
Abstract
Purpose
Diagnosis of spondylodiscitis (SD) may be challenging due to the nonspecific clinical and laboratory findings and the need to perform various diagnostic tests including serologic, imaging, and microbiological examinations. Homogeneous management of SD diagnosis through international, multidisciplinary guidance would improve the sensitivity of diagnosis and lead to better patient outcome.
Methods
An expert specialist team, comprising nuclear medicine physicians appointed by the European Association of Nuclear Medicine (EANM), neuroradiologists appointed by the European Society of Neuroradiology (ESNR), and infectious diseases specialists appointed by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID), reviewed the literature from January 2006 to December 2015 and proposed 20 consensus statements in answer to clinical questions regarding SD diagnosis. The statements were graded by level of evidence level according to the 2011 Oxford Centre for Evidence-based Medicine criteria and included in this consensus document for the diagnosis of SD in adults. The consensus statements are the result of literature review according to PICO (P:population/patients, I:intervention/indicator, C:comparator/control, O:outcome) criteria.
Evidence-based recommendations on the management of adult patients with SD, with particular attention to radiologic and nuclear medicine diagnosis, were proposed after a systematic review of the literature in the areas of nuclear medicine, radiology, infectious diseases, and microbiology.
Results
A diagnostic flow chart was developed based on the 20 consensus statements, scored by level of evidence according to the Oxford Centre for Evidence-based Medicine criteria.
Conclusions
This consensus document was developed with a final diagnostic flow chart for SD diagnosis as an aid for professionals in many fields, especially nuclear medicine physicians, radiologists, and orthopaedic and infectious diseases specialists.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Spinal infections include vertebral osteomyelitis (infection of the vertebral body), discitis (infection of the intervertebral disc), and spondylodiscitis (SD) (infection of two adjacent vertebral bodies and their intervertebral disc) [1, 2].
Our article will focus specifically on SD in adult patients.
The incidence of SD in developed countries ranges from 4 to 24 per million per year [3], and has been increasing in recent decades as a result of several factors, including an increase in the susceptible population (i.e. aged persons, patients with immunosuppression, diabetes mellitus, chronic renal or liver diseases, long-term steroid use); a rise in the number of invasive procedures, especially spinal surgery and improvements in diagnostic sensitivity [3].
It occurs at any age but is most frequent in the fifth to seventh decades. Men are affected more frequently than women [4,5,6].
In adults, spinal infections are initially localised in the anterior part of the vertebral body, which presents more vascular structures [2, 7, 8], thus extending into the adjacent tissues (intervertebral disc and adjacent vertebrae). The exact anatomical location of the infective process enables the classification of SD in anterior, posterior, spinal canal, or bone graft sites [1].
The most frequent site of vertebral infection is the lumbar spine (45%), followed by the dorsal spine (35%) and the cervical tract (20%) [2,3,4,5,6,7,8,9].
SD can be described aetiologically as pyogenic, granulomatous (tuberculous, brucellar, fungal), or parasitic [10], and clinically as primary or secondary.
In primary SD, pathogens can infect the spine by haematogenous spread or by spread from contiguous tissues. Staphylococcus aureus is the most frequently isolated pathogen (55–80% of cases) [4,5,6, 8,9,10,11,12,13,14,15,16,17]. Around 7–33% of pyogenic SD are caused by Enterobacteriaceae, mostly Escherichia coli, followed by Proteus and Klebsiella species [5, 18,19,20,21,22,23]. Coagulase-negative staphylococci (CoNS) account for 5–16% of cases [17, 19,20,21,22]. Brucellosis, a common zoonosis in endemic areas (Mediterranean Basin, Latin America, the Middle East, parts of Africa, and Western Asia) can account for 21–48% of spinal infections [19, 21]. Tuberculosis (TB) is among the commonest aetiological agents of spinal infection worldwide, and is responsible for 9–46% of SD in developed countries [19, 21, 23].
Secondary SD occurs due to direct contamination by microorganisms in surgical or interventional procedures [7,8,9, 24, 25]. The incidence of secondary SD varies according to the type of surgical procedure, ranging from 1 to 7% [8, 26,27,28,29,30,31].
Postoperative infections are caused mainly by S. aureus, isolated in almost 50% of cases, and CoNS [32,33,34]. Gram-negative bacteria may also cause post-surgical SD, with E. coli, Pseudomonas aeruginosa, Klebsiella pneumoniae, Enterobacter cloacae, Bacteroides, and Proteus species [32,33,34] representing the most frequently isolated Gram-negative bacteria.
The diagnosis of SD may be challenging due to the unspecific clinical features and laboratory findings and the need to perform different diagnostic tests including serologic, imaging, and microbiological examinations.
The clinical features include severe spine pain with or without fever. Neurological deficit, including leg weakness, paralysis, sensory deficit, radiculopathy, and loss of sphincter control, are present in one-third of cases [35].
Laboratory findings, although not specific, include elevated levels of C-reactive protein (CRP) and increased erythrocyte sedimentation rate (ESR) [35].
Differential diagnosis of SD includes other spine pathologies such as erosive osteochondrosis, osteoporotic and pathological fracture, spine metastasis, ankylosing spondyloarthritis, Scheuermann’s disease, and post-surgical changes.
Long courses of antibiotic therapy are usually necessary, and if the disease is not adequately controlled, a surgical approach is often required [36].
Aim of this consensus document
Diagnosis of SD is based on clinical, laboratory, and imaging findings. In recent decades, the sensitivity of SD diagnosis has been significantly improved; however, it is still difficult and is often delayed or missed.
Early diagnosis of SD, with the identification of the aetiology and description of the location, extent, and severity of the infectious process, as well as the presence of complications, is fundamental to supporting appropriate therapeutic management.
Although guidelines for the diagnosis of SD have been published previously, the diagnostic imaging of spine infection is still an issue. The Infectious Diseases Society of America (IDSA) guidelines, published in 2015, only provide guidance for diagnosis and treatment of native vertebral osteomyelitis (NVO), without addressing secondary SD [36]. Moreover, limited consideration is given to radiologic and nuclear medicine techniques for the assessment of spine infection.
Qualified members of the European Association of Nuclear Medicine (EANM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID), and European Society of Neuroradiology (ESNR) previously utilised a multidisciplinary approach to design a diagnostic flow chart for the management of SD [37].
Importantly, the implementation of radiologic and nuclear medicine techniques for the assessment of spine infection still varies widely, with heterogeneity in technical aspects that persists across countries in Europe with different levels of experience and preferences. The recognition of this problem led to the awareness among members of EANM, ESCMID, and ESNR that practical guidance is needed to establish standards for imaging in SD using MRI, 99mTc-methylene diphosphonate (MDP) or 99mTc-hydroxy diphosphonate (HDP) bone scan, 67Ga scintigraphy, and [18F]FDG positron emission tomography (PET)/computed tomography (CT).
Management of SD diagnosis through international multidisciplinary consensus would improve diagnostic accuracy and thus lead to better outcomes for patients with SD.
After a systematic review of the literature in the areas of nuclear medicine, radiology, infectious diseases, and microbiology, evidence-based recommendations have been proposed for the management of adult patients with SD, with particular attention to radiologic and nuclear medicine diagnosis. This consensus document was developed as an aid for professionals in many fields, especially nuclear medicine physicians, radiologists, and orthopaedic and infectious diseases specialists.
Methodology
A guideline expert panel was established, with different experts assigned a topic for review and presentation to the entire group. The panel comprised infectious disease specialists (ESCMID members), nuclear medicine physicians (EANM members), and neuroradiologists (ESNR members). EANM participants were selected by the EANM Committee on Inflammation and Infection on the basis of their publication record and a personal statement. ESCMID and ESNR participants were selected by the governing boards of the respective societies.
The panel identified 20 clinical questions to address. Panel members thoroughly reviewed the literature pertinent to each of the questions according to PICO (P: population/patients, I: intervention/indicator, C: comparator/control, O: outcome) criteria [38]. Articles presenting data pertaining to the diagnosis of SD were identified through computerised literature searches using MEDLINE (National Library of Medicine, Bethesda, MD), EMBASE, and the Cochrane database and by reviewing the references of retrieved articles. For development of the background section, we also reviewed articles describing the epidemiology of SD. Index search terms were selected according to the Oxford Centre for Evidence-based Medicine, as reported in Appendix 1.
The search was restricted to full articles published in English from January 2006 to December 2015 and including adult patients (>16 years of age). No attempt was made to obtain information on unpublished studies. Since data from randomised clinical trials were expected to be limited, we also reviewed non-randomised controlled clinical trials and cohort and case–control studies. Single case reports and reviews were excluded, as well as studies including fewer than 10 patients. After the literature review, the panel members elaborated the statements to be included and graded the level of evidence according to the 2011 Oxford Centre for Evidence-based Medicine criteria [38]. Statements were circulated first among each working group and then among all participants.
All working groups met several times between 2014 and 2016 in order to reach a consensus on the final version of each statement.
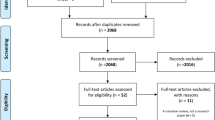
Finally, based on the results obtained from each search, we developed a diagnostic flow chart for SD (Fig. 1).

Diagnostic flow chart to be followed in case of suspected haematogenous or post-surgical SD. The predominant role of MRI in SD of haematogenous origin and of [18F]FDG-PET/CT in post-surgical SD is highlighted. *MRI should be performed with at least a 1.5 T magnet, with T1, T2 fat-suppressed, or short-tau inversion recovery (STIR) sequences with and without contrast medium. **Although indicated, in the case of PET/CT unavailability, MRI can be performed instead, with lower diagnostic accuracy. A combined 99mTc-MDP + 67Ga-citrate scintigraphy [with single-photon emission computed tomography (SPECT)/CT acquisitions] can also be performed. In these cases, if only MRI is performed or if [18F]FDG-PET/CT is inconclusive, a CT-guided biopsy is strongly indicated for final diagnosis. PET/MRI, if available, can be substituted for PET/CT
Diagnostic tools
Radiologic imaging
The role of radiology is to define the correct diagnosis as early as possible, to assist in percutaneous biopsy (if needed) and in follow-up of the disease, and to evaluate the presence of complications [39,40,41,42].
Plain film X-ray
Plain radiographs are usually the first imaging modality requested when infection is suspected [13, 43], despite their low sensitivity and specificity [44, 45]; they are also helpful for viewing implant loosening. Imaging includes anteroposterior and lateral projections of the suspected spinal segment [44, 45].
The detection of signs and abnormalities depends on the entity and can be seen when bone destruction exceeds 30%. Signs are usually not apparent on plain radiographs until 2–8 weeks after the initial symptoms [44, 45], and it should be considered that changes caused by infection may not be as apparent in patients with degenerative signs on imaging studies [44].
The main findings are blurred appearance of the cortical bone, erosion of the anterior corner of the vertebral end plate, progressive loss of disc height, narrowing of the intervertebral space, and development of osteolysis with further destruction of the subchondral plate. Tumefaction of the soft tissue and pre- or paravertebral soft tissue densities with fluid level may also be detected.
In advanced disease, the erosions can involve the entire vertebral end plate, and signs of bone reformation comprising peripheral sclerosis, osteophytosis, and a build-up of osteolytic lesions can coexist. All of these lesions may lead to significant osteolysis and vertebral compression, and disorders of spinal deformity may arise. Rarely, with indolent infections, the reactive sclerosis may produce an “ivory” appearance as the only evident change [46].
Magnetic resonance imaging (MRI)
MRI should be the first imaging modality performed, given its high sensitivity, specificity, and accuracy (reported as 96%, 92%, and 94%, respectively) for the diagnosis of SD. This is related to the high contrast resolution, direct multiplanar imaging capability, high sensitivity for soft tissue and bone marrow abnormalities, and the absence of ionising radiation, which make MRI the reference standard for imaging of spinal infections even in the postoperative setting, whereas it is usually not indicated in patient follow-up, as MRI findings can worsen despite clinical improvement [47,48,49,50,51,52,53].
The main utility of MRI is the possibility for diagnosis in the early stages of the infection, within the first 2 weeks in more than 50% of cases, when other radiologic imaging modalities are still normal. In a further 20% of patients, positive findings can be detected in the following 2 weeks, and so in the case of persistent clinical symptoms with a non-diagnostic early MRI scan, it is recommended that the exam be repeated a few days later [54].
The MRI examination should include the following sequences:
-
STIR or fat-saturated T2-weighted (T2-w) sequences that are fluid-sensitive and highly sensitive for the detection of inflammatory oedema [better than T2-w spin-echo (SE) sequences]
-
T1-weighted (T1-w) SE fat-suppressed pre- and post-administration of intravenous (i.v.) injection of contrast media, for morphological study and to differentiate between vascularised and non-vascularised lesions and/or necrotic inflammatory components
The infection usually begins near the end plate in the anterolateral vertebral body; the infection and inflammation cause marrow oedema, with a decreased signal in T1-w sequences, increased signal in T2-w sequences, and contrast enhancement in T1-w sequences after i.v. contrast injection [48,49,50].
When the erosion of the end plates occurs, the hypo-intense band of cortical bone appears thinned or absent [49]. An early sign of discitis is the loss of the intranuclear cleft seen in T2-w sequences. The intranuclear cleft consists of a linear transverse hypo-intense band within the central part of the disc in the sagittal or coronal plane; it is a normal aspect of the degenerative disc and can be detected in more than 90% of patients older than 40 years.
Following i.v. contrast media injection, disc enhancement may be homogeneous or patchy non-confluent areas of enhancement, and thick or thin areas of peripheral enhancement may be seen. If subsequently the infection involves all of the vertebral body and the intervertebral disc as well as the surrounding tissues, a hyper-intense signal on T2-w sequences or moderate and heterogeneous tissue enhancement in the T1-w sequences post-i.v. contrast injection is usually seen. If abscesses are present, they are seen as fluid collection with heterogeneous signal in T1-w sequences and with ring-enhancing thickened walls [49, 50]. When diffuse enhancement throughout the mass is seen, this is more consistent with granulation tissue, but if the clinical picture is suggestive of infection, the mass should be treated as an epidural abscess [12].
Spinal neoplasms on MRI may mimic findings in infectious discitis, especially when they are tubercular in aetiology, since both may have a low signal on T1-w and high signal on T2-w; the involvement of disc space helps in distinguishing infections from neoplasms, as tumours usually do not enter the disc space [50,51,52]. The aetiological diagnosis of SD can be made only by isolating the causative organism, but some imaging findings may be suggestive of a specific aetiology. For example, meningeal involvement, sub-ligamentous spread of infection to three or more vertebral levels, and paravertebral and intra-osseous abscesses with a thin, smooth wall are typical features of tubercular aetiology with relative sparing of the intervertebral disc [27].
