction in all fingers during and after exposure, and longer recovery times after vibration exposure. With increased duration of vibration, there were no changes in vascular responses during exposure but increased vasoconstriction after exposure and prolonged recovery times. With the greater vibration magnitude, the reduction in FBF during exposure was correlated with the time taken to recover after exposure.
Conclusions
Subjects with greater reduction in blood flow during vibration exposure also have stronger and longer vasoconstriction during subsequent recovery. The correlation between vascular changes during and after vibration exposure suggests similar mechanisms control FBF during and after vibration exposure.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Workers who are regularly exposed to hand-transmitted vibration from powered hand tools are at risk of developing disorders in the fingers, hands or arms, collectively known as the hand–arm vibration syndrome (Griffin 1997; Griffin and Bovenzi 2002). One consequence of exposure to hand-transmitted vibration can be impaired circulation in the fingers, with ‘attacks’ on finger blanching commonly provoked by exposure to cold. The blanching may occur on the distal, middle or proximal phalanges of the fingers and is called ‘vibration-induced white finger’ (Griffin 1990). Although various tests can assist a diagnosis (e.g. the measurement of finger systolic blood pressure following cold provocation), the mechanisms involved in the causation of this vascular disorder are unclear.
Laboratory experimental studies have revealed that finger blood flow reduces during exposure to hand-transmitted vibration, with the vasoconstriction depending on the frequency of vibration (Bovenzi et al. 2000), the magnitude of vibration (Bovenzi et al. 1999) and the duration of exposure to vibration (Bovenzi et al. 1998). The laboratory studies have also shown that exposure to vibration on one hand results in vasoconstriction in fingers on both the exposed hand and the unexposed hand (Bovenzi et al. 2000, 2004, 2006). Furthermore, there is continued reduction in finger blood flow on both hands after the cessation of vibration.
With increasing magnitude of vibration, there appears to be greater reductions in finger blood flow, both during vibration and after vibration (Bovenzi et al. 1999, 2000). Changing the duration of exposure to vibration seems to have little effect on vasoconstriction during vibration exposure, but one study suggests vasoconstriction after the cessation of vibration is greater after longer periods of exposure to vibration (Bovenzi et al. 1998).There has been little study of finger blood flow after cessation of exposure to hand-transmitted vibration, and no known systematic comparison of finger blood flow during and after vibration. The after-effects of acute exposures to hand-transmitted vibration may be of practical importance to those exposed at work and at risk of a blanching attack. The after-effects may also provide information that advances understanding of the vascular response to hand-transmitted vibration: their dependence on the characteristics of vibration (e.g. vibration magnitude, duration and frequency) may help to identify the mechanisms causing vasoconstriction.
This study was designed to increase the understanding of the vasoconstriction occurring during and after exposure to hand-transmitted vibration and, especially, investigate whether different mechanisms were involved. It was hypothesised that reductions in finger blood flow during vibration would be correlated with reductions in finger blood flow after vibration—so a subject showing greater vasoconstriction during vibration would also show greater vasoconstriction after vibration. It was also hypothesised that with increased magnitude of vibration, finger blood flow would reduce both during and after vibration and that the duration before finger blood flow returned to near normal after cessation of vibration would increase. With increased duration of exposure to vibration, it was hypothesised that finger blood flow would be more greatly reduced after cessation of vibration and that the duration before finger blood flow returned to normal would be increased.
Subjects and methods
Subjects
Sixteen healthy male volunteers participated in the study. All subjects were university students with no history of significant (regular or prolonged) use of hand-held vibrating tools in occupational or leisure activities. None of the subjects reported disorders that might affect finger blood flow. All subjects completed a health questionnaire, read a list of medical contraindications and gave their written informed consent to the study. Subjects had a mean age of 23.6 (SD 3.3; range 18–30) years, a mean stature of 177 (SD 7.5; range 165–197) cm, a mean weight of 70.3 (SD 14.9; range 50–106) kg and mean body mass index (BMI) of 22.3 (SD 3.4; range 17.0–29.4). From the measurements of the length, width and depth of each phalanx using vernier callipers, mean finger volumes were calculated as 19.6 (SD 6.3) cm3 and 19.8 (SD 5.9) cm3 for the middle fingers of the right and left hands, respectively, and 10.4 (SD 2.6) cm3 and 10.0 (SD 2.6) cm3 for the little fingers of the right and left hands.
