
Abstract
Summary
Hip fractures are associated with reduced health-related quality of life (HrQoL). We found pre-existing need of care or limited function, cognitive impairment, and depression to be independent factors associated with lower HrQoL during the postsurgical period. In contrast, joint replacement was associated with better HrQoL compared to internal fixation. Patients’ treatment should be focused on functional recovery and treatment of depression.
Introduction
The aim of the study was to identify independent factors that were correlated with health-related quality of life (HrQoL) after hip fracture.
Methods
A total of 402 patients with a mean age of 81 years suffering from a hip fracture were included in this prospective, observational cohort study. HrQoL (determined by the EuroQol instrument) was measured at admission and at discharge from an acute care hospital. Independent factors correlated with HrQoL at discharge and changes from pre-fracture to discharge were determined using multivariate analyses. The influence of antidepressants was evaluated by an ANOVA with repeated measurements.
Results
Need of care prior to fracture was the most important determinant of EQ-5D index at discharge (ß = −0.359, p = 0.003). Additionally, low Mini Mental Status Examination (MMSE) was associated with a lower EQ-5D index at discharge (MMSE 0–9: ß = −0.238, p <0.001; MMSE 10–19: ß = −0.294, p <0.001) and a greater decrease in EQ-5D during hospitalisation (MMSE 10–19: ß = 0.281, p <0.001), while joint replacement (compared to internal fixation) was associated with a higher EQ-5D index (ß = 0.188, p = 0.002) and a lower decrease in the index (ß = −0.216, p = 0.003). EQ VAS values at discharge were correlated with pre-fracture Barthel Index (ß = 0.253, p <0.001) and Geriatric Depression Scale scores (ß = −0.135, p = 0.026). Depressive patients on antidepressants demonstrated less of a decrease in the EQ-5D index compared to patients not receiving medication (F = 2.907, p = 0.090).
Conclusions
Acute care of hip fracture patients should be focused on functional recovery and treatment of depression. When the preferred surgical strategy is unclear, joint replacement should be considered.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hip fractures are common in elderly people. Most hip fractures occur due to simple falls in patients with advanced osteoporosis [1, 2]. The incidence of these fractures in Germany is up to 439/100,000 per year [3]. In 2008, nearly 140,000 fractures (ICD-10 S.72.0–72.2) were registered in Germany [4]. The incidence of these fractures is expected to rise considerably due to the expected demographic changes in the next decades. Hip fracture injuries are identified as one of the most serious healthcare problems affecting the elderly [5]. Despite recognised treatment algorithms, these fractures still lead to declines in function, high rates of morbidity, and premature death [5–8].
In addition, patient-reported outcomes have been shown to be impaired following hip fractures in a number of studies. Specifically, health-related quality of life (HrQoL) is considerably affected following osteoporotic fractures and hip fractures [9–15]. In a previous study, 3 months after hip fracture, physical function was found to be reduced by 51 % according to the SF-36 [12]. One year after the fracture, nearly all dimensions of the HrQoL, according to the SF-36, were reduced in comparison to controls [9]. Another investigation found that the physical function, role-physical, and social function subscales were still affected 2 years after trauma, with the greatest impact on the role-physical subscale (48.84 vs. 72.64) [10]. Ekström et al. showed decreased HrQoL with respect to the EQ-5D index from 0.69 to 0.59 1 year after trochanteric fracture and from 0.73 to 0.53 [14] 1 year after subtrochanteric fracture [15]. Several factors that impact the long-term HrQoL of hip fracture patients have been identified such as age, fracture type, co-morbidities [13], patients’ function [9], type of surgery [16], postoperative pain [17], fear of falling [18], cognitive impairment, and depression [19].
The SF-36 and the EQ-5D are the most commonly used instruments to evaluate HrQoL [20]. The EQ-5D is a validated instrument used to measure the health status of the elderly [21]. Due to its brevity and simplicity, the EQ-5D seems to be more convenient than the SF-36, particularly when assessing with geriatric patients [22].
There are only limited data on the HrQoL of hip fracture patients during acute care that have been evaluated using the EQ-5D. In previous studies, the EQ-5D was either only applied just after the fracture or small groups of patients were examined [23, 24]. We therefore used the EQ-5D in a large cohort of more than 400 geriatric hip fracture patients at hospital admission and again at discharge from the acute care hospital. The main aim of the study was to evaluate the effect of the fracture on patients’ HrQoL and to identify independent factors related to HrQoL at the end of acute care.
Patients and methods
Patients with proximal femoral fracture (ICD-10 S72.0–72.2 [25]) who were older than 60 years of age and admitted for surgical fracture treatment to our university hospital were included in this prospective observational cohort study. Exclusion criteria were polytrauma (ISS ≥16 [26]) and malignancy-related fractures. The recruitment period was from April 1, 2009 to September 30, 2011.