A disadvantage of MRI is related to the over-estimation of the amount of infected tissue, as some of the signal changes are reactive; furthermore, in the presence of severe degenerative disc disease leading to oedema-like changes in the end plates and the adjacent discs, MRI may give false-positive results [53]. Bone involvement is not as well visualised as by CT, and in the preoperative assessment, CT scan may be more useful for defining the amount of tissue necrosis that requires surgical debridement. Also, in the postoperative setting, CT may be preferred to MR to avoid difficulty in reading the exam due to the increased T2 signal and contrast uptake at the surgical site. For the same reasons, MRI is not as sensitive for the onset of reparative changes; in this sense, there is evidence suggesting that some MRI changes may persist or even worsen during treatment, even in the presence of clinical improvement and negative lab tests, and may lead to unnecessary surgery [54]. The signs of a healing process include the following: reduction in the amount of oedema due to soft tissue inflammation; loss of gadolinium enhancement, which appears later (few weeks to few months after the onset of treatment), so the detection of some enhancement in patients with clinical improvement is not necessarily related to therapy failure but to an increase in granulation tissue due to the healing process; progressive bone restoration that may be seen after a median of 15 weeks as a rim of high signal intensity on T1-w images occurring at the lesion edges [53, 54].
Computed tomography (CT)
Computed tomography (CT) is readily available, easy to perform, and faster than MRI, and represents the best modality for the detection of bony abnormalities as minimal erosion of the end plates (before they become visible on X-ray), small vertebral foci of infection, or pathological calcification suggestive of TB [55].
It may be complementary to MRI, providing better definition of the extent of bony involvement, whereas MR is more useful in the evaluation of the central canal and the spinal cord [56, 57]. Contrast media is usually not injected except when MRI cannot be performed.
The main findings in an active state of infection are loss of bone architecture with areas of transparency and soft tissue replacement, end-plate erosion, and collapse of the disc space with abscess formation [46]. In the case of spreading in pre- and paravertebral locations, soft tissue masses may be seen; for the evaluation of these structures and of the involvement of the thecal sac, MRI is certainly more indicated [48, 49].
CT is currently used mostly for percutaneous needle biopsy and percutaneous drainage of abscesses and is an excellent modality in the early postoperative evaluation of spinal alignment and implant positioning [58, 59], even though, in presence of stainless steel implants, the image quality may be low due to implant-related artefacts. It is particularly useful when MR is contraindicated, not available, or equivocal [60, 61].
Even though CT is inferior to MRI in imaging soft tissue, the affected discs may be seen with hypodense areas in this context [3], soft tissue swelling and obliteration of fat planes around the vertebral bodies may be detected [54], and paravertebral abscesses involving the psoas can be identified with contrast [62].
Image-guided biopsy
Image-guided biopsy of the infected tissue is an important tool in the diagnosis of SD. Histopathological and microbiological examinations of biopsy specimens can enable a definite diagnosis of SD and can identify the causative pathogen.
The first non-invasive step for the identification of the possible aetiological agent of SD is performing blood cultures. It has been reported that they grow the causative microorganism in up to 60% of cases [13, 18, 21, 22, 54, 63]. The percentage of positive blood cultures is lower in postoperative infections [62]. Three blood samples must be collected at three different times for cultures. Urine and/or sputum cultures and swabs from any possible portal of infection should also be considered to investigate a primary focus of infection. Bone marrow aspiration may be useful if brucellosis is suspected, as well as urine and sputum for acid-alcohol-fast bacilli [3, 54].
CT or fluoroscopy-guided biopsy is the first invasive diagnostic step [58, 59, 64,65,66,67]. It is able to identify the bacterial agent in up to 91% of patients [13, 54]. Biopsy is the main procedure in patients with postoperative spondylodiscitis, as blood cultures in these patients are frequently negative [67].
The diagnostic yield of image-guided biopsy cultures varies widely between studies and can be influenced by several factors, including previous antibiotic therapy, patient clinical features, radiologist expertise, and number of samples sent. Biopsy specimens should be sent for Gram staining, aerobic and anaerobic cultures, and histopathology, since it can distinguish between pyogenic and granulomatous disease, and it is mandatory if tumour aetiology is suspected [3, 13, 54]. In patients with specific risk factors, cultures for mycobacteria, fungi, and Brucella should also be performed; molecular methods can be used as well to improve the chances of identifying pathogens [68, 69].
Biopsy must be performed under conditions of surgical asepsis, with local anaesthesia and conscious sedation, and with the patient in a prone position. The main points of access used are as follows: anterior for cervical spine lesions, transpedicular and posterolateral for the lumbar spine, and inter-costotransverse for the thoracic spine. Typically, a small incision is made to allow needle entry and an 18-gauge trocar is used to collect at least four bone samples (two from the upper end plate and two from the lower end plate). The disc sample has to be taken with a toothed micro-needle, according to disc compactness. At least three samples should be sent for microbiological analysis and two for pathological analysis; one sample will be frozen at −20° to perform any subsequent polymerase chain reaction (PCR), if needed. At the end of the procedure, the disc should be rinsed with saline solution, which is aspirated back and sent for culture. Blood cultures can be performed within 4 h of completion of the biopsy. It is important that material is sent and processed quickly to avoid loss of viability of fragile or fastidious organisms [36, 42, 54, 58, 59, 62].
Nuclear medicine imaging
Conventional radiopharmaceuticals for diagnosis of infection, such as labelled autologous leukocytes [white blood cells (WBC)], can fail to detect vertebral osteomyelitis, and the site of infection often appears as a “cold spot” in the scan [70,71,72,73,74,75,76,77,78]. Radiopharmaceuticals available for the study of spine infection include labelled diphosphonates (99mTc-MDP/HDP), 67gallium citrate (67Ga), and fluorodeoxyglucose labelled with fluorine-18 ([18F]FDG). Each has its advantages and limitations.
Scintigraphy with 99mTc-MDP/HDP and 67Ga-citrate
A review of 30 original articles published between 1984 and 2004 regarding different radionuclide imaging for diagnosis of spine infections [78] showed that approximately 324 lesions were studied with bone scans, with sensitivity of 81.4% and specificity of 40.7%. The advantages of this radiopharmaceutical include low cost, low radiation burden, and single-day imaging procedure. It is limited, however, by low specificity.
Prandini et al. reported sensitivity of 86.3% and specificity of 35.8% in 223 lesions investigated with 67Ga for suspected vertebral infection [78, 79].
A combination of 99mTc-MDP bone scintigraphy and 67Ga-citrate can be used to increase diagnostic accuracy, particularly in the case of post-surgical infections or to complement doubtful MRI findings in the case of primary infections [80,81,82].
Pros and cons
The advantage of 67Ga and 99mTc-MDP is their ready availability. Limitations of 67Ga include a higher radiation burden and time-consuming acquisition (up to 48 h and sometimes 72 h).
Interpretation criteria
In primary spine infections, the comparison of 99mTc-MDP bone scintigraphy with 67Ga-citrate may enable differentiation of infectious from inflammatory and degenerative disease. When 67Ga-citrate uptake is higher than 99mTc-MDP, the vertebral pathology may have an infectious origin, while higher uptake of 99mTc-MDP than 67Ga-citrate may indicate a degenerative origin [81]. The overall accuracy of bone/67Ga imaging is about 65–80% [70, 81, 82].
Influence of medication
Iron therapy (Ferrograd), chemotherapy (even 3 months after the end of therapy), corticosteroids (prednisolone), and Gd-DTPA (if administered 24 h before) can alter the qualitative analysis of 67Ga-citrate.
PET or PET/CT with [18F]FDG
The role of [18F]FDG for diagnosing spinal infection has been investigated extensively. [18F]FDG is transported into cells by glucose transporters GLUT1 and GLUT3 and, after phosphorylation by hexokinase, remains inside and is not metabolised. The uptake of [18F]FDG is related to the cell metabolic rate and the number of glucose transporters on the cell surface [83]. Kubota et al. demonstrated that [18F]FDG uptake in tumours was, in fact, partly the result of newly formed granulation tissue and activated macrophages associated with tumour necrosis and growth [84]. Using autoradiography, the same investigators demonstrated that [18F]FDG uptake by non-neoplastic cells was even higher than its accumulation in viable tumour cells [85]. Detailed histopathologic and autoradiographic analysis of an experimental soft tissue abscess model in rats showed that the highest FDG uptake was within areas of inflammatory cell infiltrate, which was composed primarily of neutrophils in the acute phase and macrophages in the chronic phase [86]. In activated inflammatory cells such as neutrophils, lymphocytes, monocytes, and macrophages, an increase in both the number and expression of glucose transporters is found, as well as increased affinity of these transporters for deoxyglucose [86].
PET or PET/CT with [18F]FDG has shown very high sensitivity with relatively low specificity in diagnosing spine infections. In 2006, Rosen et al. reported the presence of abnormal spinal [18F]FDG uptake, classified on a scale of 0–4, showing the relationship between the severity of findings on 18F-FDG PET and the severity of degenerative spinal disease on CT [87], which confirmed the occasional non-specificity of [18F]FDG uptake in the spine. Ohtori et al. and Stumpe et al., however, found a high rate for the detection of spondylodiscitis if [18F]FDG-PET was used in addition to conventional radiologic imaging [88, 89]. In a prospective cohort study with over 300 patients, Ohtori et al. demonstrated that a definitive diagnosis of spine infection was achieved more often when [18F]FDG-PET was utilised [88]. This was reported specifically in patients with spinal infections presenting as Modic type 1 signals on MRI, which made the distinction between common Modic changes and spine infection challenging. [18F]FDG-PET imaging is useful in the work-up of patients with metallic implants, since it is not affected by artefacts. In fact, [18F]FDG-PET imaging can also provide results in a short time (within 2 h) with a resolution of up to 4–5 mm [87].
Kim et al. evaluated the prognostic effectiveness of follow-up imaging with [18F]FDG-PET/CT in 30 patients with spinal infection after therapy. The authors found that [18F]FDG-PET/CT is useful for the evaluation of residual infection after treatment. They suggest using quantitative indexes, such as the standardised uptake value (SUV), to evaluate the residual infection [90].
Fuster et al. prospectively evaluated the usefulness of [18F]FDG-PET/CT in comparison to bone scan and 67Ga scintigraphy for the diagnosis of SD in 34 patients, showing the best diagnostic accuracy for [18F]FDG-PET/CT [sensitivity 89%, specificity 88%, positive predictive value (PPV) 89%, negative predictive value (NPV) 87%, accuracy 88%] [82].
Hungenbach et al. reported sensitivity of 86% and specificity of 95% for the diagnosis of SD using [18F]FDG-PET. The authors note that the use of [18F]FDG uptake patterns as interpretation criteria helps to predict or exclude SD. [18F]FDG -PET is therefore an important tool in inflammation imaging and can be used in the diagnostic algorithm of difficult cases with suspected SD. In contrast, a positive [18F]FDG-PET result does not always clearly establish the cause of increased [18F]FDG uptake [91].
Despite the relatively low specificity of radiopharmaceuticals available to study spine infection, radionuclide imaging is strongly recommended for assessing disease activity during follow-up after medical therapy [92, 93].
Another interpretation criterion for [18F]FDG-PET/CT findings was proposed by Riccio et al., who state that [18F]FDG uptake confined to the margins of a destroyed disc after antibiotic therapy for pyogenic spine infection must not be considered indicative of persistent infection, and likely represents mechanically induced inflammation. [18F]FDG uptake in bone or soft tissue does indicate active infection. Quantification of activity could not reliably differentiate patients with active infection from those without active infection and those who had successful response to therapy. The pattern of activity is critical for accurate interpretation [94].
Lee et al. observed in a preliminary study that SUVmax seemed to reflect the activity of infectious spondylitis in 22 patients. [18F]FDG-PET/CT may also be complementary to MRI for differentiating pyogenic and tuberculous spondylitis [95].
Published data indicate that [18F]FDG-PET/CT is superior to 67Ga for the diagnosis of spinal infection and paraspinal soft tissue infection [82], and should be used in selected cases as an alternative to MRI [3, 61, 94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109]. All studies in which a comparison between MRI and [18F]FDG-PET/CT was performed have shown that a combination of the two techniques detects spinal infection in 100% of patients [102, 110, 111].
Because of the suboptimal specificity of [18F]FDG, alternative experimental radiotracers such as radiolabelled antibiotics [112] and radiolabelled vitamin [113, 114] are being developed and tested. Although the results obtained in preliminary studies are highly encouraging, full validation in the clinical setting requires further large-scale studies.
Pros and cons
The advantages of [18F]FDG include very high NPV, high-quality imaging, and short acquisition time. Disadvantages include relatively low specificity (ranging from 35.8% to 87.9%), and the inability of [18F]FDG-PET/CT to reliably differentiate infection from neoplastic lesions or pronounced degenerative vertebral disease [87]. Other limitations are scarce availability, non-negligible radiation burden, and higher costs.
Interpretation criteria
The qualitative analysis of [18F]FDG-PET is positive when [18F]FDG uptake is higher than that in healthy vertebral bone tissue. Only one study proposes a connection between different patterns (score 0–4) of 18F-FDG uptake and different states of spine infection diseases, as follows:
“Score 0: Normal findings and physiological [18F]FDG distribution (consistent with no infection), Score 1: Slightly elevated uptake in the inter- or paravertebral region (consistent with no infection), Score 2: Clearly elevated uptake of a linear or disciform pattern in the intervertebral space (consistent with discitis), Score 3: Clearly elevated uptake of a linear or disciform pattern in the intervertebral space and involvement of ground or cover plate or both plates of the adjacent vertebrae (consistent with SD), Score 4: Clearly elevated uptake of a linear or disciform pattern in the intervertebral space and involvement of ground or cover plate or both plates of the adjacent vertebrae + surrounding soft-tissue abscess (consistent with SD)” [91].
Influence of medication
Corticosteroids, antiepileptics, catecholamines, and chemotherapy (within 1 month after the end of therapy) can alter the qualitative analysis of [18F]FDG.
Gemmel et al. proposed a diagnostic algorithm based on the analysis of many relevant papers on diagnostic imaging published from 1986 to 2004. This algorithm separated SD of a non-violated spine from post-surgical/post-traumatic SD. The reported diagnostic method of choice was MRI in the first case (non-violated spine), followed by 99mTc-MDP bone scintigraphy with 67Ga-citrate or [18F]FDG-PET when MRI is not readily available or is contraindicated. In the non-violated spine, the diagnostic choice is based on the presence of metallic implants: the algorithm recommends [18F]FDG-PET as the first choice in patients with metallic implants (to overcome the problem of artefacts with MRI), keeping in mind that a false-positive finding is possible, likely owing to aseptic granulomatous reactions. In the absence of metallic implants, the authors suggest MRI, if possible, or [18F]FDG-PET, noting the possibility of false-positive findings up to 12 months post-event for MRI and up to 6 months for [18F]FDG-PET. 67Ga-citrate SPECT is suggested in patients without metallic implants when MRI and [18F]FDG-PET are not available [115].
