
Abstract
Introduction
The aim of this study was to evaluate the mechanical status of the spine in patients with spastic diplegia 17–26 years after selective dorsal rhizotomy (SDR).
Methods
We compared original radiographic reports from our earlier short-term follow-up study with current X-rays. In addition, we obtained magnetic resonance images (MRI) of the spine and additional information regarding back pain and clinical assessments.
Results
Thirty patients (17 males and 13 females; median age 26.8 years) participated in the current study, with median follow-up times of 4.0 and 21.4 years. Comparison of the X-ray results showed respectively: scoliosis 0% and 57%; kyphosis 0% and 7%; lordosis 21% and 40%; spondylolysis 18% and 37%; and spondylolisthesis grade I occurred in one patient. The only statistically significant difference was found for scoliosis (p < 0.01). The majority had Cobb angles <30° with only two patients with curves of 35°. MRI scans showed spinal stenosis in 27%, black discs in 10%, and disc protrusion in 3%. Daily back pain was reported in 17%, while 23% reported “moderate disability” as a result of back and leg pain. No patient to date has required any surgical intervention on the spine.
Conclusions
Except for spondylolisthesis, spinal deformities did appear to progress with time. However, this increase was not marked, and the development of relatively mild scoliosis was the only statistically significant increase. This group of patients requires continued follow-up. Further studies are required to ascertain the natural history of spinal deformity in adults with spastic diplegia who have not had SDR.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The operation of dorsal rhizotomy was first performed in the early 1900s [10], but gained greater acceptance after Warwick Peacock refined the operative technique in the 1980s while working at the Red Cross Children’s Hospital in Cape Town [32]. During the last decade, various research groups around the world have shown that selective dorsal rhizotomy (SDR) in patients with cerebral palsy (CP) leads to functional improvements during the early years after surgery [9, 43]. Recently, we were able to show sustained long-term benefits in two 20-year follow-up studies [18, 19].
Despite the fact that SDR is invariably successful in its aim of reducing spasticity, spinal instability as a result of laminectomy remains a concern [2, 19, 43]. In the early 1990s, we published studies providing incidences of spinal deformities in children with CP after SDR [34, 35]. These and five other peer-reviewed short-term follow-up studies suggest that the incidence of spinal deformities after SDR varies from 40% to 88%. Deformities include scoliosis in 16–55%, thoracic hyperkyphosis in 1–41%, lumbar hyperlordosis in 7–50%, spondylolysis in 9–12%, and spondylolisthesis in 2–24% of the patient cohorts [12, 17, 34, 35, 42, 44, 47].
However, spinal deformity may also occur as part of the natural history of CP. Morrell et al. [27] reported that patients with CP who did not undergo SDR showed an increased incidence of scoliosis with age, accompanied by increased thoracic and lumbar curves in the sagittal plane and the development of spondylolysis and spondylolisthesis. Three other studies based on institutionalized patients with CP also show increased scoliosis with age [22, 40, 46], while Harada et al. [13] found progressive lordosis and spondylolysis in adults with spastic diplegia. Nevertheless, we do not know whether patients who underwent SDR in childhood have a greater risk for developing spinal deformities over time, as there are no long-term studies that report these changes in adulthood.
Therefore, we aimed to examine the results of clinical, radiographic, and magnetic resonance imaging (MRI) examinations of patients with spastic diplegia more than 15 years after SDR to determine the long-term mechanical status of the spine. In addition, we obtained information regarding the SDR procedure, patients’ demographic characteristics, back pain, and outcomes of clinical assessments to further interpret the results of the radiological studies.
Methods
Patients
We performed a retrospective review of all patients who underwent SDR between 1981 and 1991 at Red Cross Children’s Hospital in Cape Town. In order to facilitate follow-up, we restricted the cohort to those who lived within a radius of 100 km of Cape Town at the time that the operation was performed. Based on detailed inclusion and exclusion criteria (Table 1), a neurosurgeon (JCP) and physiotherapist (NGL) completed the first patient selection. There were 106 patients operated on between 1981 and 1991 of whom 47 met the inclusion criteria. With help from other clinicians, patients, patients’ families, teachers and physiotherapists at schools, and an internet search, we were able to track down 37 of these 47 patients (79%). Thirty patients (64%) agreed to participate in the current study, while seven (15%) chose not to participate (for reasons other than health status).
This study was approved by the Human Ethics Committee at the University of Cape Town, and we obtained informed consent from each participant.