Institutional review board approval by the ethics committee of the University of Marburg was obtained (AZ 175/08). All patients or their legal representatives provided written informed consent for study participation.
All patients were examined by trained personnel, and the following patient characteristics were collected: as socio-demographic data (e.g., age, gender, residential status), type of fracture, American Society of Anesthesiologists (ASA) score [27], and Charlson comorbidity index (CCI) [28]. The patients’ pre-fracture residential status classified as either home care or nursing home or independent living. Additionally, patient medication (e.g., antidepressants) prior to fracture was documented.
Clinical data
The interval between hospital admission and surgery, as well as the type of surgery (prosthesis or internal fixation), was documented. Occurrence of local complications, such as failure of osteosynthesis, luxation, seroma, hematoma, or wound infections, were recorded as well as systemic complications, such as pneumonia, ischemic heart attack, thrombosis, lung embolism, decubital ulcer, or urinary tract infections. In-hospital mortality and the duration of inpatient treatment in our department were also documented.
Questionnaires
Health status was measured using the EQ-5D instrument [29]. The EQ-5D consists of two parts: a questionnaire and a thermometer-like visual analogue scale (EQ VAS). The questionnaire contains the following five dimensions: mobility, self care, usual activities, pain/discomfort and anxiety/depression; each dimension has three levels of severity (1: no problems; 2: moderate problems; 3: severe problems), resulting in 243 possible health states for the patient. The EQ-5D index was calculated using the lean model of the scoring algorithm for the German population [30]. Patients were asked for a retrospective HrQoL assessment (i.e., before the fracture) at admission and were asked about their current HrQoL at discharge. Patients were also asked to rate their current health status on EQ VAS ranging from 0 (worst imaginable health state) to 100 (best imaginable health state).
The pre-fracture activity level was assessed by the Barthel Index (BI) according to the Hamburger Manual [31]. Depression was evaluated using the short form of the Geriatric Depression Scale (GDS) [32]. Patients with a GDS >4 were classified as at risk for depression to achieve high sensitivity in the depression screening [33]. Cognitive impairment was assessed by the Mini Mental Status Examination (MMSE) [34]. According to the current German guidelines for dementia, results of the MMSE were divided into no cognitive impairment [27–30], mild dementia [20–26], moderate dementia [11–19], and severe dementia (<11) [35].
A Delirium Rating Scale (DRS) score was recorded every day during acute care [36]. Presence of postsurgical delirium was assumed if DRS was >11 on at least 1 day during hospitalisation. The patients’ pain level was measured 1 week after hip fracture surgery by a VAS (0 = no pain at all to 10 = intolerable pain) [37].
Statistics
The data were collected in a Filemaker® database (FileMaker Inc., Santa Clara, CA, USA). Double entry with a plausibility check was performed to monitor for data quality.
Predictive Analysis SoftWare (PASW®) version 18.0 (SPSS Inc., Chicago, IL, USA) was used for explorative data analysis. The data are presented as the mean, standard deviation (SD), median, and range.
Multiple regression analysis was performed for both the HrQoL at discharge and the difference between HrQoL prior to fracture and at discharge.
We used multiple regression analysis to identify independent determinants of HrQoL. Additionally, multiple regression analysis provides information regarding how well the independent factors explain differences in HrQoL and HrQoL changes change during hospitalisation. The variables used in the multiple regression analysis were specified based on data from previous studies. Variables were screened by means of the Spearman rank correlation. Among those variables that were significant in the bivariate analyses, relevant variables were chosen for multiple linear regressions in which the EQ-5D and EQ VAS were dependent variables. In the second analysis with forward selection, all statistically redundant variables were excluded from the hierarchical regression. All assumptions regarding multivariate analyses, including homoscedasticity, linearity, autocorrelation, normally distributed errors, and multicollinearity, were investigated by the appropriate methods. The fraction of variability explained was calculated for each regression model based on the R2 method, as appropriate. Data were presented with standardised regression coefficients (β), non standardised regression coefficients (B), and 95 % confidence intervals of non standardised regression coefficients.
T tests for dependent means were used to compare the EQ-5D index and the EQ VAS at admission and at discharge.
The influence of antidepressants and depression on HrQoL was analysed by a 2 × 2 × 2 analysis of variance (ANOVA) with repeated measurements. This method was chosen to find possible interaction effects between medication and depression on the change in HrQoL during hospitalisation.
Results
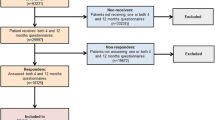
During the investigation period, a total of 539 hip fracture patients were treated in our department. Of the 477 patients who met the inclusion criteria, 75 patients declined to participate; 402 patients were included in the study. Out of 62 (15 %) patients who suffered from severe dementia, 52 patients were unable to answer the EQ-5D. Finally, 350 patients answered the EQ-5D questionnaire at admission (Fig. 1). The patients’ characteristics and parameters of treatment are shown in Table 1. Overall in-hospital mortality was 6.2 % (n = 25). In addition, 52 patients could not or refused to complete the EQ-5D at discharge, resulting in 277 completed EQ-5D questionnaires at discharge.

