
Abstract
Introduction
We evaluate reference data to examine whether there are sex-, age-, height-, weight- and BMI-related differences of quantitative ultrasound parameters (QUS) for healthy Chinese children and adolescents.
Methods
A total of 726 healthy children and adolescents (360 male and 366 female) aged from 10–21 years were examined with a Lunar Achilles Express densitometer. The measurements on the right heel included speed of sound (SOS), broadband ultrasound attenuation (BUA), and a calculated stiffness index (SI).
Results
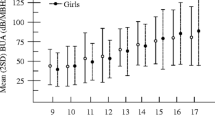
Our results found that there were no significant differences for BUA, SOS and SI between males and females, except in the age range of 12 to 13 years. The values of all parameters were significantly higher in the 12-year-old females compared to males, and BUA values were significantly higher in 13-year-old females compared to males. A spurt in QUS parameters were observed at 12 years in females and at 14 years in males. A steady increase of BUA, SOS, and SI was seen with increasing body height and weight in both sexes.
Conclusion
In conclusion, the present results can be used as reference data for children and adolescents in China.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In the past, the bone status in adults received much attention. The evaluation of bone status is usually performed by dual-energy X-ray absorptiometry (DXA) or quantitative ultrasound (QUS). Due to its radiation-free, low-cost, simple, and portable advantages, QUS is more adaptable to large-scale survey. Until recently, normal calcaneal QUS of adults has already been determined and used in screening for osteoporosis and for evaluation of fracture risk. However, less attention has been paid to the analysis of developing bone during growth in childhood. Assessing the bone health of children is becoming increasingly important because the attainment of a high peak bone mass seems to decrease the risk of osteoporosis later in life [1, 2]. In addition, the assessment of skeletal development status in children and adolescents has important clinical implications. Various congenital or acquired diseases influence the bone development in childhood and adolescence. It is necessary to diagnose alterations of bone for an optimal therapy and its control. Thus, there is increasing interest in assessing the bone health of youths.
Although the physical size of the calcaneus relative to the ultrasound beam diameter is an important factor influencing the precision of bone mass measurements due to the immaturity of bone development in children, the adjusted midregion of the calcaneus relative to the device could decrease this influence [3–7]. And many cross-sectional and longitudinal studies supported the validity of using QUS to assess bone health in youths [1, 2, 8–16]. Therefore, this method might be a good alternative to assess bone density in growing children.
Up to now, a number of studies in the USA and Europe have established the reference data on QUS variables in children and adolescents despite different measurement regions such as calcaneus, phalanx, or tibia [5, 10, 17, 18]. To our knowledge, however, there have been very few such studies in Chinese children and adolescents [19, 20] and no standard values have been established in mainland Chinese children and adolescents. Thus, the purpose of this study is to establish the reference ranges for calcaneal QUS parameters in 10 to 21-year-old Chinese children and adolescents and to examine the possible differences related to sex, age, height, and weight.
Subjects and methods
Subjects
A total number of 726 (360 male and 366 female) healthy Chinese children and adolescents aged 10–21 years participated in this study. The subjects were randomly recruited from local elementary and high schools in three provinces of China: Zhejiang, Guangxi, and Hebei, from August 2003 to September 2004. An extensive clinical history was obtained from parents and the subjects, none of the participants were taking medications or had any diseases affecting bone metabolism. Written informed consent was obtained from all participants and from parents of subjects under 18 years of age, and the study was approved by the Ethics Committee of Peking Union Medical College. The headmaster and the teachers of the enrolled schools approved the study. The subjects were divided into groups by age, height, and body weight (Tables 1, 2, and 3).
Anthropometric measurements
Data concerning sex, age, height, and weight were collected. Height of the children and adolescents was measured with the same portable stadiometer and body weight was measured with the same electronic scale, with the subjects in underwear and without shoes. The stadiometer and the electronic scale were calibrated daily before the measurements in order to decrease measurement errors. The height of each subject, measured to the nearest 0.1 cm, and weight was recorded to the nearest 0.1 kg. Body mass index (BMI) was calculated as weight (kg) divided by height squared (m2).