With the advent of hybrid imaging, and given the increasing presence of available data on SPECT/CT, PET/CT, and PET/MRI, we believe that this algorithm needs to be upgraded. The algorithm also lacks information about inconclusive findings of diagnostic imaging and the final step to take in the case of positive results.
Comparison with published guidelines
There are two available guidelines on SD: the Infectious Diseases Society of America (IDSA) guidance on native vertebral osteomyelitis published in 2015 [36], and guidance from the French Infectious Diseases Society (SPILF), published in 2007 [68].
The IDSA guidelines [36] were prepared by a panel of experts (infectologists, orthopaedic specialists, rheumatologists, and neuroradiologists) without the involvement of nuclear medicine specialists. The GRADE system [Grading of Recommendations, Assessment, Development and Evaluations] is used to evaluate the quality of evidence. It is suggested that MRI be performed as a first diagnostic imaging modality when native vertebral osteomyelitis is suspected, although there is no detailed description of the MRI acquisition modality.
With regard to biopsy, IDSA notes that the gauge of the needle and the administration of antibiotics during the biopsy procedure have no significant impact on outcome.
During follow-up, PCR and ESR assay is recommended, while MRI should be performed only in the case of clinical worsening, followed by new biopsy.
The use of nuclear medicine (combination of spine 67gallium/99mTc bone scan, or CT scan or PET scan) is suggested if MRI cannot be obtained.
The SPILF 2007 guidelines [68], formulated by a larger panel of experts (infectivologists, orthopaedic specialists, anatomopathologists, neurosurgeons, neuroradiologists, and nuclear medicine specialists), suggest X-ray as the first diagnostic imaging modality in cases of suspected vertebral osteomyelitis, followed by MRI. There is a detailed description of the acquisition modality of MRI (use of fat suppression sequences and i.v. contrast) as well as the modalities for the execution of the biopsy. The use of nuclear medicine or CT is suggested if MRI cannot be obtained.
During follow-up, PCR assay and X-ray are recommended, while MRI should be performed only in the case of clinical worsening.
Consensus statements
SD should be suspected in patients with new or worsening spine pain and/or new myelo-radicular symptoms, and at least one of the following: fever, elevated ESR or CRP, bloodstream infection, or infective endocarditis
Level of evidence: 4
The symptoms of SD are nonspecific and the onset is insidious. As a result, diagnosis of SD may be difficult. Regarding clinical symptoms, back or neck pain is frequently reported, although some studies found that up to 15% of patients can be pain-free [3, 35]. Fever is less common, occurring in about 50% of patients. Neurological deficits including leg weakness, paralysis, sensory deficit, radiculopathy, and loss of sphincter control may be present. Elevated ESR, CPR, and WBC counts are variably present.
In all patients with suspicion of SD, an accurate medical history should be obtained, with special attention to prior surgical procedures, history of urinary tract infection, bloodstream infection, skin or soft tissue infection, signs and symptoms of endocarditis, and history of intravenous drug use.
CRP, ESR, and WBC counts should always be performed in patients with suspected SD
Level of evidence: 4
Elevated ESR, CPR, and WBC counts are variably present in SD. The sensitivity of elevated ESR or CRP in patients with back pain ranges from 94% to 100% [10, 19, 116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,139,140,141], but the specificity is low. The inflammatory markers are useful to rule out the presence of an infection or a malignancy in patients with back pain. WBC counts are normal in up to 40% of patients with SD [35].
Blood cultures (for both aerobic and anaerobic bacteria) should always be performed in patients with suspected SD
Level of evidence: 4
Since the pathogenesis of SD frequently involves haematogenous spread, blood cultures could enable the identification of the bacterial agents of SD, with reported microbiological diagnosis varying between 20% and 60% [142,143,144,145,146,147]. The sensitivity of blood cultures is lower in postoperative infections [63] and higher in patients with fever [116]. At least two bacterial blood culture (aerobic and anaerobic) sets should be routinely performed for all patients with suspected SD [147]. Blood cultures may also allow the diagnosis of candidemia in patients with fungal SD. In patients with epidemiological risk factors for brucellosis, blood cultures need to be incubated for up to 2 weeks.
For patients with suspected SD and epidemiological risk factors for brucellosis, specific serological tests should be performed
Level of evidence: 4
Brucellosis is a common zoonosis in endemic areas, with high incidence in countries of the Mediterranean Basin, Latin America, the Middle East, parts of Africa, and Western Asia. In patients with suspected SD reporting travel to or residence in endemic countries or with a history of consumption of unpasteurised products or occupational history, serological test for brucellosis should be performed. The Coombs test is commonly used for the diagnosis of brucellosis [148, 149]; in one study, a titer of ≥1:160 was found in all patients with Brucella-related native vertebral osteomyelitis [150, 151]. Enzyme-linked immunosorbent assay (ELISA) has proven to be superior in complicated cases of brucellosis with negative Coombs test results and might be of value in patients with brucellar SD [149]. In a retrospective study including 96 patients with brucellar SD, Colmenero et al. reported that standard agglutination test titers were ≥ 1:160 for 68% of patients, and Coombs anti-Brucella or immunocapture-agglutination test titers were ≥ 1:320 for 79% of patients. The combined use of standard agglutination test and Coombs or immunocapture agglutination test enabled correct serological diagnosis in 89.5% of the 96 patients. In the same study, the standard agglutination test was >100 in 99% of patients [148].
For patients with suspected SD and risk factors for Mycobacterium tuberculosis, a PPD test and an interferon-γ release assay should be performed
Level of evidence: 4
Tuberculosis (TB) is a very common cause of spinal infection worldwide [19, 21, 23, 152, 153]. In countries where the incidence of TB is low, tubercular SD is most often diagnosed in patients originating from endemic countries and in immune-compromised patients. In patients with SD and risk factors for TB infection, a purified protein derivative (PPD) test or an interferon-γ release assay may be useful. The interferon-γ release assay has been associated with higher sensitivity than PPD [154]. It is important to emphasise that these tests may yield both false-positive and false-negative findings. Thus, regardless of test results, in the case of high suspicion of TB infection, an image-guided aspiration biopsy should be performed in order to perform mycobacterial tissue cultures.
In recent years, an enzyme-linked immunospot (ELISPOT) assay has been commercialised (T-SPOT.TB; Oxford Immunotec, Oxford, UK) that is based on the detection of interferon-γ released by activated T lymphocytes. The ELISPOT assay has been demonstrated to provide useful support in the diagnosis of osteoarticular TB with high sensitivity and specificity [155,156,157,158].
Plain film X-ray should always be performed in patients with suspicion of spine infection for purposes of differential diagnostic and follow-up
Level of evidence: 5
Plain radiographs are usually included in the initial imaging assessment of patients complaining of back pain [41], even though, considering the low sensitivity and specificity, they should be avoided when infectious discitis is suspected. Changes in pyogenic discitis are not apparent on plain radiographs until 2–8 weeks after the initial symptoms [42,43,44], and so negative radiographic findings do not exclude infection, especially in early phases.
No paper has analysed the role of X-rays in the follow-up of SD as well, and in particular there are no indications that X-rays might be helpful in the follow-up of patients with haematogenous SD treated with antibiotics. The actual role of X-rays, performed with dynamic acquisition, applies to patients with SD after healing for the evaluation of spine stability and/or in the follow-up of patients treated for SD with stabilisation [159].
In haematogenous SD, the first diagnostic imaging modality is MRI, if patients have no specific contraindications
Level of evidence: 5
There are no articles specifically addressing this point in the time range considered for the search. Nevertheless, MRI properties are well known, and the high sensitivity, specificity, and accuracy in the diagnosis of SD were underlined in several studies [54, 159] and in previously published guidelines [36]. MRI may detect infection in the early stages, when other imaging modalities are still normal (radiography) or nonspecific (nuclear medicine) [159, 160], and so it should be performed as first examination in first diagnosis of SD if the patient has no specific contraindications.
MRI must be performed with T1, T2, and T2 fat-suppressed or STIR sequences without and with contrast medium with T1 fat suppression technique
Level of evidence: 5
There are no recently published trials focused specifically on MRI acquisition protocols for diagnosis of SD. However, in clinical practice, MRI studies for suspected SD are usually performed using the described sequences and contrast medium injection [42, 45, 51, 57, 61, 110].
SPILF guidelines [67] recommend including T1-w, T2-w, and T2-w sagittal sequences with fat saturation, and completing the examination with i.v. contrast administration. In addition, IDSA guidelines [36] suggest the use of i.v. contrast administration, as Gd-DTPA enhancement may be the first sign of an acute inflammatory process, and it is useful for detecting the extension of infectious processes in the paravertebral spaces.
MRI in suspected spine infection should be performed with at least a 1.5 Tesla magnet
Level of evidence: 5
There are no reports specifically addressing the question of whether a 1.5 Tesla magnet is the minimum required for the diagnosis of SD. However, the vast majority of authors of published papers performed MRI using 1.5 T or higher magnet [55, 110, 161, 162].
CT may be useful for diagnosis only when MRI is contraindicated, not available, or equivocal
Level of evidence: 3
CT has a minor role in the diagnosis of SD, as it is inferior to MRI in imaging soft tissue [57]. It represents the best modality for detecting minimal bony abnormalities, so it may be complementary to MRI [9, 36, 37, 55] and constitutes an alternative if there are contraindications to MRI. It is also an excellent modality in early postoperative evaluation and allows guided biopsy to be performed [64, 163].
CT may be useful when MRI is contraindicated, not available, or equivocal, as a paper not included in this literature analysis showed [164].
In primary and post-surgical SD, if MRI is contraindicated, the imaging modality of choice is [18F]FDG-PET/CT
Level of evidence: 2
A comparison between bone scan, 67Ga scintigraphy, and [18F]FDG-PET/CT showed the best diagnostic accuracy for [18F]FDG-PET/CT (sensitivity 89%, specificity 88%, PPV 89%, NPV 87%, accuracy 88%) for diagnosing spinal infection and paraspinal soft tissue infection [82].
The added value of [18F]FDG-PET was reported specifically in patients with spinal infections presenting as Modic type 1 signal on MRI. [18F]FDG-PET imaging can also provide results within a short length of time (within 2 h), with resolution of up to 4–5 mm, and it is useful in the work-up of patients with metallic implants, since it is not affected by metal-induced artefacts [88].
The sensitivity and specificity of [18F]FDG-PET were higher for the diagnosis of spinal infection when the interpretation criteria proposed by Hungenbach et al. were applied (sensitivity 86% and specificity 95%). The authors state that the use of [18F]FDG uptake patterns in the interpretation criteria of [18F]FDG-PET helps to predict spine infection; in contrast, a positive [18F]FDG-PET result does not always clearly establish the cause of increased [18F]FDG uptake [91]. A preliminary study in 22 patients proposed the use of SUVmax of [18F]FDG as a marker of the activity of infectious spondylitis. In this small patient population, [18F]FDG-PET/CT seemed to complement MRI for differentiating pyogenic and tuberculous spondylitis [96]. Published data indicate that [18F]FDG-PET/CT is superior to 67Ga for diagnosing spine infection and paraspinal soft tissue infection [82] and should be used in selected cases as an alternative to MRI [3, 61, 95,96,97,98,99,100,101,102,103,104,105,106,107,108,109].
All included papers, both original prospective [82, 88, 90,91,92, 94, 95, 103, 105, 107,108,109,110] and retrospective [111] studies and reviews [12, 13, 37, 78,79,80, 115, 165,166,167], agree therefore that in patients with suspected SD with contraindications to MRI, [18F]FDG-PET is a promising and accurate imaging technique for diagnosis of spine infection with or without hardware. All papers also agree, however, that the number of patients studied is still limited.
In post-surgical SD, with or without spinal hardware, [18F]FDG-PET/CT can detect both spine infection and soft tissue infection
Level of evidence: 2
Twenty-five [18F]FDG-PET/CT scans performed in children and young adults with suspected infection of spinal hardware showed that increased [18F]FDG uptake in the soft tissue and bone immediately adjacent to the posterior spinal fusion rods at multiple contiguous vertebral levels was the most common [18F]FDG-PET/CT finding in the presence of hardware infection [106]. To avoid the false-positive findings of [18F]FDG-PET/CT because of nonspecific accumulation of FDG for the concomitant postoperative inflammation at the surgical site, the time between spinal hardware placement and [18F]FDG-PET/CT imaging should be at least 4 months. Moreover, it is necessary to evaluate both non-attenuation-corrected (NAC) and attenuation-corrected (AC) PET images in patients with suspected hardware infection in order to avoid the effect of metal-induced artefacts on CT AC images. Unfortunately, patients with hardware loosening have shown focal uptake associated with one or two hardware components, usually at a single vertebral level at the lower or upper extreme of the hardware construct [106]. This nonspecific sign should always be considered; inflammatory reactions triggered by spinal implants also may adversely affect specificity [101]. Nevertheless, there is an expanding body of evidence that supports the use of [18F]FDG-PET and PET/CT for diagnosing spinal infection, especially in patients with MRI contraindications and in the postoperative spine [101].
In another study [18F]FDG-PET/CT and MRI were performed in all patients with spinal hardware for the diagnosis of spine infection. [18F]FDG-PET/CT was effective in visualising infection despite the existence of spinal implants, whereas MRI was not. In addition, the distribution of infection was visible by PET/CT. Thus, the strongest attribute of PET/CT is the capacity to specify the true focus of infection, thereby facilitating selective removal of implants, although it may not always be necessary in the early phase of surgical site infection cases. These observations suggest the use of separate surgical approaches, that is, different pathways for decompression and screw insertion. In this application, PET/CT seems to provide an important benefit in choosing which implants should be preserved or removed [108]. Despite these excellent results, a large population-based study is warranted.
All papers, both original studies [102, 106, 108] and reviews [37, 78, 79, 165, 167, 168], included for the evaluation of this statement agree that [18F]FDG-PET/CT is an accurate imaging technique for post-surgical spine infection diagnosis with or without hardware. Even though the number of patients studied is still limited, evidence-based data indicate that [18F]FDG-PET/CT has better diagnostic accuracy than other diagnostic modalities.
In patients with suspected spine infection and elevated ESR and/or CRP and doubtful MRI, [18F]FDG-PET/CT should be performed
Level of evidence: 1
MRI is the diagnostic modality of choice for suspicion of haematogenous spine infection. It presents certain limitations, however, particularly when some of the classical imaging findings are atypical or even absent and in the presence of spinal hardware or bone fractures. Although most of the published series are small, [18F]FDG-PET/CT appears to be superior to MRI in the detection of spine infection and in the differentiation of degenerative from infectious end-plate abnormalities. [18F]FDG-PET/CT shows high sensitivity and image resolution; however, specificity remains an issue. In fact, [18F]FDG may not be able to differentiate infected tissue from tumours [169]. Furthermore, inflammatory reactions induced by spinal implants may also adversely affect specificity [101]. Nevertheless, there is an expanding body of evidence that supports the use of [18F]-FDG PET and PET/CT for diagnosing SI, especially when MRI is contraindicated and in the postoperative spine [101, 115].
