
Abstract
Background:
The aim of this paper was to enlarge the available knowledge on clinical and etiological aspects of patients affected by spondylodiscitis.
Patients and Methods:
All patients with spondylodiscitis admitted between January 2001 and December 2007 at the 1,300-bed University Hospital "Policlinico Umberto I" of Rome, Italy, were followed. Demographic characteristics, underlying diseases, invasive procedures, imaging studies, isolated microorganisms, treatment, complications, and outcome were recorded.
Results:
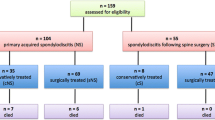
Eighty-one patients of mean age 57.7 ± 14.7 years with lumbosacral (72.8%), thoracic (14.8%), and cervical tract (12.3%) site of infection were included, of which 38 developed communityacquired (CA) spondylodiscitis and 43 developed hospital-acquired (HA) spondylodiscitis. Underlying disease was present in 49.4% of patients. HA spondylodiscitis was diagnosed earlier (46.8 ± 49.7 days) than CA spondylodiscitis (65.0 ± 55.4 days) (P < 0.05). The most frequently isolated microorganisms were Staphylococcus aureus (28 strains, 43.1%), coagulase-negative staphylococci (CNS) (eight strains, 12.3%), Pseudomonas aeruginosa (eight strains, 12.3%), and three methicillin-resistant S. aureus (MRSA) strains were isolated in CA spondylodiscitis. Fungi and yeasts, isolated in six patients, represented 9.2% of all strains but 17.6% when considering only HA spondylodiscitis. Over 85% of patients were managed by conservative treatment alone, and the treatment time depended on clinical and laboratory evidence. Poor outcome was recorded in 12 (14.8%) patients, and was associated with neurological deficit symptoms (relative risk [RR] 2.87; 95% confidence interval [CI] 1.02–8.07; P < 0.05) and the time between diagnosis and the onset of symptoms ≥ 60 days (RR 2.65; 95% CI 0.92–7.59; P < 0.05).
Conclusions:
Infectious spondylodiscitis affects most frequently the elderly population, who are more exposed to healthcare contacts. Consequently, the infection etiology includes a growing proportion of multi-resistant bacteria and fungi.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Acosta FL Jr, Chin CT, Quiñones H, Ames CP, Weinstein PR, Chou D: Diagnosis and management of adult pyogenic osteomyelitis of the cervical spine. Neurosurg Focus 2004; 17: E2.
Butler JS, Shelly MJ, Timlin M, Powderly WG, O’Byrne JM: Nontuberculous pyogenic spinal infection in adults: a 12-year experience from a tertiary referral center. Spine 2006; 31: 2695–2700.
Acosta FL Jr, Galvez LF, Aryan HE, Ames CP: Recent advances: infections of the spine. Curr Infect Dis Rep 2006; 8: 390–393.
Cottle L, Riordan T: Infectious spondylodiscitis. J Infect 2008; 56: 401–412.
O’Daly BJ, Morris SF, O’Rourke SK: Long-term functional outcome in pyogenic spinal infection. Spine 2008; 33: E246–E253.
McHenry MC, Easley KA, Locker GA: Vertebral osteomyelitis: long-term outcome for 253 patients from 7 Cleveland-area hospitals. Clin Infect Dis 2002; 34: 1342–1350.
Solis Garcia del Pozo J, Vives Soto M, Solera J: Vertebral osteomyelitis: long-term disability assessment and prognostic factors. J Infect 2007; 54: 129–134.
Bettini N, Girardo M, Dema E, Cervellati S: Evaluation of conservative treatment of non specific spondylodiscitis. Eur Spine J 2009; 18: 143–150.
Carragee EJ: Pyogenic vertebral osteomyelitis. J Bone Joint Surg Am 1997; 79: 874–880.
Hadjipavlou AG, Mader JT, Necessary JT, Muffoletto AJ: Hematogenous pyogenic spinal infections and their surgical management. Spine 2000; 25: 1668–1679.
Karadimas EJ, Bunger C, Lindblad BE, Hansen ES, Høy K, Helmig P, Kannerup AS, Niedermann B: Spondylodiscitis. A retrospective study of 163 patients. Acta Orthop 2008; 79: 650–659.
