
Abstract
Summary
Health-related quality of life in elderly women with sustained incident fractures was assessed prospectively for 1 year, using the EuroQol standard. Loss of QOL was more severe in patients after hip or vertebral fractures than those with wrist fracture. QOL was not completely restored in patients suffering from hip fracture.
Introduction
Osteoporosis-related fractures decrease mobility, social interaction, and emotional well-being. All of these characteristics determine health-related quality of life (HR-QOL). In this study, we assessed HR-QOL in elderly women following incident clinical fractures.
Methods
Thirty-seven patients with hip fractures (mean age 76.1 years), 35 with vertebral fractures (mean age 72.6 years), and 50 with wrist fractures (mean age 68.6 years) were enrolled. HR-QOL was prospectively measured using EuroQol (EQ-5D) before the fracture, 2 weeks, 3 months, 6 months, and 1 year after the fracture.
Results
During the observation period, reduction of EQ-5D values was greatest in the hip fracture group. In the wrist fracture group, EQ-5D values at 6 months after the fracture showed recovery; however, in the hip and vertebral fracture groups, recovery was significantly lower than before the fracture. One year after the fracture, EQ-5D values were not significantly different from prefracture values in the vertebral and wrist fracture groups, but remained significantly lower in the hip fracture group.
Conclusions
Loss of QOL was more severe in patients after hip or vertebral fractures than in patients with wrist fracture. HR-QOL was not completely restored in patients suffering from hip fracture.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The severity of osteoporosis ranges widely from mild cases with no symptoms or only a single minor fracture during a lifetime to severe cases with multiple fractures and sequelae. The risk of vertebral and limb fractures, such as those of the hip and wrist, increases with the progression of osteoporosis. Among the elderly, osteoporosis-related fractures are so prevalent that they cause significant morbidity. Data from the 1990s or later from Northern Europe [1] and North America [2–4] indicate that the incidence of hip fractures does not increase with time; however, most reports from Asian countries, including Japan, do show an increase [5, 6]. According to a survey performed between 1986 and 1995, the incidence of wrist and proximal humerus fractures also significantly increases with time [7]. With the rapidly increasing elderly population in Asian countries, osteoporosis-related fractures are becoming responsible for considerable health expenditures.
In addition to causing pain and disturbance of physical function, fractures may decrease mobility, social interaction, and emotional well-being [5]. All of these characteristics determine quality of life (QOL). A growing number of studies show that fragility fractures in elderly patients have a considerable impact on QOL; however, there have been only a few studies of generic health-related quality of life (HR-QOL) measured prospectively in patients with incident fractures [8–10]. There have been no reports specifically describing the prospective measurement of HR-QOL after incident fractures among elderly patients in Japan or any Asian country.
Recent anti-osteoporosis pharmaceutical therapies can reduce the risk of fragile fractures by up to 50% [11]. However, due to limited health care resources, there is an increased need to demonstrate the cost-utility of these therapies. The influence of fragility fractures on HR-QOL specifically needs to be incorporated into cost-effectiveness analyses [12]. Thus, the present study sought to assess HR-QOL in elderly women following incident hip, vertebral, and wrist fractures using a prospective observational study.
Materials and methods
Patients
For this study, we recruited patients meeting the following criteria: women 45 years old and over who sustained incident clinical fracture of the vertebra, hip, or wrist (distal radius), caused by minor trauma such as falls while standing and who were consecutively treated at one of four hospitals in Tottori Prefecture between 2004 and 2005. Exclusion criteria were pathological fractures resulting from metastatic disease or those resulting from high-energy trauma such as traffic accidents or falls from heights. Incident vertebral fractures were diagnosed by lateral radiographs of the spine as well as physical findings, and the diagnoses were confirmed by magnetic resonance images (MRI) and/or vertebral height loss or sclerotic changes evaluated from subsequent radiographs. Patients with dementia and those who could not complete the questionnaire due to severe cognitive dysfunction were also excluded. All subjects were identified at the time of their first visit or admission and prospectively followed for 1 year.