Study design
Data collection took place in 2008 in five different stages and included two visits by the patients: (1) NGL reviewed the historical radiographic reports, which were part of our former short-term follow-up studies [34, 35]; (2) X-rays and MRI scans of the spine were performed at the Medi-Clinic in Stellenbosch; (3) a neurosurgeon (JCP) and an orthopedic surgeon (EBH) examined the scans, blinded to the results of the previous imaging, and consulted two other neurosurgeons (AGF and AAF) if there was any doubt; (4) clinical assessments were performed by a neurosurgeon (JCP) and physiotherapist (NGL); and (5) patients completed the Oswestry Disability Index (ODI) [7] and a self-developed questionnaire which focused on the frequency of spinal, upper, and lower extremity pain.
Outcome measures
X-rays and MRI scans
The method of examination and evaluation of the radiographs was similar to our short-term studies [34, 35]. X-rays were taken in a standing position (or sitting erect if not possible to stand in the first study) holding onto a bar if necessary with antero-posterior (AP), lateral, and oblique views. In the frontal plane, scoliosis was measured by Cobb angles [5]. X-rays in the sagittal plane were used to evaluate thoracic kyphosis (T3–T12) and lumbar lordosis (L1–L5). In line with our previous study [35], the ranges described by Propst-Proctor and Bleck [36] were used as a reference for normal: kyphosis 12–40° and lordosis 23–54°. The incidence of spondylolysis and spondylolisthesis was examined by using lateral and oblique radiographic views. Spondylolisthesis was measured as a percentage of displacement, and was graded by the Meyerding system [25]: grade I (25%), II (50%), III (75%), and IV (100%).
The lumbar spines were examined with MRI (Siemens Magnetom Symphony 1.5 T, Germany) and a body coil. The imaging protocol consisted of the following: (1) sagittal T1- and T2-weighted fast spin-echo from mid-thoracic to sacrum; (2) axial T2-weighted fast spin-echo from L1 to S2; and (3) coronal T1-weighted fast spin-echo from L1 to S2. MRI scans were examined for spinal stenosis, black discs, and disc herniation. In addition to these degenerative disorders, the level of the conus and incidence of any other spinal abnormality were evaluated [26].
Clinical assessments
Clinical examination included evaluation of muscle tone, muscle strength, skin sensation, and deep tendon reflexes in both lower extremities (Table 2). Muscle tone was assessed using the Ashworth Scale [4]. Muscle strength assessments were scored using the Medical Research Council (MRC) scale [24]. Sensation was tested for touch, pin-prick, and deep pressure corresponding to dermatomes from L1 to S4/5. Proprioception was recorded as normal or abnormal. The reflexes evaluated included the plantar reflex and deep tendon reflexes of the hip adductor, rectus femoris, patellar, and Achilles tendons. Scores for the plantar reflex were recorded as either positive or negative, while the outcomes of the deep tendon reflexes were classified by values from 0 to 4.
In addition, patients’ demographics and general clinical characteristics were evaluated. CP diagnosis was confirmed and body weight and height were measured, which resulted in their body mass index (BMI) (underweight = <18.5; normal = 18.5–24.9; overweight = 25.0–29.9; obese = >30.0) [50]. Patients were also questioned about their walking ability, physical problems related to possible sensory loss (bowel, bladder, and sexual problems), and if they had received any other orthopedic interventions. Patients were also classified according to the Gross Motor Functional Mobility Scale (GMFCS) [15, 31], based on the assessors’ observation and self evaluation by the patient.
Pain questionnaires
We used the ODI version 2.0 which is a valid and reliable condition-specific outcome measure for back or leg pain [7, 8]. The questionnaire includes ten sections regarding pain, personal care, lifting, walking, sitting, standing, sleeping, sex life, social life, and traveling. The patients were asked per section to choose one statement which most applied to them, ranging from no problems (score 0) to severe problems (score 5), or they had to indicate that a section was not applicable. When the questionnaire was completed, a percentage was calculated and patients were classified based on their back pain problems during daily activities into: 0–20% indicating “minimal disability”, 20–40% “moderate disability”, 40–60% “severe disability”, 60–80% “housebound”, and 80–100% “bed bound” [7].
We also developed a short questionnaire which focused on the frequency of pain in different parts of the body. Questions were related to pain at spinal level and upper and lower extremities. Frequency of pain per body part could be scored as: never, occasionally, once per month, once per week, daily, or varies (occasionally to several times per week).
Statistical analysis
Data were analyzed using Stata Version 10.0 (Stata Corporation, College Station, USA). We used non-parametric statistics because our sample size was small and not normally distributed. The Wilcoxon signed-rank test was performed to explore changes over time (short-term versus long-term) for the X-ray outcome measures (incidence of scoliosis, kyphosis, lordosis, spondylolysis, and spondylisthesis). A Fisher exact test was used to examine which factors were associated with the radiographic outcomes. Significance levels were set to p ≤ 0.05.