All included papers, both original retrospective [106, 111, 139] and prospective [42, 88, 95, 105, 110] studies and reviews [12, 37, 78,79,80, 115, 167, 170], agree that [18F]FDG-PET/CT is a valid tool in the case of inconclusive MRI findings, especially in patients with suspected post-surgical infections, with or without hardware. From the data in the literature, evidence clearly emerges that FDG-PET is superior to MRI for detecting low-grade spondylitis or discitis, and is a useful adjunct to MRI for differentiating severe spinal degenerative changes from infection [88].
In patients with suspected spine infection, elevated ESR and/or CRP, doubtful or unperformable MRI, and doubtful or unperformable [18F]FDG-PET/CT, a CT scan should be performed with an image-guided biopsy
Level of evidence: 2
There are no articles in the available literature specifically focused on this point.
According to SPILF guidelines [68], when MRI or scintigraphy is doubtful, the examination should be repeated if symptoms persist, and so a similar approach may be suggested if the results of [18F]FDG-PET/CT and/or MRI are doubtful. In addition, given the high NPV of MRI and PET/CT, a diagnosis of SD should be excluded if these examinations are negative.
CT scan is indicated in patients who cannot undergo other imaging studies (MRI or PET/CT); the combination with percutaneous needle aspiration biopsy has high specificity and is therefore quite useful when positive, especially in patients with doubtful results at MRI and PET/CT. However, it has low sensitivity and can miss a substantial proportion of patients, so surgical debridement and open biopsy are sometimes required for definitive diagnosis [171]. Even though there are no evidence-based medicine (EBM) data on the benefits of CT image-guided biopsy, the panel believes that CT-guided biopsy should be performed in all cases with high suspicion of spinal infection and inconclusive or unperformable MRI and/or PET/CT.
The role of hybrid PET/MRI, although promising, needs to be evaluated
Level of evidence: 5
No articles describing the potential role of hybrid PET/MRI for diagnosis of infection were found for the period from 2006 to 2015. We report one study, published in September 2016, not included in this literature analysis, where the authors note that the use of FDG-PET/MRI in 30 patients with inconclusive clinical or MRI findings significantly increased diagnostic accuracy for the detection of SD [172].
It is reasonable to think that PET/MRI can be substituted for [18F]FDG-PET/CT imaging in the diagnosis of spine infection.
In case of negative MRI or negative [18F]FDG-PET/CT, the diagnosis of SD should be excluded
Level of evidence: 5
One retrospective [110] and two prospective [103, 110] studies reported on the high NPV of [18F]FDG-PET/CT and MRI in patients with suspected haematogenous spine infection. All published studies from January 2006 to December 2015 underlined the importance of a negative [18F]FDG-PET/CT for the exclusion of spine infection. Even though there are no EBM data on the utility of the high NPV of [18F]FDG-PET/CT in suspected post-surgical spine infection, it is reasonable to think that [18F]FDG-PET/CT, with its high sensitivity, should be the first imaging modality in patients with secondary SD.
An image-guided aspiration biopsy should be performed in all patients with suspected SD based on clinical, laboratory, and imaging studies
Level of evidence: 4
Microbiological diagnosis of SD is extremely important for choosing the appropriate antimicrobial therapy. The microbiological findings should guide the treatment of SD to improve the outcome of patients and to limit the use of unnecessary antibiotics, which can cause adverse effects in humans and can have negative ecological implications. Empirical broad-spectrum antibiotic treatment should be administered in cases of severe sepsis once blood cultures have been taken [36].
Image-guided percutaneous needle aspiration biopsy is a relatively safe diagnostic tool [58, 59, 171, 173,174,175,176,177]; it can confirm the suspicion of SD and, importantly, can allow for the identification of the aetiological agent causing SD. It has been reported that cultures of specimens obtained from an image-guided biopsy may enable a microbiological diagnosis in 50–60% or more of cases [116, 174]. Aerobic and anaerobic cultures should be performed from biopsy specimens, although inoculation of biopsy material into blood culture bottles has been performed by some investigators [65, 116]. To improve the diagnostic yield, more than one specimen should be submitted for culture [173].
Mycobacterial, brucellar, and fungal cultures should be obtained in patients with risk factors for these infections [39, 130, 144, 148,149,150,151, 178,179,180,181].
Molecular diagnostic methods using PCR can be employed, in addition to standard cultures, to improve the chance of identifying microorganisms responsible for SD [141, 182,183,184,185,186,187]. The use of PCR methods can be particularly helpful when cultures of biopsy specimens are negative and in patients who have received prior antimicrobial therapy [141, 188].
PCR is also useful for detecting Mycobacterium tuberculosis from biopsy specimens. Studies have reported sensitivity of 95% and specificity of 83% for this test in detecting M. tuberculosis from formalin-fixed, paraffin-embedded tissue samples in cases of histologically proven tuberculous spondylitis [182]. Molecular methods may be used for diagnosis of brucellosis [186, 187].
In patients with risk factors for fungal SD (i.e. immunosuppression, long-term indwelling venous catheter, intravenous drug abuse, neutropenia), biopsy specimens should be sent for fungal cultures. PCR for the detection of fungal-specific nucleic acids can increase the sensitivity of standard cultures [189].
Histological analysis of biopsy specimens should be performed along with microbiological examinations. Histological analysis can reveal the presence of acute or chronic inflammation, granuloma, and malignancy. Ziehl–Neelsen staining for mycobacteria can be helpful.
In some cases, image-guided biopsy might be avoided.
According to the IDSA guideline for the diagnosis and treatment of native vertebral osteomyelitis, biopsy is not recommended for patients with a blood culture positive for S. aureus [35]. In our literature review, we found only one paper supporting this suggestion, which reported a retrospective study including 125 patients with vertebral osteomyelitis. The authors found that 12% of patients (9/74) with microbiologically confirmed vertebral osteomyelitis had a previous finding of bacteraemia with the same pathogen within the prior year; 24% of patients with S. aureus vertebral osteomyelitis had previous S. aureus bacteraemia [146].
According to the IDSA guideline, image-guided biopsy should not be performed in patients with persistent positive blood cultures for Staphylococcus lugdunensis, or in dialysis patients or patients with intravascular devices infected with other CoNS [36]. No definite recommendations are reported for patients with suspected SD and concomitant bloodstream infection with other microorganisms (i.e., Candida species, Enterobacteriaceae, streptococci, Pseudomonas species); in these clinical settings, the decision to perform an image-guided aspiration biopsy remains at the discretion of the treating physicians [36].
Evaluating the available published data on brucellar SD, it seems reasonable not to perform image-guided biopsy in patients coming from or living in areas where brucellosis is endemic and who have serological tests or blood cultures positive for Brucella [131, 145, 148]. Colmenero et al. reported retrospective data on 96 patients who received a diagnosis of brucellar vertebral osteomyelitis in a tertiary care hospital in Spain, the large majority of whom were diagnosed through blood cultures and serological tests for Brucella, with only 34% of patients requiring vertebral biopsy [148].
Antibiotic therapy should be discontinued or postponed before biopsy
Level of evidence: 4
In clinical practice, the dogma of withholding antibiotics before obtaining microbiological cultures is well recognised. Some studies have confirmed the importance of discontinuing antibiotic therapy in order to improve the chances of obtaining a microbiological diagnosis of SD. De Lucas et al. found that diagnostic rates obtained in patients with previous antibiotic treatment were significantly lower (23% vs 60%, p = 0.027) than those in patients not exposed to antibiotics [180]. Kim et al. retrospectively collected data on patients diagnosed with primary pyogenic vertebral osteomyelitis to identify factors associated with positive results on microbiological diagnosis. Duration of antibiotic exposure was assessed and defined as the time between initiation of antibiotics and obtaining vertebral tissue or blood samples for culture. The authors found that the proportion of patients exposed to antibiotics in the group with a microbiological diagnosis was significantly lower than that in the group with negative blood or biopsy cultures (12.7% vs 46.7%, p = 0.001) [116].
However, some studies found no significant effect of antibiotic exposure on the probability of identifying the causative microorganism in patients with SD [171, 190, 191].
In adult patients with haematogenous SD, the effect of antibiotic exposure within 14 days pre-biopsy was evaluated. A multivariate regression model for predicting a positive biopsy culture result among patients with haematogenous SD showed that a positive biopsy result was found only when open biopsy was performed. Previous antibiotic treatment (OR = 2.3; 95% CI: 0.8–6.2; P 5 1), was not significantly associated with negative culture results [191]. Only 17 (28%) of 60 patients with antibiotic exposure had potentially false-negative culture results because of the empirical antibiotic treatment. A possible explanation reported by the authors was that severely ill patients are more likely to be started on empirical treatment before undergoing biopsy. These patients may also have more severe infections. Importantly, in this study, the frequency with which empirical antibiotics matched the susceptibility of recovered pathogens was assessed, and the authors found that 63% (38/60) of patients given empirical antibiotics had been treated with an antibiotic matching susceptibility and still grew the bacteria [192]. In a further retrospective study, Agarwal et al. found no statistical difference in the rate of biopsy positivity even when the rate of culture positivity was lower in patients who had been receiving antibiotics. Importantly, in this study the duration of antibiotic exposure was assessed: culture positivity was lower in patients receiving antibiotics for 4 or more days as compared to patients exposed to antibiotics for 1–3 days [193]. Similarly, Kim et al. reported that short-term exposure to antibiotics had a weak negative effect on culture outcome and that the effect increased with duration of antibiotic treatment [116].
Even though not all studies were able to demonstrate the effect of previous antibiotic therapy on the rate of microbiological culture positivity, the panel believes that antibiotics should be discontinued or postponed before performing a diagnostic biopsy. Antimicrobial therapy should not be withheld in patients with impending sepsis or haemodynamic instability. The optimal duration of antibiotic-free time before the image-guided biopsy has not been established.
In patients with suspected SD based on clinical, laboratory, and imaging studies and a negative biopsy (histology and microbiology), another biopsy should be done
Level of evidence: 4
There are no studies that specifically address the issue of management of patients with suspicion of SD and non-diagnostic blood cultures and biopsy specimens results.
In these cases, if not already done, the first step could be to search for mycobacterial, fungal, or brucellar infection (through both specific cultures and molecular methods). Epidemiological evaluation is essential in guiding the choice of tests to be performed. A second image-guided biopsy should then be considered.
A retrospective multicenter study evaluated the microbiological diagnostic yield of a second needle biopsy following an initial negative biopsy in suspected SD. The two percutaneous needle biopsies (first and second) had a similar yield (43% vs 39.4%). A positive first biopsy and a positive second biopsy following an initial negative one led to microbiological diagnosis in 79.6% (74/93) versus 44.1% (60/136) of cases, respectively [179].
Similarly, Friedman et al. reported an increase in the rate of percutaneous biopsy positivity with repeated biopsy [194].
Percutaneous endoscopic discectomy and drainage (PEDD) has been also proposed as an option to obtain diagnostic specimens. In a retrospective study, Yang et al. compared the diagnostic value of CT-guided biopsy with that of PEDD. The causative pathogens of SD were found in 90% of patients in the PEDD group, and the positive culture rate was superior to that in the CT-guided biopsy group [58]. Another study reported the usefulness of PEDD for identifying the causative pathogen of SD [195].
Some experts recommend performing an open biopsy when image-guided biopsy is inconclusive [37]. The rationale behind the recommendation is that some studies have reported a higher rate of culture positivity with surgical samples [174, 196, 197].
Bhavan et al. noted that open biopsy was more likely to result in pathogen recovery [14 (93%) of 15 open biopsies vs 14 (48%) of 29 needle biopsies; p = 0.003] [119].
In another study, four out of seven negative cultures (57.1%) from percutaneous CT-guided biopsies were positive in subsequent cultures of samples obtained during surgery [120].
In patients with SD diagnosed by [18F]FDG-PET/CT, a second [18F]FDG-PET/CT scan can be performed to evaluate the response to antibiotic therapy
Level of evidence: 4
Because [18F]FDG uptake signals increased metabolic activity of the activated cells that are present in infected tissue, semiquantitative analysis of the [18F]FDG-PET/CT images can be useful for evaluating the response to therapy.
Thirty patients with SD underwent dual-time-point acquisition [18F]FDG PET/CT after antibiotic therapy in order to evaluate treatment response. The maximum and mean SUVs of the initial and follow-up images were calculated, and the authors found that the change in maximum SUV was a powerful predictor of residual spinal infection, concluding that [18F]FDG-PET/CT seemed to be useful for the discrimination of residual and non-residual spinal infection after treatment [90].
Riccio et al. proposed another interpretation criterion for [18F]FDG−PET/CT images during treatment response in patients with post-surgical pyogenic SD. They state that [18F]FDG accumulation in bone or soft tissue does indicate active infection, while [18F]FDG accumulation limited to the margins of a destroyed disc after antibiotic therapy may be considered nonspecific and likely represents inflammation due to mechanically induced reactions. Quantification of activity could not reliably differentiate patients with active infection from those without active infection and those with a successful response to therapy. The pattern of activity is critical for accurate interpretation [94]. [18F]FDG-PET/CT, performed for the interim evaluation of response to therapy in patients with haematogenous spine infection [92], has shown very high diagnostic accuracy and seems to be a valid tool for decisions regarding patient treatment. However, two reviews [166, 168], along with original prospective [90, 92, 94, 105, 107] and retrospective [111, 198] studies, showed inconsistent results when [18F]FDG-PET/CT was repeated in patients during follow-up, so we can conclude that the number of cases (150 patients) is still too small to definitively state that [18F]FDG-PET/CT is the correct diagnostic method for evaluation of treatment response.
Conclusions
Clinical evaluation in patients with suspected spinal infection represents the first step in the diagnostic work-up of the disease. The presence of symptoms such as new or worsening spine pain and/or new myelo-radicular disorders, accompanied by fever and/or elevated ESR, CRP, or WBC and/or bloodstream infection and/or infective endocarditis, should suggest a diagnosis of SD. Blood cultures (for both aerobic and anaerobic bacteria) should always be performed in patients with suspected SD; in patients with epidemiological risk factors for brucellosis, specific serological tests for Brucella should also be performed. In the case of suspected TB infection, a PPD test and an interferon-γ release assay should be performed. Evaluation of the morphology and/or functionality of the region of interest is mandatory if the presence of infection is suspected with clinical evaluation of the patient; the same evaluation is recommended for the monitoring of treatment and follow-up of the disease. The imaging technique of choice in suspected spinal infection of haematogenous origin is MRI in patients without contraindications. MRI must be performed with T1, T2, and T2 fat-suppressed or STIR sequences without and with contrast medium with T1 fat suppression technique. MRI must be performed with at least a 1.5 Tesla magnet.
