
Abstract
Introduction
Scaphoid nonunion remains challenging for hand surgeons. Several treatment options are available such as: non-vascularized or vascularized bone grafting, with or without additional stabilization. In the last few decades, extracorporeal shockwave therapy (ESWT) has become an established procedure for treating delayed and nonunions. Purpose of this retrospective follow-up study was (a) to investigate union rate and clinical outcome of the different implants [either one/two headless compression screws (HCS) or a plate] and (b) union rate and clinical outcome using only surgery, or a combination of surgery and ESWT.
Materials and methods
The study included 42 patients with scaphoid nonunions of the waist with a mean follow-up of 52 months. All patients received a non-vascularized bone graft from the iliac crest and stabilization was achieved by using one, two HCS or a plate. ESWT was performed with 3000 impulses, energy flux density per pulse 0.41 mJ/mm2 within 2 weeks after surgery. Clinical assessment included range of motion (ROM), pain according to the Visual Analog Scale (VAS), grip strength, Disability of the Arm Shoulder and Hand Score, Patient-Rated Wrist Evaluation Score, Michigan Hand Outcomes Questionnaire and modified Green O’Brien (Mayo) Wrist Score. In addition, each patient had a CT scan of the wrist.
Results
A total of 33/42 (79%) patients showed union at the follow-up investigation. Patients treated with additional ESWT showed bony healing in 21/26 (81%) and without ESWT in 12/16 (75%). Patients that were stabilized using one HCS showed bony healing in 6/10 (60%), with two HCS 10/12 (83%) and by plate 17/20 (85%). The ESWT group had a significantly lower pain score according to the VAS and better modified Green O’Brien (Mayo) Score. No differences could be found in respect of ROM, grip strength, functional outcome score depending of which stabilization method was used.
Conclusions
Stabilization of scaphoid waist nonunions with two HCS or plate showed higher union rates than a stabilization using only one HCS. In addition, ESWT combined with a nonvascularized bone graft from the iliac crest seems a suitable option for treating scaphoid nonunions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Scaphoid fractures account for 60% of all fractures of the carpus and 10% of all hand fractures, but overall only 2–3% of all fractures [1,2,3,4,5,6,7]. The majority of scaphoid fractures heal when treated conservatively, but nonunion is registered in 10% of all cases [8,9,10,11,12].
Scaphoid nonunions are primarily treated to achieve union, correct deformity, relieve symptoms, improve range of motion and prevent the progression of osteoarthritis [13,14,15,16]. Several treatment options are available for scaphoid nonunions: non-vascularized bone grafting from the iliac crest or distal radius, vascularized bone grafting with or without additional stabilization using either K-wires, headless compression screw (HCS) or plate [17,18,19,20,21].
Plate fixation in scaphoid nonunion was first introduced by Ender 1977, using the so-called scaphoid-beaked plate [22]. The distal fragment is stabilized by a screw, and the proximal by a staved hook. The Ender plate simultaneously joins the bone fragments together whilst applying compression on the impacted bone transplant [23, 24]. Recently, several different scaphoid plates have been developed and some authors have published their studies in the literature [17, 22,23,24].
In the last few decades extracorporeal shock wave therapy (ESWT) has gained importance in the treatment of nonunions [25]. Union rates using only ESWT are reported to range between 50% and 85% [26]. Schaden et al. [27] reported a union rate in treatment of 115 delayed and nonunion of 85% and especially in scaphoid nonunions of 67%. Wang et al. [28] used a combination of surgery and ESWT in a randomized controlled trial focusing on acute long-bone fractures, and registered a significantly higher rate of fracture healing in patients who received both treatments.
However, the effects of ESWT on bone are not yet completely researched [27]. ESWT causes a significant neovascularization in the treated tissue, up-regulation and expression of various pro-angiogenic and pro-osteogenic growth factors. As shown in recent publications, the shockwave exerts a positive impact on the migration of stem cells [29,30,31,32,33,34].
The aim of this retrospective follow-up study was twofold: (1) to compare union rate and clinical outcome of the different implants (either one/two HCS or a plate) and (2) to investigate union rate and clinical outcome using only surgery, or a combined treatment of surgery and ESWT. The null hypothesis presupposed no significant differences in union rate and clinical outcome between one/two HCS or plate and patients treated with or without additional ESWT after surgery.
Materials and methods
Location and eligibility criteria
Institutional review board approval was obtained for this retrospective follow-up study. It included all scaphoid nonunions treated with a nonvascularized bone graft from the iliac crest from 2002 to 2014. Because the literature reported such promising results, some surgeons started in 2010 to use ESWT 2 weeks after surgery in a partner hospital.
Scaphoid nonunions were classified according to the criteria of Herbert and Krimmer [35, 36] using the primary CT Scans. Two hand surgeons, who were blinded to the treatment of the patients, carried out the classification process. Inclusion criteria were: (1) age equal or older than 18 years; (2) nonunion of the scaphoid at the waist; (3) CT scan prior to surgery; (4) nonunion of the scaphoid with a minimum interval between injury or last operative/nonoperative intervention of 6 months [18]; (5) treatment by non-vascularized bone graft from the iliac crest; (6) stabilization with either one or two HCS or a plate. Exclusion criteria were (1) younger than 18 years of age; (2) additional injuries to the hand; (3) pregnancy and (4) proximal pole nonunions.
All patients were treated surgically at the same European Hand Trauma Center, validated by the Hand Trauma Committee of the Federation of European Societies for Surgery of the Hand.
Surgical procedure
The patients underwent surgery in a supine position under regional or general anesthesia. The arm was placed on a radiolucent table, and the image intensifier positioned cranially. A pneumatic tourniquet was applied to the proximal end of the arm and inflated to 250 mmHg.