Results
Patients
The study cohort consisted of 30 patients with spastic diplegia (five patients had mild unilateral arm involvement) of whom 17 were male and 13 were female. Seventy percent of patients had laminectomies performed from L1/2 to S1, 10% at levels L1–L5, 10% at L2–L5, 3% at L2–S2, and 7% at L3–S1. The median age of the study cohort at time of SDR was 5.2 ± 5 years (range 2–27 years), and during the current study they were aged 26.8 ± 5 years (21–44 years). The median short-term follow-up time in this cohort of the original study was 4.0 ± 2 years (1–8 years), while the mean current (long-term) follow-up time was 21.4 ± 3 years (17–26 years). All patients were ambulant at follow-up, and the walking ability varied: 20 patients (67%) walked without walking devices, four patients (13%) used one or two crutches only outdoors, and six (20%) patients always had to use their crutches. Half were classified as GMFCS level I, nine patients (30%) as level II, and six patients (20%) as level III.
The mean BMI of the study cohort ranged between 18 and 36; two patients (7%) were classified as underweight, 16 (53%) as normal, six (20%) as overweight, and six (20%) as obese. None of the patients reported problems with sexual, bowel, or bladder function. One patient was diagnosed with Crohn’s disease and another patient with Graves’ disease. This latter patient required oral baclofen medication regularly to reduce muscle spasms. None of the patients who participated in this study ever received intrathecal baclofen or botox before or after SDR. Before SDR, at least one orthopedic surgical operation had been performed on almost half of the cohort (48%), which included muscle releases in 14 patients (48%) and osteotomies of the femur or foot/toes in three patients (10%). After SDR, 18 patients (62%) received orthopedic interventions including muscle releases and osteotomies in 59% and 31% of the study cohort, respectively.
X-rays and MRI scans
Two of the 30 patients did not take part in our short-term follow-up studies [34, 35] and so historical comparison of imaging was only available for 28 patients. Of these 28 patients, none had been initially diagnosed with scoliosis, while at the long-term follow-up study 15 of the 30 patients (50%) had a scoliosis curve of <30° and two (7%) had curves of 35° on the AP X-rays (Figs. 1a and 2a). Scoliosis was significantly more common in the long-term follow-up study (p < 0.01). During our initial study, none of the patients were diagnosed with kyphosis and six patients had lordosis, while in the present study kyphosis and lordosis occurred in two (7%) and 12 (40%) patients, respectively. Although thoracic kyphosis and lumbar lordosis were more frequent at follow-up, these differences were not significant (p = 0.32 and p = 0.13, respectively). Spondylolysis was diagnosed in five patients (11% at L3–4 and 7% at L5–S1) at the short-term follow-up. Despite the fact that four of these patients showed healing of their pars interarticularis, in the long term spondylolysis was reported in 11 patients (15% at L2–3, 38% at L3–4, 31% at L4–5, and 13% at L5–S1), which was not significantly different from the initial study (p = 0.13) (Figs. 1a and 2b). At the first study, one of the five patients had spondylolysis bilaterally at the same level, while in the present study five of the 11 patients with spondylolysis were bilateral. Spondylolisthesis grade I was found in both the short- and long-term follow-up study in only one patient, who was also diagnosed with bilateral spondylolysis at level L3–4 during the first and last study (Fig. 1a).

a Outcomes of X-rays at short-term (I) (n = 28) and long-term (II) (n = 30) follow-up studies. b Outcomes of MRI scans at long-term follow-up study. Note: Incidences of scoliosis include relatively mild scoliosis with the majority of curves <30° and two curves 35°. Spondyl. spondylolysis, Slip grade I spondylolysthesis. Asterisk means that there was a significant difference with p < 0.05

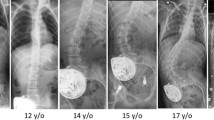
a AP X-ray of a typical patient with mild scoliosis. b An oblique X-ray of a patient with spondylolysis
As shown in Fig. 1b, 18 of the 30 patients (60%) who participated in the long-term follow-up study did not have any abnormalities on their MRI scans. Lumbar stenosis was seen in eight patients (27%) (involving two levels in two patients and three levels in one patient), black discs were seen in six patients (20%), and two patients had disc protrusions (7%), but no disc extrusion or sequestration. Two patients had combined lumbar stenosis and black discs, and all three abnormalities were seen in one patient (without any spinal deformity on X-ray). No other abnormalities were found. The conus was situated at T12 in two patients, at L1 in 18, at the lower border of L1 in one, and at L2 in nine patients. None of the patients who participated in the current study required any spinal operations after their SDR.
Clinical assessments
One patient was not available for the second assessment, and so we only had clinical assessment outcomes of 29 patients. As is apparent from Fig. 3a and b, the majority of our study cohort had normal tone (Ashworth scale 0) and strength (MRC 5) in the various muscle groups evaluated. No patients had abnormalities in proprioception, touch, or deep pressure, and most patients had no impaired pin-prick sensations (Fig. 3c). In addition, most patients had reduced deep tendon reflexes and positive plantar reflexes (Fig. 3d).

