
Abstract
Summary
Fractures and falls are serious cause of morbidity and cost to society. Our results suggest that the main burden to morbidity, measured as impact on health-related quality of life, is due to fear of falling rather than falls or their sequelae, such as fractures.
Introduction
Fractures and falls are serious cause of morbidity and cost to society. We investigated the impact on health-related quality of life (HRQoL) associated with falls, fractures and fear of falling and falls and fractures cost.
Methods
Three datasets providing longitudinal data on fear of falling, HRQoL and a common set of baseline risk factors for fracture (smoking status, weight and age) were analysed. Multilevel random effects models were used to estimate the long-term impact on HRQoL associated with falls, fractures and fear of falling. Healthcare resource use primary data were collected to estimate falls and fractures cost.
Results
Older, low weight and smoking women reported lower HRQoL. The impact on HRQoL of a fracture was at least twice as large as that associated with falls. The largest negative effect on HRQoL was associated with self-reported fear of falling. The cost of falls was £1088. Similarly, the cost of falls leading to a fracture was £15,133, £2,753, £1,863, £1,331 and £3,498 for hip, wrist, arm, vertebral and other fractures, respectively.
Discussion
The main burden to morbidity is due to fear of falling. Interventions aimed at reducing fear of falling may produce larger gains in HRQoL.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Fractures and falls are serious cause of morbidity and cost to society [1]. In the UK, the importance of fall-related injuries has been recognised in the recently published National Service Framework (NSF) for Older People [2]. The NSF calls for health improvement plans to be devised that will reduce the burden of fall-related injuries. A previous study estimated the cost burden of fractures to society in the region of £1.8 billion [3] ($2.8US billion and €2.5 billion, 2003 PPP [4]). The hip fracture cost estimate was partly based on patient-level data but non-hip fracture costs and were largely based on published estimates from aggregated data, and therefore, may not be entirely accurate. Furthermore, of equal importance is the health-related quality life (HRQoL) loss due to falls, fear of falling as well as hip and other fall-related fractures.
Between 1993 and 2006, fracture costs reported in the literature have been estimated from a variety of sources such as expert opinion [5, 6], medical records [7–9] and decision models [10]. Only one study has reported to have collected patient-level resource use data [11]. However, the mean age of the patients participating in that study was 55 years, considerably younger than the group of patients considered at higher risk of fracture, i.e. women aged 70 years and over. These cost estimates, derived from a cohort of relatively young women, are likely to underestimate the fracture costs of women aged 70 years and over, who represent the majority of fracture cases. The cost of falls that do not cause a fracture is relatively unknown. However, because the incidence of falls is higher than that of fractures [12–14] even if they were associated with relatively slight costs and poorer quality of life, this would be a considerable burden. As well as increasing costs, of [12] more importance is the impact fractures have upon HRQoL. A systematic review conducted in 2003 found that most economic studies of treatments for fracture prevention have not used patient-derived quality of life [15]. The impact of both falls and fear of falling has not been quantified. The aim of this study is to use an opportunistic sample of UK women to assess the impact of falls, fracture and fear of falling on costs and generic quality of life.
Materials and methods
Individual patient-level data from two randomised controlled trials and one cohort study conducted by one of the authors in the field of fracture prevention were used to explore the impact of falls and fractures on HRQoL, as measured by the EuroQol-5D (EQ-5D) [16] questionnaire. The EQ-5D ‘utility’ scores range from −0.594 to 1, where a value of ‘one’ indicates perfect health, ‘zero’ represents dead and negative values indicate that individuals perceive those health states as worse than dead [17]. The interval properties of this instrument make it useful within economic evaluations of healthcare technologies [17]. The main characteristics of the data sets used are described below.
Hip protector study
This is a pragmatic, randomised trial of hip protectors for the prevention of hip fractures among women living in the community [18]. Women aged 70 years and over with one or more risk factors for hip fracture (low body weight, current smoker, prior fracture, family history of hip fracture) were eligible. Furthermore, data on fear of falling were measured on a six-level Likert scale that went from stating to have been worried about falling ‘all of the time’ to have been worried ‘none of the time’ [19]. Four thousand one hundred and ninety-six women were recruited into this study (mean age 77.8 years). Participants were followed-up for a minimum of 2 years and a maximum of 42 months (median follow-up 28 months). Data on fracture and fall incidence, risk factors for fracture, i.e. weight, age, smoking status, HRQoL, were collected at baseline and at six monthly intervals after that.