Flow chart of the study
The average pre-fracture EQ-5D index was 0.71 (95 % CI 0.67–0.74) and the average pre-fracture EQ VAS was 57 (95 % CI 54–59). During the hospitalisation period, the mean EQ-5D index and EQ VAS were reduced to 0.46 (95 % CI 0.41–0.51, p <0.001) and 53 (95 % CI 50–56, p = 0.024), respectively (Table 2).
In the univariate analyses, we found 10 parameters that were significantly correlated with the EQ-5D index at discharge. These parameters included patient age, pre-fracture CCI, pre-fracture residential status, pre-fracture BI, GDS at admission, MMSE at admission, type of surgery, length of stay in the ICU, occurrence of systemic complications, and occurrence of delirium (Table 3). The strongest correlations were found with the pre-fracture residential status (Spearman’s coefficient r = −0.512), pre-fracture BI (r = 0.496), and MMSE at admission (r = 0.470) (Table 3). Six parameters (patient age, pre-fracture residential status, MMSE at admission, type of surgery, length of stay in the ICU, and presence of delirium) were significantly correlated with the difference between the pre-fracture EQ-5D index and the EQ-5D index at discharge (Table 3). The correlations between these parameters and change in the EQ-5D index were the opposite of the correlations of these parameters with the EQ-5D at discharge (Table 3). The correlation coefficients were low compared to the average coefficients between the EQ-5D index and patient characteristics (Table 3). EQ VAS at discharge was most strongly correlated with the pre-fracture Barthel Index (r = 0.279), pre-fracture residential status (r = −0.253), and pre-fracture Charlson Index (r = −0.249). The correlations were also in the opposite direction compared to the correlation of these parameters with the EQ VAS at discharge (Table 3).
In the multiple regression analysis (adjusted R 2 = 0.382), pre-fracture residential status (home care or nursing home; ß = −0.359, p <0.001) and low MMSE (MMSE 0–9: ß = −0.238, p <0.001, MMSE 10–19: ß = −0.294, p <0.001) were significantly associated with a lower EQ-5D index at discharge. In contrast, hip replacement with prosthesis was associated with higher EQ-5D index levels compared to internal fixation (ß = 0.188, p = 0.002) (Table 4). With respect to the difference between pre-fracture and discharge EQ-5D, we identified moderate dementia (MMSE: 10–19; ß = 0.281, p <0.001) and the type of surgery (prosthesis, ß = −0.216, p = 0.003) as independent variables (adjusted R 2 = 0.097, Table 5).
In the multiple regression analysis of the EQ VAS at discharge (adjusted R 2 = 0.093), a greater BI at admission was related to higher EQ VAS (ß = 0.253, p <0.001), while a GDS of more than 4 points was related to lower EQ VAS (ß = −0.135, p = 0.026, Table 6). We found no variables that significantly influenced the differences between pre-fracture and EQ VAS at discharge in the multiple regression analysis.
Thirty-four (8 %) patients were on antidepressants prior to the fracture. HrQoL with respect to antidepressant intake and GDS are given in Table 7. Patients using antidepressants had a lower EQ-5D index (0.40 vs. 0.58; p = 0.011), while patients with a GDS >4 had a lower EQ VAS (50 vs. 61, p = 0.003, Table 7). The ANOVA with repeated measurements showed no influence of antidepressant medication or GDS >4 on the variations in EQ VAS during hospitalisation (F = 0.208, p = 0.649). Regarding the EQ-5D index, patients with GDS ≤4 had a similar decrease in HrQoL during hospitalisation, independent of antidepressant medication use (Fig. 2a); however, we found a lower decrease in the EQ-5D index in depressive patients (GDS >4) using antidepressant medication compared to those not using medication (Fig. 2b; F = 2.907, p = 0.090).

a EQ-5D index in patients with GDS ≤4 with respect to anti-depressive medication. b EQ-5D index in patients with GDS >4 with respect to anti-depressive medication
Discussion
In this study, we aimed to identify independent factors that influence HrQoL at the end of acute care in patients treated for hip fracture. Additionally, we searched for factors that influence the change in HrQoL from pre-fracture to discharge from acute care.