Quantitative ultrasound measurements
Calcaneal QUS variables were measured with the Lunar Achilles ultrasonometer (GE Healthcare, Madison, WI, USA) according to the manufacture’s instructions. The Achilles densitometer has been shown to provide good precision in adults and youths [5, 7, 21, 22]. It measures broadband ultrasound attenuation (BUA) (decibels/megahertz) and speed of sound (SOS) (meters/second). A third parameter, the stiffness index (SI), derived for BUA and SOS , was calculated automatically in the Achilles system according to the following equation: \( {\text{SI}} = {\left( {0.67 \times {\text{BUA}}} \right)} + {\left( {0.28 \times {\text{SOS}}} \right)} - 420 \). The calculated SI parameter normalizes the BUA and SOS measurements [23]. For measurement, the right heel was placed in the measurement chamber with the lid as a calf support. The midregion of the calcaneus relative to the transducers was adjusted by placing none to three shims under the foot, as previously described [4–6]. The foot was positioned using a special positioning procedure. For quality control, a heel phantom provided by the manufacturer was scanned daily prior to the measurements. Two trained operators performed all the measurements. The coefficients of variation (CVs) for within-day measurements have previously been reported to be 1.8% for BUA, 0.3% for SOS, and 1.9% for SI. The CVs for between-day measurements were 0.6, 1.8, and 3.2% for these parameters, respectively [10].
Statistical analysis
The results are expressed as the mean±standard deviation (SD). Data management and analyses were performed using the software package SPSS for windows software programs version 11.0 (Statistical Package for Social Sciences, SPSS 11.0, Inc., Chicago, Illinois, USA). A linear regression model and Pearson’s correlation coefficients were calculated to examine the relations between the ultrasound parameters and age, height, weight, and BMI. Comparisons between various age groups were by ANOVA. The differences were considered statistically significant for p < 0.05.
Results
Basic characteristics of the study population
The heights and weights of the subjects were collected as basic data. Table 1 shows the descriptive characteristics of the study subjects and the comparisons between age, height, weight, and BMI. The overall age mean was 15.0 ± 3.0 years (15.0 ± 3.0 for males and 15.0 ± 3.1 for females), with no statistical differences between the two groups. The males were heavier (51.6 ± 12.2 kg versus 47.0 ± 8.5 kg) and taller (162.1 ± 12.4 cm versus 155.6 ± 7.2 cm) than females (p = 0.000 in both cases). BMI was similar, with no statistical differences between males and females (19.3 ± 2.6 kg/m2 versus 19.3 ± 2.6 kg/m2). There were progressive increases in height, weight, and BMI for both sexes with age. The peak height velocity (PHV; cm/year) occurred at 13 years in males and at 11 years in females. The peak weight velocity (PWV; kg/year) occurred at 13–14 years in males and at 12 years in females. Females were significantly taller than males at the age of 11. While for subjects over age 14, males were significantly taller and heavier than females.
QUS parameters in relation to age, sex, height, weight, and BMI
The three parameters (BUA, SOS, and SI) all increased with age throughout childhood and adolescence and reached a plateau by age 17–18 and 19–20 for males and females, respectively. After the plateau, there was a decline trend in both sexes. A spurt in QUS parameters was observed at 12 years in females and at 14 years in males. The linear regression showed the mean increasing rates of the three QUS values for young males were 2.315 dB/MHz/year for BUA, 2.962 m/s/year for SOS and 2.366/yr for SI, respectively. And those of young females were 1.552 dB/MHz/year for BUA, 2.340 m/s/year for SOS and 1.684/year for SI, respectively. The total age-related increase between 10 and 21 years was 26.9% for BUA, 2.1% for SOS, 32.8% for SI in young males; 17.6% for BUA, 1.6% for SOS, 22.7% for SI in young females. The increases of three QUS values in males were significantly higher than females.