Outcomes of the clinical assessments (n = 29). a Muscle tone, b muscle strength, c pin-prick sensation, d deep tendon reflexes. Fl flexion, Ext extension, Ad adduction, Ab abduction, Dors dorsiflexion, Plant plantar flexion
Pain questionnaires
All 30 patients who participated in the long-term follow-up study completed the ODI. Twenty-three patients (77%) scored 0–20% (“minimal disability” because of back pain), while the other seven patients scored 20–40% (“moderate disability”). The outcomes of our self-developed questionnaire are presented in Table 3. Few patients (3–10%) reported pain in their upper extremities, but 23–40% of the patients had pain in their lower extremities. None of the patients suffered from pain in the upper thorax, while 20% of the cohort reported pain at cervical and 67% at lumbosacral spinal level. Pain in the lower back (lumbosacral region) was most common in our study cohort and was reported as occurring on a weekly basis in two patients (7%) and daily in five patients (17%).
Pain was reported on a weekly or daily basis in seven of the 17 patients with scoliosis (41%), one of the two with kyphosis, four of the 12 with lordosis (33%), three of the 11 with spondylolysis (27%), and in the patient who had spondylolisthesis. In addition, daily back pain was reported by one of the eight patients with spinal stenosis, one of the six with a black disc, and one of the two patients with disc protrusion. Eight patients of the current study cohort used medication intermittently to relieve their pain.
Associations with spinal deformities
Table 4 shows the frequency of scoliosis, lordosis and spondylolysis for each different variable related to the SDR operation, patients’ demographic characteristics, MRI scan outcomes, and pain questionnaire. Since kyphosis (n = 2) and spondylolisthesis (n = 1) were rare, we did not include these conditions in our statistical analysis. Scoliosis, lordosis, and spondylolysis were more common when SDR was performed at a young age (2–5 years) compared to older age (>13 years). These differences were smaller between age groups 2–5 years and 6–12 years for scoliosis and spondylolysis, while the incidence of lordosis was still twice as high in the youngest group. In addition, patients who were currently aged between 21 and 25 years had a relatively higher incidence of scoliosis and spondylolysis compared to patients in the oldest age group (>31 years old), while lordosis was diagnosed mostly in the age group 26–30 years old. However, there was no statistically significant difference in the frequency of spinal deformities for the two different follow-up times (16–20 and 21–26 years).
The five patients diagnosed with mild unilateral involvement of an upper extremity were significantly more likely to have spondylolysis than patients with pure spastic diplegia (p = 0.05), but no major differences were seen for scoliosis and lordosis. Females and males had about the same incidence of scoliosis and spondylolysis, but almost twice as many females compared with males were diagnosed with lordosis. Patients’ level of BMI and functioning (GMFCS) was not significantly related to the spinal deformities. However, patients with a higher BMI had a slightly lower frequency of spondylolysis, and spondylolysis was more common in patients with higher levels of functioning (GMFCS I and II).
Disc abnormalities were not associated with radiographic spinal abnormalities. The overall number of spinal abnormalities found with the MRI scans only showed a marginally significant relationship with spondylolysis (p = 0.04). No significant relationships were seen between the outcomes of the validated pain questionnaire and spinal deformities.
Discussion
This follow-up study provides information about the incidence of spinal abnormalities based on X-rays and MRI scans in patients with spastic diplegia (or with minor unilateral involvement of an upper extremity) more than 15 years after they received SDR. Extending the results of short-term follow-up studies after SDR [12, 17, 35, 42, 44, 47], we report further progression of spinal deformities (scoliosis, kyphosis, lordosis, and spondylolysis) in the long term. However, only the incidence of relatively mild scoliosis was statistically significantly increased, and no patients with spondylolysis developed spondylolisthesis. In 60% of our study cohort, we found no MRI abnormalities. The total number of disc degeneration and spinal stenosis was statistically significantly associated with spondylolysis, as well as the diagnosis of spastic diplegia with mild unilateral upper limb involvement. Seventy-seven percent of the study cohort had no or minimal disability because of back or leg pain, and none of the patients required any other spinal interventions.
Scoliosis
Studies of CP patients report various ranges for the incidence of scoliosis, from 38% of patients with CP aged between 14 and 19 [39], 54% in patients older than 20 years [37], to 64% for institutionalized adults [21]. Short-term follow-up studies after SDR (mean follow-up time 4–8 years) describe scoliosis in 17–55% of patients based on sitting and standing radiographs [12, 17, 35, 42, 44, 47].