The study was approved by the local research ethics committee of the Faculty of Medicine, Tottori University and performed in accordance with the Declaration of Helsinki. All enrollments were carried out after obtaining informed consent.
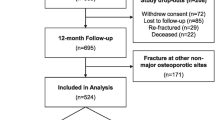
Although informed consent was initially provided, two patients with hip and two patients with wrist fracture withdrew from the study before the evaluation 3 months after the fracture; these four patients were excluded from the analysis. A total of 37 patients with hip fractures (mean age 76.1 years) including 16 with femoral neck and 21 with trochanteric fractures, 35 with vertebral fractures (mean age 72.6 years), and 50 with wrist fractures (mean age 68.6 years) were enrolled and followed in this study (Table 1). Mean patient age was significantly higher, and body mass index (BMI) was significantly lower, in the hip fracture group than in the other two groups. If a patient sustained new fractures during the course of the study, not only second fracture but also other clinical fractures, the HR-QOL evaluation was stopped for that patient. Among the enrolled patients, one in each group was eliminated by new fractures; one of the hip fracture patients dropped out due to a newly developed complication; three of the hip fracture patients, three vertebral fracture patients, and nine wrist fracture patients dropped out due to loss of contact for no specified reason, and one of the hip fracture patients and one of the vertebral fracture patients died during the observational period.
In the hip, the vertebral, and the wrist fracture groups, 5, 8, and 5 patients, respectively, had been diagnosed as having osteoporosis before the fracture. The numbers of patients receiving anti-osteoporosis drugs before and after the fracture are presented in Table 1. It was unclear whether some patients were receiving the medications, since they had been prescribed by other doctors and details could not be obtained. Nine patients in the hip fracture group, 8 in the vertebral fracture group, and 12 in the wrist fracture group had previous fractures. Several patients had comorbidities before the fracture: In the hip fracture group, four patients had cancer, three had stroke, and two had rheumatoid arthritis; there were 2, 3, and 0 in the vertebral fracture group, and 1, 2, and 1 in the wrist fracture group, respectively. Among patients with vertebral fractures, the fracture level was defined at the T9, T11, T12, L1, L2, and L3 vertebra in 2, 3, 8, 11, 7, and 4 patients, respectively. Four patients had prevalent lumbar fractures.
All patients with hip fractures, 22 of those with vertebral fractures, and 25 of those with wrist fractures were admitted to the hospital for treatment. Mean durations of hospitalization for primary treatment were 61.3 days (range 9–157, median 56.0), 25.9 days (7–58, 22.0), and 16.2 days (1–48, 14.0) in the hip, vertebral, and wrist fracture groups, respectively. All patients with hip fractures, none of those with vertebral fractures, and 22 of those with wrist fractures were treated with surgery. The numbers of patients receiving nonsteroidal anti-inflammatory drugs (NSAIDs) are presented in Table 1.
Health-related quality of life
HR-QOL was measured using the EuroQol standard (EQ-5D) [13]. EQ-5D is a generic questionnaire with a visual analogue scale (VAS). Each of the five dimensions or domains of the EQ-5D profile [EQ-5D(profile); mobility, self-care, performance of usual activities, pain/discomfort, and anxiety/depression (not to be confused with clinically diagnosed depression)] is divided into three levels of difficulty: no problem, some problem, or extreme problem. This is expressed as a health profile, and each of the 243 possible health states defined by this profile has been assigned a health utility rating (EQ-5D(utility)) based on data collected from a representative sample of the Japanese general population [14, 15]. The anchor points for EQ-5D(utility) are “perfect health” = 1 and “death” = 0. Since calculation of the weighted health utility score requires comparison with the general population, we have used the Japanese general population as our comparator. Age-specific normative values (mean ± SD) for EQ-5D (utility) have been reported for Japanese women aged 65 to 69 years, 70 to 74 years, 75 to 79 years, 80 to 84 years, and 85 years and over as 0.862 ± 0.167, 0.810 ± 0.187, 0.771 ± 0.182, 0.769 ± 0.173, and 0.684 ± 0.230, respectively [16]. We used these values and calculated the age-adjusted values of EQ-5D (utility) for our patients (since age-specific normative values for Japanese women are available only for those aged 65 and older, age-adjusted QOL values were calculated for patients age 65 years and older).