A palmar approach between the flexor carpi radialis (FCR) tendon and the radial artery was used to access the scaphoid directly. The FCR tendon was retracted ulnarly, the radiopalmar ligaments were dissected and the scaphoid exposed. Hohmann hooks were placed on either site of the scaphoid and the nonunion exposed. Fibrous and necrotic tissue was removed and a palmar cortical window cut into the bone, thus the remaining sclerotic and fibrous tissue could be debrided using a slow rotating spherical burr. After preparation of the nonunion side, scaphoid length and shape was restored. To reduce the fragments anatomically, two 1.2-mm K-wires were inserted perpendicularly into each fragment and used as joysticks.
Once the scaphoid was aligned, two special HCS guidewires were inserted distally, drilled preferably parallel and along the central axis of the scaphoid up to the subchondral bone. Correct positioning of the K-wires was confirmed under fluoroscopy.
The cancellous bone was harvested from the iliac crest using standard procedure and used to fill and manually impact the bone defect in the scaphoid. Using the image intensifier ensured the complete filling of the cavity with the cancellous bone graft. After determining the screw length, a non-reamed 3.0-mm HCS was inserted and the other anti-rotation K-wire removed. The screw length was measured precisely and positioned 2 mm below the articular cartilage.
In the case of two HCS (2.2 mm), the second screw was placed over the additional anti-rotational K-wire. Due to the increased rotational stability achieved in the double screw technique, a central placement of the screws is not always possible or even necessary [37]. If one HCS is used, central placement is mandatory to maximize stiffness and load to failure. We agree with Dodds et al. [38] and McCallister [39] that longer screw lengths significantly increase stability and as Garcia et al. [40] we also aimed to achieve the longest possible screw length without cortical penetration.
In plate stabilization, after filling and impacting the cancellous bone graft, the plate was placed on the palmar aspect of the scaphoid. Under image intensification, the correct positioning of the plate was maintained by temporarily affixing it to the scaphoid with two K-wires. The screw length was determined, and after reaming, the screws were inserted. Care was taken to ensure that the screws did not protrude at the articular surface. Finally, all K-wires were removed and the palmar capsule closed with resorbable sutures. The skin was closed in standard fashion.
For the following 8 weeks, all patients were immobilized with either a below-elbow cast or thermoplastic splint with thumb inclusion.
Extracorporeal shockwave therapy
All patients in the ESWT group were referred to our partner hospital for one session of ESWT within 2 weeks post-surgery. The ESWT was carried out under general or regional anesthesia because of the pain incurred. The pronated arm was positioned over the image intensifier and the scaphoid nonunion localized. Sterile ultrasound gel was then applied to the overlying skin to reduce refractation. The center of the shock wave targeting device (the focal point) was positioned to direct the shock waves directly onto the nonunion site. Shockwaves were applied over three points on the extensor site as well as the entire proximal pole of the scaphoid (Fig. 1). High-energy shock waves were administered with 3000 impulses, an energy flux density of 0.41 mJ/mm2, and a frequency of 4 Hz (Orthowave 280, MTS, Konstanz, Germany).

ESWT performed in general or regional anesthesia within 2 weeks after surgery with 3000 impulses, energy flux density per pulse 0.41 mJ/mm2
After the ESWT treatment, the splint/cast was again applied for the remainder of 8 weeks.
Outcome evaluation
The assessment included a clinical examination and verification using a computed tomography (CT) scan. All CT scans were performed at our institute and the results analyzed by two hand surgeons (C.P., T.B.) with regard to the following criteria: union was calculated according to Grewal et al. [41], postoperative osteoarthritis, DISI deformity, humpback deformity, and a SNAC wrist [42]. A humpback deformity was measured according to the height-to-length (H/L) ratio described by Bain et al. [43], an H/L greater than 0.65 was defined as a malalignment. DISI deformity was measured by the capitolunate (CL) angle in the lateral CT scans. An angle greater than 30° was considered as a DISI deformity [44]. Grade of postoperative osteoarthritis (POA) was staged in stage 0 (none), stage 1 (mild beaking of the radius without involvement of the radioscaphoid joint), stage 2 (narrowing of the radioscaphoid joint space), and stage 3 (loss of the radioscaphoid joint space) [45].
The following data were collected for statistical and clinical analysis: age, gender, range of motion (ROM), visual analog scale [VAS; ranging from 0 (no pain) to 10 (worst possible pain)], grip strength in kilograms (Jamar, Sammons Preston Rolyan, Mississauga, Ontario, Canada), date of accident, surgery and final check-up.
The patient´s self-assessment by patients was registered on the Disability of the Arm, Shoulder and Hand (DASH) score (0–100 points) [46], the Patient-rated Wrist Evaluation (PRWE) (0–100 points) [47] and the Michigan Hand Outcomes Questionnaire (MHQ) (0–100 points) [48]. In addition, the modified Green O´Brien (Mayo) Wrist score (0–100 points) [49] was used.
Statistical methods
Shapiro test was used to test the assumption of normal distribution of scaled parameters. Since this assumption could not be upheld, the outcome was analyzed non-parametrically using Mann–Whitney U test to compare differences between the two groups with and without ESWT treatment. To compare scaled parameters between one, two HCS or plate, the Kruskal–Wallis test was used. If Kruskal–Wallis test was significant, post hoc analysis was performed by using the Mann–Whitney U test.
Fisher’s exact test was used for nominal parameters to determine differences in frequency distribution between the two groups.
Union rates were compared by calculating 95% confidence intervals, whereas non-overlapping intervals indicated a significant difference at the 5% level. Threshold for statistical significance was p < 0.05.
Patients characteristics
A total of 58 scaphoid nonunions that matched the inclusion criteria were invited to attend the follow-up investigation. Of these, 13 patients were unavailable and three declined to attend the follow-up investigation. Therefore, the final clinical and radiological analysis totaled 42 (40 men and 2 female) patients with a mean age of 32 (range 18–71) and mean follow-up interval of 52 months (range 4–144). Mean interval between injury and surgery of the nonunion was 29 (range 6–175) months. 27 of 42 (64%) patients presented with either non-diagnosed fractures or those that failed to heal conservatively. 15/42 (36%) developed a nonunion despite previous surgery.