The study was approved by the Human Experimentation Safety and Ethics Committee of the Institute of Sound and Vibration Research at the University of Southampton.
Measurement of finger blood flow
Finger blood flow (FBF) was measured simultaneously in the middle and little fingers of the right and left hands using strain gauge plethysmography. A plastic cuff was fitted around the proximal phalanx of the finger, with a soft plastic tube from the cuff connected to a HVLab Multi-channel Plethysmograph (HVLab, University of Southampton). A mercury-in-silicon strain gauge was placed around the finger at the base of the finger nail. The FBF was measured using a venous occlusion method. The pressure cuffs were inflated to a pressure of 60 mm Hg (8.0 kPa), and the consequent rises in fingertip volumes were detected by means of the strain gauges according to the criteria given by Greenfield et al. (1963) The FBF measurements were expressed as millilitres per 100 ml per second (ml/100 ml/s).
Brachial systolic and diastolic blood pressures were measured in the upper left arm by an auscultatory technique while the participants were supine.
Finger skin temperature (FST) was measured by using k-type thermocouples attached by micropore tape to the distal phalanx of the right and left ring fingers. The room temperature was measured by a mercury-in-glass thermometer to an accuracy of ±0.5 °C. The thermometer was located adjacent to the heads of the subjects.
Experimental protocol
The experiment was performed in a room with a mean temperature of 24.8 (SD 0.5) °C. The subjects were requested to avoid consuming caffeine for 2 h and alcohol for 12 h prior to testing.
Each subject was exposed on separate days to four conditions, consisting of three different vibration stimuli and one control condition with no vibration. The order of conditions was randomised.
In each session, subjects experienced five successive experimental periods, with no break between the five periods:
-
i.
Pre-exposure period (5 min): no force and no vibration;
-
ii.
Pre-exposure application of force (5 min): with 2-N force with no vibration;
-
iii.
Vibration period (15 or 7.5 min): with 2-N force and 125-Hz vibration at 22 or 88 ms−2 rms;
-
iv.
Post-exposure application of force (5 min): with 2-N force with no vibration;
-
v.
Recovery period (60 min): no force and no vibration.
The condition without vibration consisted of the same five periods, but with the 2-N force applied without vibration during period (iii). In all conditions, the left hand remained motionless with no vibration and no force throughout all five periods.
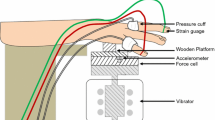
Throughout each session, subjects lay supine with both hands resting on platforms alongside their body at heart level. After acclimatisation to the environment for 15–20 min, finger blood flow in the middle and little fingers of both hands was measured simultaneously at 1-min intervals during the first 5-min period. The right hand was then gently moved by the experimenter to place the centre of the palm on a spherical wooden surface with all fingers suspended in air (Fig. 1). There was a 25-mm diameter contact area with the spherical surface having a radius of 25 mm. During the second period, the subjects applied a 2-N downward force to the wooden surface that was supported by a Huntleigh force cell secured to the table of an electrodynamic vibrator (VP4, Derritron). The force cell was connected to a metre that provided visual feedback to the subject of the downward force applied by the hand. The same experimental arrangement has been used in some previous studies of the effect of vibration applied to the palm (Griffin et al. 2006; Ye et al. 2012). During the third period, sinusoidal vertical vibration was presented for either 7.5 or 15 min. The vibration was monitored by an Entran 233E accelerometer attached to the metal plate supported on the force cell. This was followed by a period with force but without vibration during the fourth period. The right hand was then gently moved by the experimenter to make sure it was supported on a platform at heart level alongside the body during the fifth period.

Arrangement of apparatus for generating vibration, controlling the contact force and measuring finger blood flow

Percentage change in finger blood flow (% of pre-exposure) in the middle and little fingers of the right (exposed) and left (unexposed) hands during the five exposure periods and four experimental conditions (C). The plotted symbols are mean values
The sinusoidal vibration at 125 Hz was produced in the vertical direction with an rms acceleration of either 22 or 88 ms−2 (unweighted), corresponding to a frequency-weighted acceleration of either 2.75 or 11 ms−2 rms according to International Standard 5349-1 (2001).