Calcium and vitamin D study
This is a pragmatic, open, randomised, controlled study of calcium and cholecalciferol (vitamin D3) for prevention of fractures in primary care [12]. A total of 3,314 women were recruited into this study (mean age 76.8 years). Women aged 70 years and over with one of more risk factors for hip fracture [any previous fracture, low body weight (less than 58 kg), current smoker, family history of hip fracture, fair or poor self-reported health] were eligible. Data on fracture and fall incidence, HRQoL measured with the EQ-5D and fear of falling measured on the same six-level Likert scale used in the hip protector study were collected at baseline and every 6 months after that for a minimum of 2 years and a maximum of 42 months (mean follow-up 25 months).
Epidemiological risk factors study
This was a prospective, comprehensive, cohort study of women aged 70 years and over living in North Yorkshire and Cumbria regions in England [20]. Four thousand two hundred and ninety-two women were recruited into this study (mean age 76.9). Data on risk fractures for fracture (personal history of previous fracture, family history of hip fracture, low body weight, i.e. less than 58 kg, smoking status), incidence of falls and fractures were measured at baseline and on a 12-month basis for 24 months. As for the previous studies, the authors collected individual-level data on HRQoL and fear of falling using the same Likert scale used in the hip protector study. Although the study collected these data at three different time points, the present application includes measurements at the first and second follow-ups when data on HRQoL were collected. This was necessary in order to ensure comparability with the other two case studies. This study sample also includes a subgroup of participants from the hip protector trial. This is because two of the larger centres from the hip protector study also recruited participants for the epidemiological cohort study. Thus, all women aged 70+ who either consented for the hip protector trial or the cohort study were included.
Resource use data collection
A fall and fracture questionnaire was designed and administered to individuals (N = 1190) participating in the calcium and vitamin D trial who had previously indicated to be willing to be contacted in the future for research purposes. Participants were asked whether in the last 12 months they had experienced a fall and/or a fracture, the number of times they had seen a doctor, GP or consultant and whether they had been hospitalised for reasons other than a fall or fracture and for how long. In addition, those participants having experienced either a fall or a fracture were also asked about whether they had been hospitalised and their length of stay in hospital, the number of times they had seen a doctor or nurse, whether they had changed residence as a consequence of their fall and/or fracture and for how long. Finally, they were asked to describe any treatments that had been specifically prescribed for their fall or fracture over the same 12-month period.
Resource use was valued using routinely published UK national data to estimate the economic impact of falls and fracture in the sample of patients enrolled in the vitamin D trial. Table 1 lists the unit costs associated with the key resource use. Hospital inpatient length of stay was costed using NHS reference costs [21], which represent fully allocated cost estimates, as opposed to purely ‘hotel costs’. Similarly, the cost of surgery following hip, wrist, arm and vertebral fractures were also obtained from the NHS reference cost. Specialist contact visits were valued using the costs indicated in the Chartered Institute of Public Finance and Accountancy (CIPFA) data base [22], while GP and nurse visits, residential accommodation and the cost of home help were valued using the figures routinely produced from the Personal and Social Services Research Unit at the University of Canterbury [23].
Analysis
Descriptive statistics were obtained to assess the similarity of the patients’ sample in the three studies. Where three or more measurements per individual were available, a hierarchical (multilevel) regression model was used to analyse the data and account for the longitudinal collection of the outcome (i.e. quality of life measure), which was expected to display high within subject correlation. This modelling strategy facilitates the analysis of the entire data set even in presence of missing or incomplete observations over time [24, 25].
The models were implemented in the statistical package MLwiN 2.02 [26] and estimated using maximum likelihood estimation procedures (i.e. RIGLS). Model comparison was carried out using the deviance statistic which is calculated as minus twice the log-likelihood. Difference between the deviance statistics obtained from two alternative models were contrasted against a chi-square distribution with degrees of freedom equal to the difference between the number of parameters in the two models. The lower the deviance, the best the model fit.