Baseline questionnaires inquired about prefracture mental status and prefracture comorbidities. When necessary, these questions were asked of patients’ relatives. EQ-5D (profile) and VAS (EQ-5D (vas), with “perfect health” = 100 and “worst possible health” = 0) were prospectively evaluated for the period before the fracture as well as for 2 weeks, 3 months, 6 months, and 1 year after the fracture. Prefracture QOL was evaluated based on the patient’s recollection. Questionnaires were self-completed, but assistance was provided by relatives if necessary because of pain or hearing difficulties.
Statistical analysis
Multiple comparisons among groups were performed using Tukey’s test after a repeated-measures analysis of variance (ANOVA) for age, body height, body weight, and BMI. Nonparametric multiple comparisons with prefracture values were performed using Dunn’s test for EQ-5D (utility). For comparisons between two groups, the Mann–Whitney test was performed. Statistical analysis was performed using SPSS (SPSS II for Windows Version 11.0.1J, SPSS Japan, Tokyo, Japan) and Stat Flex (Version 5, Arteck, Osaka, Japan); p < 0.05 was considered statistically significant.
Results
EQ-5D(utility)
Prefracture values
Mean values of EQ-5D(utility) for patients with hip, vertebral, and wrist fractures were 0.795, 0.882, and 0.934, respectively (Table 2). EQ-5D(utility) for patients with hip fractures was the lowest among the three groups, and there was a significant difference between the hip fracture and wrist fracture groups (p < 0.01 by Dunn’s test). There were no significant differences before the fracture between fracture types (neck and trochanteric) among patients with hip fractures, thoracic or lumbar fractures among patients with vertebral fractures, or surgical and nonsurgical treatment among patients with wrist fractures. Mean value of EQ-5D (utility) for patients with vertebral fractures admitted to hospital was 0.838 (median 0.887) and that for those not admitted was 0.973 (median 1.000), showing a significant difference (p = 0.024, by Mann–Whitney). There was no significant difference between these two groups for patients with wrist fractures.
Mean (median) values of age-adjusted EQ-5D(utility) in patients aged 65 years and over were 102.1% (100%), 111.7% (119.7%), and 116.9% (123.5%) for the hip, vertebral, and wrist fracture groups, respectively (Fig. 1).

Sequential changes in age-adjusted EQ-5D (utility) for patients aged 65 years and over. Left box represents hip fracture group, middle box represents vertebral fracture group, and right box represents wrist fracture group at each observational point (before fracture, at 2 weeks, 3 months, 6 months, and 1 year after the fracture). Data points represent EQ-5D (utility) age-adjusted to values for the Japanese general population aged 65 years and over. The vertical bars indicate the range (maximum and minimum), and the horizontal boundaries of the boxes represent the first quartile, median, and third quartile. +indicates mean values. *p < 0.05, **p < 0.01, ***p < 0.001 vs. wrist fracture (by Dunn’s test). a p < 0.01, b p < 0.05 vs. values before fracture (by Dunn’s test)
Sequential changes
Mean values of EQ-5D(utility) for patients with hip fractures at 2 weeks, 3 months, 6 months, and 1 year after the fracture were 0.373, 0.635, 0.634, and 0.680, respectively (Table 2). Those for patients with vertebral fractures were 0.531, 0.758, 0.746, and 0.838, respectively. Those for patients with wrist fractures were 0.717, 0.812, 0.873, and 0.881, respectively.
Among the vertebral fracture patients, there was no significant difference between patients with thoracic and lumbar fractures except at 6 months after the fracture, when EQ-5D(utility) was 0.827 for thoracic and 0.695 for lumbar fractures, with a significant difference (p = 0.028, by Mann–Whitney). There were no significant differences in EQ-5D (utility) throughout the observational period between neck and trochanteric fractures among patients with hip fractures or between surgical and nonsurgical treatment among patients with wrist fractures. In the vertebral and wrist fracture groups, there were no significant differences in EQ-5D (utility) between patients admitted and not admitted to the hospital at any time after the fracture.