The characteristics of patients included in our study (Table 1) were comparable to those of other studies on patients with geriatric hip fractures with respect to age, gender distribution, fracture type and pre-fracture residential status. Currently, evaluations of HrQoL in hip fracture patients in Germany do not exist. We found a reduced HrQoL before the fracture in comparison to the HrQoL found by König et al. for the advanced elderly [38]. In our study, more than half of the patients reported ‘some problems’ or even ‘extreme problems’ concerning mobility or pain before the fracture. However, it should be noted that patients reported their pre-fracture HrQoL in our hospital at admission after the fracture had occurred, which might pose a bias. The average EQ VAS score was 61 in König et al.’s investigation while the patients in our study scored an average of 57 before the fracture (Table 2). These findings are consistent with Rohde et al.’s findings, which showed reduced quality of life before hip fracture in a controlled study using the Quality of Life Scale and the SF-36. Rohde explained the difference citing more co-morbidities and lower physical function in the hip fracture group [39]. Tidermark et al.’s results for the EQ-5D are comparable to our findings [40], while Miedel et al. found a higher EQ-5D index (0.85) in Swedish patients with subtrochanteric fractures [41]. Tidermark et al.’s results for the EQ-5D are comparable to our findings [43].
The EQ-5D index at discharge did not reach the pre-fracture level in our study. The EQ-5D index decreased from 0.71 to 0.46. The EQ VAS score also diminished but to a lesser degree compared to the EQ-5D index (Table 2). In contrast, Hagino et al. found similar decreases in both measurements but the EQ VAS values were higher in their study (70 points) compared to our results [23]. Unfortunately, EQ VAS values were not given in other studies. The different results in the declines of the EQ-5D index and EQ VAS in our patient sample may be due to the EQ VAS being a single question that is more general than the EQ-5D. In contrast, the different dimensions of the EQ-5D index, such as mobility, self care, and pain, are obviously affected directly by the fracture (Table 2). The results fit well with previous studies. It can be expected that the HrQoL improves during the first year, as measured with the EQ-5D and the Osteoporosis Assessment Questionnaire-Short Version, unless a new fracture occurs [23, 42]. The impact of hip fractures on long-term quality of life determined with the WHO Quality of Life questionnaire appears to be stronger in comparison to the impact of vertebral or distal forearm fractures [11]. Even the long-term results are often associated with reduced quality of life [9–15]. In a previous study, the physical function 3 months after hip fracture was reduced by 51 % according to the SF-36 [12]. One year after the fracture, nearly all dimensions of the HrQoL according to the SF-36 were reduced in comparison to controls [9]. Another investigation found that physical function, role-physical and social function subscales were affected 2 years after trauma, with the greatest impact on the role-physical subscale (48.84 vs. 72.64) [10]. Ekström et al. showed a decrease in HrQoL with respect to the EQ-5D index from 0.69 to 0.59 and from 0.73 to 0.53 1 year after trochanteric fracture [14] and subtrochanteric fracture, respectively [15]. These findings emphasise that hip fractures require a long rehabilitation period and yet complete recovery sometimes cannot be achieved.
We found 10 variables that correlated with the EQ-5D index at discharge in the bivariate analysis, while five variables did not show any correlation. We found similar results for the EQ VAS (Table 3), though we found only six factors that correlated significantly with the EQ VAS. Specifically, in contrast to the EQ-5D index, the type of surgery, presence of delirium or systemic complications and the length of stay in the ICU were not significantly correlated with the EQ VAS. In general, Spearman’s coefficients showing the correlation between the factors and the HrQoL were greater for the EQ-5D index than for the EQ VAS (Table 3). Similar variables were correlated with the decrease in HrQoL from pre-fracture to discharge in HrQoL. These correlations were in the opposite direction from the correlations with HrQoL at discharge for all the significant variables. This result indicates that variables associated with higher HrQoL at discharge were also associated with a lower decrease in HrQoL during hospitalisation, and vice versa (Table 3).
Some parameters such as age, co-morbidities [13], patient function [9], cognitive impairment, and depression [19], have been shown to influence long-term HrQoL. In accordance with others who found better long-term HrQoL after prosthetic surgery in comparison to internal fixation for patients after displaced hip fracture [16, 43, 44], we found that patients who underwent internal fixation had lower EQ-5D index scores at discharge and showed a greater decrease during hospitalisation compared to patients who received prosthesis. In addition, HrQoL was more affected in patients who had a longer stay in the ICU and patients with delirium or other systemic complications. A prolonged stay in the ICU may be a surrogate parameter for complications or poor health status. Interestingly, male gender, which was associated with poorer outcome after hip fracture in a previous study [45], was not associated with lower EQ-5D in our study. This difference could be explained by the results of König et al., who found that elderly women in general reported problems more often in three out of the five dimensions (mobility, usual care and pain/discomfort) according to the EQ-5D [38]. In contrast to Shyu et al., who found poorer HrQoL in patients with more pain during the first year after the fracture [17], we found no significant impact of postoperative pain levels on HrQoL in our analysis. Although early surgery for hip fracture patients is part of current guidelines [46–48], the duration between admission and surgery did not influence the EQ-5D. Additionally, local complications such as hematomas or implant failure had no impact on the EQ-5D. Perhaps patients had coped with these complications at discharge. A history of complications during acute care may seem not as important in the patients’ view, although such complications are of great importance to healthcare providers (e.g., surgical revisions). Duration of stay in the acute care hospital, which is important for economic reasons, had no influence on the EQ-5D (Table 3).