In the risk factors study, only two measurements per individual were available. In this case, we used an analysis of covariance (ANCOVA) model, regressing the value of the outcome variable at the end of the study against a set of baseline covariates, including the baseline value of the outcome.
Mean EQ-5D decrements associated with falls and fractures estimated from the multilevel model were combined with life expectancy data for the UK general population of women aged 70 to estimate the quality-adjusted life years lost for women with falls and fractures. Quality-adjusted life years (QALYs) estimation was performed assuming a linear interpolation between time points and a constant EQ-5D score over the remaining life expectancy of British women aged 70 years and over.
A simple analysis of resource use data was undertaken; this was dictated by the fact that very few events (i.e. falls and fractures) were reported to have occurred in the last 12 months by the participants in the calcium and vitamin D3 trial who had agreed to be contacted again for research purposes. Hence, a simple account of the healthcare resource use associated with each event was preferred to any regression-based analysis.
Results
Impact of falls and fractures on HRQoL
Table 2 reports the baseline characteristics of women who took part in each of the three case studies. These are used in the analyses presented in the following section. In view of the fact that a difference in treatment effect was neither found in the hip protector or the calcium and vitamin D3 trials, the present analysis does not distinguish between treatment groups.
Compared to the participants of the calcium and vitamin D3 and the epidemiological risk factors studies, women in the hip protector trial were older, had lower bodyweight, were more likely to have had previous fractures and falls and were current smokers. Despite this, women in the hip protector study had only marginally lower HRQoL at baseline; see Table 2.
The hip protector trial
Of the 4,196 subjects who participated in the hip protector [18] trial, 3,223 had a baseline measurement of HRQoL described by the EQ-5D, with response rate at 6, 12 and 18 months being respectively 89%, 83% and 82%. The longitudinal nature of the data collection means that individual-level observations are expected to display a certain degree of correlation.
A graphical exploration of inter-temporal trends in the mean EQ-5D, SF-12 mental and physical summary scores and their 95% confidence intervals indicated low variability associated with EQ-5D scores over time. This suggests that a model linear in the covariate ‘measurement occasion’ may be adequate. Unlike the EQ-5D, both mental and physical scores of the SF-12 showed a statistically significant sharp departure from baseline to 6 months and a linear trend after that (data not presented but can be requested from authors).
Table 3 reports the results of the models explained in the ‘Materials and methods’ section applied to EQ-5D data. The starting point of the analysis was to fit a ‘null model’ including measurement occasion (‘Time’) as the only explanatory variable. By separating the total variance into the component related to between-patients variation and within-patient variation, this model facilitated the estimation of the intra cluster correlation (ICC) coefficient, calculated as \(\left( {{{\sigma _{u_0 }^2 } \mathord{\left/ {\vphantom {{\sigma _{u_0 }^2 } {\left( {\sigma _{u_0 }^2 + \sigma _e^2 } \right)}}} \right. \kern-\nulldelimiterspace} {\left( {\sigma _{u_0 }^2 + \sigma _e^2 } \right)}}} \right)\), which represents the degree of similarity between measurements taken from the same individual over time. The ICC for the null model is 0.74. The null model does not identify any important trend over time in the EQ-5D score.
The ‘full model’ results of which are reported in Table 3 introduces a set of explanatory variables, representing factors that are expected to have an impact on the risk of fractures (and consequently to affect HRQoL), together with the time-by-fracture and time-by-fall interaction terms. Several considerations can be made from the results of this model fitted to data from the hip protector study. First of all, most covariates have a statistically significant impact on HRQoL as measured by the EQ-5D questionnaire. The coefficient of the variable current smoker has the expected negative sign suggesting that, all things being equal, smokers (on average) had a lower average HRQoL. Similarly, patients older than the overall mean in this trial (see Table 2) have on average lower HRQoL, with a decrease in the EQ-5D score of 0.0017 for every year departing from the sample mean. Neither bodyweight nor measurement occasion has a statistically significant impact on the EQ-5D score. A major role in affecting the EQ-5D score is played by the intensity of the ‘fear of fall’, with statistically significant quality of life decrements associated with increasing level of anxiety. With regard to the impact of fractures and falls over time, the model suggests that these events have a (statistically significant in the case of fractures) negative impact on HRQoL, as measured by the EQ-5D score.