Each of the subjects attended four sessions (Table 1). Condition 0 was a control condition, with the other three conditions designed to explore the effects of the magnitude and the duration of exposure to vibration. Using the frequency weightings and daily time dependency for hand-transmitted vibration in ISO 5349-1:2001, the 8-h equivalent exposures, a hw(8h), were 0.486, 1.375 and 1.944 ms−2 rms, respectively.
Statistical methods
Statistical analysis was performed using the software package Stata (version 11.2 SE, Stata Corporation, College Station, TX, USA). The data were summarised with the mean as a measure of central tendency and the standard deviation (SD) or the 95 % confidence intervals (95 % CI) as measures of dispersion. Pairwise correlations between variables were tested by means of the Pearson’s coefficient.
The generalised estimating equations (GEE) method for repeated measures data set was used to test the hypothesis of no difference in the vascular responses in different exposure conditions taking into account the within-subject correlation over time. The Wald test was carried out to test the difference between the regression coefficients estimated by the fitted GEE models. A p value of 0.05 was set as the limit for statistical significance.
Results
There were no significant correlations between the FBF in any finger and the age, height, weight, BMI or finger volume during any experimental session. The FBF was not correlated with finger skin temperature (FST) during any period of any of the four conditions (n = 16, r = 0.03–0.41, p = 0.91–0.11, respectively).
Systolic/diastolic brachial arterial pressures measured before the first period ranged from 130/70 to 90/50 mmHg, with no significant differences within subjects across conditions. No differences were observed between brachial arterial blood pressures measured at the beginning and at the end of the four experimental conditions (data not shown).
The air temperature in the laboratory did not show significant differences across the four experimental conditions (p = 0.88), ranging between 24.0 and 26.0 (mean 24.8)°C. There was no significant correlation between FBF and room temperature for any finger during the pre-exposure period (p = 0.16–0.85) or over the whole experiment (p = 0.16–0.98).
Finger circulation before exposure
In the first period before exposure to the push force alone, the mean FBF across the sessions ranged from 0.93 to 1.35 ml/100 ml/s in the right middle finger, 0.91 to 1.16 ml/100 ml/s in the right little finger, 1.04 to 1.44 ml/100 ml/s in the left middle finger, and 0.94 to 1.15 ml/100 ml/s in the left little finger. There were no differences in FBF between the exposed and unexposed fingers.
The finger skin temperature during the first period averaged 34.7 (SD 1.5)°C in the right fourth finger and 34.4 (1.8)°C in the left fourth finger, with no significant differences across the four experimental conditions.
Circulatory effects of exposure to push force (condition 0)
In condition 0 (exposure to push force with no vibration), there was no significant change in the FBF in any finger over periods (ii) to (iv) compared with period (i) (i.e. pre-exposure). In period (v) (i.e. during recovery), an increase in FBF was observed in all fingers, with the exception for the right little finger, but this increase was significant only in the right middle finger (14–23 %, p < 0.05).
Circulatory effects of exposure to vibration with different magnitudes and durations (conditions 1, 2, and 3)
Table 2 and Fig. 2 report the changes in %FBF (mean FBF expressed as a percentage of the mean FBF measured during the first period) in the exposed and unexposed fingers during exposure to 2-N push force and vibration with different acceleration magnitudes and durations [period (iii)].
Vibration with an acceleration magnitude of 88 ms−2 rms and a duration of 15 min (condition 3) caused a more powerful digital vasoconstriction in both fingers of both hands than a vibration of 22 ms−2 rms with the same duration (condition 1), (p < 0.001).
There were no significant differences in the reduction of FBF in any finger when the right hand was exposed to vibration with the same acceleration magnitude (88 ms−2 rms) but a different duration (7.5 min for condition 2 and 15 min for condition 3).
Finger circulation after exposure
Table 3 compares the effect of exposure to vibration with different magnitudes and durations on the recovery time needed for %FBF to first exceed 80 % of the pre-exposure value (R 80 % in minutes) during the 60-min recovery period [period (v)].
Exposure to vibration in condition 3 (88 ms−2 rms, 15 min) caused a greater delay in R 80 % in all fingers compared to condition 1 (22 ms−2 rms, 15 min) and condition 2 (88 ms−2 rms, 7.5 min), (p < 0.001). Over the four fingers, R 80 % averaged 17–22 min longer for condition 3 than for condition 1, and 13–19 min longer for condition 3 than for condition 2, indicating that both the magnitude and the duration of vibration influenced the vascular after-effects in both the exposed and the unexposed fingers.