Among the hip and wrist fracture groups at 3 months after the fracture, values of EQ-5D (utility) were significantly lower in patients who received analgesics than in those not receiving analgesics (p = 0.023 and p = 0.012, respectively, by Mann–Whitney); this was also the case in the vertebral fracture group at 1 year after the fracture (p = 0.031). However, there were no significant differences at the other observational points from 3 months to 1 year after the fracture. There were no significant differences in EQ-5D (utility) throughout the observational period between patients administered and not administered anti-osteoporosis drugs in all fracture groups.
Percent changes (means ± SD) of EQ-5D(utility) from baseline (before fracture) for patients with hip fracture at 2 weeks, 3 months, 6 months, and 1 year after the fracture were −55.1 ± 32.9% (range from −112.9% to 0%), −19.1 ± 22.8 (−55.6 to 10.6), −16.6 ± 24.8 (−80.5 to 31.9), and −12.9 ± 33.1 (−99.6 to 70.4), respectively. Those for vertebral fractures were −37.5 ± 23.6 (−94.8 to 0.0), −13.8 ± 22.3 (−54.1 to 30.2), −13.2 ± 25.7 (−42.3 to 87.6), and −7.8 ± 17.3 (−40.4 to 30.2), respectively. Those for wrist fractures were −22.2 ± 16.2 (−54.1 to 30.2), −12.9 ± 19.4 (−88.5 to 29.2), −5.9 ± 18.2 (−39.2 to 38.1), and −5.8 ± 15.9 (−36.9 to 44.3), respectively.
The reduction of EQ-5D(utility) during the observational period was greatest in the hip fracture group. In the wrist fracture group, EQ-5D (utility) at 6 months after the fracture showed recovery; however, values in the hip and vertebral fracture groups were significantly lower than before the fracture. One year after the fracture, EQ-5D (utility), values were not significantly different from prefracture values in the vertebral and wrist fracture groups, but remained significantly lower in the hip fracture group (Table 2).
Changes in age-adjusted EQ-5D (utility) for patients aged 65 years and over are presented in Fig. 1. The reduction of age-adjusted EQ-5D (utility) during the observational period was greatest in the hip fracture group; mean (median) values of percent changes from baseline at 2 weeks, 3 months, 6 months, and 1 year after the fracture were 46.9%(62.8%), 84.8%(80.1%), 83.2%(83.1%), and 88.1%(84.4%), respectively.
EQ-5D (profile)
Among the groups, the proportion of patients reporting problems in each of the five health domains of EQ-5D (profile) was higher in the hip fracture group than in the other two groups (Fig. 2). The difference between the hip fracture and other groups was most evident in the “mobility” and “usual activity” domains.

Sequential changes in health profile. Left box represents hip fracture group, middle box represents vertebral fracture group, and right box represents wrist fracture group at each observational point (before fracture, at 2 weeks, 3 months, 6 months, and 1 year after the fracture). Data points represent the percentage of patients reporting no problem, some problems, or extreme problems in each domain of EQ-5D profile
EQ-5D (vas)
Changes in EQ-5D (vas) were similar to those in EQ-5D (utility) (Fig. 3). There were no significant differences in EQ-5D (vas) between neck and trochanteric fractures among patients with hip fractures, between thoracic and lumbar fractures among patients with vertebral fractures, or between surgical and nonsurgical treatment among patients with wrist fractures throughout the observational period.

Sequential changes in VAS. Data represent means ± SD. *p < 0.05, **p < 0.01, ***p < 0.001 vs. wrist fracture, #p < 0.05 vs. vertebral fracture (Dunn’s test). a p < 0.01, b p < 0.05 vs. values before fracture (Dunn’s test)
Discussion
The present study demonstrates that among clinical fragility fractures, hip and vertebral fractures have the highest impact on patients’ HR-QOL. HR-QOL indices of these two fractures did not return to prefracture levels even one full year after the fracture occurrence. These findings are in accordance with previous reports [9, 17–19]. This is the first report to describe the prospective measurement of HR-QOL in Asian patients with incident fragility fractures.