In multiple regression analysis, we found three independent factors that were associated with lower EQ-5D index at discharge, pre-fracture residence in nursing home or home care, cognitive impairment, and hip fracture repair with internal fixation (Table 4). Factors that were independently correlated with lower EQ VAS at discharge were lower pre-fracture BI and pre-existing depression (Table 6). Moderate cognitive impairment (MMSE 10–19) and internal fixation were associated with a greater decrease in the EQ-5D index during hospitalisation as well (Table 5). We found no independent parameters that were associated with the decrease in EQ VAS during hospitalisation.
Because three of the five categories of the EQ-5D are mobility, self care and usual activities, it is expected that residential status is associated with the EQ-5D Index. Therefore, it is not surprising that patients who lived in a nursing home or received home care before the fracture had a lower HrQoL at discharge (Table 4). Correspondingly, our results suggest that patients with limited function prior to fracture according to the BI are at risk for lower HrQoL (according to the EQ VAS) at the end of hospitalisation (Table 6). Nearly half (40 %) of the patients received care or even lived in a nursing home before the fracture occurred. Although detriments to activities and dependency prior to fracture usually cannot be reversed, further deterioration should be prevented. Patients, who were independent before the fracture, should be protected from a loss of independency. Along with state-of-the-art surgery, comprehensive orthogeriatric co-management might be a key to improving patient outcomes following hip fracture. In the authors’ opinion, successful mobilisation—and as a consequence, regain of function—is one of the most important goals in the treatment of hip fracture patients. It is assumed that mobilisation has a preventive effect on the incidence of perioperative complications. In the study by Boonen et al., functional status at discharge was the strongest predictor of functional status 1-year post fracture [9]. The degree of postoperative mobilisation has also been shown to predict 1-year mortality after hip fracture [49]. Even long-term results suggested that mobility and function were more affected by osteoporotic hip fracture than by other osteoporotic fractures [50]. The severity of cognitive impairment was an additional independent factor for lower EQ-5D index at discharge. Interestingly, only moderate cognitive impairment (MMSE 10–19) was an independent factor for HrQoL deterioration. Perhaps patients with at most mild dementia do not differ from patients without cognitive impairment with respect to the postoperative course, while patients with severe cognitive impairment may not be able to estimate their situation as well as the other patients.
According to our results, hip replacement was associated with better HrQoL at discharge according to the EQ-5D index and less deterioration during hospitalisation (Tables 4 and 5). Joint replacement is not considered straightforward for all proximal femoral fractures (e.g., intertrochanteric or subtrochanteric fractures). Additionally, in-hospital mortality is greater after prosthesis in comparison to internal fixation [51]. On the other hand, recent data showed lower reoperation rates and long-term mortality for displaced femoral neck fractures that were treated with prosthesis in comparison to non-displaced femoral neck fractures treated with internal fixation [52]. These results suggest that joint replacement should be considered, when the ideal treatment for the fracture is unclear, because in previous studies prosthetic surgery was associated with better long-term HrQoL [16, 43, 44],
Finally, we identified depression as an independent factor for limited HrQoL at discharge according to the EQ VAS (Table 6). Depression seems to be a common comorbidity in hip fracture patients [19]. We confirmed Feng et al.’s finding that hip fracture patients with depression and cognitive impairment had a lower HrQoL in comparison to hip fracture patients without depression or cognitive impairment [19]. It is assumed that late-life depression is still under-diagnosed and under-treated [53]. While in our cohort, 86 patients had a GDS >4 prior to fracture and only 34 of our patients were receiving antidepressant medication at the same time. Patients on an antidepressant had a lower HrQoL in comparison to patients not on an antidepressant (Table 7), but those who had a GDS >4 at admission showed a greater decrease in the EQ-5D index if they were not receiving antidepressants at admission (Fig 2b). Antidepressant medication was not started in our study patients during hospitalisation. Based on our results, hip fracture patients should be routinely screened for depression at admission with appropriate instruments, and if there are any symptoms of depression, a psychiatrist should be consulted. If indicated, an adequate antidepressant therapy should be initiated.