Twenty-six (62%) were also treated with additional ESWT within 2 weeks after surgery with a mean age of 31 (range 18–71) years and follow-up interval of 29 (range 4–67) months and 16 (38%) only had surgery with a mean age of 34 (range 18–48) years and follow-up interval of 97 (range 32–144) months. No significant differences could be found in either age (p = 0.24) and gender distribution (p = 0.52) or time elapsed between injury and surgery of the nonunion (21 months ESWT group versus 42 months without ESWT group; p = 0.34). Follow-up interval was significantly higher in the group without ESWT (p < 0.001). No significant difference was found regarding the primary treatment of the scaphoid fracture between the group with and without ESWT. 9/26 (35%) were previously treated surgically in the ESWT group and 6/16 (38%) in the group without ESWT (p = 0.55).
Detailed demographic data are presented in Table 1.
A total of 10 patients were stabilized with one HCS, 12 with two HCS and 20 using an angular stable scaphoid plate. In the ESWT group four patients were stabilized with one HCS, nine with two HCS and 13 with an angular stable plate. In the group without ESWT, six were stabilized with one HCS, three with two HCS and seven with an angular stable scaphoid plate. No significant differences were found regarding the stabilization methods between the groups (p = 0.22). The mean interval between injury and surgery of the nonunion (one HCS: 31 months, two HCS: 26 months, plate: 30 months; p > 0.05) and follow-up intervals did not differ significantly between the groups (p > 0.05).
Detailed demographic data are given in Table 2.
Results
79% (33/42) of the scaphoid nonunion showed bony healing at the final check-up. Nonunion persisted in the remaining 9/42 patients. Seven of the nine patients were pain-free and refused any further treatment, one had a proximal row carpectomy and the other patient a four-corner arthrodesis procedure.
Mean range of motion in extension/flexion was 144 (SD 33)°, in supination/pronation 172 (SD 23)° and in radial/ulnar deviation 48 (SD 9)°. In mean, patients regained 88% of ROM in extension/flexion, 96% of supination/pronation and 87% of radial/ulnar deviation compared to the uninjured hand. Grip strength was in mean 40 kg or 84% of the uninjured hand. Pain according to the VAS was in mean 1.27 (SD 1.95)°. DASH Score was in mean 12.6 (SD 15.4) points, PRWE Score 15.6 (SD 19.4) points and the MHQ 83.4 (SD 17.7) points. Compared to the uninjured hand patients had 87% of the MHQ on the injured hand. The Mayo Wrist Score showed a “good” clinical outcome with a mean of 83 (SD 16.0) points.
With or without ESWT
The ESWT group presented 21/26 (81%) healed scaphoid nonunions, whereas the group without ESWT showed union in 12/16 (75%) patients (p > 0.05). Pain according to the VAS (p = 0.02) was significantly lower and modified Green O´Brien score higher in the ESWT group (p = 0.01) than in the group without ESWT. Patients in the ESWT group showed with a mean of 89 (SD 12) points a “good”, whereas the group without ESWT had only a “fair” outcome, and a mean of 72 (SD 17) points in the Green O´Brien score.
No significant differences could be found between the groups in ROM, grip strength, DASH score, PRWE score, MHQ, H/L ratio or CL angle.
Detailed information is presented in Tables 1, 3 and 4.
Stabilization with one, two HCS or angular stable scaphoid plate
Patients stabilized with one HCS showed 6/10 (60%), with two HCS 10/12 (83%) and with a scaphoid plate 17/20 (85%) union. No significant differences could be found regarding union rates between the groups (p > 0.05).
No significant differences could be found between the groups with respect to VAS, ROM, grip strength, PRWE Score, DASH Score, MHQ, H/L ratio and CL angle.
Detailed information is shown in Tables 2, 5 and 6.
Three patient examples are given in Figs. 2, 3 and 4.

20-year-old man, injury to his dominant right hand in December 2009. a The patient was initially treated in another hospital after injuring his right hand. X-rays showed a scaphoid fracture with bony avulsion. b X-rays after stabilizing the scaphoid fracture with one HCS 10 days after injury. c, d CT scans in October 2010 (10 months after surgery of the scaphoid fracture) showing a scaphoid nonunion with loosening of the screw and a humpback deformity. e Follow-up surgery in December 2010 using a nonvascularized bone graft from the iliac crest and K-wire stabilization (11 months after the primary surgery). f, g Patients attended our outpatient clinic in June 2011 (6 months post-operatively of the nonunion) CT scan showed no bony healing and K-wire loosening. h–k Scaphoid nonunion was stabilized with a plate and nonvascularized bone graft from the iliac crest at our hospital (December 2011; 24 months after primary injury) and also ESWT within 2 weeks. At the follow-up the X-rays and CT scans of the scaphoid showed bony. l Intraoperative view with an angular stable scaphoid plate

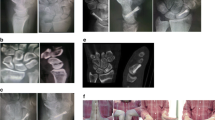
21-year-old man, injury to his dominant right hand. a–d Patient attended our outpatient clinic, 35 months after a fall on his right hand. Initially he did not seek help. His CT scan and MRI showed a nonunion of the scaphoid with cyst formation and humpback deformity. e The scaphoid nonunion was treated with a nonvascularized bone graft from the iliac crest and double HCS fixation. Additionally, the patient received ESWT within 2 weeks after surgery. f–m X-rays and CT scans at follow-up showing the bony healing of the scaphoid nonunion and stabilization with the two HCS

33-year-old man, injury to his dominant right hand. a–c Patient arrived at our outpatient clinic after 8 months, complaining of pain in his right wrist without any recollection of an accident. X-rays and CT scans showed scaphoid nonunion. d, e The nonunion was treated with a nonvascularized bone graft from the iliac crest and stabilized by a plate plus ESWT treatment. f, g CT scan at follow-up showing the healed scaphoid nonunion. The plate was removed 9 months after surgery due to the persisting restriction in wrist flexion
Discussion
Scaphoid nonunion continues to be challenging for hand surgeons and when it occurs, has considerable consequences in patient's hand function. Studies focusing on the long-term outcome after scaphoid nonunion showed that the natural history includes progression to arthritis and wrist pain in the majority of the patients over time [50,51,52,53,54,55,56,57]. Therefore, main aim of treating scaphoid nonunion is to achieve union, correct the deformity, relieve symptoms, improve the range of motion, and prevent progression of osteoarthritis [13, 14, 58].