The calcium and vitamin D3 prevention trial
Of the 3,314 women who participated in the calcium and vitamin D3 study, [12] 3,240 had a baseline measurement of EQ-5D, with response rate at 6, 12 and 18 months being 79%, 74% and 59%, respectively. As for the hip protector trial, there is high correlation between the outcome variables at each time point. Inspection of the baseline characteristics of women enrolled in this trial (Table 2) indicates that this sample is somewhat similar to the sample of women who participated in the hip protector study. Compared to participants in this study, individuals enrolled in the calcium and vitamin D3 trial were 1 year younger, had a greater bodyweight by 4 kg, had experienced less falls in the previous 12 months, were less likely to be a smoker (7.8% smoked), had a lower number of past fractures and had a better HRQoL at baseline as measured by the EQ-5D score. In this trial, no reduction in the fear of falls over time was observed. In fact, while 44% of women reported to have no concern at all regarding the fear of fall at baseline, this percentage falls to 31% at 6 months, 28% at 12 and 27% at 18 months.
Table 3 reports the analysis of EQ-5D scores from participants in the calcium and vitamin D3. There is no significant trend over time in the EQ-5D score. The full model introduces a set of baseline covariates in the attempt to reduce some of the between-individuals variation observed in the null model. This model suggests that smoker women with lower bodyweight and older than this trial’s overall mean for weight and age (see Table 2) have statistically significantly lower HRQoL as measured by the EQ-5D score. As expected, baseline EQ-5D is a strong predictor, and this does not raise any particular issue. Measurement occasion is still not statistically significant. The change in the algebraic sign of the parameter Time between the two models is probably due to chance. As found in the hip protector trial, one of the most important factors affecting the HRQoL in women is their fear of falls. Table 3 suggests that the higher the fear of fall, the lower the EQ-5D score, with a 20% reduction in women who are worried all the time about falls. This is to be expected as the dimension anxiety/depression has a strong impact on the EQ-5D score, with reductions of 0.071 for moderate anxiety and of 0.231 for severe anxiety [27]. The full model represents a significant improvement with respect to the null model as measured by the change in deviance of 2,702 and reduction of the between-individuals’ unexplained variability. The findings regarding the impact of falls and fractures on EQ-5D scores support the expectation that both events are associated with a decrement in HRQoL, with fractures involving a much greater loss in quality of life. In particular, the results of this model suggest that fractures have twice the impact of falls in reducing HRQoL (−0.0062 versus −0.003).
The epidemiological risk factors cohort study
The epidemiological risk factors cohort study [20] provides the third piece of evidence regarding the role that falls and fractures play in affecting women’s HRQoL. As mentioned previously, the risk factors study was a longitudinal survey, which recruited women with and without risk factors for fractures at baseline. Given, only two observations of HRQoL (baseline and 12 months) were available for each individual in this sample. The analysis was therefore conducted using a simple ANCOVA approach.
Table 3 reports the results of the regression model, including all covariates. This analysis suggests that women who are currently smokers have on average a lower EQ-5D score, although the impact of smoking impact is not statistically significant. Consistently, with the analyses presented so far for the other case studies, the evidence provided by the risk factors study suggests that women older than the trial mean (76.9) patients have a statistically significant lower EQ-5D score, with the opposite being true for women younger than 76.9 years old. Similarly, women whose bodyweight is greater than the overall mean (64.2 kg) have a statistically significant lower EQ-5D score. Furthermore, as it was found in the other data sets, the greater the fear of fall, the lower the EQ-5D score.