There were no significant differences in R 80 % during recovery between fingers within each experimental condition (Wald χ2 = 0.27–5.69, p = 0.13–0.97; Table 4). Consistently, R 80 % values correlated significantly between exposed and unexposed hands (r = 0.80–0.84, p < 0.001).
Correlation between finger blood flow during and after vibration exposure
Correlations between FBF during the third period (2-N push force with vibration) and the fifth period (recovery) varied between the three vibration conditions and varied over the recovery period (Fig. 3). In condition 3 with the greatest magnitude and duration of vibration exposure (88 ms−2 rms for 15 min), the FBF during recovery tended to be correlated with the FBF during vibration exposure. As recovery proceeded, the correlations weakened. A similar pattern is apparent on the two fingers on the exposed hand and the two fingers on the unexposed hand. With the lower magnitude of vibration (condition 1), the correlations are almost non-existent.

p values of the correlations (Pearson’s r) between the average FBF during the third period (exposure to 2-N force + vibration) and the average FBF during 15-min epochs of the fifth period (60-min recovery). Condition 1: 22 ms−2 rms, 15 min; condition 2: 88 ms−2 rms, 7.5 min; condition 3: 88 ms−2 rms, 15 min
The reduction in FBF during exposure to vibration was correlated with R 80 % in all fingers for conditions 2 and 3 (0.001 < p < 0.05), but not for condition 1 (p = 0.42–0.84).
Discussion
Finger blood flow during vibration exposure
Effects of vibration magnitude
Vibration with an unweighted acceleration magnitude of 22 ms−2 rms (2.75 ms−2 rms frequency-weighted) induced immediate reductions in finger blood flow in fingers on both the exposed right hand and the unexposed left hand. With increased magnitude of vibration (88 ms−2 rms unweighted, 11 ms−2 rms frequency-weighted), finger blood flow was further reduced on both hands. These findings are consistent with previous studies: 125-Hz vibration presented at magnitudes increasing from 5.5 to 62 ms−2 rms caused increased vasoconstriction in fingers of both hands (Bovenzi et al. 1999), and 125-Hz vibration applied to the intermediate phalanx of the right middle finger with magnitudes increasing from 16 to 64 ms−2 rms progressively reduced finger blood flow (Bovenzi et al. 2004). Similar effects of the magnitude of vibration have been reported with 60-Hz vibration at unweighted magnitudes from 3.16 to 31.6 ms−2 rms (Luo et al. 2000) and with vibration at each one-third octave centre frequency from 16 to 315 Hz for frequency-weighted accelerations from 0 to 15 ms−2 rms (Thompson and Griffin 2009). With 125-Hz vibration applied to a small area of the thenar eminence of the right hand, a stronger vasoconstriction has been found when the vibration magnitude increased from 0.5 to 1.5 ms−2 rms (Ye and Griffin 2011). Although exciting different locations of the hand (i.e. fingers, palm, thenar eminence or whole hand), all of these studies show a greater vasoconstrictor with greater magnitudes of vibration.
Effects of exposure duration
During exposure to vibration with both durations (i.e. 7.5 and 15 min), there were no significant changes in finger blood flow: the vasoconstriction remained constant, similar to a previous study with 125-Hz vibration at 87 ms−2 rms and 7.5-, 15-, and 30-min exposure durations (Bovenzi et al. 1998). This seems to suggest there is no accumulative effect of vibration through such exposures. However, studies on animals suggest exposure of the rat tail to 60-Hz vibration at 49 ms−2 rms for 4 h/day results in a progression of endothelial cell death over 9 days (Curry et al. 2002). The absence of a change during the present short durations of exposure does not exclude the possibility of accumulative effects over longer durations.
Finger blood flow after vibration exposure
Effect of vibration magnitude
There was a continued reduction in finger blood flow after cessation of vibration at both 22 and 88 ms−2 rms, with the extent of the reduction and the time before recovery to 80 % of pre-exposure FBF dependent on the magnitude of vibration. With increased magnitude of acceleration, the vasoconstriction after cessation of vibration was greater and the recovery time longer on both the exposed right hand and the unexposed left hand. After 2-min exposures to high-intensity vibration from a pneumatic chisel, incomplete recovery of finger blood flow has been reported, broadly consistent with the present findings (Egan et al. 1996). Other studies have found greater reductions in finger blood flow after exposure to greater magnitudes of vibration (Bovenzi et al. 1999; Thompson and Griffin 2009). The findings indicate the vasomotor changes during recovery are increased and take longer to recover after exposure to greater magnitudes of vibration.