The limitations of the present study need to be considered before interpretation. Firstly, it was a retrospective follow-up investigation, therefore not randomized. Indications for ESWT were established by two of the authors, as they used ESWT in all of their treated patients since 2010 ESWT. Due to the limited inclusion criteria, the sample size comprised 58 patients of which 16 were excluded for various reasons.
This study included three different types of stabilization methods as well as an additional subdivision of two groups (with ESWT group versus without ESWT group). Therefore, the analysis of the different outcomes in bony healing depending on ESWT and fixation method necessarily became small groups. Even the descriptive analysis would have shown no conclusive results because of the small sample size. This also accounted for the fact that no significant differences could be determined when comparing union rate between with/without ESWT, or stabilization method. To prove a difference between a union rate of 88% and 91%, conclusively, 3.400 patients (80% power and 5% significance level) are mandatory [59]. Therefore, many more case series are required to qualify for systematic reviews.
It is also not possible to make any valid statements regarding the time to union in the different groups because not all patients were followed up continually (some of the patients only returned on request) and there was no standard follow-up protocol. Conclusive data on improvement of range of motion, grip strength or functional outcome scores were also not possible as no reference value was established prior to surgery. Because of the promising results in the literature [27], some of the authors in this study started to use ESWT in addition to surgery in 2010. Thus, the follow-up interval was significantly higher in patients treated without ESWT, which could have impacted on the significant higher pain and poorer modified Green O´ Brien score in the group without ESWT.
Surgical treatment of scaphoid nonunion was first described by Adams et al. [60] in 1928. However, it was Matti and Russe’s technique that changed the overall view on bone grafting. Only after introduction of the headless bone screw by Herbert and Fisher in 1984 [36] did the treatment of scaphoid fractures and nonunions become revolutionized. Whipple and other surgeons, modified the screw into the HCS and thus made percutaneous treatment possible [61, 62]. The advantages lie in a minimal invasive percutaneous approach. Displaced scaphoid fractures and nonunions are typically treated with a single variable-pitch compression screw. Therefore, many authors consider non-vascularized bone grafting and internal screw fixation as the standard therapy in treating scaphoid nonunions to date [63, 64].
Looking at the multidirectional movement of the scaphoid during extension/flexion, radial/ulnar deviation and dart-throwing motion, it is easily conceivable, that a single screw may not provide total stability, especially against rotational forces [40, 65, 66]. Bending strength and resistance is biomechanically well researched in the literature, but only few studies have focused on rotational stability. Jurkowitsch et al. showed in a recent biomechanical study that stabilization of scaphoid waist fractures using two HCS or scaphoid plate has a significantly higher resistance against rotational forces than using only one HCS [67]. Mandaleson et al. compared one, two HCS and scaphoid plate in load to failure in a scaphoid nonunion model and found a significantly greater stability, stiffness and energy absorption when stabilizing with two HCS and scaphoid plate than when using only one HCS. Additionally, they found out that the main mode of failure in one HCS was a rotational failure. As in the study by Jurkowitsch et al. [68], no significant differences could be found between two HCS and scaphoid plate fixation. Other biomechanical studies also tested load to failure between screw and plate fixation. They showed similar results between screw and plate fixation, but plate fixation proved superior to screw fixation in gap recovery after applied load to failure and in osteopenic bone [69, 70].
Aiming to increase rotational stability, several authors started using derotational K-wires [71, 72]. Garcia et al. did a retrospective review on 19 patients that were treated by two HCS to increase the rotational stability. In all cases, evidence for clinical and radiological bone union after a mean of 3.6 months could be reported [40]. Similarly, another study reported higher union rates in unstable scaphoid type B2 fractures, when stabilized with two HCS compared to one HCS [37].
Screw fixation of scaphoid nonunions is more suitable in waist fractures with minimal bone loss. Recent studies reported technical difficulties especially in cases of nonunions with palmar bone defects and small proximal pole fragments [73]. Another disadvantage is the bone graft extrusion whilst inserting the screw and therefore the use of a small impactor is recommended during screw insertion [74, 75]. As a result, some surgeons started using plates in the fixation of scaphoid nonunions. The Ender plate, the first plate used for scaphoid fixation, was first published in 1977 [22]. Huene and Stankovic used the Ender plate in scaphoid nonunions and both achieved a union rate by 95% [23, 24]. Plates have been developed and further improved since the Ender plate. Braun et al. and Ghoneim used a buttress plate for stabilization of scaphoid nonunions including a non-vascularized bone graft from the iliac crest. They reported a union rate of 93 and 94% [64, 76]. Leixnering et al. [17] reported a 100% union rate in 11 patients that were treated with a plate for scaphoid nonunion. Nowadays, low-profile plates with angular stable screw fixation systems are available [77]. Dodds et al. [77] treated nine patients with recalcitrant scaphoid waist nonunion using plate fixation and volar carpal artery vascularized bone grafting, they reported union in eight of nine (88%) patients.
Generally, the union rates for non-vascularized bone grafting are reported to range between 80 and 90% [13], yet the union rates do not differ significantly if harvested from either the distal radius or iliac crest (89% distal radius, 88% iliac crest) [59]. In 2012 Garg et al. [78] published a prospective randomized trial comparing nonvascularized bone grafting from the iliac crest and distal radius. Both graft types showed union at about 87% and no significant differences in ROM and functional scores. Patients presenting with scaphoid nonunion for longer than 1 year were excluded from this study, and therefore mean duration between injury and surgery was 4.5 months in the distal radius group and 5.4 months in the iliac crest group. A 79% union rate was shown in this study, and ROM in extension/flexion and grip strength was slightly better in the study by Garg et al [78]. This may be due to the fact, that interval between injury and surgery of the scaphoid in this study, was clearly longer with a mean of 29 months. Schreuder et al. retrospectively reviewed 18 scaphoid nonunions using a nonvascularized bone graft from the iliac crest. They showed union in 13/18 (72%) of the nonunions. The mean interval between injury and surgery of 27 months was comparable, but they also included patients with a shorter than 6-month interval. In comparison this study showed marginally higher union rates when treated with ESWT and two HCS or scaphoid plate. ROM, grip strength, DASH Score and PRWE Score were similar in both studies [79].