Finally, both falls and fractures were associated with a reduction in EQ-5D, but this was not statistically significant. This result might be related to the small percentage of fractures in the 12 months of the study (e.g. 9%), although percent of falls was 26%. In addition, in the epidemiological risk factors study, the time interval for the measurement of the EQ-5D is twice as long (12 months) as the one used in the hip fracture and the calcium and vitamin D3 studies (6 months); this could have diluted the effect of falls and fractures in self-reported HRQoL.
Impact of falls and fractures on healthcare resource use and costs
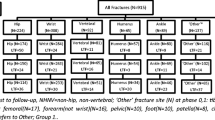
The overall response rate to the postal fall and fracture questionnaire was 93% (1,110/1,190); valid responses were provided in 99.6% of these cases. Eight hundred individuals (72.3%) reported not having had a fall or a fracture in the previous 12 months. Of the 302 respondents (27.2%) who reported falls in the previous 12 months, 62 (20.5%) said their fall resulted in a fracture. The incidence of fractures associated with an event other than a fall was 0.3%; only three individuals reported to have had a fracture without having experienced a fall.
Table 4 reports summary statistics of NHS contacts related to falls with and without fractures in the calcium and vitamin D3 trial. Nine of the 237 women experiencing a fall without a fracture were also hospitalised, while 25 of the 37 women who reported a fracture following a fall were also hospitalised. As expected, falls which did not lead to a fracture required only limited health care resources. On the other hand, falls leading to fractures were more often associated with large resource use (e.g. hospital stay, surgery, etc.). As expected, only a small minority of falls led to hospital in patient stay (4% of cases) as opposed to a third of women who reported a fracture. Most women had an inpatient length of stay, which ranged between 1 and 32 days (mean 9.6). In two cases, the fracture required day hospital admission only. Only a third of women who experienced a fall went to see either a GP or hospital doctor, as opposed to 77% of women who had a fracture. The latter group had more frequent contacts with their doctor, unlike nurse contacts which were similar between the two groups. Only eight women in total reported a change of residence in the last 12 months, and five responders related this event to their fracture. In this sample, the change in residence had little if no impact on the NHS budget, as all women except one said that they went to live with relatives. Finally, the need to use home help was similar between the two groups.
Three final questions were also included in questionnaire, which were aimed to ascertain whether responders who had experienced a fall and/or a fracture had a higher propensity to seek health care contacts. These questions related specifically to GP and hospital (doctor and inpatient stay) contacts. The two groups seemed to be balanced in terms of their GP contacts, with approximately 85% of women in each group reporting one or more GP contacts in the previous 12 months. Similarly, hospital inpatient stay for any reason was similar between women reporting a fall and those experiencing a fracture. The only difference was in the proportion of people reporting having hospital doctor contacts. Women who reported a fracture in the previous 12 months had higher frequency of outpatient contacts (78%) than those reporting to have had a fall (53%).
Estimates of health care cost by cost category (hospital stay, doctor visit, nurse visit, home help) and by event and/or fracture type (fall, hip, wrist, arm, vertebral and other fracture) are reported in Table 5. Hospital stay and home help were the two main resource categories contributing to the cost of falls and fractures. Whilst treatment cost associated with fall was some how lower than that associated with a fractures (any type), the magnitude of this difference was not as large as might have been expected.
Burden of falls and fracture
Falls represented both a significant cost and quality of life burden. Few fallers were admitted to hospital; however, because the incidence of falling is so much higher than the incidence of fractures, even relatively small proportions will represent a high cost burden. In this study, we found that 4% of fallers were admitted to hospital and 30% saw a doctor (Table 4). In contrast, those who fell and fractured did have a much higher use of health care resources than the fallers with 33% having to be admitted to hospital. Because of this higher cost, fractures still represent a higher cost burden to society than falls (Table 6),
In terms of the quality of life burden, the greatest burden of loss of quality of life is for fear of falling rather than the fall or fracture. Many women in our study had a significant fear of falling, and modelling this fear to a cohort of 10,000 women, we found that by far, the largest quality of life lost was due to this fear of falling. The 597 QALYs lost per year significantly exceeded that lost from both falling and fracture combined (Table 6).