Our study has several limitations. First, only 84.3 % of the patients who fulfilled the inclusion criteria agreed to participate in the study (15.7 % denied participation (Fig. 1)). Second, the EQ-5D questionnaire was not completed by 52 patients (13 %) at admission (Fig. 1). The main reason the questionnaire was not completed was cognitive impairment, which is a common comorbidity in geriatric hip fracture patients [54]. Unfortunately, in previous studies, demented patients were excluded a priori. In addition, 27 % of our patients were not able or refused to complete the EQ-5D at discharge. In a previous publication by Boonen et al., only 51 % of the patients were able to complete the SF-36 survey [9], and the EQ-5D and SF-36 survey showed good correspondence in hip fracture patients [55]; therefore, in our opinion, the EQ-5D is an adequate instrument to measure health status even in cognitively impaired patients. Third, we assessed the pre-fracture HrQoL retrospectively. Bryant et al. found accurate ratings of preoperative quality of life 2 weeks after knee arthroscopy [56]. Our patients, however, were older and had higher morbidity compared to Bryant et al.’s patients, and the special circumstances at admission might have resulted in a bias. In our opinion, the EQ-5D was an acceptable method to assess patients’ pre-fracture HrQoL.
In summary, the HrQoL in hip fracture patients at the end of acute care following surgery was reduced. We identified several factors that influenced the HrQoL according to the EQ-5D. It should be taken into consideration that there might be a difference between hip fracture patients’ views and healthcare providers’ views concerning the relevance of such factors. Our multivariate model was more valuable for the EQ-5D index than for the EQ VAS. For both measurements, there may be factors that affect HrQoL but were not considered in the present study. To the best of our clinical knowledge, we have included evident variables. Therefore, further investigations are necessary. In conclusion, patients’ pre-admission living in nursing homes or receiving home care, limited function, cognitive impairment and depression as well as surgical hip fracture repair with internal fixation were associated with lower health-related quality of life in the postsurgical period. Therefore, efforts should be made in the acute clinical phase to maintain patients’ independence and regain function and to diagnose and treat dementia and depression adequately. In cases when the ideal hip fracture treatment is unclear, joint replacement should be considered instead of internal fixation.
References
Cooper C, Campion G, Melton LJ (1992) Hip fractures in the elderly: a world-wide projection. Osteoporos Int 2:285–289
Cummings SR, Nevitt MC, Browner WS, Stone K, Fox KM, Ensrud KE, Cauley J, Black D, Vogt TM (1995) Risk factors for hip fracture in white women. Study of Osteoporotic Fractures Research Group. N Engl J Med 332:767–773
Kanis JA, Odén A, McCloskey EV, Johansson H, Wahl DA, Cooper C, IOF Working Group on Epidemiology and Quality of Life (2012) A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos Int 23(9):2239–2256
Federal bureau of statistics. Germany. Hospital statistics. Wiesbaden 2011;https://www.destatis.de/DE/Publikationen/Thematisch/Gesundheit/Krankenhaeuser/DiagnosedatenKrankenhaus2120621097004.pdf?__blob=publicationFile
Marks R (2010) Hip fracture epidemiological trends, outcomes, and risk factors, 1970–2009. Int J Gen Med 3:1–17
Sernbo I, Johnell O (1993) Consequences of a hip fracture: a prospective study over 1 year. Osteoporos Int 3:148–153
Becker C, Gebhard F, Fleischer S, Hack A, Kinzl L, Nikolaus T, Muche R (2003) Prediction of mortality, mobility and admission to long-term care after hip fractures. Unfallchirurg 106:32–38
Leibson CL, Tosteson AN, Gabriel SE, Ransom JE, Melton LJ (2002) Mortality, disability, and nursing home use for persons with and without hip fracture: a population-based study. J Am Geriatr Soc 50:1644–1650
Boonen S, Autier P, Barette M, Vanderschueren D, Lips P, Haentjens P (2004) Functional outcome and quality of life following hip fracture in elderly women: a prospective controlled study. Osteoporos Int 15:87–94
Hallberg I, Rosenqvist AM, Kartous L, Löfman O, Wahlström O, Toss G (2004) Health-related quality of life after osteoporotic fractures. Osteoporos Int 15:834–841
Chiu MH, Hwang HF, Lee HD, Chien DK, Chen CY, Lin MR (2012) Effect of fracture type on health-related quality of life among older women in Taiwan. Arch Phys Med Rehabil 93:512–519
Randell AG, Nguyen TV, Bhalerao N, Silverman SL, Sambrook PN, Eisman JA (2000) Deterioration in quality of life following hip fracture: a prospective study. Osteoporos Int 11:460–466