Extracorporeal shockwave therapy has been an established procedure for a few decades now, showing union rates from 50 to 85% [26]. The effects of ESWT on bone are poorly investigated. The current hypothesis is based on the induction of osteogenesis through stimulation of angiogenesis, release of growth factors and subsequent callus formation [80]. Several studies showed that ESWT leads to cell membrane hyperpolarization, followed by an increased release of growth factors. ESWT also increases oxygen radicals, which leads to induction of growth factors and the differentiation of mesenchymal cell towards osteoprogenitors. In addition, ESWT stimulates the migration of mesenchymal stem cells into the treated tissue. These processes culminate to intensify the blood supply to the treated tissue [29,30,31,32,33]. In an animal study, Wang et al. investigated the effects of ESWT on bone healing in rabbits with femoral fractures. They were treated with ESWT and results showed significantly better bone strength, more cortical bone formation, more numerous neo-vessels, and a rise in angiogenic and osteogenic growth markers. One can therefore conclude that ESWT improves bone healing through greater neovascularization and up-regulation of angiogenic and osteogenic growth factors [81].
Wang et al. were the first to describe the effects of combined surgery and ESWT in displaced diaphyseal fractures of the femur and the tibia; the patients received ESWT immediately after surgery. Union rates were significantly better in those who received both treatments than in the surgery-only group [28]. Cacchio et al. prospectively randomized patients with hypertrophic long-bone nonunions into two ESWT groups and one surgery group. Union rates after 6 months were 70% and 71% in the two ESWT groups, and 74% in the surgery-only group; the difference was not significant. At 6 and 12 months the DASH Score and VAS Score were significantly better in the ESWT groups than in the surgery-only group [82]. According to many clinical studies, the effectiveness of ESWT depends on the type of nonunion: hypertrophic nonunions treated with ESWT are associated with higher success rates than atrophic nonunions [25].
Very few studies exist that focus on the effects of scaphoid nonunion and ESWT. In 21 scaphoid nonunions, Schaden et al. [27] achieved union in 14 of 21 cases treated only with ESWT. In a recent randomized controlled trial, Notarnicola et al. compared scaphoid nonunions treated only with ESWT and the other group, surgically with the Matti–Russe’s technique. They registered a union rate of 79% in the ESWT group and 78% in the operatively treated group, respectively. At the 12-month follow-up, no significant differences were shown between the two groups regarding union and functional outcome [83].
Despite the limitations of the study, patients with ESWT, two HCS or plate stabilization showed similar results to patients with one HCS or without ESWT. One can only assume that these differences could reach statistical significance in bigger study groups. In our opinion ESWT increases vascularity in the treated tissue and stabilization with two HCS or plate, increases rotational stability and therefore new vessel formation is protected.
More studies comprising larger patient populations—especially multicenter prospective randomized trials—are needed to confirm the positive effects of a combined treatment. Further studies should also be carried out to confirm the higher union rates attained when using a scaphoid plate or two HCS.
Conclusions
The results of this retrospective study suggest that a stabilization by two HCS or scaphoid plate provides higher unions rates than a stabilization by one HCS and a combination of ESWT and surgery is suitable in treating scaphoid nonunions.
References
Duckworth AD, Jenkins PJ, Aitken SA et al (2012) Scaphoid fracture epidemiology. J Trauma Acute Care Surg 72:1. https://doi.org/10.1097/TA.0b013e31822458e8
Hove LM (1999) Epidemiology of scaphoid fractures in Bergen, Norway. Scand J Plast Reconstr Surg Hand Surg 33:423–426. https://doi.org/10.1080/02844319950159145
Schmidle G, Ebner HL, Klauser AS et al (2018) Correlation of CT imaging and histology to guide bone graft selection in scaphoid non-union surgery. Arch Orthop Trauma Surg. 1–11
Mallee WH, Mellema JJ, Guitton TG et al (2016) 6-week radiographs unsuitable for diagnosis of suspected scaphoid fractures. Arch Orthop Trauma Surg 136:771–778. https://doi.org/10.1007/s00402-016-2438-4
Rein S, Hanisch U, Rammelt S et al (2010) Histopathological, radiological and clinical aspects of the temporal assignment of scaphoid non-union. Arch Orthop Trauma Surg 130:1243–1250. https://doi.org/10.1007/s00402-009-1010-x
Kahl T, Razny FK, Benter JP et al (2016) Diagnosis of the scaphoid bone: fractures, nonunion, circulation, perfusion. Orthopade 45:938–944. https://doi.org/10.1007/s00132-016-3333-y
Schädel-Höpfner M, Bickert B, Dumont C et al (2016) Acute scaphoid fractures: Management under consideration of the new S3-level guideline. Orthopade 45:945–950. https://doi.org/10.1007/s00132-016-3336-8
Cooney WP, Dobyns JH, Linscheid RL (1980) Fractures of the scaphoid: a rational approach to management. Clin Orthop Relat Res 149: 90–97