None of the patients who also participated in our original follow-up study had scoliosis at 4 years (range 1–8 years) after SDR. In the current study, we found an incidence of scoliosis of 57% at 21.4 years (range 17–26 years) after SDR. This increase was statistically significant between the short- and long-term follow-up. However, the majority had curves <30° and only two had curves of 35°. Steinbok et al. (based on standing X-rays) also found the incidence of scoliosis to be 55% and 6% of their patients had curves >35° in a short-term study [44].
Some studies based on institutionalized patients with CP have reported progression of the scoliotic curve with age [22, 40, 46]. In our study, however, the oldest patients had the lowest incidence of scoliosis, and there was no increased incidence with longer follow-up time. However, younger age at SDR (2–5 years old) had a higher incidence of scoliosis. This is in line with the results of other short-term data [44]. On the other hand, this concern might be balanced by the need for less lower limb orthopedic surgery in younger patients [29].
Kyphosis
As far as we could discern, there is very little published data on the natural history of kyphosis in adults with CP. Most short-term follow-up studies after SDR described hyperkyphotic curves between 1% and 16% [12, 17, 35, 42, 47], while one study reported kyphosis in 41% of the patients [44].
None of our patients were diagnosed with kyphosis in the initial short-term follow-up study. However, overall in the long term 7% had kyphosis defined as a thoracic curve >40°. Compared to our own and other short-term follow-up studies, this suggests that there is minimal progression of kyphosis with time. Since only two patients in this study were diagnosed with kyphosis, we were not able to determine associations between different variables.
Lordosis
Harada et al. [13] found in their 84 patients with spastic diplegia an average curve for lumbar lordosis of 54°, which is considered to be the upper limit for normal. In short-term follow-up studies after SDR, the incidence of hyperlordosis varied from 7% to 50% using standing X-rays [12, 17, 35, 42, 44], while a combination of standing and sitting (if standing was not possible) X-rays resulted in an incidence of 21% [44], and another study, where the X-ray position was not described in detail, found 15% [47].
An incidence of 21% was found in the patients who participated in our initial short-term follow-up study, while now more than 15 years after SDR we found an overall incidence of 40%. This is higher compared to other short-term follow-up studies after SDR, with the exception of the study published by Johnson et al. [17], who reported an incidence of 50% after the longest mean follow-up time of 8.6 years.
One of the reasons for the increase in incidence could be the natural history of CP, as Harada et al. [13] and Steinbok et al. [44] found a correlation between hyperlordosis and age of the patients. Golan et al. [12] reported an increased lordosis of 3.6° for each year after SDR, and Johnson et al. [17] reported a higher incidence with longer follow-up time. Although none of our associations were statistically significant, it appeared that young age at SDR (2–5 years) had the highest incidence of lordosis, but patients who were classified in the longest follow-up time group had only an 11% higher incidence. As with scoliosis, these observations need further investigation as other factors (such as the need for orthopedic surgeries of the lower extremities [29]) should also be taken into account before age criteria for SDR are changed. Like Golan et al. [12], we also found a higher incidence of lordosis in females, although this was not statistically significant.
Spondylolysis and spondylisthesis
Frederickson et al. [11] reported spondylolysis in 4% of the children in a normal population, which increased to 6% in adulthood, and 74% of these patients also showed spondylolisthesis. These results were however based on X-rays taken in a supine position which underestimates the true incidence [11]. Oblique and lateral standing radiographs are necessary to detect the true incidence [20]. Harada et al. [13] reported (using standing X-rays and oblique views) spondylolysis at level L5 in 21% of a cohort of patients with spastic diplegia, in which two thirds were older than 20 years. They also found spondylolisthesis in 4% compared to 6% in the healthy control group. The short-term SDR follow-up studies, where no oblique views were used, reported (mainly at level L5) spondylolysis in 12% [12] and spondylolisthesis in 2–24% [12, 17, 42, 47]. In our post-SDR follow-up studies, we always included standing X-rays with oblique views and the first study showed spondylolysis in 9% and spondylolisthesis in 4% [35], while at follow-up these were 13% and 6%, respectively [34].
The patients who were eligible for our current follow-up study progressed from 18% in the short term to 37% in the long term. Spondylolisthesis grade I was diagnosed in the same patient as in the short- and long-term follow-up study with no progression. Spondylolysis was more common in this long-term study than in the other short-term studies. We found these abnormalities at different levels between L2 and S1, while other short-term follow-up studies reported abnormalities mainly at L5–S1. When compared with X-ray results of spastic diplegia patients who did not undergo SDR (using similar radiographic methods) [13], spondylolysis was slightly more common in our study, but the patients may not be exactly comparable, despite the fact that four patients showed spontaneous healing of the defect in the pars interarticularis, as also reported by other research groups [49].
