
Abstract
Background
Total thyroidectomy is a well-established surgical approach for the management of papillary thyroid cancer (PTC). However, the best surgical approach for papillary microcarcinoma is nowadays still debated. Both total thyroidectomy and simple lobectomy are used. We report the experience of a single University center in the treatment of thyroid microcarcinoma.
Methods
A retrospective analysis on all patients who underwent thyroid surgery at our institution over a 24-year period (1991–2015) was performed. Patients were grouped according to whether they received total thyroidectomy (Group 1) or lobectomy (Group 2). Follow-up was made by routine clinical and ultrasound examination. Specific outcomes such as recurrence and need for reoperation as well as complications (transient vocal cord paralysis and hypocalcemia) were analyzed.
Results
During the study period 880 patients underwent surgery for PTC. Group 1 and 2 consisted, respectively, of 756 and 124 patients. A micro PTC (<10 mm) was present in 251 and 69 specimen of Group 1 and 2. No evidence of disease recurrence in the follow-up was reported in patients with microPTC in Group 1 and in 57 patients of Group 2. In the remaining 12 patients completion thyroidectomy was carried out due to ultrasound findings of contralateral nodules (10), lymphadenopathy (1), and capsular invasion (1). Five of these patients had a contralateral papillary carcinoma on final histopathologic examination. Thus recurrence rate for patients of Group 2 was 7.3 %. Morbidity rates were, respectively, for Group 1 and 2: transient nerve palsy 81 and 5 (11 vs. 7.3 %, p = ns), transient hypoparathyroidism (Calcium <2.00 mmol/L) 137 (18.6 %) and 0 (p < 0.0001). Three of the 12 patients of Group 2 undergoing further surgery had a transient hypoparathyroidism.
Conclusions
Thyroid lobectomy is an effective surgical strategy to manage papillary microcarcinomas with low complications. Routine completion thyroidectomy is not mandatory. Appropriate selection excluding high-risk patients is of paramount importance in order to achieve the best results.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Thyroid cancer is the most common endocrine malignancy, with 62980 estimated new cases in the United States in 2014 [1–3]. Papillary thyroid carcinoma (PTC) accounts for about 80 to 90 % of all thyroid cancers [1–3]. The long-term prognosis is usually excellent with a 10-year survival rate of up to 98 % [3–5]. Recent studies demonstrated an increasing incidence of PTC and particularly, nowadays, cancer smaller than 1 cm (microPTC) are the most common type of thyroid carcinoma diagnosed in patients older than 45 years [1, 2, 6]. Guidelines published worldwide by different scientific associations differ in the management of PTC [7–10]. Western countries usually recommend total thyroidectomy plus post-operative radioactive iodine (RAI) ablation for PTC [7–9] as well as simple lobectomy, with or without ipsilateral central neck dissection, is the preferred management in Japan [10]. Regarding microPTC, the standardized surgical approach is still not established yet [4, 6, 10–21]. Particularly considering the indolent course of most of these microPTCs, the extent of surgery is debated regarding the need for oncological completeness and possible associated complications [4, 11–14, 16, 17, 20, 21]. The objective of our study is to evaluate the surgical management of microPTC in a single University Hospital comparing total thyroidectomy with simple lobectomy.