All parameters were significantly higher in the 12-year-old females than in males at the same age and BUA values were significantly higher in 13-year-old females than in males. In the other age groups, there were no significant differences for BUA, SOS, and SI between males and females (Table 1). A steady increase of BUA, SOS, and SI was seen with increasing body height in both sexes. The values of all parameters were significantly higher in females than in males in the 150–159 cm groups in height (Table 2). A steady increase of BUA, SOS, and SI was seen with increasing body weight in both sexes. BUA and SI values were significantly higher in females than in males in the 40–49 kg group (Table 3).
Distributions and curve-fitting models of QUS parameters
Figures 1 and 2 display scatter distributions and curve-fitting models of age-related QUS parameters in male and female children and adolescents, respectively. We adopted linear, logarithmic, quadratic, cubic, compound, power, growth, and exponential regression models to concurrently determine age-related QUS variations. We found that the quadratic or cubic regression model fit best, i.e., R2 was consistently maximized.

Scatterplots of age-related changes of QUS parameters (BUA, SOS and SI) in healthy mainland Chinese females. The center line represents the regression of QUS parameter on age, and upper and lower lines represent 95% confidence limits. a The relation between BUA and age, BUA = 39.595895 + 7.723146 (age) − 0.197624 (age)2. (R2 = 0.09110, p < 0.001). b The relation between SOS and age. SOS = 1490.696631 + 7.399622 (age) − 0.006662 (age)3. (R2 = 0.04136, p < 0.001). c The relation between SI and age, SI = 34.645363 + 5.103739 (age) − 0.004531 (age)3. (R2 = 0.09421, p < 0.001)

Scatterplots of age-related changes of QUS parameters (BUA, SOS, and SI) in healthy mainland Chinese males. The center line represents the regression of QUS parameter on age and upper and lower lines represent 95% confidence limits. a The relation between BUA and age, BUA = 26.292938 + 6.970507 (age) − 0.006099 (age)3.(R2 = 0.22991, p < 0.001). b The relation between SOS and age, SOS = 1468.581474 + 8.728582 (age) − 0.007519 (age)3.(R2 = 0.05029, p < 0.001). c The relation between SI and age, SI = 8.806913 + 7.071054 (age) − 0.006153 (age)3. (R2 = 0.16201, p < 0.001)
Relationship between QUS and age, height, weight, and BMI
Correlation analysis showed significant relationships between measured QUS variables. Although the correlation coefficient between BUA and SOS was low (r = 0.405), there was still statistic significance (p = 0.000).
Associations between the subjects’ basic data (age, height, weight, and BMI) for both sexes and the three QUS parameters were examined by Pearson correlations (Table 4). Three QUS parameters correlated positively with age, height, weight, and BMI except that SOS did not correlate with weight and BMI for males, and SOS with height for females. The stepwise multiple linear regression analyses (Table 5) showed height and BMI were less important factors for QUS in both males and females. For both sexes, SOS was significantly dependent only on age. SI for males was also a function of age. BUA for both sexes and SI for females were both dependent on age and weight.
Discussion
The calcaneus is the commonest skeletal site of ultrasonometry since there is only a thin soft tissue (relatively consistent) covering the bone and this bone is a more than 90% trabecular, which has a high metabolic activity and is more responsive to age-, disease-, or therapy-induced bone alterations than cortical bone [9]. Furthermore, it is easily accessible. The most commonly measured calcaneus QUS parameters are BUA, SOS, and SI. It has been proposed that BUA is determined predominantly by the scatter of sound waves and reflects the spatial orientation of the bone trabeculae where the value increases with greater trabecular complexity [22]. SOS, on the other hand, is related to the ultrasound velocity, assuming a constant heel stiffness [24]. Besides bone mass, BUA and SOS have been suggested to measure bone elasticity and microarchitecture [25]. SI is a third parameter of QUS and is derived from the combination of BUA and SOS. Hans et al. [26] reported a better correlation between QUS SI and DXA BMD than between the latter and BUA or SOS. However, Jaworski et al. [5] compared 71 normal and 18 osteopenic children and reported that BUA had high correlations to BMD (r, ∼0.83), and SOS the lowest (r, ∼0.67), SI was intermediate (r, ∼0.80).