The development of spondylolysis is in most cases a result of a fatigue fracture of the pars. Patients who are not ambulant have a much lower chance of developing spondylolysis and spondylolisthesis than the more functionally mobile patients. This is supported by the results of Rosenberg et al. [38], who reported that none of their non-ambulant patients developed spondylolysis or spondylolisthesis. In line with this, spondylolysis was less common in our study in patients who were classified as GFMCS level III. In addition, we found that patients with mild involvement of an upper limb had a significantly higher incidence of spondylolysis than the patients with no upper limb involvement, which might be related to more asymmetrical strain experienced by the lumbar spine. With regard to the MRI outcomes, spondylosis was more common in patients who had spinal stenosis (not significant), compared to those without this spinal abnormality. In addition, a statistically significant association was found for the total number of MRI abnormalities and spondylolysis.
MRI scan outcomes
Degenerative changes of the spine in adults with CP have been described in the literature [13, 38], although there is an incomplete overview of the incidence of spinal abnormalities other than the bony spinal deformities.
Disc degeneration is a result of progressive structural failure, which is often the result of aging or excessive loading of the spine [1]. Asymmetrical and increased strain and excessive mobility are all described in the pathogenesis of spinal stenosis and most of our cases with spinal stenosis appear to have been caused by facet hypertrophy. In addition, we found that spinal stenosis was most common at level L4–5 but sometimes occurred at multiple levels, which is in accordance with what is described in the literature [26].
Clinical assessments
Different short-term [9, 43] and long-term [18] follow-up studies provided convincing evidence that muscle tone is significantly decreased and that muscle strength might deteriorate, remain unchanged, or improve as a result of SDR. Persistent sensory loss has been reported in 23% of children with CP [23] and in 4–20% in short-term SDR follow-up studies [33, 45]. In addition, significant decreased or absent deep tendon reflexes have been reported in most patients in short-term follow-up studies [28]. The outcomes of muscle tone, strength, sensation, and reflexes of our current long-term study were similar.
Pain questionnaires
Low back pain and pain in the lower extremities were the most commonly reported sites for pain in adults with CP [3, 6, 14, 16, 30, 41, 48]. In a mixed study, cohorts of patients with CP aged from 18 to 70+ years, back pain was reported in 54–67% of the cases [6, 16, 30, 41]. Some studies found that this pain had no or minor impact on patients’ daily functioning [6, 14, 41], while another study showed that this had a moderate to extreme impact on one third of their patients’ activities [16]. These outcomes are similar to our results of 67% of our adults who reported back pain (17% on a daily basis) and 23% of them who were ‘moderately’ disabled because of back or leg pain more than 15 years after SDR.
In addition to these more descriptive articles, back pain has also been discussed in radiographic spinal deformity studies. Short-term SDR follow-up studies in children found back pain in 0–29% of the patients [17, 42, 45, 47] with 24% occurring with lordosis [17] and 38–50% with spondylolisthesis [42]. In a population of patients with spastic diplegia aged 20–30+ years who did not undergo SDR, back pain was reported in 53–64% of the cohort [13], and 55% of their patients with spondylolysis complained about back pain, while 75% with lordosis curves >70° and 39% with curves <50°. Our adults with spastic diplegia who did receive SDR had a higher frequency of back pain, but this was similar to adults who have not had SDR.
Methodological limitations
There are several potential limitations to our study. First, the sample size was relatively small, especially in the subgroup analysis; therefore, some statistically significant associations may not have been observed and these results should be regarded as preliminary. However, these are the only data on long-term spinal deformities after SDR. Second, there is limited data on long-term spinal deformity of patients with CP who did not receive SDR. We could not adequately compare our results with the natural history of the condition, and so cannot distinguish an independent effect of SDR. Third, the outcomes of the short-term follow-up were based on historical radiographic reports of analog X-rays, while the long-term outcomes were evaluated from digital X-rays. Although there was a difference in type of X-rays, we still believe that these results are reliable and the evaluations of both studies were completed by the same experienced neurosurgeon (JCP) and orthopedic surgeon (EBH). Fourth, even though the follow-up period in the study is long, our patients were still relatively young (age range 21–44 years) and follow-up to later ages is still necessary.
Conclusions
Seventeen to 26 years after SDR, spinal deformities, except for spondylolisthesis, did appear to be more common. However, this increase was not marked. In fact, the only statistically significant increase was for relatively mild scoliosis. The majority had curves of less than 30° and only two patients had curves of 35°. No patient to date has required any spinal operations after their SDR. It is known that spinal deformities also increase as part of the natural history of CP, so there is a need for further studies to ascertain if the rate of development of spinal deformities after SDR is any different from that of the natural history of the condition.