Materials and methods
A retrospective analysis of all patients who underwent surgery for thyroid papillary thyroid carcinoma in the Department of Endocrine Surgery of Poitiers University was performed. Data were prospectively collected in a database in the period between January 1991 and December 2014. All patients received full clinical and radiological (US for thyroid and regional neck lymph nodes study and FNAC) examination prior to surgery. Specific data parameters and outcomes were collected: age, sex, multifocality (defined as the presence of two or more foci of thyroid cancer within the same lobe), type of surgery, lesion size, surgical complications (nerve palsy, post-operative calcemia <2.00 mmol/L), need of further completion thyroidectomy. Patients were assigned to Group 1 (total thyroidectomy) or Group 2 (lobectomy) regarding the type of surgery. According to current practice subtotal thyroidectomy was performed until the year 2002. All patients who were managed by subtotal thyroidectomy were within Group 1. Only patients whose pathological reports were consistent with PTC or follicular variant (FVPTC) were included within the study, thus excluding Follicular, Hurthle cells, Medullary, and Anaplastic Carcinomas. Exclusion criteria to perform a lobectomy, as first surgical approach, were US lesion size >10 mm, intra-operative findings of macroscopic extra-thyroidal extension (ETE), multifocality on frozen section, lymph nodes involvement (pre-operatively or intra-operatively found), prior neck irradiation, and anamnesis of familial thyroid malignancies. ETE was defined as the invasion of peri-thyroid soft tissue, strap muscles, and adjacent structures. Completion thyroidectomy, according to our Department of Endocrinology, was selectively performed when final pathology found one or more of the following: multifocal disease with an overall sum of all lesions’ diameters >10 mm, actual size of PTC >10 mm, positive lymph nodes, microscopic or macroscopic extra-thyroid extension (ETE), aggressive features (tall cell, columnar cell or diffuse sclerosing variant), thus not filling the post-operative low-risk ATA’s classification for thyroid cancer [8]. The goal of this study was to analyze outcomes of microPTC so we only included in our review patients who underwent surgery for thyroid carcinoma ≤10 mm. RAI therapy according to guidelines [7, 8, 22], was not given to patients either after total thyroidectomy or lobectomy if final pathology did not show findings potentially increasing the risk of recurrence [8]. Recurrence was defined as the presence of thyroid carcinoma within the thyroid bed, regional lymph nodes, distant site or (for patients of Group 2) the contralateral lobe. This definition was used to follow patients considered to had a previous complete resection. Patients of Group 1 were followed by annual measurement serum thyroglobulin (Tg), Anti-thyroglobulin antibodies (Ab-Tg), and annual neck US exam, while patients of Group 2 had US evaluation twice a year for the first 2 years plus Tg, Ab-Tg measurement if under suppressive treatment with L-T4, then annually to evaluate the contralateral lobe. RAI therapy after simple lobectomy was not administered, but was performed after total thyroidectomy or completion thyroidectomy in case of multifocal disease, ETE or lymph nodes metastases. All data were included in a Specific Database accessible to all physicians involved. Patient’s specific data were then recalled and updated by simple query. Completion thyroidectomy in Group 2, in our current practice, is performed in case of development of nodules in the contralateral thyroid lobe during follow-up.
Statistical analysis
Descriptive statistics were tabulated for baseline demographics and clinical characteristics by extent of surgery. Variables were expressed as the mean. Results were compared using the Fisher exact test, as appropriate (GraphPad Software©). Values of p < 0.05 were considered statistically significant.
Results
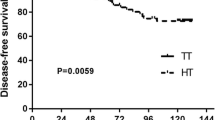