In the present study, the correlation analysis between three QUS parameters showed that the correlation between BUA or SOS and SI was higher than that between SOS and BUA in both sexes. This result may be due to different representations of SOS and BUA (as mentioned above, SOS and BUA represent ultrasound speed and broadband ultrasound attenuation, respectively) and the derivation of SI from a formula based on SOS and BUA. Accordingly, the changes in the three QUS parameters with sex, age, and growth variables were not completely identical.
Age, weight, and height were almost significantly positively associated with all QUS parameters, as has been observed in other studies [5, 27–32]. But there were exceptions, for example, our results showed that SOS did not correlate with weight and BMI for males, and SOS did not correlate with height for females. Stepwise multiple linear regression has shown different determinants for SOS and BUA. For SOS, the strongest factor was age; For BUA, age and weight were both the influencing factors; and for SI in males, age was the most important factor, and in females, age and weight were both the influencing factors. Comparatively, height and BMI were not effective influencing factors on QUS. Van den Bergh et al. [33] also investigated the relationship of BUA to foot dimensions and pubertal stage in 491 healthy Caucasian children and adolescents aged between 10 and 21 years. They indicated that foot length was also an independent predictor of the ultrasound parameter in males and not in females. In our study, we did not examine the foot dimensions and pubertal stage, which is a limitation in the present study.
Although three QUS parameters all significantly correlated with age and the change trends of the QUS values with age were similar, their increasing percentages with age were different. The total increasing rates of QUS for young males between 10 and 21 years were 26.9% for BUA, 2.1% for SOS and 32.8% for SI per year, respectively. And those of young females were 17.6% for BUA, 1.6% for SOS and 22.7% for SI per year, respectively. The results indicated the magnitude of gains varied considerably depending on the QUS parameter examined. Sawyer et al. [11] found that mean values for BUA increased by 40%, mean SOS by only 4%, and mean SI by 80% between ages 7 and 18. Other studies have also shown gains of 22–62% in calcaneus BUA between children and late adolescent [30, 31, 34]; Increases in calcaneus SOS during puberty reported previously were approximately 4–6% [30, 35]. Van den Bergh et al. [33] stated in their conclusions that “BUA increased significantly with age in both sexes, SOS increased with age in both males and females, but the increase was small and not statistically significant in males”. The differences of three QUS values in the increasing rate may be due to different representations of them (SOS and BUA represent ultrasound speed and broadband ultrasound attenuation, respectively) and SOS is not sensitive to the changes of skeletal status in youths. The broad range of values in different studies most likely reflects differences in the race, the number of subjects and method of measurement. The inconsistent increasing rate in both sexes may reflect differences of the growth during puberty between males and females.
In our results, for three QUS values, there was a clear spurt at 12 years of age in females and 14 years of age in males. Furthermore, the QUS spurts were observed to have occurred 1 year after the age of peak height velocity (PHV) in both sexes, and there was an age-related delay in QUS increases compared to the linear growth pattern. These results are in agreement with many studies, which confirmed that QUS of the calcaneus is influenced by the growth process [2, 17, 36, 37]. We also indicated QUS parameters of both genders in 10 to 11-year--old individuals were very similar, while in females at the age of 12 and 13 years, measurements were higher than in males, which is probably due to the fact that puberty occurs physiologically at an earlier chronological age in females. It is well known, in fact, that in adolescence bone mass is heavily influenced by sex steroids which increase dramatically in this age period. Our result was consistent with another study in Chinese youths with DXA, which showed that BMD in individuals younger than 12 years of age has no gender difference from the lateral spine, neck, and trochanter of femur, and total hip [38]. Other studies using QUS at patella and proximal phalanges of the hand found that higher values in females compared to males in middle puberty [1, 39]. By contrast, Sawyer et al. [11] examined 311 healthy American children and adolescents and found that gender differences were not significant. The probable explanation for this difference is relative small cohort size.