References
Adams MA, Roughley PJ (2006) What is intervertebral disc degeneration, and what causes it? Spine 31:2151–2161
Aiona MD, Sussman MD (2004) Treatment of spastic diplegia in patients with cerebral palsy: part II. J Pediatr Orthop B 13:S13–S38
Andersson C, Mattsson E (2001) Adults with cerebral palsy: a survey describing problems, needs, and resources, with special emphasis on locomotion. Dev Med Child Neurol 43:76–82
Ashworth B (1964) Prelimimary trial of carisopordol in multiple sclerosis. Practitioner 192:540–542
Cobb JR (1948) Outline for the study of scoliosis. AAOS Instr Course Lect 5:261
Engel JM, Jensen MP, Hoffman AJ, Kartin D (2003) Pain in persons with cerebral palsy: extension and cross validation. Arch Phys Med Rehabil 84:1125–1128
Fairbank JC, Couper J, Davies JB, O'Brien JP (1980) The Oswestry low back pain disability questionnaire. Physiotherapy 66:271–273
Fairbank JC, Pynsent PB (2000) The Oswestry Disability Index. Spine 25:2940–2952
Farmer JP, Sabbagh AJ (2007) Selective dorsal rhizotomies in the treatment of spasticity related to cerebral palsy. Childs Nerv Syst 23:991–1002
Foerster O (1913) On the indications and results of the excision of posterior nerve roots in men. Surg Gynecol Obstet 6:463–474
Fredrickson BE, Baker D, Mcholick WJ, Yuan HA, Lubicky JP (1984) The natural history of spondylolysis and spondylolisthesis. J Bone Joint Surg Am 66A:699–707
Golan JD, Hall JA, O'Gorman G, Poulin C, Benaroch TE, Cantin MA, Farmer JP (2007) Spinal deformities following selective dorsal rhizotomy. J Neurosurg 106:441–449
Harada T, Ebara S, Anwar MM, Kajiura I, Oshita S, Hiroshima K, Ono K (1993) The lumbar spine in spastic diplegia—a radiographic study. J Bone Joint Surg Br 75:534–537
Hilberink SR, Roebroeck ME, Nieuwstraten W, Jalink L, Verheijden JM, Stam HJ (2007) Health issues in young adults with cerebral palsy: towards a life-span perspective. J Rehabil Med 39:605–611
Jahnsen R, Aamodt G, Rosenbaum P (2006) Gross Motor Function Classification System used in adults with cerebral palsy: agreement of self-reported versus professional rating. Dev Med Child Neurol 48:734–738
Jahnsen R, Villien L, Aamodt G, Stanghelle JK, Holm I (2004) Musculoskeletal pain in adults with cerebral palsy compared with the general population. J Rehabil Med 36:78–84
Johnson MB, Goldstein L, Thomas SS, Piatt J, Aiona M, Sussman M (2004) Spinal deformity after selective dorsal rhizotomy in ambulatory patients with cerebral palsy. J Pediatr Orthop 24:529–536
Langerak NG, Lamberts RP, Fieggen AG, Peter JC, Peacock WJ, Vaughan CL (2009) Functional status of patients with cerebral palsy according to the International Classification of Functioning, Disability and Health model: a 20-year follow-up study after selective dorsal rhizotomy. Arch Phys Med Rehabil 90:994–1003
Langerak NG, Lamberts RP, Fieggen AG, Peter JC, Van Der Merwe L, Peacock WJ, Vaughan CL (2008) A prospective gait analysis study in patients with diplegic cerebral palsy 20 years after selective dorsal rhizotomy. J Neurosurg Pediatr 1:180–186
Lowe RW, Hayes TD, Kaye J, Bagg RJ, Luekens CA (1976) Standing roentgenograms in spondylolisthesis. Clin Orthop Relat Res 117:80–84
Madigan RR, Wallace SL (1981) Scoliosis in the institutionalized cerebral palsy population. Spine 6:583–590
Majd ME, Muldowny DS, Holt RT (1997) Natural history of scoliosis in the institutionalized adult cerebral palsy population. Spine 22:1461–1466
McLaughlin JF, Felix SD, Nowbar S, Ferrel A, Bjornson K, Hays RM (2005) Lower extremity sensory function in children with cerebral palsy. Pediatr Rehabil 8:45–52
Medical Research Council (1943) Aids to the investigation of the peripheral nervous injuries. Her Majesty's Stationery Office, London
Meyerding H (1932) Spondylolisthesis. Surg Gynecol Obstet 54:371–377
Modic MT (1994) Degenerative disorders of the spine. In: Modic MT, Masaryk TJ, Ross JS (eds) Magnetic resonance imaging of the spine, 2nd edn. Mosby, St Louis, pp 80–150
Morrell DS, Pearson JM, Sauser DD (2002) Progressive bone and joint abnormalities of the spine and lower extremities in cerebral palsy. Radiographics 22:257–268