Measurement of the effects of diseases on HR-QOL is of importance, since it allows a broad assessment of health domains not always captured in standard clinical or disease-specific assessments [20]. The EQ-5D is a generic measure of health status developed by the EuroQol Group and was originally standardized for use in England and Northern Europe. Translations have been undertaken in several languages; the official Japanese version of the EQ-5D instrument was developed in May 1998 (Japanese EuroQol Translation Team, 1998) [15]. EQ-5D is a self-completed, easy-to-use questionnaire that provides a health profile with a VAS [20]. Because this study targeted aged patients, we adopted EQ-5D for its simplicity and ease of use. EQ-5D also allows measurement of health utility, which forms the basis for estimation of quality-adjusted life years (QALY) [13].
Hip fractures cause acute pain and loss of function and nearly always require surgery. Recovery is slow and rehabilitation is often incomplete. We reported that the ratio of patients who could go out with assistance was 69% before hip fracture, whereas only 40% could go out at 1 year after the fracture [21]. Therefore, a considerable reduction of HR-QOL, as well as impairment of physical function, occurs after hip fractures [8, 9, 22–24]. A prospective, case-control study showed significant reductions of HR-QOL in the SF-36 domains: −51% for Physical Function, −24% for Vitality, and −26% for Social Function at 3 months after fracture [25]. Tidermark et al. demonstrated that EQ-5D scores decreased from 0.78 before the fracture to 0.59 at 4 months after surgery, and further decreased to 0.51 at 17 months after surgery, in relatively healthy elderly patients treated with internal fixation [10]. Our data from before and 3 months after fracture were very close to the scores of Tidermark et al. from before and 4 months after fracture, indicating that the impact of hip fracture on HR-QOL dose not differ much between the two populations in spite of the cultural differences.
The morbidity of vertebral fractures varies from mild cases, with only slight pain, to severe and multiple fracture cases with acute pain and many reoccurrences. Several studies have investigated the impact of prevalent or incident vertebral fractures on HR-QOL. A progressive worsening trend in HR-QOL with an increasing number of prevalent fractures has been observed [26]. Incident vertebral fractures have an adverse impact on HR-QOL regardless of symptomatology, and QOL score changes for patients with subclinical (absence of symptoms) vertebral fractures were intermediate between those for patients with clinical (symptomatic) vertebral fractures and patients without incident vertebral fractures [19]. The adverse health impact was most marked among patients with incident fractures who had a prevalent vertebral fracture, suggesting that the effect of multiple fractures on HR-QOL is cumulative [19, 27]. In the current study, only clinical fractures were evaluated, and we did not find any difference in the impact on HR-QOL between patients with and without prevalent vertebral fractures. This might be due to the small number of patients; only four patients presented with prevalent vertebral fractures. We showed a statistical difference in HR-QOL between patients with thoracic and lumbar fractures that is in agreement with previous studies [26]. This difference occurs because lumbar fractures are more often symptomatic than thoracic fractures, due to stabilization of the thoracic spine by the rib cage.
Wrist fractures cause pain and loss of function, but fracture healing and regain of function are usually favorable. Dolan et al. observed considerable loss in the first 3 months, but recovery was fast, and the HR-QOL impairment was small [28]; these findings are compatible with our observations.
In a previous study, each of the five dimensions or domains of the EQ-5D (profile) were collected from a representative sample of the Japanese general population aged 65 years and over [16]. The percentages reporting “some” or “extreme” problems were 29.2% and 0.8% for mobility, 6.0% and 1.5% for self-care, 21.5% and 3.4% for usual activity, 40.3% and 2.0% for pain/discomfort, and 15.5% and 1.1% for anxiety/depression, respectively. Compared with these data, the percentage of patients complaining of “some” or “extreme” problems in each domain seemed to recover to normal levels by 6 months in the wrist fracture group, and by 1 year in the vertebral fracture group; however, in the hip fracture group, a substantially higher percentage of patients complained of “some” or “extreme” problems in all domains throughout the observational period.