Between January 1991 and February 2015, 11207 patients underwent thyroid operations at our institution. Overall, 880 patients were operated on for a PTC (16.2 %), including follicular variant of PTC (FVPTC). Other histological types of thyroid cancers (Follicular, Hurthle, Medullary, Anaplastic) were not included. Total thyroidectomy (bilateral procedure, including total, near-total and subtotal) for PTC was performed in 756 patients (Group 1), while lobectomy (with or without isthmusectomy) was performed in 124 (Group 2) cases. MicroPTC (size lesion <10 mm) was present in 251/756 in Group 1 (33.2 %) and in 69/124 in Group 2 (55.7 %), p < 0.0001. Patient’s demographics were comparable between groups and are listed in Table 1. Comparing the population of patients who underwent surgery for microPTC, multifocality was slightly higher in Group 1 (13.9 vs. 7.3 %, p = 0.16), while mean size of the microPTC was 7.8 (range 2–10 mm) versus 7.1 mm (range 1–10 mm) in Group 1 and Group 2, respectively, (p = ns). In 54/251 patients of Group 1 (21.5 %) the initial procedure was simple lobectomy, followed during the same operation by completion thyroidectomy due to a positive frozen section for papillary carcinoma. Multifocality was present in 12/54 patients (22.2 %). Pathological lymph nodes (confirmed at frozen section, but not diagnosed at US pre-operative evaluation) were also found in 34/251 patients of Group 1 (13.5 %). All these patients had an ipsilateral central neck dissection at the time of surgery. Regarding the 54 patients supposed to only have lobectomy, also in 8 out of 54 patients (14.7 %) intra-operative positive lymph nodes were found. In Group 2 final pathology found 1 patient with positive lymph nodes that underwent completion thyroidectomy + unilateral central neck dissection. Complication rate was higher for both transient and permanent nerve palsy and hypoparathyroidism in Group 1(see Table 2), although only transient laryngeal nerve palsy (10.8 vs. 7.3 %, p = 0.02) and transient hypoparathyroidism (18.1 vs. 1.6 %, p < 0.0001) were statistically significative. Post-operative RAI was then performed in 74/251 patients (29.5 %) of Group 1 and in 7/69 patients (10.2 %) of Group 2 after completion thyroidectomy. Mean follow-up was 130.4 months (range 3–292) for Group 1 and 134.8 months for Group 2 (range 6–287), p = ns. No patients in Group 1 operated on for microPTC showed local (thyroid bed), regional lymph nodes or distant site recurrence, while 12/69 (17.4 %) of the patients who previously had lobectomy (Group 2) underwent completion procedure (p < 0.0001), with a mean delay from the first procedure of 43.5 months (range 5–105) (Fig. 1). A PTC was found in the contralateral lobe in 5 of these 12 patients (3 microPTC, 1 PTC >10 mm, 1 microPTC with capsular invasion), thus we may conclude a recurrence in 5 out 69 patients (7.3 %) compared to none in Group 1 (p = 0.0004). Three out of the 12 patients (25 %) who underwent a second operation had a transient hypocalcemia, none presented RLN palsy. Indications for reoperation are listed in Table 2.

Recurrence free survival comparing simple lobectomy to total thyroidectomy as first operation
Discussion
The optimal surgical treatment for PTC remains a subject of controversy [4, 5, 7–21].Total thyroidectomy is often advocated to be the better approach to minimize both recurrence and mortality [5]. Several reasons are given to support this approach: (I) allows complete removal of all the tumor, especially for multifocal/bilateral disease; (II) permits an accurate and comprehensive staging of the carcinoma; (III) RAI can be used to detect and treat thyroid remnants and/or local/regional recurrence and metastases (IV) the serum Tg levels is a sensitive marker of recurrence that can be used after total thyroidectomy only; (V) it improves both recurrence and survival rates; (VI) re-operative surgery carries a higher complication rate [5, 7–11]. On the other hand, some authors report no differences in term of survival for PTC managed with more aggressive approach than a lobectomy [3, 4, 12, 14, 20]. Reasons to limit the extent of surgery are (I) There is no randomized trial which demonstrates the benefit of one approach compared to the other in low-risk patients in terms of recurrence/survival in appropriate groups of patients; (II) surgical complications are lower; (III) patients