In patients with inconclusive MRI results or in the presence of contraindications to MRI, [18F]FDG-PET/CT is recommended. A negative MRI can rule out the presence of infective pathology in the spine, while in the case of inconclusive results or suspicion of post-surgical spinal infection, PET/CT with [18F]FDG is suggested. 99mTc-MDP and 67Ga-citrate scintigraphy can be performed if [18F]FDG-PET/CT imaging is not available. An image-guided aspiration biopsy should be performed in all patients with suspected SD based on clinical, laboratory, and imaging studies. Antibiotic therapy should be discontinued before biopsy; however, the optimal duration of antibiotic-free time before image-guided biopsy has not been established.
A negative [18F]FDG-PET/CT can rule out the presence of infective pathology of the spine, while with an inconclusive result a CT image-guided bone biopsy should be performed. Bone biopsy should eventually be repeated if the first biopsy finding is negative. Some experts recommend performing an open biopsy when the image-guided biopsy is inconclusive.
Evidence-based diagnostic flow chart
Based on the above statements and evidence from the published literature, we have developed a diagnostic flow chart, shown in Fig. 1.
In some cases the flow was integrated by consensus opinion amongst the experts, since not all steps are always clearly deducible from the literature. The flow chart does not take into consideration socioeconomic factors or the availability of diagnostic methods. It also presumes that all exams are performed at their best (possibly following procedural guidelines published by each society) and by expert professionals [199].
References
Calderone RR, Larsen JM. Overview and classification of spinal infection. Orthop Clin North Am. 1996;27:1–8.
Lazzeri E. Nuclear medicine imaging of vertebral infections: role of radiolabelled biotin. 2009.
Gouliouris T, Aliyu SH, Brown NM. Spondylodiscitis: update on diagnosis and management. J Antimicrob Chemother. 2010;65(Suppl 3):iii11–24.
Carragee EJ. Pyogenic vertebral osteomyelitis. J Bone Joint Surg Am. 1997;79:874–80.
Torda AJ, Gottlieb T, Bradbury R. Pyogenic vertebral osteomyelitis: analysis of 20 cases and review. Clin Infect Dis. 1995;20:320–8.
Pigrau C, Almirante B, Flores X, et al. Spontaneous pyogenic vertebral osteomyelitis and endocarditis: incidence, risk factors, and outcome. Am J Med. 2005;118(11):1287.
Sapico FL, Montgomerie JZ. Pyogenic vertebral osteomyelitis: report of nine cases and review of the literature. Rev Infect Dis. 1979;1:754–76.
Lew DP, Waldvogel FA. Current concepts: osteomyelitis. N Engl J Med. 1997;336:999–1007.
Mandell GL, Bennett JE, Dolin R, eds. Principles and Practice of Infectious Diseases. Vol. 1. Churchill Livingstone, 2000: 1182–1196.
Weissman S, Parker RD, Siddiqui W, et al. Vertebral osteomyelitis: retrospective review of 11 years of experience. Scand J Infect Dis. 2014;46(3):193–9.
Fantoni M, Trecarichi EM, Rossi B, et al. Epidemiological and clinical features of pyogenic spondylodiscitis. Eur Rev Med Pharmacol Sci. 2012;16(Suppl 2):2–7.
Cheung WY, Luk KD. Pyogenic spondylitis. Int Orthop. 2012;36(2):397–404.
Duarte RM, Vaccaro AR. Spinal infection: state of the art and management algorithm. Eur Spine J. 2013;22(12):2787–99.
Honan M, White GW, Eisenberg GM. Spontaneous infectious discitis in adults. Am J Med. 1996;100:85–9.
Chen HC, Tzaan WC, Lui TN. Spinal epidural abscesses: a retrospective analysis of clinical manifestations, sources of infection, and outcomes. Chang Gung Med J. 2004;27(5):351–8.
Patzakis MJ, Rao S, Wilkins J, et al. Analysis of 61 cases of vertebral osteomyelitis. Clin Orthop. 1991:264, 178–183.
Hadjipavlou AG, Mader JT, Necessary JT, Muffoletto AJ. Hematogenous pyogenic spinal infections and their surgical management. Spine. 2000;25(13):1668–79.
Legrand E, Flipo RM, Guggenbuhl P, et al. Management of nontuberculous infectious discitis. Treatments used in 110 patients admitted to 12 teaching hospitals in France. Joint Bone Spine. 2001;68:504–9.
Turunc T, Demiroglu YZ, Uncu H, et al. A comparative analysis of tuberculous, brucellar and pyogenic spontaneous spondylodiscitis patients. J Inf Secur. 2007;55:158–63.
Euba G, Narvaez JA, Nolla JM, et al. Long-term clinical and radiological magnetic resonance imaging outcome of abscess-associated spontaneous pyogenic vertebral osteomyelitis under conservative management. Semin Arthritis Rheum. 2008;38:28–40.
Colmenero JD, Jimenez-Mejias ME, Sanchez-Lora FJ, et al. Pyogenic, tuberculous, and brucellar vertebral osteomyelitis: a descriptive and comparative study of 219 cases. Ann Rheum Dis. 1997;56:709–15.
McHenry MC, Easley KA, Locker GA. Vertebral osteomyelitis: long-term outcome for 253 patients from 7 Cleveland-area hospitals. Clin Infect Dis. 2002;34:1342–50.
Perronne C, Saba J, Behloul Z, et al. Pyogenic and tuberculous spondylodiskitis (vertebral osteomyelitis) in 80 adult patients. Clin Infect Dis. 1994;19:746–50.
Hershkovitz I, Donoghue HD, Minnikin DE, et al. Detection and molecular characterization of 9000-year-old mycobacterium tuberculosis from a Neolithic settlement in the eastern Mediterranean. PLoS One. 2008;3(10):e3426.
Perry M. Erythrocyte sedimentation rate and C reactive protein in the assessment of suspected bone infection – are they reliable indices? J R Coll Surg Edinb. 1996;41:116–8.
Yoon HJ, Song YG, Park WI, et al. Clinical manifestations and diagnosis of extrapulmonary tuberculosis. Yonsei Med J. 2004;45:453–61.
Trecarichi EM, Di Meco E, Mazzotta V, et al. Tuberculous spondylodiscitis: epidemiology, clinical features, treatment, and outcome. Eur Rev Med Pharmacol Sci. 2012;16(Suppl 2):58–72.
Ozuna RM, Delamarter RB. Pyogenic vertebral osteomyelitis and postsurgical disc space infections. Orthop Clin North Am. 1996;27:87–94.
Brown EM, Pople IK, de Louvois J, et al. Spine update: prevention of postoperative infection in patients undergoing spinal surgery. Spine. 2004;29:938–45.
Fang A, Hu SS, Endres N, et al. Risk factors for infection after spinal surgery. Spine. 2005;30:1460–5.
Richards BR, Emara KM. Delayed infections after posterior TSRH spinal instrumentation for idiopathic scoliosis: revisited. Spine. 2001;26:1990–6.
Levi AD, Dickman CA, Sonntag VK. Management of postoperative infections after spinal instrumentation. J Neurosurg. 1997;86:975–80.
Wimmer C, Gluch H. Franzreb M, et al. Predisposing factors for infection in spine surgery: a survey of 850 spinal procedures. J Spinal Disord. 1998;11:124–8.
Massie JB, Heller JG, Abitbol JJ, et al. Postoperative posterior spinal wound infections. Clin Orthop Relat Res. 1992;(284):99–108.
Mylona E, Samarkos M, Kakalou E, et al. Pyogenic vertebral osteomyelitis: a systematic review of clinical characteristics. Semin Arthritis Rheum. 2009;39:10–7.
Berbari EF, Kanj SS, Kowalski TJ, et al. 2015 Infectious Diseases Society of America (IDSA) clinical practice guidelines for the diagnosis and treatment of native vertebral osteomyelitis in adults. Clin Infect Dis. 2015;61(6):e26–46. https://doi.org/10.1093/cid/civ482.
Jutte P, Lazzeri E, Sconfienza LM, et al. Diagnostic flowcharts in osteomyelitis, spondylodiscitis and prosthetic joint infection Q. J Nucl Med Mol Imaging. 2014;58(1):2–19.
Oxford Centre for Evidence-based Medicine. www.cebm.net/finding-the-evidence-1-using-pico-to-formulate-a-search-question. website. 2016. Ref Type: Electronic Citation.
Felix SC, Mitchell JK. Diagnostic yield of CT-guided percutaneous aspiration procedures in suspected spontaneous infectious diskitis. Radiology. 2001;218:211–4.
Tyrell PN, Cassar-Pullicino VN, McCall IW. Spinal infection. Eur Radiol. 1999;9:1066–77.
Tali ET. Spinal infections. Eur J Radiol. 2004;50(2):120–33.
Gasbarrini AL, Bertoldi E, Mazzetti M, et al. Clinical features, diagnostic and therapeutic approaches to haematogenous vertebral osteomyelitis. Eur Rev Med Pharmacol Sci. 2005;9(1):53–66.
Jevtic V. Vertebral infection. Eur Radiol. 2004;14(Suppl 3):E43–52.
Khoo LA, Heron C, Patel U, et al. The diagnostic contribution of the frontal lumbar spine radiograph in community referred low back pain-a prospective study of 1030 patients. Clin Radiol. 2003;58(8):606–9.
Leone A, Dell'Atti C, Magarelli N, et al. Imaging of spondylodiscitis. Eur Rev Med Pharmacol Sci. 2012;16(Suppl 2):8–19.
Graham TS. The ivory vertebra sign. Radiology. 2005;235:614–5.
DeSanto J, Ross JS. Spine infection/inflammation. Radiol Clin N Am. 2011;49(1):105–27.
Tin BJ, Cassar-Pullicino VN. MR imaging of spinal infection. Semin Musculoskelet Radiol. 2004;8(3):215–29.
Grane P, Josephsson A, Seferlis A, et al. Septic and aseptic post-operative discitis in the lumbar spine: evaluation by MR imaging. Acta Radiol. 1998;39:108–15.
Kawakyu-O'Connor D, Bordia R, Nicola R. Magnetic resonance imaging of spinal emergencies. Magn Reson Imaging Clin N Am. 2016;24(2):325–44.
Tins BJ, Cassar-Pullicino VN, Lalam RK. Magnetic resonance of spinal infection. Top Magn Reson Imaging. 2007;18(3):213–22.
Danchaivijitr N, Temram S, Thepmongkhol K, et al. Diagnostic accuracy of MR imaging in tuberculous spondylitis. J Med Assoc Thail. 2007;90(8):1581–9.
Hong SH, Choi JY, Lee JW, et al. MR imaging assessment of the spine: infection or an imitation? Radiographics. 2009;29(2):599–612.
Cottle L, Riordan T. Infectious spondylodiscitis. J Inf Secur. 2008;56(6):401–12.
Kowalski TJ, Layton KF, Berbari EF, et al. Follow-up MR imaging in patients with pyogenic spine infections: lack of correlation with clinical features. Am J Neuroradiol. 2007;28(4):693–9.
Rauf F, Chaudhry UR, Atif M, et al. Spinal tuberculosis: our experience and a review of imaging methods. Neuroradiol J. 2015;28(5):498–503.
Go JL, Rothman S, Prosper A, et al. Spine infections. Neuroimaging Clin N Am. 2012;22(4):755–72.
Yang SC, Fu TS, Chen LH, et al. Identifying pathogens of spondylodiscitis: percutaneous endoscopy or CT-guided biopsy. Clin Orthop Relat Res. 2008;466(12):3086–92.
Brenac F, Huet H. Diagnostic accuracy of the percutaneous spinal biopsy. Optimization of the technique. J Neuroradiol. 2001;28(1):7–16.
Di Martino A, Papapietro N, Lanotte A, et al. Spondylodiscitis: standards of current treatment. Curr Med Res Opin. 2012;28(5):689–99.
Diehn FE. Imaging of spine infection. Radiol Clin N Am. 2012;50(4):777–98.
Sans N, Faruch M, Lapègue F, et al. Infections of the spinal column--spondylodiscitis. Diagn Interv Imaging. 2012;93(6):520–9.
Dufour V, Feydy A, Rillardon L, et al. Comparative study of postoperative and spontaneous pyogenic spondylodiscitis. Semin Arthritis Rheum. 2005;34:766–71.
Enoch DA, Cargill JS, Laing R, et al. Value of CT-guided biopsy in the diagnosis of septic discitis. J Clin Pathol. 2008;61:750–3.
Sehn JK, Gilula LA. Percutaneous needle biopsy in diagnosis and identification of causative organisms in cases of suspected vertebral osteomyelitis. Eur J Radiol. 2012;81:940–6.
Gasbarrini A, Boriani L, Salvadori C, et al. Biopsy for suspected spondylodiscitis. Eur Rev Med Pharmacol Sci. 2012;16(Suppl 2):26–34.
Chaudhary SB, Vives MJ, Basra SK, et al. Postoperative spinal wound infections and postprocedural diskitis. J Spinal Cord Med. 2007;30(5):441–51.
SPILF. [Primary infectious spondylitis, and following intradiscal procedure, without prosthesis. Short text]. Med Mal Infect. 2007;37(9):554–72.
Cebrián Parra JL, Saez-Arenillas Martín A, Urda Martínez-Aedo AL, et al. Management of infectious discitis. Outcome in one hundred and eight patients in a university hospital. Int Orthop. 2012;36(2):239–44.
Palestro CJ, Torres MA. Radionuclide imaging in orthopaedic infections. Semin Nucl Med. 1997;27:334–45.
Palestro CJ, Kim CK, Swyer AJ, et al. Radionuclide diagnosis of vertebral osteomyelitis: indium-111-leukocyte and technetium-99m-methylene diphosphonate bone scintigraphy. J Nucl Med. 1991;32:1861–5.
Devillers A, Moisan A, Jean S, et al. Technetium-99m hexamethyl-propylene amine oxime leucocyte scintigraphy for the diagnosis of bone and joint infections: a retrospective study in 116 patients. Eur J Nucl Med. 1995;22:302–7.
Coleman RE, Welch D. Possible pitfalls with clinical imaging of indium-111 leukocytes. J Nucl Med. 1980;21:122–5.
Fernandex-Ulloa M, Vasavada PJ, Hanslits ML, et al. Diagnosis of vertebral osteomyelitis: clinical, radiological and scintigraphic features. Orthopedics. 1985;8:1144–50.
Datz FL, Thorne DA. Cause and significance of cold bone defects on indium-111-labelled leukocyte imaging. J Nucl Med. 1987;28:820–3.
Whalen JL, Brown ML, McLeod R, et al. Limitations of indium leukocyte imaging for the diagnosis of spine infections. Spine. 1991;16:193–7.
Jacobson AF, Gilles CP, Cerqueira MD. Photopenic defects in marrow-containing skeleton on indium-111 leucocyte scintigraphy: prevalence at sites suspected of osteomyelitis and as an incidental finding. Eur J Nucl Med. 1992;19:858–64.
Prandini N, Lazzeri E, Rossi B, et al. Nuclear medicine imaging of bone infections. Nucl Med Commun. 2006;27:633–44.