In North America, QALY loss in the first year after hip fracture was 0.4681, mainly due to the hospital and nursing home stay, whereas the QALY loss after a vertebral fracture with severe pain was up to 0.5000 [29, 30]. This type of analysis is indispensable, but has not been done in Japan, since to date, there have been no data available to estimate QALY loss after fragility fractures among the Japanese population. The data presented in this study could make possible a cost-utility analysis of osteoporosis therapies.
This study had several limitations. First, the number of the subjects was limited, which might introduce some sampling biases. In this study, patients who could not complete the EQ-5D questionnaire were not enrolled, which could lead to overestimation of HR-QOL scores for hip and vertebral fracture patients. Second, the dropout rate could have affected the results. Most patients who dropped out were in the wrist fracture group; many of them fully recovered and thereafter lost contact. This could have led to underestimation of HR-QOL scores. Third, the severity of the fracture may affect QOL status, i.e., patients with more severe fractures may become more pessimistic, while patients with slight fractures may be more optimistic even at the time of recollection. Therefore, patients with more severe disabling fractures may overestimate prefracture quality of life. Hospitalization or residence at the evaluation point might affect the HR-QOL scores: hospitalized patients showed lower prefracture QOL scores for vertebral fractures, and patients who received analgesics tended to have lower QOL scores. The findings could represent possible biases in the pre- and postfracture QOL assessment. Finally, further studies are required to assess the influence of comorbidity on HR-QOL scores in patients with osteoporosis-related fractures.
In conclusion, HR-QOL data obtained in this study showed that loss of quality of life is more severe after hip or vertebral fractures than after wrist fracture. HR-QOL was not completely restored in patients suffering from hip fracture. Collectively, these data suggest that prevention of osteoporotic fractures is of the utmost importance for maintaining quality of life.
References
Lofman O, Berglund K, Larsson L et al (2002) Changes in hip fracture epidemiology: redistribution between ages, genders and fracture types. Osteoporos Int 13:18–25
Jaglal SB, Weller I, Mamdani M et al (2005) Population trends in BMD testing, treatment, and hip and wrist fracture rates: are the hip fracture projections wrong? J Bone Miner Res 20:898–905
Melton LJ 3rd, Atkinson EJ, Madhok R (1996) Downturn in hip fracture incidence. Public Health Rep 111:146–150 discussion 151
Kannus P, Niemi S, Parkkari J et al (2006) Nationwide decline in incidence of hip fracture. J Bone Miner Res 21:1836–1838
Rowe SM, Song EK, Kim JS et al (2005) Rising incidence of hip fracture in Gwangju City and Chonnam Province, Korea. J Korean Med Sci 20:655–658
Hagino H, Katagiri H, Okano T et al (2005) Increasing incidence of hip fracture in Tottori Prefecture, Japan: trend from 1986 to 2001. Osteoporos Int 16:1963–1968
Hagino H, Yamamoto K, Ohshiro H et al (1999) Changing incidence of hip, distal radius, and proximal humerus fractures in Tottori Prefecture, Japan. Bone 24:265–270
Boonen S, Autier P, Barette M et al (2004) Functional outcome and quality of life following hip fracture in elderly women: a prospective controlled study. Osteoporos Int 15:87–94
Brenneman SK, Barrett-Connor E, Sajjan S et al (2006) Impact of recent fracture on health-related quality of life in postmenopausal women. J Bone Miner Res 21:809–816
Tidermark J, Zethraeus N, Svensson O et al (2002) Femoral neck fractures in the elderly: functional outcome and quality of life according to EuroQol. Qual Life Res 11:473–481