Peak bone mass is the highest level of bone mass achieved as a result of normal growth, and is well recognized risk factor for osteoporosis later in life. Thus, increasing peak bone mass during childhood and adolescence is considered as important for osteoporosis prevention as slowing bone loss in older ages. Despite the known importance of peak bone mass, the age at which peak values are reached remains controversial. Some studies indicated that peak bone mass is reached as late as 35 years of age. However, other studies have shown that more than 85% of peak skeletal mass is accrued by the age of 18 years, making bone growth during childhood and adolescence a critical process [40, 41]. W Liu et al. [42] reported the QUS values of Chinese males and females peaked after 20 years and the values of youths before 20 years can reach more than 90% of the peak. Many reports have also indicated that peak bone mass is achieved between 16–18 years of age [41, 43–45]. Similarly, our results found that QUS values peaked by late adolescence after which there was a decline trend in both sexes.
In our study, the pubertal staging using the method of Tanner was not performed. The unknown pubertal status of the subjects is a limitation of this study. In addition, studies have shown that dairy intake and physical activity growth rate also influence QUS parameters [46]. The current study focused only on a healthy population in cross-sectional design, and data on bone QUS parameters longitudinal changes due to dairy intake, physical activity, disease or medication during childhood and adolescences should be further investigated.
Despite these limitations, the present study presents the important data of QUS indices measured with Achilles for healthy mainland Chinese children and adolescents, which could serve as reference data for evaluating the bone status of young people. We have also presented the relationships of the major determinants of bone mass, that is, age, height and body weight, to QUS. We conclude in the present study that, we determined, for the first time, the normative values of calcaneal QUS values in mainland Chinese children and adolescents.
References
Lappe JM, Stegman M, Davies KM, Barber S, Recker RR (2000) A prospective study of quantitative ultrasound in children and adolescents. J Clin Densitom 3:167–175
Kaga M, Takahashi K, Suzuki H, Matsueda M, Moriwake T, Miyatake N (2002) Ultrasound assessment of tibial cortical bone acquisition in Japanese children and adolescents. J Bone Miner Metab 20:111–115
Hans D, Njeh CF, Genant HK, Meunier PJ (1998) Quantitative ultrasound in bone status assessment. Rev Rhum Engl Ed 65:489–498
Fielding KT, Backrach LK, Hudes ML, Crawford PB, Wang MC (2002) Ethnic differences in bone mass of young women vary with method of assessment. J Clin Densitom 5:229–238
Jaworski M, Lebiedowski M, Lorenc RS, Trempe J (1995) Ultrasound bone measurement in pediatric subjects. Calcif Tissue Int 56:368–371
Tsuda-Futami E, Hans D, Njeh CF, Fuerst T, Fan B, Li J, He YQ, Genant HK (1999) An evaluation of a new gel-coupled ultrasound device for the quantitative assessment of bone. Br J Radiol 72:691–700
Lees B, Stevenson JC (1993) Preliminary evaluation of a new ultrasound bone densitometer. Calcif Tissue Int 53:149–152
Volta C, Bagni B, Iughetti L, Rossi M, Corazzari T, Bagni I, Bernasconi S (2004) Bone mass evaluated by calcaneous ultrasound and radial peripheral computed tomography in 726 youngsters. Acta Paediatr 93:747–751