Concia E, Prandini N, Massari L, et al. Osteomyelitis: clinical update for practical guidelines. Nucl Med Commun. 2006;27(8):645–60.
Love C, Palestro CJ. Nuclear medicine imaging of bone infections. Clin Radiol. 2016;71:632–46.
Gratz S, Dorner J, Oestmann JW, et al. 67Ga-citrate and 99mTc-MDP for estimating the severity of vertebral osteomyelitis. Nucl Med Commun. 2000;21:111–20.
Fuster D, Solà O, Soriano A, et al. A prospective study comparing whole-body FDG PET/CT to combined planar bone scan with 67Ga SPECT/CT in the diagnosis of spondylodiskitis. Clin Nucl Med. 2012;37:827–32.
Pauwels EKJ, Ribeiro MJ, Stoot JHMB, et al. FDG accumulation and tumor biology. Nucl Med Biol. 1998;25:317–22.
Kubota R, Yamada S, Kubota K, et al. Intratumoral distribution of fluorine-18-fluorodeoxyglucose in vivo: high accumulation in macrophages and granulation tissues studied by microautoradiography. J Nucl Med. 1992;33:1972–80.
Yamada S, Kubota K, Kubota R, et al. High accumulation of fluorine-18-fluorodeoxyglucose in turpentine-induced inflammatory tissue. J Nucl Med. 36:1301–6.
Kaim AH, Weber B, Kurrer MO, et al. Autoradiographic quantification of 18F-FDG uptake in experimental soft-tissue abscesses in rats. Radiology. 2002;223:446–51.
Rosen RS, Fayad L, Wahl RL. Increased 18F-FDG uptake in degenerative disease of the spine: characterization with 18F-FDG PET/CT. J Nucl Med. 2006;47:1274–80.
S O, Suzuki M, Koshi T, et al. 18F-fluorodeoxyglucose-PET for patients with suspected spondylitis showing Modic change. Spine. 2010;35(26):E1599–603.
Stumpe KD, Zanetti M, Weishaupt D, et al. FDG positron emission tomography for differentiation of degenerative and infectious endplate abnormalities in the lumbar spine detected on MR imaging. Am J Roentgenol. 2002;179:1151–7.
Kim SJ, Kim IJ, Suh KT, et al. Prediction of residual disease of spine infection using F-18 FDG PET/CT. Spine. 2009;34(22):2424–30.
Hungenbach S, Delank KS, Dietlein M, et al. 18-F fluorodeoxyglucose uptake pattern in patients with suspected spondylodiscitis. Nucl Med Commun. 2013;34:1068–74.
Nanni C, Boriani L, Salvadori C, et al. FDG PET/CT is useful for the interim evaluation of response to therapy in patients affected by haematogenous spondylodiscitis. Eur J Nucl Med Mol Imaging. 2012;39:1538–44.
Ito K, Kubota K, Morooka M, et al. Clinical impact of (18)F-FDG PET/CT on the management and diagnosis of infectious spondylitis. Nucl Med Commun. 2010;31(8):691–8.
Riccio SA, Chu AK, Rabin HR, et al. Fluorodeoxyglucose positron emission tomography/computed tomography interpretation criteria for assessment of antibiotic treatment response in pyogenic spine infection. Can Assoc Radiol J. 2015;66(2):145–52.
Lee In S, Lee JS, Kim SJ, et al. Fluorine-18-fluorodeoxyglucose positron emission tomography/computed tomography imaging in pyogenic and tuberculous spondylitis: preliminary study. J Comput Assist Tomogr. 2009;33:587–92.
Stumpe KD, Dazzi H, Schaffner A, et al. Infection imaging using whole-body FDG-PET. Eur J Nucl Med. 2000;27:822–32.
Kalicke T, Schmitz A, Risse JH, et al. Fluorine-18 fluorodeoxyglucose PET in infectious bone diseases: results of histologically confirmed cases. Eur J Nucl Med. 2000;27:524–8.
Schmitz A, Kalicke T, Willkomm P, et al. Use of fluorine-18 fluoro-2-deoxy-D-glucose positron emission tomography in assessing the process of tuberculous spondylitis. J Spinal Disord. 2000;13:541–4.
Gratz S, Dorner J, Fischer U, et al. 18F-FDG hybrid PET in patients with suspected spondylitis. Eur J Nucl Med. 2002;29:516–24.
Zhuang H, Alavi A. 18-Fluorodeoxyglucose positron emission tomographic imaging in the detection and monitoring of infection and inflammation. Semin Nucl Med. 2002;32:47–59.
De Winter F, Gemmel F, Van De Wiele C, et al. 18-fluorine fluorodeoxyglucose positron emission tomography for the diagnosis of infection in the postoperative spine. Spine. 2003;28:1314–9.
Mazzie JP, Brooks MK, Gnerre J. Imaging and management of postoperative spine infection. Neuroimaging Clin N Am. 2014;24(2):365–74.
Seifen T, Rettenbacher L, Thaler C, et al. Prolonged back pain attributed to suspected spondylodiscitis. The value of 18F-FDG PET/CT imaging in the diagnostic work-up of patients. Nuklearmedizin. 2012;51:194–200.
Georgakopoulos A, Pneumaticos SG, Sipsas NV, et al. Positron emission tomography in spinal infections. Clin Imaging. 2015;39(4):553–8.
Ioannou S, Chatziioannou S, Pneumaticos SG, et al. Fluorine-18 fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography scan contributes to the diagnosis and management of brucellar spondylodiskitis. BMC Infect Dis. 2013;7:13–73.
Bagrosky BM, Hayes KL, Koo PJ, et al. 18F-FDG PET/CT evaluation of children and young adults with suspected spinal fusion hardware infection. Pediatr Radiol. 2013;43(8):991–1000.
Dureja S, Sen IB, Acharya S. Potential role of F18 FDG PET-CT as an imaging biomarker for the noninvasive evaluation in uncomplicated skeletal tuberculosis: a prospective clinical observational study. Eur Spine J. 2014;23(11):2449–54.
Inanami H, Oshima Y, Iwahori T, et al. Role of 18F-fluoro-D-deoxyglucose PET/CT in diagnosing surgical site infection after spine surgery with instrumentation. Spine. 2015;40:109–13.
Dauchy FA, Dutertre A, Lawson-Ayayi S, et al. Interest of [(18)F]fluorodeoxyglucose positron emission tomography/computed tomography for the diagnosis of relapse in patients with spinal infection: a prospective study. Clin Microbiol Infect. 2016;22(5):438–43.
Fuster D, Tomas X, Mayoral M, et al. Prospective comparison of whole-body 18F-FDG PET/CT and MRI of the spine in the diagnosis of haematogenous spondylodiskitis. Eur J Nucl Med Mol Imaging. 2015;42:264–71.
Skanjeti A, Penna D, Douroukas A, et al. PET in the clinical work-up of patients with spondylodiscitis: a new tool for the clinician? Q J Nucl Med Mol Imaging. 2012;56(6):569–76.
Sonmezoglu K, Sonmezoglu M, Halac M, et al. Usefulness of 99mTc-ciprofloxacin (Infecton) scan in diagnosis of chronic orthopedic infections: comparative study with 99mTc-HMPAO leukocyte scintigraphy. J Nucl Med. 2001;42:567–74.
Lazzeri E, Erba P, Perri M, et al. Scintigraphic imaging of vertebral osteomyelitis with 111In-biotin. Spine. 2008;33(7):E198–204. https://doi.org/10.1097/BRS.0b013e31816960c9.
Lazzeri E, Erba P, Perri M, et al. Clinical impact of SPECT/CT with In-111 biotin on the management of patients with suspected spine infection. Clin Nucl Med. 2010;35:12–7.
Gemmel F, Rijk PC, Collins JMP, et al. Expanding role of 18F-fluoro-d-deoxyglucose PET and PET/CT in spinal infections. Eur Spine J. 2010;19(4):540–51.
Kim CJ, Kang SJ, Yoon D, et al. Factors influencing culture positivity in pyogenic vertebral osteomyelitis patients with prior antibiotic exposure. Antimicrob Agents Chemother. 2015;59(4):2470–3.
Zarrouk V, Feydy A, Sallès F, et al. Imaging does not predict the clinical outcome of bacterial vertebral osteomyelitis. Rheumatology (Oxford). 2007;46(2):292–5.
Torrie PA, Leonidou A, Harding IJ, et al. Admission inflammatory markers and isolation of a causative organism in patients with spontaneous spinal infection. Ann R Coll Surg Engl. 2013;95(8):604–8.
Bhavan KP, Marschall J, Olsen MA, et al. The epidemiology of hematogenous vertebral osteomyelitis: a cohort study in a tertiary care hospital. BMC Infect Dis. 2010;10:158.
Loibl M, Stoyanov L, Doenitz C, et al. Outcome-related co-factors in 105 cases of vertebral osteomyelitis in a tertiary care hospital. Infection. 2014;42(3):503–10.
D'Agostino C, Scorzolini L, Massetti AP, et al. A seven-year prospective study on spondylodiscitis: epidemiological and microbiological features. Infection. 2010;38(2):102–7.
Mete B, Kurt C, Yilmaz MH, et al. Vertebral osteomyelitis: eight years' experience of 100 cases. Rheumatol Int. 2012;32(11):3591–7. https://doi.org/10.1007/s00296-011-2233-z.
Horasan ES, Colak M, Ersöz G, et al. Clinical findings of vertebral osteomyelitis: Brucella spp. versus other etiologic agents. Rheumatol Int. 2012;32(11):3449–53.
Bettini N, Girardo M, Dema E, et al. Evaluation of conservative treatment of non specific spondylodiscitis. Eur Spine J. 2009;18(Suppl 1):143–50.
Kaya S, Ercan S, Kaya S, et al. Spondylodiscitis: evaluation of patients in a tertiary hospital. J Infect Dev Ctries. 2014;8(10):1272–6.
Moromizato T, Harano K, Oyakawa M, et al. Diagnostic performance of pyogenic vertebral osteomyelitis. Intern Med. 2007;46(1):11–6.
Hamdan TA. Postoperative disc space infection after discectomy: a report on thirty-five patients. Int Orthop. 2012;36(2):445–50.
Ziu M, Dengler B, Cordell D, et al. Diagnosis and management of primary pyogenic spinal infections in intravenous recreational drug users. Neurosurg Focus. 2014;37(2):E3.
Hassoun A, Taur Y, Singer C. Evaluation of thin needle aspiration biopsy in the diagnosis and management of vertebral osteomyelitis (VO). Int J Infect Dis. 2006;10(6):486–7.
Eren Gök S, Kaptanoğlu E, Celikbaş A, et al. Vertebral osteomyelitis: clinical features and diagnosis. Clin Microbiol Infect. 2014;20(10):1055–60.
Park KH, Cho OH, Jung M, et al. Clinical characteristics and outcomes of hematogenous vertebral osteomyelitis caused by gram-negative bacteria. J Inf Secur. 2014;69(1):42–50.
Luzzati R, Giacomazzi D, Danzi MC, et al. Diagnosis, management and outcome of clinically- suspected spinal infection. J Inf Secur. 2009;58(4):259–65.
Lora-Tamayo J, Euba G, Narváez JA, et al. Changing trends in the epidemiology of pyogenic vertebral osteomyelitis: the impact of cases with no microbiologic diagnosis. Semin Arthritis Rheum. 2011;41(2):247–55.
Koslow M, Kuperstein R, Eshed I, et al. The unique clinical features and outcome of infectious endocarditis and vertebral osteomyelitis co-infection. Am J Med. 2014;127(7):669.e9–669.e15.
Urrutia J, Campos M, Zamora T, et al. Does pathogen identification influence the clinical outcomes in patients with pyogenic spinal infections? J Spinal Disord Tech. 2015;28(7):E417–21.
Kim CJ, Song KH, Jeon JH, et al. A comparative study of pyogenic and tuberculous spondylodiscitis. Spine. 2010;35:E1096–100.
Kang SJ, Jang HC, Jung SI, et al. Clinical characteristics and risk factors of pyogenic spondylitis caused by gram-negative bacteria. PLoS One. 2015;10(5).
Aagaard T, Roed C, Dragsted C, et al. Microbiological and therapeutic challenges in infectious spondylodiscitis: a cohort study of 100 cases, 2006-2011. Scand J Infect Dis. 2013;45(6):417–24.
Fransen BL, de Visser E, Lenting A, et al. Recommendations for diagnosis and treatment of spondylodiscitis. Neth J Med. 2014;72(3):135–8.
Siemionow K, Steinmetz M, Bell G, et al. Identifying serious causes of back pain: cancer, infection, fracture. Cleve Clin J Med. 2008;75:557–66.
Fuursted K, Arpi M, Lindblad BE, et al. Broad-range PCR as a supplement to culture for detection of bacterial pathogens in patients with a clinically diagnosed spinal infection. Scand J Infect Dis. 2008;40(10):772–7.
Jensen AG, Espersen F, Skinhoj P, et al. Bacteremic Staphylococcus aureus spondylitis. Arch Intern Med. 1998;158:509–17.
Pigrau C, Rodríguez-Pardo D, Fernández-Hidalgo N, et al. Health care associated hematogenous pyogenic vertebral osteomyelitis: a severe and potentially preventable infectious disease. Medicine (Baltimore). 2015;94(3):e365.
Corrah TW, Enoch DA, Aliyu SH, et al. Bacteraemia and subsequent vertebral osteomyelitis: a retrospective review of 125 patients. QJM. 2011;104(3):201–7.
Kim J, Kim YS, Peck KR, et al. Outcome of culture-negative pyogenic vertebral osteomyelitis: comparison with microbiologically confirmed pyogenic vertebral osteomyelitis. Semin Arthritis Rheum. 2014;44:246–52.
Wang Z, Lenehan B, Itshayek E, et al. Primary pyogenic infection of the spine in intravenous drug users: a prospective observational study. Spine. 2012;37(8):685–92.
Lee A, Mirrett S, Reller LB, et al. Detection of bloodstream infections in adults: how many blood cultures are needed? J Clin Microbiol. 2007;45:3546–8.
Colmenero JD, Ruiz-Mesa JD, Plata A, Bermúdez P, Martín-Rico P, Queipo-Ortuño MI, et al. Clinical findings, therapeutic approach, and outcome of brucellar vertebral osteomyelitis. Clin Infect Dis. 2008;46(3):426–33.
Araj GF, Kattar MM, Fattouh LG, et al. Evaluation of the PANBIO Brucella immunoglobulin G (IgG) and IgM enzyme-linked immunosorbent assays for diagnosis of human brucellosis. Clin Diagn Lab Immunol. 2005;12:1334–5.
Koubaa M, Maaloul I, Marrakchi C, et al. Spinal brucellosis in south of Tunisia: review of 32 cases. Spine J. 2014;14(8):1538–44.
Bozgeyik Z, Ozdemir H, Demirdag K, et al. Clinical and MRI findings of brucellar spondylodiscitis. Eur J Radiol. 2008;67(1):153–8.