with low-risk PTC are often overtreated with RAI, with no benefits but actually even increasing the risk of developing a second malignancy [4, 12–14, 16, 20–24]. Currently for PTC >10 mm, both American and European Society recommend total thyroidectomy, while Japanese guidelines still advise simple lobectomy, with RAI reserved for intermediate and high-risk patients to avoid unnecessary exposure for the patients [7–10, 22–24]. In our Department, we currently use this approach for PTC >10 mm, considering that only in this cluster of patients recurrence after total thyroidectomy was reported (67/505, 13,3 % at 10 years, undisclosed data). Focusing our attention on microPTC, the indolent course of this neoplasia actually needs to address the question of the optimal surgical treatment. It reported firstly the “harmless” nature of microPTC observing for a mean time of 74 months 340 patients with no surgery performed, demonstrating the minimal clinical significance of such carcinomas [21, 25, 26]. More reports in literature confirm these findings. Hughes et al. reported an increasing incidence of small thyroid PTC diagnosed as incidental findings due to better imaging rather than improved clinical skills, with no impact on recurrence/survival [6]. Hay investigated 900 patients followed by the Mayo Clinic in a mean period of 17.2 years [27]. In 892 patients whom underwent total thyroidectomy as the first approach, no metastases developed in a period of 20 years [27]. The low aggressiveness of microPTC is also confirmed by the report of Baudin which found a recurrence rate of 3.9 % in 281 microPTC within a follow-up of 7.3 years [28]. These findings of an innocent behavior are corroborated by the meta-analysis of Roti et al. [29]. The latter reviewed 17 series of microPTC reporting, overall, an incidence of 35 distant metastases out of 9.313 patients (0.37 %) and a cancer-related death of 0.34 % (32 patients) [29]. All these publications substantiate the hypothesis that microPTC does not necessitate an aggressive surgical management, as we reported no recurrence in Group 1 after a mean followup of 10.9 years and only 5 patients in Group 2 (mean follow-up of 11.2 years) who developed a PTC within the contralateral lobe (7.3 %). We did not experience any death related to microPTC. We would like to emphasize that although both groups presented excellent results in term of disease-free and disease-specific survival, the complication rate was, as expected, higher for those who underwent total thyroidectomy, especially for transient hypoparathyroidism (p < 0.0001). These results highlight that patients with microPTC represent a very low-risk cluster and benefit from a less aggressive management, to avoid unnecessary morbidity [4, 20, 21, 30]. Our study has some limitations, as it is a review of collected data and some of them may suffer from collection and or recall biases. Nevertheless, it confirms findings from other large series which agree on a less aggressive treatment for microPTC. We would like to borrow the expression “less is better” by the study of Schlumberger et al. [23]. In fact as RAI therapy in low-risk PTC does not add any benefit, but on the contrary, may cause further disease [23, 24]. Our belief is that when facing patients with microPTC filling the criteria we selected, the best approach is the simple lobectomy and follow-up. It maximizes the results while minimizing the impact on the patient’s quality of life. The key to achieve excellent results in patients with PTC is then careful selection. This is also supported by a recent meta-analysis by Macedo [31], who found a higher recurrence rate for those microPTC which showed multifocality, aggressive histologic features, local node metastases and extra-thyroidal involvement. Comparing our patients with multifocal disease to those of the meta-analysis actually the recurrence rate was similar (7.3 vs. 7.9 %), confirming the needs of strict criteria to achieve the best result. In conclusion, the optimal surgical management for microPTC has to be tailored, evaluating the actual risk to each patient to maximize the benefits of surgery.
References