Discussion
In this study, we have analysed several large datasets that collected generic quality of life outcomes and costs on older women who were at risk of falling and fracture. We have shown that fractures are a cause of significant cost and morbidity to older women. These results support other studies [28–31]. A comparison of our cost estimates for hip and vertebral fracture with those available in the literature indicated that our estimates were within the confidence limits of earlier studies [29, 32]. Estimates of acute hospitalisation costs for hip fracture (£12,163) from a more contemporary study [8] indicate that our estimate may be underestimating the true hospitalisation costs for hip fracture. Conversely, our estimates for wrist and arm fracture were considerably higher than previously reported. Given the small number of fracture events included in our sample and our inability to confirm outcomes and consumption of resources with the participant’s GP, these results should be taken with caution.
We have also estimated a cost for a non-fracture fall. The cost of a non-fracture fall was unexpectedly high, amounting to about the third of a cost of wrist fracture or half of a cost of vertebral fracture (Table 5). It is possible that the costs of the falls might be biased towards the higher cost falls. Falls that had more serious physical and financial consequences, such as having to be seen by a GP, are likely to have been remembered and reported more than a fall that did not require any medical assistance. Therefore, we may have overestimated the costs of the ‘average’ fall. However, our estimate of falls is not too dissimilar to that reported from previous cross-sectional studies, where the fall rate in women aged 70 to 74 and 75 to 79 has been estimated as 26% and 33%, respectively [33].
Fear of falling was the largest cause of morbidity in this population of women. The fear of falling was the equivalent of the 6% decrement in a QALY per woman per year. In contrast, the QALY lost due to fracture was only a tenth of this amount.
Previous research into the fear of falling has found it to have a significant impact on quality of life. Cumming and colleagues in a study of 528 people in Australia found that fear of falling was a significant predictor of poor quality of life [34]. Our study confirms and extends those findings. First, our study is a sample from the community, whereas the Australian study recruited participants from hospitals. Also, in our study, we have measured quality of life with a measure of utility (the EuroQol-5D), which allows the burden of fear of falling to be converted to a single measure of HRQoL. Similarly, a recently published RCT of fall prevention programmes and quality of life in the elderly found evidence that improvements on HRQoL associated with exercise training were matched with reductions in self-reported fear of falling [35]. Unlike the other two fall prevention programmes evaluated in this study (education and home assessment and modification), individuals on exercise training were the only ones consistently reporting reductions in their fear of falling overtime. This coincides with our result that fear of falling is a major factor influencing quality of life in the elderly.
Our study does have some weaknesses that must be acknowledged. For the quantification of falls and fractures, we relied on self-report via postal questionnaire. Whilst this may be a less accurate form of outcome assessment—subject to under or over reporting—other methods such as telephone interviews and collection of data from clinical records required higher human and financial resources [36, 37]. Furthermore, there is evidence supporting the use of self-report of fractures in elderly populations as a reasonably accurate mean to collect fracture data when the recall interval is shorter than 2 years [38]. Having said that, our inability to confirm the occurrence of a fall /fracture implies that potential ascertainment bias cannot be fully discounted.
Although we recruited participants from the community, most people we sampled either refused or could not participate in the study. Therefore, we may have sampled a relatively healthy proportion of the population as such ‘volunteer’ bias tends towards including healthier individuals. Our results may have been different if we could have recruited and retained a true random sample of older women from the population. This issue should be addressed in future studies. Similarly, a recently published study proposes an algorithm to map the health states described in the SF-12 into a preference-based score [39]; the impact of fear of falling in this alternative score shall be the subject of a future study. Qualitative research may be used to gain a deeper understanding of the main sources for fear of falling related anxiety reported by the participants in the three case studies used here.
It could be argued that the impact of fractures on HRQoL depends on whether it is the first, second, third, etc. fracture event. The datasets available to us did not contain sufficiently detailed information to allow us to explore this issue, but this could be addressed in future prospective studies. Finally, our results consider only women; however, there is some evidence to suggest that the mortality rate after hip fracture is higher in men than in women [40]. Furthermore, the same study found that the proportion of years of life lost is higher for men, which in turn suggests that the impact of hip fractures of survival is worse for men. Consequently, had men been included in this study, we may had observed a higher impact on HRQoL associated with both falls and fractures. This could be explored in a future study including both men and women.