Su SH, Tsai WC, Lin CY, et al. Clinical features and outcomes of spinal tuberculosis in southern Taiwan. J Microbiol Immunol Infect. 2010;43(4):291–300.
Mulleman D, Mammou S, Griffoul I, et al. Characteristics of patients with spinal tuberculosis in a French teaching hospital. Joint Bone Spine. 2006;73(4):424–7.
Menzies D, Pai M, Comstock G. Meta-analysis: new tests for the diagnosis of latent tuberculosis infection: areas of uncertainty and recommendations for research. Ann Intern Med. 2007;146:340–54.
Wu X, Ma Y, Li D, et al. Diagnostic value of ELISPOT technique for osteoarticular tuberculosis. Clin Lab. 2014;60(11):1865–70.
Cho OH, Park SJ, Park KH, et al. Diagnostic usefulness of a T-cell-based assay for osteoarticular tuberculosis. J Inf Secur. 2010;61(3):228–34.
Yuan K, Wu X, Zhang Q, et al. Enzyme-linked immunospot assay response to recombinant CFP-10/ESAT-6 fusion protein among patients with spinal tuberculosis: implications for diagnosis and monitoring of surgical therapy. Int J Infect Dis. 2013;17(9):e733–8.
Yuan K, Zhong ZM, Zhang Q, et al. Evaluation of an enzyme-linked immunospot assay for the immunodiagnosis of atypical spinal tuberculosis (atypical clinical presentation/atypical radiographic presentation) in China. Braz J Infect Dis. 2013;17(5):529–37.
An HS, Seldomridge A. Spinal infections. Diagnostic tests and imaging studies. Clin Orthop Relat Res. 2006;444:27–33.
Modic MT, Feiglin DH, Piraino DW, et al. Vertebral osteomyelitis: assessment using MR. Radiology. 1985;157:157–66.
Nakahara M, Ito M, Hattori N, et al. 18F-FDG-PET/CT better localizes active spinal infection than MRI for successful minimally invasive surgery. Acta Radiol. 2015;56(7):829–36.
Ledbetter LN, Salzman KL, Shah LM. Imaging psoas sign in lumbar spinal infections: evaluation of diagnostic accuracy and comparison with established imaging characteristics. Am J Neuroradiol. 2016;37(4):736–41.
Garg V, Kosmas C, Young PC, et al. Computed tomography-guided percutaneous biopsy for vertebral osteomyelitis: a department's experience. Neurosurg Focus. 2014;37(2):E10.
Raininko RK, Aho AJ, Laine MO. Computed tomography in spondylitis. CT versus other radiographic methods. Acta Orthop Scand. 1985;56:372–7.
Che W, Li RY, Dong J. Progress in diagnosis and treatment of cervical postoperative infection. Orthop Surg. 2011;3(3):152–7.
Treglia G, Focacci C, Caldarella C, et al. The role of nuclear medicine in the diagnosis of spondylodiscitis. Eur Rev Med Pharmacol Sci. 2012;16(Suppl 2):20–5.
Chahoud J, Kanafani Z, Kanj SS. Surgical site infections following spine surgery: eliminating the controversies in the diagnosis. Front Med (Lausanne). 2014;7(1). https://doi.org/10.3389/fmed.2014.00007.
Palestro CJ. Radionuclide imaging of osteomyelitis. Semin Nucl Med. 2015;45:32–46.
Gemmel F, Dumarey N, Palestro CJ. Radionuclide imaging of spinal infections. Eur J Nucl Med Mol Imaging. 2006;33:1226–37.
Guerado E, Cerván AM. Surgical treatment of spondylodiscitis. An update. Int Orthop. 2012;36:413–20.
Pupaibool J, Vasoo S, Erwin PJ, et al. The utility of image-guided percutaneous needle aspiration biopsy for the diagnosis of spontaneous vertebral osteomyelitis: a systematic review and meta-analysis. Spine J. 2015;15(1):122–31.
Fahnert J, Purz S, Javers J-S, et al. Use of simultaneous FDG-PET/MRI for the detection of spondylodiskitis. J Nucl Med. 2016;57:1396–401.
Sehn JK. Gilula LA. Percutaneous needle biopsy in diagnosis and identification of causative organisms in cases of suspected vertebral osteomyelitis. Eur J Radio. 2012;81(1):940–6.
Mohanty SP, Bhat S, Nair NS. An analysis of clinicoradiological and histopathological correlation in tuberculosis of spine. J Indian Med Assoc. 2011;109(3):161–5.
Kornblum MB, Wesolowski DP, Fischgrund JS, et al. Computed tomography-guided biopsy of the spine. A review of 103 patients. Spine. 1998;23:81–5.
Babu NV, Titus VT, Chittaranjan S, et al. Computed tomographically guided biopsy of the spine. Spine. 1994;19:2436–42.
Peh W. CT-guided percutaneous biopsy of spinal lesions. Biomed Imaging Interv J. 2006;2:e25.
Yoon YK, Jo YM, Kwon HH, et al. Differential diagnosis between tuberculous spondylodiscitis and pyogenic spontaneous spondylodiscitis: a multicenter descriptive and comparative study. Spine J. 2015;15(8):1764–71.
Gras G, Buzele R, Parienti JJ, et al. Microbiological diagnosis of vertebral osteomyelitis: relevance of second percutaneous biopsy following initial negative biopsy and limited yield of post-biopsy blood cultures. Eur J Clin Microbiol Infect Dis. 2014;33(3):371–5.
de Lucas EM, González Mandly A, Gutiérrez A, et al. CT-guided fine-needle aspiration in vertebral osteomyelitis: true usefulness of a common practice. Clin Rheumatol. 2009;28:315–20.
Watt JP, Davis JH. Percutaneous core needle biopsies: the yield in spinal tuberculosis. S Afr Med J. 2013;104(1):29–32.
Berk RH, Yazici M, Atabey N, et al. Detection of mycobacterium tuberculosis in formaldehyde solution-fixed, paraffin-embedded tissue by polymerase chain reaction in Pott’s disease. Spine. 1996;21:1991–5.
Choi SH, Sung H, Kim SH, et al. Usefulness of a direct 16S rRNA gene PCR assay of percutaneous biopsies or aspirates for etiological diagnosis of vertebral osteomyelitis. Diagn Microbiol Infect Dis. 2014;78(1):75–8.
Fenollar F, Roux V, Stein A, et al. Analysis of 525 samples to determine the usefulness of PCR amplification and sequencing of the 16S rRNA gene for diagnosis of bone and joint infections. J Clin Microbiol. 2006;44:1018–28.
Levy PY, Fournier PE, Fenollar F, et al. Systematic PCR detection in culture-negative osteoarticular infections. Am J Med. 2013;126(12):1143.e25–33.
Al Dahouk S, Tomaso H, Nöckler K, et al. The detection of Brucella spp. using PCR-ELISA and real-time PCR assays. Clin Lab. 2004;50(7–8):387–94.
Navarro-Martinez A, Navarro E, Castano MJ, et al. Rapid diagnosis of human brucellosis by quantitative real-time PCR: a case report of brucellar spondylitis. J Clin Microbiol. 2008;46:385–7.
Lucio E, Adesokan A, Hadjipavlou AG, et al. Pyogenic spondylodiskitis: a radiologic/pathologic and culture correlation study. Arch Pathol Lab Med. 2000;124:712–6.
Chen SCA, Halliday CL, Meyer W. A review of nucleic acid-based diagnostic tests for systemic mycoses with an emphasis on polymerase chain reaction-based assays. Med Mycol. 2002;40:333–57.
Chang CY, Simeone FJ, Nelson SB, et al. Is biopsying the paravertebral soft tissue as effective as biopsying the disk or vertebral endplate? 10-year retrospective review of CT-guided biopsy of diskitis-osteomyelitis. Am J Roentgenol. 2015;205(1):123–9.
Heyer CM, Brus LJ, Peters SA, et al. Efficacy of CT-guided biopsies of the spine in patients with spondylitis—an analysis of 164 procedures. Eur J Radiol. 2012;81(3):e244–9.
Marschall J, Bhavan KP, Olsen MA, et al. The impact of prebiopsy antibiotics on pathogen recovery in hematogenous vertebral osteomyelitis. Clin Infect Dis. 2011;52(7):867–72.
Agarwal V, Wo S, Lagemann GM, et al. Image-guided percutaneous disc sampling: impact of antecedent antibiotics on yield. Clin Radiol. 2016;71:228–34.
Friedman JA, Maher CO, Quast LM, et al. Spontaneous disc space infections in adults. Surg Neurol. 2002;57(2):81–6.
Haaker RG, Senkal M, Kielich T, et al. Percutaneous lumbar discectomy in the treatment of lumbar discitis. Eur Spine J. 1997;6:98–101.
Ito M, Abumi K, Kotani Y, et al. Clinical outcome of posterolateral endoscopic surgery for pyogenic spondylodiscitis: results of 15 patients with serious comorbid conditions. Spine. 2007;32:200–6.
Jimenez-Mejias ME, de Dios Colmenero J, Sanchez-Lora FJ, et al. Postoperative spondylodiskitis: etiology, clinical findings, prognosis, and comparison with nonoperative pyogenic spondylodiskitis. Clin Infect Dis. 1999;29:339–45.
Niccoli Asabella A, Iuele F, Simone F, et al. Role of (18)F-FDG PET/CT in the evaluation of response to antibiotic therapy in patients affected by infectious spondylodiscitis. Hell J Nucl Med. 2015;18(Suppl 1):17–22.
Signore A, Jamar F, Israel O, et al. Clinical indications, image acquisition and data interpretation for white blood cells and anti-granulocyte monoclonal antibody scintigraphy: an EANM procedural guideline. Eur J Nucl Med Mol Imaging. 2018;45:1816–31.
Acknowledgements
We wish to thank the many people who contributed to this consensus document through active work on the document or simply by contributing with useful discussion. First of all, we thank the members of the previous EANM Committee on Infection and Inflammation (John Buscombe, Riddhika Chakravarrty, Paola Erba, Ora Israel, Francois Jamar, and Josè Martin-Comin) and the ESNR and ESCMID boards for supporting this work and disseminating our results in international congresses.
Each practice guideline, representing a strategic statement, has undergone a thorough consensus process as a result of an extensive review.
This document was brought to the attention of all other EANM committees and the European national societies of nuclear medicine. The comments and suggestions from the Oncology Committee and Physics Committee and from the Czech, Russian, German, Italian, Latvian and Belgian national societies are highly appreciated and have been considered for this consensus document.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure statements
The European Association of Nuclear Medicine (EANM), founded in 1985, is a professional nonprofit medical association that facilitates communication worldwide between individuals pursuing clinical and research excellence in nuclear medicine.
The European Society of Neuroradiology (ESNR), founded in 1977, is a professional society of European neuroradiologists and a leader in education and training, with courses including the brain, spine, and diagnostic neuroradiology, as well as a forum for professional development of European neuroradiology.
The European Society of Clinical Microbiology and Infectious Diseases (ESCMID), founded in 1983, is an influential component in the professional lives of microbiologists and infectious disease specialists around the world. ESCMID facilitates the advance of scientific knowledge and the dissemination of professional guidelines and consensus documents in the field of clinical microbiology and infectious diseases.
EANM, ESNR, and ESCMID members are physicians, biologists, technologists, and scientists specialising in the research and practice of nuclear medicine, neuroradiology, and infectious diseases, respectively.
This consensus paper, representing a policy statement by the EANM/ESNR (with ESCMID endorsement), has undergone a thorough consensus process in which an extensive review was performed. The EANM, ESNR, and ESCMID recognise that the safe and effective use of diagnostic imaging requires specific training, skills, and techniques, as described in the introduction section. Reproduction or modification of the published paper is not authorised.
They report what ideally should be done based on evidence from the literature. However, these recommendations should be carefully adapted to local practice, where not all diagnostic tests or imaging modalities may be available. Resources available to care for patients, as well as legislation and local regulations, may vary greatly from one European country to another.
The recommendations contained herein are intended as an educational tool to assist practitioners in providing appropriate care for patients. They are not inflexible rules or requirements of practice and are not intended, nor should they be used, to establish a legal standard of care. For these reasons and those set forth below, the EANM, ESNR, and ESCMID caution against the use of these recommendations in litigation in which the clinical decisions of a practitioner are called into question.
The ultimate judgement regarding the propriety of any specific procedure or course of action must be made by the physician or medical physicist in light of all the circumstances presented. A conscientious practitioner may responsibly adopt a course of action different from that set forth in this document when such course of action is indicated by the condition of the patient, limitations of available resources, or advances in knowledge or technology subsequent to publication of these recommendations.
The practice of medicine includes the prevention, diagnosis, alleviation, and treatment of disease. The variety and complexity of human conditions make it impossible to always reach the most appropriate diagnosis or to predict with certainty a particular response to treatment. Therefore, it should be recognised that adherence to these guidelines will not ensure an accurate diagnosis or a successful outcome. All that should be expected is that the practitioner will follow a reasonable course of action based on current knowledge (evidence-based medicine), available resources, and the needs of the patient to deliver effective and safe medical care. The sole purpose of this document is, therefore, to assist practitioners in achieving this objective.
The EANM and ESNR (with ESCMID endorsement) will periodically define new guidelines for the diagnosis of spine infection in adults to improve the quality of service to patients throughout the world. Existing diagnostic guidelines will be reviewed for revision or renewal, as appropriate, on their fifth anniversary or sooner, if indicated.
Conflict of interest
Elena Lazzeri is a senior advisor of the EANM Committee on Inflammation and Infection. She has nothing to declare.
Alessandro Bozzao has nothing to declare.
Maria Adriana Cataldo has nothing to declare.
Nicola Petrosillo has nothing to declare.
Luigi Manfrè has nothing to declare.
Andrej Trampuz has nothing to declare.
Alberto Signore is a senior advisor of the EANM Committee on Inflammation and Infection. He has nothing to declare.
Mario Muto has nothing to declare.
Ethical approval
This consensus document does not contain any studies with human participants or animals performed by any of the authors. The human studies described herein have been published previously.
Informed consent
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Oncology – Brain.
Appendix
Appendix
Consensus statements
-
1)
SD should be suspected in patients with new or worsening spine pain and/or new myelo-radicular symptoms, and at least one of the following: fever, elevated ESR or CRP, bloodstream infection, or infective endocarditis.
All papers found: 2289.
Included papers for thorough reading: 183.
Included papers evidence-based statement: 28.
-
2)
CRP, ESR, and WBC counts should always be performed in patients with suspected SD.
P: spine infection OR spinal infection OR vertebral infection OR vertebral osteomyelitis OR post-surgical spine infection OR spondylodiscitis OR discitis OR infectious spondylitis.
I: diagnostic methods.
C: none.
O: diagnosis.
All papers found: 2289.
Included papers for thorough reading: 183.
Included papers evidence-based statement: 28.