American Cancer Society. Cancer Facts, Figures. 2014. Available at:http://www.cancer.org/acs/groups/content/@research/documents/webcontent/acspc-042151.pdf
Davies L, Welch HG (2006) Increasing incidence of thyroid cancer in the United States, 1973–2002. JAMA 295(18):2164–2167
Abdelgadir Adam M, Pura J, Goffredo P, Dinan MA, Hyslop T, Reed SD, Scheri RP, Roman SA, Sosa JA (2015) Impact of extent of surgery on survival for papillary thyroid cancer patients younger than 45 years. J Clin Endocrinol Metab 100(1):115–121. doi:10.1210/jc.2014-3039
Matsuzu K, Sugino K, Masudo K, Nagahama M, Kitagawa W, Shibuya H, Ohkuwa K, Uruno T, Suzuki A, Magoshi S, Akaishi J, Masaki C, Kawano M, Suganuma N, Rino Y, Masuda M, Kameyama K, Takami H, Ito K (2014) Thyroid lobectomy for papillary thyroid cancer: long-term follow-up study of 1088 cases. World J Surg 38(1):68–79. doi:10.1007/s00268-013-2224-1
Bilimoria KY, Bentrem DJ, Ko CY, Stewart AK, Winchester DP, Talamonti MS, Sturgeon C (2007) Extent of surgery affects survival for papillary thyroid cancer. Ann Surg 246(3):375–381 discussion 381–384
Hughes DT, Haymart MR, Miller BS, Gauger PG, Doherty GM (2011) The most commonly occurring papillary thyroid cancer in the United States is now a microcarcinoma in a patient older than 45 years. Thyroid 21(3):231–236. doi:10.1089/thy.2010.0137
Pacini F, Schlumberger M, Dralle H, Elisei R, Smit JW, Wiersinga W (2006) European Thyroid Cancer Taskforce. European consensus for the management of patients with differentiated thyroid carcinoma of the follicular epithelium. Eur J Endocrinol 154(6):787–803. No abstract available. Erratum in: Eur J Endocrinol. 2006 155(2):385
American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer, Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, Mazzaferri EL, McIver B, Pacini F, Schlumberger M, Sherman SI, Steward DL, Tuttle RM (2009) Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009 19(11):1167–1214. doi: 10.1089/thy.2009.0110. Erratum in: Thyroid. 2010 20(8):942. Hauger, Bryan R [corrected to Haugen, Bryan R]. Thyroid. 2010 20(6):674–675
Perros P, Boelaert K, Colley S, Evans C, Evans RM, Gerrard Ba G, Gilbert J, Harrison B, Johnson SJ, Giles TE, Moss L, Lewington V, Newbold K, Taylor J, Thakker RV, Watkinson J, Williams GR (2014) British Thyroid Association. Guidelines for the management of thyroid cancer. Clin Endocrinol (Oxf). 81(Suppl 1):1–122. doi: 10.1111/cen.12515 (No abstract available)
Takami H, Ito Y, Okamoto T, Onoda N, Noguchi H, Yoshida A (2014) Revisiting the guidelines issued by the Japanese Society of Thyroid Surgeons and Japan Association of Endocrine Surgeons: a gradual move towards consensus between Japanese and western practice in the management of thyroid carcinoma. World J Surg 38(8):2002–2010. doi:10.1007/s00268-014-2498-y
Kebebew E, Clark OH (2000) Differentiated thyroid cancer: “complete” rational approach. World J Surg 24(8):942–951. doi:10.1007/s002680010165 Review
Mendelsohn AH, Elashoff DA, Abemayor E (2010) St John MA. Surgery for papillary thyroid carcinoma: is lobectomy enough? Arch Otolaryngol Head Neck Surg 136(11):1055–1061. doi:10.1001/archoto.2010.181
Rosato L, Avenia N, Bernante P, De Palma M, Gulino G, Nasi PG, Pelizzo MR, Pezzullo L (2004) Complications of thyroid surgery: analysis of a multicentric study on 14,934 patients operated on in Italy over 5 years. World J Surg 28(3):271–276. doi:10.1007/s00268-003-6903-1
Adam MA, Pura J, Gu L, Dinan MA, Tyler DS, Reed SD, Scheri R, Roman SA, Sosa JA (2014) Extent of surgery for papillary thyroid cancer is not associated with survival: an analysis of 61,775 patients. Ann Surg 260(4):601–605. doi:10.1097/SLA.0000000000000925 (discussion 605–607)
Verburg FA, Mäder U, Tanase K, Thies ED, Diessl S, Buck AK, Luster M, Reiners C (2013) Life expectancy is reduced in differentiated thyroid cancer patients ≥45 years old with extensive local tumor invasion, lateral lymph node, or distant metastases at diagnosis and normal in all other DTC patients. J Clin Endocrinol Metab 98(1):172–180. doi:10.1210/jc.2012-2458
Hay ID, Thompson GB, Grant CS, Bergstralh EJ, Dvorak CE, Gorman CA, Maurer MS, McIver B, Mullan BP, Oberg AL, Powell CC, van Heerden JA, Goellner JR (2002) Papillary thyroid carcinoma managed at the Mayo Clinic during six decades (1940–1999): temporal trends in initial therapy and long-term outcome in 2444 consecutively treated patients. World J Surg 26(8):879–885. doi:10.1007/s00268-002-6612-1