Effect of exposure duration
Although the duration of exposure to vibration did not influence finger blood flow during exposure, there was a greater reduction in finger blood flow and delayed recovery after the longer duration of exposure. After 7.5-min exposure to 125-Hz vibration at 88 ms−2 rms, the FBF recovered to 80 % of the pre-exposure value within about 20 min, but by extending the duration to 15 min, around 35 min was required for similar recovery. With 7.5-, 15- and 30-min exposures to 125-Hz vibration at 87 ms−2 rms, greater vasoconstriction has been reported after the longer exposures to vibration (Bovenzi et al. 1998). Increased vasoconstriction with increased duration of exposure to 31.5-Hz vibration with a frequency-weighted acceleration of 16 ms−2 rms has also been reported (Olsen 1993). These findings suggest that after exposure to hand-transmitted vibration, the vascular responses of both exposed and non-exposed hands depend on the exposure duration, with longer durations inducing stronger vasoconstriction.
Relation between the finger blood flow during and after vibration
There were positive correlations between reductions in finger blood flow during vibration exposure and the extent of vasoconstriction (both reductions in finger blood flow and time before recovery) after exposure to 88 ms−2 rms in conditions 2 and 3. This indicates that individuals with stronger reductions in FBF during vibration also had greater vasoconstriction during recovery. However, in condition 1 with the lower magnitude of vibration (22 ms−2 rms), the relation between the FBF during and after vibration was less clear. This may have been because the reduced vibration exposure triggered less vasoconstriction and allowed a more rapid return to baseline (Fig. 2). There may also have been a more variable response both during vibration and during recovery.
In conditions 2 and 3, there was a correlation between the recovery period R 80 % and the vasoconstriction during vibration exposure. This indicates that recovery to baseline levels of FBF took longer in subjects with the greatest reductions in FBF during vibration. The absence of a significant correlation in condition 1 (with low magnitude vibration) suggests the extent of vasoconstriction during exposure is not the only factor influencing the recovery period.
The method of evaluating the severity of chronic exposures to hand-transmitted vibration defined in International Standard (ISO 5394-1, 2001) was influenced by subjective responses (i.e. discomfort) during exposure to vibration, whereas the probability and the severity vascular disorders might be expected to be more closely related to the acute vascular responses occurring both during and after exposure to vibration. Collectively, the present and previous studies show that vascular responses during and after exposure depend on the magnitude, frequency and duration of vibration (Bovenzi et al. 1998, 1999, 2000; Thompson and Griffin 2009), although much more is known about vasoconstriction during exposure than vasoconstriction after exposure. The correlations observed in the present study show associations between vasoconstriction on exposed and unexposed hands, and between vasoconstriction during and after exposure to vibration. This does not necessarily imply that the same mechanisms are responsible for vasoconstriction, but the associations suggest that increases in one of the two vibration characteristics investigated here (i.e. vibration magnitude) increase vasoconstriction both during and after exposure. Increases in the other vibration characteristic investigated here (i.e. duration of vibration) do not increase vasoconstriction during exposure but do increase vasoconstriction after exposure. Although the influence of vibration frequency on the correlation between FBF during and after exposure has not been studied in this study, it seems that frequencies that induce stronger vasoconstriction during exposure (e.g. 125 and 250 Hz) also induce stronger vasoconstriction after exposure (Thompson and Griffin 2009). The after-effects of vibration need to be better understood so that they can be taken into account when evaluating vibration severity and arranging work so as to allow finger circulation to recover to baseline levels.
The correlations between finger blood flow during and after vibration imply either a common mechanism or two different mechanisms controlling vasoconstriction during and after vibration that are similarly dependent on the magnitude of vibration. With greater magnitudes of vibration, the findings are consistent with greater sympathetic vasoconstriction during and after exposure. With greater durations of exposure, the response during exposure remains constant (for the durations studied), but there is a greater central response after cessation of longer exposures, possibly due to some form of ‘accumulation’ during exposure.