-
3)
Blood cultures (for both aerobic and anaerobic bacteria) should always be performed in patients with suspected SD.
P: spine infection OR spinal infection OR vertebral infection OR vertebral osteomyelitis OR post-surgical spine infection OR spondylodiscitis OR discitis OR infectious spondylitis.
I: diagnostic methods.
C: none.
O: diagnosis.
All papers found: 2289.
Included papers for thorough reading: 183.
Included papers evidence-based statement: 30.
-
4)
For patients with suspected SD and epidemiological risk factors for brucellosis, specific serological tests should be performed.
P: spine infection OR spinal infection OR vertebral infection OR vertebral osteomyelitis OR post-surgical spine infection OR spondylodiscitis OR discitis OR infectious spondylitis.
I: diagnostic methods.
C: none.
O: diagnosis.
All papers found: 2289.
Included papers for thorough reading: 183.
Included papers evidence-based statement: 6.
-
5)
For patients with suspected SD and risk factors for Mycobacterium tuberculosis , a PPD test and an interferon-γ release assay should be performed.
P: spine infection OR spinal infection OR vertebral infection OR vertebral osteomyelitis OR post-surgical spine infection OR spondylodiscitis OR discitis OR infectious spondylitis.
I: diagnostic methods.
C: none.
O: diagnosis.
All papers found: 2289.
Included papers for thorough reading: 183.
Included papers evidence-based statement: 8.
-
6)
Plain film X-ray should always be performed in patients with suspicion of spine infection for purposes of differential diagnostic and follow-up.
P: spine infection OR spinal infection OR vertebral infection OR vertebral osteomyelitis OR post-surgical spine infection OR spondylodiscitis OR discitis OR infectious spondylitis = 9683.
I: radiography OR x-ray OR radiographic diagnosis OR digital radiography OR plain radiography = 497487.
C: none.
O: early diagnosis = 150145.
All papers found: 200.
Included papers for thorough reading: 6.
Included papers evidence-based statement: 6.
-
7)
In haematogenous SD, the first diagnostic imaging modality is MRI, if patients have no specific contraindications.
P: spine infection OR spinal infection OR vertebral infection OR vertebral osteomyelitis OR post-surgical spine infection OR spondylodiscitis OR discitis OR infectious spondylitis = 9683.
I: magnetic resonance OR MR OR MRI = 392979.
C: none.
O: diagnosis of spine infection OR diagnosis of vertebral osteomyelitis OR diagnosis of vertebral infection OR diagnosis of soft tissue infection OR diagnosis of paravertebral soft tissue infection = 5623.
All papers found: 1545.
Included papers for thorough reading: 6.
Included papers evidence-based statement: 5.
-
8)
MRI must be performed with T1, T2, and T2 fat-suppressed or STIR sequences without and with contrast medium with T1 fat suppression technique.
P: spine infection OR spinal infection OR vertebral infection OR vertebral osteomyelitis OR post-surgical spine infection OR spondylodiscitis OR discitis OR infectious spondylitis = 9683.
I: MRI must be performed with T1, T2, and T2 fat-suppressed or STIR sequences without and with contrast medium with T1 fat-suppressed technique = 25.
C: none.
O: diagnosis of spine infection OR diagnosis of vertebral osteomyelitis OR diagnosis of vertebral infection OR diagnosis of soft tissue infection OR diagnosis of paravertebral soft tissue infection = 5623.
All papers found: 8.
Included papers for thorough reading: 8.
Included papers evidence-based statement: 8.
-
9)
MRI in suspected spine infection should be performed with at least a 1.5 Tesla magnet.
P: spine infection OR spinal infection OR vertebral infection OR vertebral osteomyelitis OR post-surgical spine infection OR spondylodiscitis OR discitis OR infectious spondylitis = 9683.
I: MRI must be performed with a 1.5 Tesla magnet = none.
C: none.
O: diagnosis of spine infection OR diagnosis of vertebral osteomyelitis OR diagnosis of vertebral infection OR diagnosis of soft tissue infection OR diagnosis of paravertebral soft tissue infection = 5623.
All papers found: 4.
Included papers for thorough reading: 4.
Included papers evidence-based statement: 4.
-
10)
CT may be useful for diagnosis only when MRI is contraindicated, not available, or equivocal.
P: spine infection OR spinal infection OR vertebral infection OR vertebral osteomyelitis OR post-surgical spine infection OR spondylodiscitis OR discitis OR infectious spondylitis = 9683.
I: CT OR computed tomography OR CeT = 324788.
C: none.
O: diagnosis of spine infection OR diagnosis of vertebral osteomyelitis OR diagnosis of vertebral infection OR diagnosis of soft tissue infection OR diagnosis of paravertebral soft tissue infection = 5623.
All papers found: 5.
Included papers for thorough reading: 5.
Included papers evidence-based statement: 5.
-
11)
In primary and post-surgical SD, if MRI is contraindicated, the imaging modality of choice is [ 18 F]FDG-PET/CT.
P: spine infection OR spinal infection OR vertebral infection OR vertebral osteomyelitis OR post-surgical spine infection OR spondylodiscitis OR discitis OR infectious spondylitis = 9683.
Contraindications to MRI = 120 (none on SD).
I: PET OR PET/CT OR FDG-PET OR fluorodeoxyglucose OR FDG OR positron emission tomography = 62923.
C: none.
O: diagnosis of spine infection OR diagnosis of vertebral osteomyelitis OR diagnosis of vertebral infection OR diagnosis of soft tissue infection OR diagnosis of paravertebral soft tissue infection = 5377.
All papers found: 94.
Included papers for thorough reading: 30.
Included papers evidence-based statement: 24.
-
12)
In post-surgical SD, with or without spinal hardware, [ 18 F]FDG-PET/CT can detect both spine infection and soft tissue infection.
P: post-surgical spine infection OR post-surgical vertebral infection OR post-surgical vertebral osteomyelitis OR post-surgical spine OR post-surgical spondylodiscitis OR spinal hardware = 9683.
I: FDG-PET OR PET OR fluorodeoxyglucose OR FDG OR positron emission tomography OR PET/CT = 62923.
C: none.
O: diagnosis of spine infection OR diagnosis of vertebral osteomyelitis OR diagnosis of vertebral infection OR diagnosis of soft tissue infection OR diagnosis of paravertebral soft tissue infection = 5377.
All papers found: 2.
Included papers for thorough reading: 12.
Included papers evidence-based statement: 10.
-
13)
In patients with suspected spine infection and elevated ESR and/or CRP and doubtful MRI, [ 18 F]FDG-PET/CT should be performed.
P: inconclusive MR OR doubtful MR OR not diagnostic MR OR inconclusive MRI OR doubtful MRI OR no diagnostic MRI = 23502.
P: spine infection and elevated ESR and/or CRP = 23299.
I: FDG-PET OR PET OR fluorodeoxyglucose OR FDG OR positron emission tomography OR PET/CT = 62923.
C: none.
O: diagnosis of spine infection OR diagnosis of vertebral osteomyelitis OR diagnosis of vertebral infection OR diagnosis of soft tissue infection OR diagnosis of paravertebral soft tissue infection = 5377.
All papers found: 18.
Included papers for thorough reading: 18.
Included papers evidence-based statement: 17.
-
14)
In patients with suspected spine infection, elevated ESR and/or CRP, doubtful or unperformable MRI, and doubtful or unperformable [ 18 F]FDG-PET/CT, a CT scan should be performed with an image-guided biopsy.
P: spine infection OR spinal infection OR vertebral infection OR vertebral osteomyelitis OR post-surgical spine infection OR spondylodiscitis OR discitis OR infectious spondylitis = 9683.
I: Inconclusive FDG-PET OR PET OR inconclusive fluorodeoxyglucose OR inconclusive FDG OR inconclusive positron emission tomography OR inconclusive PET/CT OR doubtful FDG-PET OR doubtful PET/CT =47758.
C: none.
O: CT-guided vertebral biopsy OR vertebral biopsy = 23943.
All papers found: 30.
Included papers for thorough reading: 7.
Included papers evidence-based statement: 7.
-
15)
The role of hybrid PET/MRI, although promising, needs to be evaluated.
P: spine infection OR spinal infection OR vertebral infection OR vertebral osteomyelitis OR post-surgical spine infection OR spondylodiscitis OR discitis OR infectious spondylitis = 9683.
I: PET/MRI OR PET/MR OR hybrid PET/MRI OR hybrid PET/MR = 949.
C: none.
O: diagnosis of spine infection OR diagnosis of vertebral osteomyelitis OR diagnosis of vertebral infection OR diagnosis of soft tissue infection OR diagnosis of paravertebral soft tissue infection = 5377.
All papers found: none.
Included papers for thorough reading: none.
Included papers evidence-based statement: none.
-
16)
In case of negative MRI or negative [ 18 F]FDG-PET/CT, the diagnosis of SD should be excluded.
P: spine infection OR spinal infection OR vertebral infection OR vertebral osteomyelitis OR post-surgical spine infection OR spondylodiscitis OR discitis OR infectious spondylitis = 9683.
I: negative FDG-PET OR negative PET OR negative fluorodeoxyglucose OR negative FDG OR negative positron emission tomography OR negative PET/CT = 5800.
negative MR OR negative MRI OR negative magnetic resonance = 18549.
C: none.
O: absence of spine infection OR absence of vertebral infection OR absence of spondylodiscitis = 131.
All papers found: 5.
Included papers for thorough reading: 3.
Included papers evidence-based statement: 3.
-
17)
An image-guided aspiration biopsy should be performed in all patients with suspected SD based on clinical, laboratory, and imaging studies.
P: spine infection OR spinal infection OR vertebral infection OR vertebral osteomyelitis OR post-surgical spine infection OR spondylodiscitis OR discitis OR infectious spondylitis.
I: diagnostic methods.
C: none.
O: diagnosis.
All papers found: 2289.
Included papers for thorough reading: 183.
Included papers evidence-based statement: 28.
-
18)
Antibiotic therapy should be discontinued or postponed before biopsy.
P: spine infection OR spinal infection OR vertebral infection OR vertebral osteomyelitis OR post-surgical spine infection OR spondylodiscitis OR discitis OR infectious spondylitis.
I: diagnostic methods.
C: none.
O: diagnosis.
All papers found: 2289.
Included papers for thorough reading: 183.
Included papers evidence-based statement: 9.
-
19)
In patients with suspected SD based on clinical, laboratory, and imaging studies and a negative biopsy (histology and microbiology), another biopsy should be done.
P: spine infection OR spinal infection OR vertebral infection OR vertebral osteomyelitis OR post-surgical spine infection OR spondylodiscitis OR discitis OR infectious spondylitis.
I: diagnostic methods.
C: none.
O: diagnosis.
All papers found: 2289.
Included papers for thorough reading: 183.
Included papers evidence-based statement: 11.
-
20)
In patients with SD diagnosed by [ 18 F]FDG-PET/CT, a second [ 18 F]FDG-PET/CT scan should be performed to evaluate the response to antibiotic therapy.
P: spine infection OR spinal infection OR vertebral infection OR vertebral osteomyelitis OR post-surgical spine infection OR spondylodiscitis OR discitis OR infectious spondylitis = 9683.
I: FDG-PET OR PET OR fluorodeoxyglucose OR FDG OR positron emission tomography OR PET/CT = 62923.
C: none.
O: response to therapy OR treatment response OR antibiotic response = 416536.
All papers found: 19.
Included papers for thorough reading: 9.
Included papers evidence-based statement: 8.
Statements 1, 2, 3, 4, 5, 6, 18, 19, 20 (ESCMID)
(((“spine”[MeSH Terms] OR “spine”[All Fields] OR “vertebral”[All Fields]) AND (“osteomyelitis”[MeSH Terms] OR “osteomyelitis”[All Fields])) OR (spinal[All Fields] AND (“osteomyelitis”[MeSH Terms] OR “osteomyelitis”[All Fields])) OR (“discitis”[MeSH Terms] OR “discitis”[All Fields] OR “spondylodiscitis”[All Fields]) OR (“discitis”[MeSH Terms] OR “discitis”[All Fields] OR “spondylodiskitis”[All Fields]) OR (“discitis”[MeSH Terms] OR “discitis”[All Fields] OR “diskitis”[All Fields]) OR (“discitis”[MeSH Terms] OR “discitis”[All Fields]) OR (infectious[All Fields] AND (“spondylitis”[MeSH Terms] OR “spondylitis”[All Fields])) OR (septic[All Fields] AND (“spondylitis”[MeSH Terms] OR “spondylitis”[All Fields])) OR (spinal[All Fields] AND (“infection”[MeSH Terms] OR “infection”[All Fields])) OR (spinal[All Fields] AND (“infection”[MeSH Terms] OR “infection”[All Fields] OR “infections”[All Fields])) OR ((“spine”[MeSH Terms] OR “spine”[All Fields]) AND (“infection”[MeSH Terms] OR “infection”[All Fields])) OR ((“spine”[MeSH Terms] OR “spine”[All Fields]) AND (“infection”[MeSH Terms] OR “infection”[All Fields] OR “infections”[All Fields])) OR ((“spine”[MeSH Terms] OR “spine”[All Fields] OR “vertebral”[All Fields]) AND (“infection”[MeSH Terms] OR “infection”[All Fields])) OR ((“spine”[MeSH Terms] OR “spine”[All Fields] OR “vertebral”[All Fields]) AND (“infection”[MeSH Terms] OR “infection”[All Fields] OR “infections”[All Fields])) OR (disk[All Fields] AND space[All Fields] AND (“infection”[MeSH Terms] OR “infection”[All Fields])) OR (disk[All Fields] AND space[All Fields] AND (“infection”[MeSH Terms] OR “infection”[All Fields] OR “infections”[All Fields])) OR (disc[All Fields] AND space[All Fields] AND (“infection”[MeSH Terms] OR “infection”[All Fields])) OR (disc[All Fields] AND space[All Fields] AND (“infection”[MeSH Terms] OR “infection”[All Fields] OR “infections”[All Fields]))) AND ((“diagnosis”[Subheading] OR “diagnosis”[All Fields] OR “diagnosis”[MeSH Terms]) OR (“diagnosis”[MeSH Terms] OR “diagnosis”[All Fields] OR “diagnostic”[All Fields])) AND ((“2006/01/01”[PDAT]: “2015/12/31”[PDAT]) AND “humans”[MeSH Terms] AND English[lang] AND “adult”[MeSH Terms]) NOT (“case reports”[Publication Type] OR “case reports”[All Fields])
All papers found: 2289. Included papers for thorough reading: 183. Included papers evidence-based statement: 61.
Rights and permissions
About this article

Cite this article
Lazzeri, E., Bozzao, A., Cataldo, M.A. et al. Joint EANM/ESNR and ESCMID-endorsed consensus document for the diagnosis of spine infection (spondylodiscitis) in adults. Eur J Nucl Med Mol Imaging 46, 2464–2487 (2019). https://doi.org/10.1007/s00259-019-04393-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-019-04393-6