Rohde G, Haugeberg G, Mengshoel AM, Moum T, Wahl AK (2010) Two-year changes in quality of life in elderly patients with low-energy hip fractures. A case–control study. BMC Musculoskelet Disord 11:226
Ekström W, Miedel R, Ponzer S, Hedström M, Samnegård E, Tidermark J (2009) Quality of life after a stable trochanteric fracture–a prospective cohort study on 148 patients. J Orthop Trauma 23:39–44
Ekström W, Németh G, Samnegård E, Dalen N, Tidermark J (2009) Quality of life after a subtrochanteric fracture: a prospective cohort study on 87 elderly patients. Injury 40:371–376
Gjertsen JE, Vinje T, Lie SA, Engesaeter LB, Havelin LI, Furnes O, Fevang JM (2008) Patient satisfaction, pain, and quality of life 4 months after displaced femoral neck fractures: a comparison of 663 fractures treated with internal fixation and 906 with bipolar hemiarthroplasty reported to the Norwegian Hip Fracture Register. Acta Orthop 79:594–601
Shyu YI, Chen ML, Chen MC, Wu CC, Su JY (2009) Postoperative pain and its impact on quality of life for hip-fractured older people over 12 months after hospital discharge. J Clin Nurs 18:755–764
Iglesias CP, Manca A, Torgerson DJ (2009) The health-related quality of life and cost implications of falls in elderly women. Osteoporos Int 20:869–878
Feng L, Scherer SC, Tan BY, Chan G, Fong NP, Ng TP (2010) Comorbid cognitive impairment and depression is a significant predictor of poor outcomes in hip fracture rehabilitation. Int Psychogeriatr 22:246–253
Hutchings L, Fox R, Chesser T (2011) Proximal femoral fractures in the elderly: how are we measuring outcome? Injury 42:1205–1213
Coast J, Peters TJ, Richards SH, Gunnell DJ (1998) Use of the EuroQoL among elderly acute care patients. Qual Life Res 7:1–10
Brazier JE, Walters SJ, Nicholl JP, Kohler B (1996) Using the SF-36 and Euroqol on an elderly population. Qual Life Res 5:195–204
Hagino H, Nakamura T, Fujiwara S, Oeki M, Okano T, Teshima R (2009) Sequential change in quality of life for patients with incident clinical fractures: a prospective study. Osteoporos Int 20:695–702
Borgström F, Zethraeus N, Johnell O, Lidgren L, Ponzer S, Svensson O, Abdon P, Ornstein E, Lunsjö K, Thorngren KG, Sernbo I, Rehnberg C, Jönsson B (2006) Costs and quality of life associated with osteoporosis-related fractures in Sweden. Osteoporos Int 17:637–650
ICD-10 Version:2010. International Statistical Classification of Diseases and Related Health Problems 10th Revision. Available at: http://apps.who.int/classifications/apps/icd/icd10online/. Accessed 2 May 2012
Baker SP, O’Neill B, Haddon W, Long WB (1974) The injury severity score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma 14:187–196
Anesthesiologists ASo ASA physical status classification system(2010) http://www.asahq.org/clinical/physicalstatus.htm. Accessed 2 May 2012
Charlson ME, Pompei P, Ales KL, MacKenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40:373–383
EQ-5-D;A standardised instrument for use as a measure of health outcome;User Giude; 2009;http://www.euroqol.org/fileadmin/user_upload/Documenten/PDF/User_Guide_v2_March_2009.pdf. Accessed 2 May 2012
Greiner W, Claes C, Busschbach JJ, von der Schulenburg JM (2005) Validating the EQ-5D with time trade off for the German population. Eur J Health Econ 6:124–130
Lübke N, Meinck M, Von Renteln-Kruse W (2004) The Barthel Index in geriatrics. A context analysis for the Hamburg Classification Manual. Z Gerontol Geriatr 37:316–326
Sheikh JI, Yesavage JA (1986) Geriatric Depression Scale (GDS): recent evidence and development of a shorter version. In: Brink TL (ed) Clinical gerontology: a guide to assessment and intervention. Haworth, New York, pp 165–173
Almeida OP, Almeida SA (1999) Short versions of the geriatric depression scale: a study of their validity for the diagnosis of a major depressive episode according to ICD-10 and DSM-IV. Int J Geriatr Psychiatry 14:858–865
Folstein MF, Folstein SE, McHugh PR (1975) “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12:189–198
Arbeitsgemeinschaft Wissenschaftlich Medizinischer Fachgesellschaften (AWMF) (2009) S3-guideline „dementia“, long version. http://www.awmf.de. Accessed 10 July 2012
Trzepacz PT, Baker RW, Greenhouse J (1988) A symptom rating scale for delirium. Psychiatry Res 23:89–97
Bond MR, Pilowsky I (1966) Subjective assessment of pain and its relationship to the administration of analgesics in patients with advanced cancer. J Psychosom Res 10:203–208
König HH, Heider D, Lehnert T, Riedel-Heller SG, Angermeyer MC, Matschinger H, Vilagut G, Bruffaerts R, Haro JM, de Girolamo G, de Graaf R, Kovess V, Alonso J, ESEMeD/MHEDEA 2000 investigators (2010) Health status of the advanced elderly in six European countries: results from a representative survey using EQ-5D and SF-12. Health Qual Life Outcomes 8:143