Udelsman R, Shaha A (2005) Is total thyroidectomy the best possible surgical management for well-differentiated thyroid carcinoma? Lancet Oncol 6:529–531
Wanebo H, Coburn M, Teates D, Cole B (1998) Total thyroidectomy does not enhance disease control or survival even in high-risk patients with differentiated thyroid cancer. Ann Surg 227(6):912–921
Haigh PI, Urbach DR, Rotstein LE (2005) Extent of thyroidectomy is not a major determinant of survival in low- or high-risk papillary thyroid cancer. Ann Surg Oncol 12(1):81–89
Nixon IJ, Ganly I, Patel SG, Palmer FL, Whitcher MM, Tuttle RM, Shaha A, Shah JP (2012) Thyroid lobectomy for treatment of well differentiated intrathyroid malignancy. Surgery. 151(4):571–579. doi:10.1016/j.surg.2011.08.016
Grant CS (2015) Recurrence of papillary thyroid cancer after optimized surgery. Gland Surg 4(1):52–62. doi:10.3978/j.issn.2227-684X.2014.12.06 Review
Pacini F, Schlumberger M, Harmer C, Berg GG, Cohen O, Duntas L, Jamar F, Jarzab B, Limbert E, Lind P, Reiners C (2005) Sanchez Franco F, Smit J, Wiersinga W. Post-surgical use of radioiodine (131I) in patients with papillary and follicular thyroid cancer and the issue of remnant ablation: a consensus report. Eur J Endocrinol 153(5):651–659 Review
Schlumberger M, Catargi B, Borget I, Deandreis D, Zerdoud S, Bridji B, Bardet S, Leenhardt L, Bastie D, Schvartz C, Vera P, Morel O, Benisvy D, Bournaud C, Bonichon F, Dejax C, Toubert ME, Leboulleux S, Ricard M, Benhamou E (2012) Tumeurs de la Thyroïde Refractaires Network for the Essai Stimulation Ablation Equivalence Trial. Strategies of radioiodine ablation in patients with low-risk thyroid cancer. N Engl J Med 366(18):1663–1673. doi:10.1056/NEJMoa1108586
Iyer NG, Morris LG, Tuttle RM, Shaha AR, Ganly I (2011) Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy. Cancer 117(19):4439–4446. doi:10.1002/cncr.26070
Ito Y, Uruno T, Nakano K, Takamura Y, Miya A, Kobayashi K, Yokozawa T, Matsuzuka F, Kuma S, Kuma K, Miyauchi A (2003) An observation trial without surgical treatment in patients with papillary microcarcinoma of the thyroid. Thyroid. 13(4):381–387
Ito Y, Miyauchi A, Inoue H, Fukushima M, Kihara M, Higashiyama T, Tomoda C, Takamura Y, Kobayashi K, Miya A (2010) An observational trial for papillary thyroid microcarcinoma in Japanese patients. World J Surg 34(1):28–35. doi:10.1007/s00268-009-0303-0
Hay ID, Hutchinson ME, Gonzalez-Losada T, McIver B, Reinalda ME, Grant CS, Thompson GB, Sebo TJ, Goellner JR (2008) Papillary thyroid microcarcinoma: a study of 900 cases observed in a 60-year period. Surgery 144(6):980–987. doi:10.1016/j.surg.2008.08.035 discussion 987–988
Baudin E, Travagli JP, Ropers J, Mancusi F, Bruno-Bossio G, Caillou B, Cailleux AF, Lumbroso JD, Parmentier C, Schlumberger M (1998) Microcarcinoma of the thyroid gland: the Gustave–Roussy Institute experience. Cancer 83(3):553–559
Roti E, DegliUberti EC, Bondanelli M, Braverman LE (2008) Thyroid papillary microcarcinoma: a descriptive and meta-analysis study. Eur J Endocrinol 159(6):659–673. doi:10.1530/EJE-07-0896 Review
Hauch A, Al-Qurayshi Z, Randolph G, Kandil E (2014) Total thyroidectomy is associated with increased risk of complications for low- and high-volume surgeons. Ann Surg Oncol 21(12):3844–3852. doi:10.1245/s10434-014-3846-8
Macedo FI, Mittal VK (2015) Total thyroidectomy versus lobectomy as initial operation for small unilateral papillary thyroid carcinoma: a meta-analysis. Surg Oncol. doi:10.1016/j.suronc.2015.04.005
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
The authors have nothing to disclose.
Additional information
Paper Accepted at the IAES 2015 meeting in Bangkok, 23rd–27th August 2015.
Rights and permissions
About this article

Cite this article
Donatini, G., Castagnet, M., Desurmont, T. et al. Partial Thyroidectomy for Papillary Thyroid Microcarcinoma: Is Completion Total Thyroidectomy Indicated?. World J Surg 40, 510–515 (2016). https://doi.org/10.1007/s00268-015-3327-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-015-3327-7