Dias JJ, Brenkel IJ, Finlay DB (1989) Patterns of union in fractures of the waist of the scaphoid. Bone Joint J 71–B:307–310
Muramatsu K, Doi K, Kuwata N et al (2002) Scaphoid fracture in the young athlete–therapeutic outcome of internal fixation using the Herbert screw. Arch Orthop Trauma Surg 122:510–513. https://doi.org/10.1007/s00402-002-0417-4
Neshkova IS, Jakubietz RG, Kuk D et al (2015) [Percutaneous screw fixation of non- or minimally displaced scaphoid fractures]. Oper Orthop Traumatol 27:448–454. https://doi.org/10.1007/s00064-014-0325-0
Langer MF, Oeckenpöhler S, Breiter S et al (2016) Anatomy and biomechanics of the scaphoid. Orthopade 45:926–937. https://doi.org/10.1007/s00132-016-3339-5
Buijze GA, Ochtman L, Ring D (2012) Management of scaphoid nonunion. J Hand Surg Am 37:1095–1100. https://doi.org/10.1016/j.jhsa.2012.03.002
Pao VS, Chang J (2003) Scaphoid nonunion: diagnosis and treatment. Plast Reconstr Surg 112:1666–1669
Griffis CE, Olsen C, Nesti L et al (2017) Validity of computed tomography in predicting scaphoid screw prominence: a cadaveric study. Arch Orthop Trauma Surg 137:573–577. https://doi.org/10.1007/s00402-017-2658-2
Quadlbauer S, Pezzei C, Jurkowitsch J et al (2017) Spontaneous radioscapholunate fusion after septic arthritis of the wrist: a case report. Arch Orthop Trauma Surg 137:579–584. https://doi.org/10.1007/s00402-017-2659-1
Leixnering M, Pezzei C, Weninger P et al (2011) First experiences with a new adjustable plate for osteosynthesis of scaphoid nonunions. J Trauma Inj Infect Crit Care 71:933–938. https://doi.org/10.1097/TA.0b013e3181f65721
Kawamura K, Chung KC (2008) Treatment of scaphoid fractures and nonunions. J Hand Surg Am 33:988–997
Hannemann PFW, Brouwers L, Dullaert K et al (2015) Determining scaphoid waist fracture union by conventional radiographic examination: an analysis of reliability and validity. Arch Orthop Trauma Surg 135:291–296. https://doi.org/10.1007/s00402-014-2147-9
Meszaros T, Vögelin E, Mathys L, Leclère FM (2018) Perilunate fracture-dislocations: clinical and radiological results of 21 cases. Arch Orthop Trauma Surg 138:287–297. https://doi.org/10.1007/s00402-017-2861-1
Roh YH, Noh JH, Lee BK et al (2014) Reliability and validity of carpal alignment measurements in evaluating deformities of scaphoid fractures. Arch Orthop Trauma Surg 134:887–893. https://doi.org/10.1007/s00402-014-1998-4
Ender HG (1977) A new method of treating traumatic cysts and pseudoarthrosis of the scaphoid (author’s transl). Unfallheilkunde 80:509–513
Stankovic P, Burchhardt H (1993) Experience with the Ender hooked plate in the management of 42 scaphoid pseudarthroses. HandchirMikrochir Plast Chir 25:217–222
Huene DR, Huene DS (1991) Treatment of nonunions of the scaphoid with the Ender compression blade plate system. J Hand Surg Am 16:913–922. https://doi.org/10.1016/S0363-5023(10)80160-1
Birnbaum K, Wirtz DC, Siebert CH, Heller KD (2002) Use of extracorporeal shock-wave therapy (ESWT) in the treatment of non-unions. a review of the literature. Arch Orthop Trauma Surg 122:324–330. https://doi.org/10.1007/s00402-001-0365-4
Wang CJ (2012) Extracorporeal shockwave therapy in musculoskeletal disorders. J Orthop Surg Res 7:11. https://doi.org/10.1186/1749-799X-7-11
Schaden W, Fischer A, Sailler A (2001) Extracorporeal shock wave therapy of nonunion or delayed osseous union. Clin Orthop Relat Res 387:90–94. https://doi.org/10.1097/00003086-200106000-00012
Wang CJ, Liu HC, Fu TH (2007) The effects of extracorporeal shockwave on acute high-energy long bone fractures of the lower extremity. Arch Orthop Trauma Surg 127:137–142. https://doi.org/10.1007/s00402-006-0236-0
Wang FS, Wang CJ, Sheen-Chen SM et al (2002) Superoxide mediates shock wave induction of ERK-dependent osteogenic transcription factor (CBFA1) and mesenchymal cell differentiation toward osteoprogenitors. J Biol Chem 277:10931–10937. https://doi.org/10.1074/jbc.M104587200
Wang FS, Yang KD, Chen RF et al (2002) Extracorporeal shock wave promotes growth and differentiation of bone-marrow stromal cells towards osteoprogenitors associated with induction of TGF-β1. J Bone Jt Surg 84:457–461. https://doi.org/10.1302/0301-620X.84B3.11609
Chen YJ, Wurtz T, Wang CJ et al (2004) Recruitment of mesenchymal stem cells and expression of TGF-β1 and VEGF in the early stage of shock wave-promoted bone regeneration of segmental defect in rats. J Orthop Res 22:526–534. https://doi.org/10.1016/j.orthres.2003.10.005
Wang FS, Wang CJ, Chen YJ et al (2004) Ras induction of superoxide activates ERK-dependent angiogenic transcription factor HIF-1α and VEGF-A expression in shock wave-stimulated osteoblasts. J Biol Chem 279:10331–10337. https://doi.org/10.1074/jbc.M308013200
Wang FS, Yang KD, Wang CJ et al (2004) Shockwave stimulates oxygen radical-mediated osteogenesis of the mesenchymal cells from human umbilical cord blood. J Bone Miner Res 19:973–982. https://doi.org/10.1359/JBMR.040121
Wang CJ, Wang FS, Yang KD et al (2003) Shock wave therapy induces neovascularization at the tendon-bone junction. A study in rabbits. J Orthop Res 21:984–989. https://doi.org/10.1016/S0736-0266(03)00104-9
Low CK, Ang BT (1999) Herbert screw fixation of scaphoid fractures. Hand Surg 04:63–66. https://doi.org/10.1142/S0218810499000022