Kowalski TJ, Berbari EF, Huddleston PM, Steckelberg JM, Osmon DR: Do follow-up imaging examinations provide useful prognostic information in patients with spine infection?. Clin Infect Dis 2006; 43: 172–179.
Luzzati R, Giacomazzi D, Danzi MC, Tacconi L, Concia E, Vento S: Diagnosis, management and outcome of clinically-suspected spinal infection. J Infect 2009; 58: 259–265.
Roblot F, Besnier JM, Juhel L, Vidal C, Ragot S, Bastides F, Le Moal G, Godet C, Mulleman D, Azaïs I, Becq-Giraudon B, Choutet P: Optimal duration of antibiotic therapy in vertebral osteomyelitis. Semin Arthritis Rheum 2007; 36: 269–277.
Kowalski TJ, Layton KF, Berbari EF, Steckelberg JM, Huddleston PM, Wald JT, Osmon DR: Follow-up MR imaging in patients with pyogenic spine infections: lack of correlation with clinical features. Am J Neuroradiol 2007; 28: 693–699.
Govender S: Spinal infections. J Bone Joint Surg Br 2005; 87: 1454–1458.
Jiménez-Mejías ME, de Dios Colmenero J, Sánchez-Lora FJ, Palomino-Nicás J, Reguera JM, García de la Heras J, García-Ordoñez MA, Pachón J: Postoperative spondylodiskitis: etiology, clinical findings, prognosis, and comparison with nonoperative pyogenic spondylodiskitis. Clin Infect Dis 1999; 29: 339–345.
Friedman ND, Kaye KS, Stout JE, McGarry SA, Trivette SL, Briggs JP, Lamm W, Clark C, MacFarquhar J, Walton AL, Reller LB, Sexton DJ: Healthcare-associated bloodstream infections in adults: a reason to change the accepted definition of community-acquired infections. Ann Intern Med 2002; 137: 791–797.
Venditti M, Falcone M, Corrao S, Licata G, Serra P: Outcomes of patients hospitalized with community-acquired, health careassociated and hospital-acquired pneumonia. Ann Intern Med 2009; 150: 19–26.
Lam KS, Webb JK: Discitis. Hosp Med 2004; 65: 280–286.
Le Moal G, Roblot F, Paccalin M, Sosner P, Burucoa C, Roblot P, Becq-Giraudon B: Clinical and laboratory characteristics of infective endocarditis when associated with spondylodiscitis. Eur J Clin Microbiol Infect Dis 2002; 21: 671–675.
Pigrau C, Almirante B, Flores X, Falco V, Rodríguez D, Gasser I, Villanueva C, Pahissa A: Spontaneous pyogenic vertebral osteomyelitis and endocarditis: incidence, risk factors, and outcome. Am J Med 2005; 118: 1287.e17–1287.e24.
Chia SL, Tan BH, Tan CT, Tan SB: Candida spondylodiscitis and epidural abscess: management with shorter courses of antifungal therapy in combination with surgical debridement. J Infect 2005; 51: 17–23.
Garcia-Vidal C, Cabellos C, Ayats J, Font F, Ferran E, Fernandez-Viladrich P: Fungal postoperative spondylodiscitis due to Scedosporium prolificans. Spine J 2009; 9: e1–e7.
Johnson MD, Perfect JR: Fungal infections of the bones and joints. Curr Infect Dis Rep 2001; 3: 450–460.
Hendrickx L, Van Wijngaerden E, Samson I, Peetermans WE: Candidal vertebral osteomyelitis: report of 6 patients, and a review. Clin Infect Dis 2001; 32: 527–533.
Parry MF, Grant B, Yukna M, Adler-Klein D, McLeod GX, Taddonio R, Rosenstein C: Candida osteomyelitis and diskitis after spinal surgery: an outbreak that implicates artificial nail use. Clin Infect Dis 2001; 32: 352–357.
Grados F, Lescure FX, Senneville E, Flipo RM, Schmit JL, Fardellone P: Suggestions for managing pyogenic (non-tuberculous) discitis in adults. Joint Bone Spine 2007; 74: 133–139.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
D’Agostino, C., Scorzolini, L., Massetti, A.P. et al. A Seven-Year Prospective Study on Spondylodiscitis: Epidemiological and Microbiological Features. Infection 38, 102–107 (2010). https://doi.org/10.1007/s15010-009-9340-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-009-9340-8