In summary, we have used an opportunistic sample of women to assess the impact of falls, fracture and fear of falling on costs and quality of life. We have found that the main burden of morbidity is due to fear of falling rather than falls or the sequelae of falls. Consequently, interventions aimed at reducing fear of falling may produce large quality of life gains, and this may be a cost-effective approach to increasing quality of life in society. Future health policy programmes aimed at improving/maintaining HRQoL in the elderly should consider evaluating interventions such as exercise programmes [35] that could potentially positively influence both fear of falling and fall prevention.
References
Fraser WD (2004) The burden of osteoporosis and the case for disease management. Disease Management and Health Outcomes 12:409–418
UK Department of Health (2001) National service framework for older people. Department of Health, London
Torgerson DJ Iglesias CP Reid DM (2001) The economics of fracture prevention. In Barlow DH, Francis RM, Miles A (eds) The effective management of osteoporosis. Aesculapius Medical, London, pp 111–121
OECD—Organisation for Economic Co-operation and Development (2007) Purchasing power parities (PPP). http://www.oecd.org/std/ppp
Daly E, Vessey MP, Barlow D, Gray A, McPherson K, Roche M (1996) Hormone replacement therapy in a risk-benefit perspective. Maturitas 23:247–259
Daly E, Gray A, Barlow D, McPherson K, Roche M, Vessey M (1993) Measuring the impact of menopausal symptoms on quality of life. Br Med J 307:836–840
Coyle D, Cranney A, Lee KM, Welch V, Tugwell P (2001) Cost effectiveness of nasal calcitonin in postmenopausal women: use of cochrane collaboration methods for meta-analysis within economic evaluation. PharmacoEconomics 19:565–575
Lawrence TM, White CT, Wenn R, Moran CG (2005) The current hospital costs of treating hip fractures. J Care Injured 36:88–91
Stevenson MD, Davis SE, Kanis JA (2006) The hospitalisation costs and out-patient costs of fragility fractures. Women’s Health Medicine Journal 3:149–151
Kanis JA, Dawson A, Oden A, Johnell O, De Laet C, Jonsson B (2001) Cost-effectiveness of preventing hip fracture in the general female population. Osteoporos Int 12:356–361
Fleurence R, Torgerson DJ, Reid DM (2002) Cost-effectivenesss of hormone replacement therapy for fracture prevention in young postmenopausal women: an economic analysis based on a prospective cohort study. Osteoporos Int 13:637–643
Porthouse J, Cockayne S, King C, Saxon L, Steele E, Aspray T et al (2005) Randomised controlled trial of calcium and supplementation with cholecalciferol (vitamin D3) for prevention of fractures in primary care. Br Med J 330:1003–1008
Tinetti ME, Speechley M, Ginter SF (1988) Risk factors for falls among elderly persons living in the community. N Engl J Med 319:1701–1707
Pluijm SM, Smit JH, Tromp EA, Stel VS, Deeg DJ, Bouter LM, Lips P (2006) A risk profile for identifying community-dwelling elderly with a high risk of recurrent falling: results of a 3-year prospective study. Osteoporos Int 17:417–425
Fleurence R, Iglesias CP, Torgerson DJ (2008) Economic aspects of osteoporosis treatments. In Treatment and prevention of osteoporosis. Arnold (in press)
Kind P (1996) The EuroQoL instrument: an index of health-related quality of life. In: Spilker B (ed) Quality of life and pharmacoeconomics in clinical trials. Lippincott-Raven, Philadelphia, pp 191–201
Drummond MF, Sculpher MJ, Torrance G, O’Brien BJ, Stoddart G (2005) Methods for the economic evaluation of health care programmes. Oxford University Press, Oxford
Birks YF, Porthouse J, Addie C, Loughney K, Saxon L, Baverstock M et al (2004) Randomised controlled trial of hip protectors among women living in the community. Osteoporos Int 15:701–706
Likert R (1932) A technique for the measurement of attitudes. Arch Psychol 140:1–55