Rohde G, Haugeberg G, Mengshoel AM, Moum T, Wahl AK (2008) Is global quality of life reduced before fracture in patients with low-energy wrist or hip fracture? A comparison with matched controls. Health Qual Life Outcomes 6:90
Tidermark J, Zethraeus N, Svensson O, Törnkvist H, Ponzer S (2002) Quality of life related to fracture displacement among elderly patients with femoral neck fractures treated with internal fixation. J Orthop Trauma 16:34–38
Miedel R, Törnkvist H, Ponzer S, Söderqvist A, Tidermark J (2011) Musculoskeletal function and quality of life in elderly patients after a subtrochanteric femoral fracture treated with a cephalomedullary nail. J Orthop Trauma 25:208–213
Silverman S, Viswanathan HN, Yang YC, Wang A, Boonen S, Ragi-Eis S, Fardellone P, Gilchrist N, Lips P, Nevitt M, Palacios Gil-Antuñano S, Pavelka K, Revicki D, Simon J, Macarios D, Siris ES (2012) Impact of clinical fractures on health-related quality of life is dependent on time of assessment since fracture: results from the FREEDOM trial. Osteoporos Int 23:1361–1369
Frihagen F, Nordsletten L, Madsen JE (2007) Hemiarthroplasty or internal fixation for intracapsular displaced femoral neck fractures: randomised controlled trial. BMJ 335:1251–1254
Blomfeldt R, Törnkvist H, Ponzer S, Söderqvist A, Tidermark J (2005) Comparison of internal fixation with total hip replacement for displaced femoral neck fractures. Randomized, controlled trial performed at four years. J Bone Joint Surg Am 87:1680–1688
Holt G, Smith R, Duncan K, Hutchison JD, Gregori A (2008) Gender differences in epidemiology and outcome after hip fracture: evidence from the Scottish Hip Fracture Audit. J Bone Joint Surg Br 90:480–483
Network GR Acute care Hip Fracture Clinical Pathway October 2011 http://www.gtarehabnetwork.ca/clinical-care-guidelines-hip-fracture Accessed 25 Dec 2011.
(SIGN) SIGN Management of hip fracture in older people—a national clinical guideline http://www.sign.ac.uk/pdf/sign111.pdf Accessed 25 Dec 2011.
Leitlinie Schenkelhalsfraktur, Deutsche Gesellschaft für Unfallchirurgie, 2008, http://www.awmf.org/uploads/tx_szleitlinien/012-001_S2e_Schenkelhalsfraktur_leitlinientext_05-2008_05-2013.pdf Accessed 14 Jun 2011.
Heinonen M, Karppi P, Huusko T, Kautiainen H, Sulkava R (2004) Post-operative degree of mobilization at two weeks predicts one-year mortality after hip fracture. Aging Clin Exp Res 16:476–480
Papaioannou A, Kennedy CC, Ioannidis G, Sawka A, Hopman WM, Pickard L, Brown JP, Josse RG, Kaiser S, Anastassiades T, Goltzman D, Papadimitropoulos M, Tenenhouse A, Prior JC, Olszynski WP, Adachi JD, Group CS (2009) The impact of incident fractures on health-related quality of life: 5 years of data from the Canadian Multicentre Osteoporosis Study. Osteoporos Int 20:703–714
AQUA – Institut für angewandte Qualitätsförderung und Forschung im Gesundheitswesen. Bundesauswertung zum Erfassungsjahr 2011. 17/1 - Hüftgelenksnahe Femurfraktur. Qualitätsindikatoren. www.aqua-institut.de. Accessed 31 May 2012
Gjertsen JE, Fevang JM, Matre K, Vinje T, Engesæter LB (2011) Clinical outcome after undisplaced femoral neck fractures. Acta Orthop 82:268–274
Wilkins CH, Mathews J, Sheline YI (2009) Late life depression with cognitive impairment: evaluation and treatment. Clin Interv Aging 4:51–57
Yiannopoulou KG, Anastasiou IP, Ganetsos TK, Efthimiopoulos P, Papageorgiou SG (2012) Prevalence of dementia in elderly patients with hip fracture. Hip Int 22:209–213
Tidermark J, Bergström G, Svensson O, Törnkvist H, Ponzer S (2003) Responsiveness of the EuroQol (EQ 5-D) and the SF-36 in elderly patients with displaced femoral neck fractures. Qual Life Res 12:1069–1079
Bryant D, Norman G, Stratford P, Marx RG, Walter SD, Guyatt G (2006) Patients undergoing knee surgery provided accurate ratings of preoperative quality of life and function 2 weeks after surgery. J Clin Epidemiol 59:984–993
Conflicts of interest
Each author certifies that he or she and members, or a member of his/her immediate family, have no commercial associations (e.g., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose as a conflict of interest in connection with the content of the submitted article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Buecking, B., Struewer, J., Waldermann, A. et al. What determines health-related quality of life in hip fracture patients at the end of acute care?—a prospective observational study. Osteoporos Int 25, 475–484 (2014). https://doi.org/10.1007/s00198-013-2415-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-013-2415-5