Nordmark E, Josenby AL, Lagergren J, Andersson G, Stromblad LG, Westbom L (2008) Long-term outcomes five years after selective dorsal rhizotomy. BMC Pediatr 14(8):54
O'Brien DF, Park TS (2006) A review of orthopedic surgeries after selective dorsal rhizotomy. Neurosurg Focus 21:e2
Opheim A, Jahnsen R, Olsson E, Stanghelle JK (2009) Walking function, pain, and fatigue in adults with cerebral palsy: a 7-year follow-up study. Dev Med Child Neurol 51:381–388
Palisano R, Rosenbaum P, Walter S, Russell D, Wood E, Galuppi B (1997) Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol 39:214–223
Peacock WJ, Eastman RW (1981) The neurosurgical management of spasticity. S Afr Med J 60:849–850
Peter JC, Arens LJ (1993) Selective posterior lumbosacral rhizotomy for the management of cerebral palsy spasticity—a 10-year experience. S Afr Med J 83:745–747
Peter JC, Hoffman EB, Arens LJ (1993) Spondylolysis and spondylolisthesis after five-level lumbosacral laminectomy for selective posterior rhizotomy in cerebral-palsy. Childs Nerv Syst 9:285–287
Peter JC, Hoffman EB, Arens LJ, Peacock WJ (1990) Incidence of spinal deformity in children after multiple level laminectomy for selective posterior rhizotomy. Childs Nerv Syst 6:30–32
Propst-Proctor SL, Bleck EE (1983) Radiographic determination of lordosis and kyphosis in normal and scoliotic children. J Pediatr Orthop 3:344–346
Robson P (1968) Prevalence of scoliosis in adolescents and young adults with cerebral palsy. Dev Med Child Neurol 10:447–452
Rosenberg NJ, Bargar WL, Friedman B (1981) The incidence of spondylolysis and spondylolisthesis in non-ambulatory patients. Spine 6:35–38
Rosenthal RK, Levine DB, McCarver CL (1974) Occurrence of scoliosis in cerebral palsy. Dev Med Child Neurol 16:664–667
Saito N, Ebara S, Ohotsuka K, Kumeta H, Takaoka K (1998) Natural history of scoliosis in spastic cerebral palsy. Lancet 351:1687–1692
Schwartz L, Engel JM, Jensen MP (1999) Pain in persons with cerebral palsy. Arch Phys Med Rehabil 80:1243–1246
Spiegel DA, Loder RT, Alley KA, Rowley S, Gutknecht S, Smith-Wright DL, Dunn ME (2004) Spinal deformity following selective dorsal rhizotomy. J Pediatr Orthop 24:30–36
Steinbok P (2007) Selective dorsal rhizotomy for spastic cerebral palsy: a review. Childs Nerv Syst 23:981–990
Steinbok P, Hicdonmez T, Sawatzky B, Beauchamp R, Wickenheiser D (2005) Spinal deformities after selective dorsal rhizotomy for spastic cerebral palsy. J Neurosurg 102:363–373
Steinbok P, Schrag C (1998) Complications after selective posterior rhizotomy for spasticity in children with cerebral palsy. Pediatr Neurosurg 28:300–313
Thometz JG, Simon SR (1988) Progression of scoliosis after skeletal maturity in institutionalized adults who have cerebral palsy. J Bone Joint Surg Am 70A:1290–1296
Turi M, Kalen V (2000) The risk of spinal deformity after selective dorsal rhizotomy. J Pediatr Orthop 20:104–107
Turk MA, Geremski CA, Rosenbaum PF, Weber RJ (1997) The health status of women with cerebral palsy. Arch Phys Med Rehabil 78:S10–S17
Wiltse LL, Widell EH, Jackson DW (1975) Fatigue fracture—basic lesion in isthmic spondylolisthesis. J Bone Joint Surg Am A 57:17–22
World Health Organisation Expert Committee (1995) Physical status: the use and interpretation of anthropometry. WHO Technical Report Series 854, Geneva
Acknowledgments
We would like to thank Dr. Richard VP de Villiers and his supportive staff of the radiological practice of Dr. Van Wageningen and Partners, Stellenbosch Medi-Clinic, for the use of their facilities to capture the X-rays and MRI scans. In addition, we would like to thank Robert P. Lamberts for his assistance with transportation and taking care of the patients during data collection. This study was funded by the Medical Research Council of South Africa.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Langerak, N.G., Vaughan, C.L., Hoffman, E.B. et al. Incidence of spinal abnormalities in patients with spastic diplegia 17 to 26 years after selective dorsal rhizotomy. Childs Nerv Syst 25, 1593–1603 (2009). https://doi.org/10.1007/s00381-009-0993-5
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-009-0993-5