Marcus R, Wong M, Heath H 3rd et al (2002) Antiresorptive treatment of postmenopausal osteoporosis: comparison of study designs and outcomes in large clinical trials with fracture as an endpoint. Endocr Rev 23:16–37
Brazier JE, Green C, Kanis JA (2002) A systematic review of health state utility values for osteoporosis-related conditions. Osteoporos Int 13:768–776
Dolan P, Gudex C, Kind P et al (1996) The time trade-off method: results from a general population study. Health Econ 5:141–154
Ikeda S, Ikegami N (2001) Preference-based measure(EQ-5D) In: Ikegami N, Fukuhara S, Shimozuma K, Ikeda S (eds) QOL evaluation handbook for clinical practice(in Japanese). Igakushoin, Tokyo, pp 14–18
Ikeda S, Ikegami N (1999) Health status in Japanese population: results from Japanese EuroQol study. Iryou to Shakai 9:83–92
Nawata S, Yamad Y, Ikeda S et al (2000) EuroQol study of the elderly general population: Relationship with IADL and other attributes. Iryou to Shakai (in Japanese) 10:75–86
Hallberg I, Rosenqvist AM, Kartous L et al (2004) Health-related quality of life after osteoporotic fractures. Osteoporos Int 15:834–841
Lips P, van Schoor NM (2005) Quality of life in patients with osteoporosis. Osteoporos Int 16:447–455
Oleksik AM, Ewing S, Shen W et al (2005) Impact of incident vertebral fractures on health related quality of life (HRQOL) in postmenopausal women with prevalent vertebral fractures. Osteoporos Int 16:861–870
Dhillon V, Hurst N, Hannan J et al (2005) Association of low general health status, measured prospectively by Euroqol EQ5D, with osteoporosis, independent of a history of prior fracture. Osteoporos Int 16:483–489
Sakamoto K, Nakamura T, Hagino H et al (2006) Report on the Japanese Orthopaedic Association’s 3-year project observing hip fractures at fixed-point hospitals. J Orthop Sci 11:127–134
Cranney AB, Coyle D, Hopman WM et al (2005) Prospective evaluation of preferences and quality of life in women with hip fractures. J Rheumatol 32:2393–2399
Hall SE, Williams JA, Senior JA et al (2000) Hip fracture outcomes: quality of life and functional status in older adults living in the community. Aust N Z J Med 30:327–332
Fierens J, Broos PL (2006) Quality of life after hip fracture surgery in the elderly. Acta Chir Belg 106:393–396
Randell AG, Nguyen TV, Bhalerao N et al (2000) Deterioration in quality of life following hip fracture: a prospective study. Osteoporos Int 11:460–466
Oleksik A, Lips P, Dawson A et al (2000) Health-related quality of life in postmenopausal women with low BMD with or without prevalent vertebral fractures. J Bone Miner Res 15:1384–1392
Cockerill W, Lunt M, Silman AJ et al (2004) Health-related quality of life and radiographic vertebral fracture. Osteoporos Int 15:113–119
Dolan P, Torgerson D, Kakarlapudi TK (1999) Health-related quality of life of Colles’ fracture patients. Osteoporos Int 9:196–199
Lips P, Cooper C, Agnusdei D et al (1999) Quality of life in patients with vertebral fractures: validation of the Quality of Life Questionnaire of the European Foundation for Osteoporosis (QUALEFFO). Working Party for Quality of Life of the European Foundation for Osteoporosis. Osteoporos Int 10:150–160
NOF (1998) Osteoporosis: review of the evidence for prevention, diagnosis and treatment and cost-effectiveness analysis. Introduction. Osteoporos Int 8(Suppl 4):S7–S80
Acknowledgments
The authors thank Masatoshi Nakashima, M.D., Masaaki Shimizu, M.D., Kimiko Tsuda, M.D., and Noboru Yamagata, M.D., for their help and support.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hagino, H., Nakamura, T., Fujiwara, S. et al. Sequential change in quality of life for patients with incident clinical fractures: a prospective study. Osteoporos Int 20, 695–702 (2009). https://doi.org/10.1007/s00198-008-0761-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-008-0761-5