Conclusions
The application of 125-Hz vibration to the palm of the right hand provokes an immediate reduction in finger blood flow in the right and left hands. With increases in vibration magnitude (from 22 to 88 ms−2 rms, unweighted; 2.75 to 11 ms−2 rms, weighted), there is increased correlation between reductions in finger blood flow during exposure to vibration and reductions in finger blood flow after cessation of exposure to vibration. Similarly, with increases in the duration of vibration (from 7.5 to 15 min), there is increased correlation between the vasoconstriction during and after exposure to vibration. With the greater magnitude of vibration (88 ms−2 rms, unweighted; 11 ms−2 rms, weighted), there is a negative correlation between finger blood flow during exposure and the time to recover finger blood flow after cessation of vibration. The results show that people with stronger vascular changes during vibration also experience greater and longer vasoconstriction after removal of vibration. The statistical associations between reductions in finger blood flow during exposure to vibration and reductions in finger blood flow after exposure to vibration suggest common mechanisms may be involved in vibration-induced vasoconstriction during and after exposure to hand-transmitted vibration.
References
Bovenzi M, Lindsell CJ, Griffin MJ (1998) Duration of acute exposure to vibration and finger circulation. Scand J Work Environ Health 24(2):130–137
Bovenzi M, Lindsell CJ, Griffin MJ (1999) Magnitude of acute exposure to vibration and finger circulation. Scand J Work Environ Health 25(3):278–284
Bovenzi M, Lindsell CJ, Griffin MJ (2000) Acute vascular responses to the frequency of vibration transmitted to the hand. Occup Environ Med 57(6):422–430
Bovenzi M, Welsh AJL, Griffin MJ (2004) Acute effects of continuous and intermittent vibration on finger circulation. Int Arch Occup Environ Health 77(4):255–263
Bovenzi M, Welsh AJL, Della Vedova A, Griffin MJ (2006) Acute effects of force and vibration on finger blood flow. Occup Environ Med 63:84–91
Curry BD, Bain JLW, Yan JG, Zhang LL, Yamaguchi M, Matloub HS et al (2002) Vibration injury damages arterial endothelial cells. Muscle Nerve 25:527–534
Egan CE, Hspie BH, McGrann S, McKenna KM, Allen JA (1996) Acute effects of vibration on peripheral blood flow in healthy subjects. Occup Environ Med 53:663–669
Greenfield ADM, Whitney RJ, Mowbray JF (1963) Methods for the investigation of peripheral blood flow. Br Med Bull 19:101–109
Griffin MJ (1990) Handbook of human vibration. Academic Press, London
Griffin MJ (1997) Measurement, evaluation, and assessment of occupational exposures to hand-transmitted vibration. Occup Environ Med 54:73–89
Griffin MJ, Bovenzi M (2002) The diagnosis of disorders caused by hand-transmitted vibration: Southampton Workshop 2000. Int Arch Occup Environ Health 75:1–5
Griffin MJ, Welsh AJL, Bovenzi M (2006) Acute response of finger circulation to force and vibration applied to the palm of the hand. Scand J Work Environ Health 32:383–391
International Organization for Standardization (2001) Mechanical vibration: guidelines for the measurement and the assessment of human response to hand-transmitted vibration. International Standard, ISO 5349-1
Luo J, Sakakibara H, Zhu SK, Kondo T, Toyoshima H (2000) Effect of vibration magnitude and repetitive vibration on finger blood flow in healthy subjects. Int Arch Occup Environ Health 73:281–284
Olsen N (1993) Vibration after effects on vasoconstrictors response to cold in the normal finger. Eur J Appl Physiol Occup Physio 66:246–248
Thompson AJL, Griffin MJ (2009) Effect of the magnitude and frequency of hand-transmitted vibration on finger blood flow during and after exposure to vibration. Int Arch Occup Environ Health 82:1151–1162
Ye Y, Griffin MJ (2011) Reductions in finger blood flow in men and women induced by 125-Hz vibration: association with vibration perception thresholds. J Appl Physiol 111:1606–1613
Ye Y, Mauro M, Bovenzi M, Griffin MJ (2012) Acute effects of mechanical shocks on finger blood flow: influence of shock repetition rate and shock magnitude. Int Arch Occup Environ Health 85:605–614
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ye, Y., Mauro, M., Bovenzi, M. et al. Association between vasoconstriction during and following exposure to hand-transmitted vibration. Int Arch Occup Environ Health 87, 41–49 (2014). https://doi.org/10.1007/s00420-012-0836-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-012-0836-7