Herbert TJ, Fisher WE (1984) Management of the fractured scaphoid using a new bone screw. J Bone Joint Surg Br 66:114–123
Quadlbauer S, Beer T, Pezzei C et al (2017) Stabilization of scaphoid type B2 fractures with one or two headless compression screws. Arch Orthop Trauma Surg 137:1587–1595. https://doi.org/10.1007/s00402-017-2786-8
Dodds SD, Panjabi MM, Slade JF (2006) Screw fixation of scaphoid fractures: a biomechanical assessment of screw length and screw augmentation. J Hand Surg Am 31:405–413. https://doi.org/10.1016/j.jhsa.2005.09.014
McCallister WV, Knight J, Kaliappan R, Trumble TE (2003) Central placement of the screw in simulated fractures of the scaphoid waist: a biomechanical study. J Bone Jt Surg Ser A 85:72–77. https://doi.org/10.2106/00004623-200301000-00012
Garcia RM, Leversedge FJ, Aldridge JM et al (2014) Scaphoid nonunions treated with 2 headless compression screws and bone grafting. J Hand Surg Am 39:1301–1307. https://doi.org/10.1016/j.jhsa.2014.02.030
Grewal R, Frakash U, Osman S, McMurtry RY (2013) A quantitative definition of scaphoid union: determining the inter-rater reliability of two techniques. J Orthop Surg Res https://doi.org/10.1186/1749-799X-8-28
Krimmer H, Krapohl B, Sauerbier M, Hahn P (1997) Post-traumatic carpal collapse (SLAC- and SNAC-wrist)—stage classification and therapeutic possibilities. Handchir Mikrochir Plast Chir 29:228–233
Bain GI, Bennett JD, MacDermid JC et al (1998) Measurement of the scaphoid humpback deformity using longitudinal computed tomography: Intra- and interobserver variability using various measurement techniques. J Hand Surg Am 23:76–81. https://doi.org/10.1016/S0363-5023(98)80093-2
Greenspan A (2011) Orthopedic imaging: a practical approach. Lippincott Williams & Wilkins, Philadelphia
Trumble TE, Gilbert M, Murray LW et al (2000) Displaced scaphoid fractures treated with open reduction and internal fixation with a cannulated screw. J Bone Joint Surg Am 82:633–641
Hudak PL, Amadio PC, Bombardier C (1996) Development of an upper extremity outcome measure: The DASH (disabilities of the arm, shoulder, and head). Am J Ind Med 29:602–608. https://doi.org/10.1002/(SICI)1097-0274(199606)29:6%3C602::AID-AJIM4%3E3.0.CO;2-L
Hemelaers L, Angst F, Drerup S et al (2008) Reliability and validity of the german version of “the patient-rated wrist evaluation (PRWE)” as an outcome measure of wrist pain and disability in patients with acute distal radius fractures. J Hand Ther 21:366–376. https://doi.org/10.1197/j.jht.2008.03.002
Knobloch K, Kuehn M, Papst S et al (2011) German standardized translation of the michigan hand outcomes questionnaire for patient-related outcome measurement in dupuytren disease. Plast Reconstr Surg 128:39e–40e. https://doi.org/10.1097/PRS.0b013e318218fd70
Amadio PC, Berquist TH, Smith DK et al (1989) Scaphoid malunion. J Hand Surg Am 14:679–687. https://doi.org/10.1016/0363-5023(89)90191-3
Inoue G, Sakuma M (1996) The natural history of scaphoid non-union. Arch Orthop Trauma Surg 115:1–4. https://doi.org/10.1007/BF00453208
Euler S, Erhart S, Deml C et al (2014) The effect of delayed treatment on clinical and radiological effects of anterior wedge grafting for non-union of scaphoid fractures. Arch Orthop Trauma Surg 134:1023–1030. https://doi.org/10.1007/s00402-014-2007-7
Schädel-Höpfner M, Marent-Huber M, Gazyakan E et al (2010) Acute non-displaced fractures of the scaphoid: earlier return to activities after operative treatment. A controlled multicenter cohort study. Arch Orthop Trauma Surg 130:1117–1127. https://doi.org/10.1007/s00402-009-1004-8
Arora R, Gschwentner M, Krappinger D et al (2007) Fixation of nondisplaced scaphoid fractures: making treatment cost effective. Prospective controlled trial. Arch Orthop Trauma Surg 127:39–46. https://doi.org/10.1007/s00402-006-0229-z
Spies CK, Hohendorff B, Müller LP et al (2016) Proximal carpal row carpectomy. Oper Orthop Traumatol 28:204–217. https://doi.org/10.1007/s00064-016-0440-1
Spies C, Unglaub F (2017) (Partial) arthrodesis of the hand and wrist. Oper Orthop Traumatol 29:373. https://doi.org/10.1007/s00064-017-0518-4
Hernekamp J-F, Kneser U, Kremer T, Bickert B (2017) Mediokarpale teilarthrodese mit winkelstabiler Plattenosteosynthese. Oper Orthop Traumatol 29:409–415. https://doi.org/10.1007/s00064-017-0514-8
Unglaub F, Langer MF, Unglaub JM et al (2017) (Partial) fusion of the wrist: Indications and surgical procedures. Unfallchirurg 120:513–526. https://doi.org/10.1007/s00113-017-0356-8
Citak M, O’Loughlin PF, Kendoff D et al (2010) Navigated scaphoid screw placement using customized scaphoid splint: an anatomical study. Arch Orthop Trauma Surg 130:889–895. https://doi.org/10.1007/s00402-010-1044-0
Pinder RM, Brkljac M, Rix L et al (2015) Treatment of scaphoid nonunion: a systematic review of the existing evidence. J Hand Surg Am 40:1797–1805. https://doi.org/10.1016/j.jhsa.2015.05.003
Adams JD, Leonard RD (1928) Fracture of the carpal scaphoid. N Engl J Med 198:401–404. https://doi.org/10.1056/NEJM192804121980803
Whipple TL (1995) Stabilization of the fractured scaphoid under arthroscopic control. Orthop Clin North Am 26:749–754
Inoue G, Shionoya K (1997) Herbert screw fixation by limited access for acute fractures of the scaphoid. J Bone Jt Surg 79:418–421. https://doi.org/10.1302/0301-620X.79B3.7254