Porthouse J, Birks YF, Torgerson DJ, Cockayne S, Puffer S, Watt I (2004) Risk factors for fracture in a UK population: a prospective cohort study. Q J Med 97:569–574
Department UK of Health (2004) Reference cost 2002/2003. Department of Health, London
The Chartered Institute of Public Finance and Accountancy (CIPFA) (2004) The Health Service Database. http://www.cipfa.org.uk
Netten A, Dennett J, Knight J (2004) Unit costs of health and social care. PSSRU, University of Kent, Canterbury
Beacon HJ, Thompson SG (1996) Multi-level models for repeated measurement data: application to quality of life data in clinical trials. Stat Med 15:2717–2732
Omar RZ, Wright EM, Turner RM, Thompson SG (1999) Analysing repeated measurements data: a practical comparison of methods. Stat Med 18:1587–1603
Rasbash J, Browne W, Goldstein H et al (2000) A user’s guide to MLwiN Version 2.1. Institute of Education, University of London, London
Dolan P (1997) Modeling valuations for EuroQol health states. Medical Care 35:1095–1108
Kanis JA, Brazier JE, Stevenson M, Calvert NW, Lloyd Jones M (2002) Treatment of established osteoporosis: a systematic review and cost-utility analysis. Health Technol Assess (Winchester, England) 6:1–146
Dolan P, Torgerson DJ (1998) The cost of treating osteoporotic fractures in the United Kingdom female population. Osteoporos Int 8:611–617
Fleurence RL, Iglesias CP, Torgerson DJ (2006) Economic evaluations of interventions for the prevention and treatment of osteoporosis: a structured review of the literature. Osteoporos Int 17:29–40
Iglesias CP, Torgerson DJ, Bearne A, Bose U (2002) The cost utility of bisphosphonate treatment in established osteoporosis. QJM—Monthly Journal of the Association of Physicians 95:305–311
Puffer S, Torgerson DJ, Sykes D, Brown P, Cooper C (2004) Health related cost of women with symptomatic vertebral fractures. Bone 35:383–386
O’Neill TW, Varlow J, Reeve J, Reid DM, Todd C, Woolfe AD, Silman AJ (1995) Fall frequency and incidence of distal forearm fracture in the UK. J Epidemiol Comm Hlth 49:597–598
Cumming RG, Salkeld G, Thomas M, Szonyi G (2000) Prospective study of the impact of fear of falling on activities of daily living, SF-36 scores, and nursing home admission. J Gerontol 55A:M299–M305
Lin MR, Wolf SL, Hwang HF, Gong SY, Chen CY (2007) A randomized, controlled trial of fall prevention programs and quality of life in older fallers. J Am Geriatr Soc 55:499–506
Nevitt M, Cummings S, Browner W, Seeley D, Canley J, Vogt T (1992) The accuracy of self-report of fractures in elderly women: evidence from a prospective study. A J Epidemiol 135:490–499
McColl E, JAcoby A, Thomas L, Soutter J, Thomas R, Harvey E, Garrat A, Bond J (2003) Design and use of questionnaires: a review of best practice applicable to surveys of health service staff and patients. Health Technol Assess 5:1–272
Bush T, Miller S, Golden A, Hale W (1989) Self-report and medical record report agreement of selected medical conditions in the elderly. Am J Public Health 79:1554–1556
Brazier JE, Roberts J (2004) The estimation of a preference-based measure of health from the SF-12. Medical Care 42:851–859
Trombetti A, Herrmann F, Hoffmeyer P, Schurch M, Bonjour J, Rizzoli R (2002) Survival and potential years of life lost after hip fracture in men and age-matched women. Osteoporos Int 13:731–737
Acknowledgements
This work was undertaken by The University of York who received funding from the Department of Health. The views expressed in the publication are those of the authors and not necessarily those of the Department of Health. Also, we would like to thank two anonymous referees for their valuable comments on a previous version of this manuscript.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Iglesias, C.P., Manca, A. & Torgerson, D.J. The health-related quality of life and cost implications of falls in elderly women. Osteoporos Int 20, 869–878 (2009). https://doi.org/10.1007/s00198-008-0753-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-008-0753-5