Munk B, Larsen CF (2004) Bone grafting the scaphoid nonunion: A systematic review of 147 publications including 5 246 cases of scaphoid nonunion. Acta Orthop Scand 75:618–629
Ghoneim A (2011) The unstable nonunited scaphoid waist fracture: Results of treatment by open reduction, anterior wedge grafting, and internal fixation by volar buttress plate. J Hand Surg Am 36:17–24. https://doi.org/10.1016/j.jhsa.2010.10.003
Moojen TM, Snel JG, Ritt MJPF et al (2002) Scaphoid kinematics in vivo. J Hand Surg Am 27:1003–1010. https://doi.org/10.1053/jhsu.2002.36519
Wolfe SW, Neu C, Crisco JJ (2000) In vivo scaphoid, lunate, and capitate kinematics in flexion and in extension. J Hand Surg Am 25:860–869. https://doi.org/10.1053/jhsu.2000.9423
Jurkowitsch J, Dall’Ara E, Quadlbauer S et al (2016) Rotational stability in screw-fixed scaphoid fractures compared to plate-fixed scaphoid fractures. Arch Orthop Trauma Surg 136:1623–1628. https://doi.org/10.1007/s00402-016-2556-z
Mandaleson A, Tham SK, Lewis C et al (2017) Scaphoid fracture fixation in a nonunion model: a biomechanical study comparing 3 types of fixation. J Hand Surg Am. https://doi.org/10.1016/j.jhsa.2017.10.005
Goodwin J, Castañeda P, Drace P, Edwards S (2017) A biomechanical comparison of screw and plate fixations for scaphoid fractures. J Wrist Surg. https://doi.org/10.1055/s-0037-1606123
Goodwin JA, Castañeda P, Shelhamer RP et al (2017) A Comparison of Plate Versus Screw Fixation for Segmental Scaphoid Fractures: A Biomechanical Study. Hand (NY). https://doi.org/10.1177/1558944717732065
Trumble TE, Clarke T, Kreder HJ (1996) Non-union of the scaphoid. Treatment with cannulated screws compared with treatment with Herbert screws. J Bone Joint Surg Am 78:1829–1837
Manske PR, McCarthy JA, Strecker WB (1988) Use of the Herbert bone screw for scaphoid nonunions. Orthopedics 11:1653–1661
Stark A, Brostrom LA, Svartengren G (1987) Scaphoid nonunion treated with the Matti–Russe technique. Long-term results. Clin Orthop Relat Res. 214 175–180
Nakamura R, Horii E, Watanabe K et al (1993) Scaphoid non-union: factors affecting the functional outcome of open reduction and wedge grafting with herbert screw fixation. J Hand Surg (British Eur Vol 18:219–224. https://doi.org/10.1016/0266-7681(93)90114-U
Cooney WP, Linscheid RL, Dobyns JH, Wood MB (1988) Scaphoid nonunion: role of anterior interpositional bone grafts. J Hand Surg Am 13:635–650. https://doi.org/10.1016/S0363-5023(88)80116-3
Braun C, Gross G, Buhren V (1993) Osteosynthesis using a buttress plate-a new principle for stabilizing scaphoid pseudarthroses. Unfallchirurg 96:9–11
Dodds SD, Halim A (2016) Scaphoid plate fixation and volar carpal artery vascularized bone graft for recalcitrant scaphoid nonunions. J Hand Surg Am 41:e191–e198. https://doi.org/10.1016/j.jhsa.2016.04.021
Garg B, Goyal T, Kotwal PP et al (2013) Local distal radius bone graft versus iliac crest bone graft for scaphoid nonunion: a comparative study. Musculoskelet Surg 97:109–114. https://doi.org/10.1007/s12306-012-0219-y
Schreuder M, Degreef I, De Smet L (2008) Treatment of scaphoid non-unions with a corticocancellous graft and Herbert screw fixation: results at five years follow-up. Acta Orthop Belg 74:24–28
Haupt G, Haupt A, Ekkernkamp A et al (1992) Influence of shock waves on fracture healing. Urology 39:529–532. https://doi.org/10.1016/0090-4295(92)90009-L
Wang CJ, Wang FS, Yang KD (2008) Biological effects of extracorporeal shockwave in bone healing: a study in rabbits. Arch Orthop Trauma Surg 128:879–884. https://doi.org/10.1007/s00402-008-0663-1
Cacchio A, Giordano L, Colafarina O et al (2009) Extracorporeal shock-wave therapy compared with surgery for hypertrophic long-bone nonunions. J Bone Jt Surg Ser A 91:2589–2597. https://doi.org/10.2106/JBJS.H.00841
Notarnicola A, Moretti L, Tafuri S et al (2010) Extracorporeal shockwaves versus surgery in the treatment of pseudoarthrosis of the carpal scaphoid. Ultrasound Med Biol 36:1306–1313. https://doi.org/10.1016/j.ultrasmedbio.2010.05.004
Acknowledgements
We thank Rose-Marie Sedlacek for proof reading this article. Without her help, this English publication would not have been possible.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Dr. Schaden reports other financial activities apart from the submitted study. [Shareholder of Tissue Regeneration Technology (TRT, Atlanta).] In addition, Dr. Schaden has issued several patents with some still pending, for example: stimulating the regeneration of biological tissue using shockwaves.
All other authors of this manuscript certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Ethical approval
Institutional review board approval was obtained for this retrospective follow-up study.
Ethical standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Institutional review board approval was obtained for this study.
Rights and permissions
About this article

Cite this article
Quadlbauer, S., Pezzei, C., Beer, T. et al. Treatment of scaphoid waist nonunion by one, two headless compression screws or plate with or without additional extracorporeal shockwave therapy. Arch Orthop Trauma Surg 139, 281–293 (2019). https://doi.org/10.1007/s00402-018-3087-6
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-018-3087-6