Wunsche K, Wunsche B, Fahnrich H, Mentzel HJ, Vogt S, Abendroth K (2000) Ultrasound bone densitometry of the os calcis in children and adolescents. Calcif Tissue Int 67:349–355
Vignolo M, Brignone A, Mascagni A, Ravera G, Biasotti B, Aicardi G (2003) Influence of age, sex, and growth variables on phalangeal quantitative ultrasound measures: a study in healthy children and adolescents. Calcif Tissue Int 72:681–688
Sawyer A, Moore S, Fielding KT, Nix DA, Kiratli J, Bachrach LK (2001) Calcaneus ultrasound measurements in a convenience sample of healthy youth. J Clin Densitom 4:111–120
Halaba ZP, Pluskiewicz W (2004) Quantitative ultrasound in the assessment of skeletal status in children and adolescents. Ultrasound Med Biol 30:239–243
Halaba Z, Pluskiewicz W (1997) The assessment of development of bone mass in children by quantitative ultrasound through the proximal phalanxes of the hand. Ultrasound Med Biol 23:1331–1335
Ikeda Y, Iki M, Morita A, Aihara H, Kagamimori S, Kagawa Y, Matsuzaki T, Yoneshima H, Marumo F (2004) Ultrasound bone densitometry of the calcaneus, determined with Sahara, in healthy Japanese adolescents: Japanese Population-based Osteoporosis (JPOS) Study. J Bone Miner Metab 22:248–253
Vignolo M, Parodi A, Mascagni A, Torrisi C, De Terlizzi F, Aicardi G (2006) Longitudinal assessment of bone quality by quantitative ultrasonography in children and adolescents. Ultrasound Med Biol 32:1003–1010
Zadik Z, Sinai T, Borondukov E, Zung A, Yaniv I, Reifen R (2005) Longitudinal monitoring of bone accretion measured by quantitative multi-site ultrasound (QUS) of bones in patients with delayed puberty (a pilot study). Osteoporos Int 16:1036–1041
Barkmann R, Rohrschneider W, Vierling M, Troger J, de TF, Cadossi R (2002) German pediatric reference data for quantitative transverse transmission ultrasound of finger phalanges. Osteoporos Int 13:55–61
Lequin MH, van Rijn RR, Robben SG, Hop WC, van Kuijk C (2000) Normal values for tibial quantitative ultrasonometry in Caucasian children and adolescents (aged 6 to 19 years). Calcif Tissue Int 67:101–105
Cheng JC, Leung SS, Lee WT, Lau JT, Maffulli N, Cheung AY (1998) Determinants of axial and peripheral bone mass in Chinese adolescents. Arch Dis Child 78:524–530
Liao XP, Zhang WL, He J, Sun JH, Huang P (2005) Bone measurements of infants in the first 3 months of life by quantitative ultrasound: the influence of gestational age, season, and postnatal age. Pediatr Radiol 35:847–853
Faulkner KG, McClung MR, Coleman LJ, Kingston-Sandahl E (1994) Quantitative ultrasound of the heel: correlation with densitometric measurements at different skeletal sites. Osteoporos Int 4:42–47
Schott AM, Hans D, Sornay-Rendu E, Delmas PD, Meunier PJ (1993) Ultrasound measurements on os calcis: precision and age-related changes in a normal female population. Osteoporos Int 3:249–254
Hans D, Arlot ME, Schott AM, Roux JP, Kotzki PO, Meunier PJ (1995) Do ultrasound measurements on the os calcis reflect more the bone microarchitecture than the bone mass?: a two-dimensional histomorphometric study. Bone 16:295–300
Njeh CF, Boivin CM, Langton CM (1997) The role of ultrasound in the assessment of osteoporosis: a review. Osteoporos Int 7:7–22
Prins SH, Jorgensen HL, Jorgensen LV, Hassager C (1998) The role of quantitative ultrasound in the assessment of bone: a review. Clin Physiol 18:3–17
Hans D, Dargent-Molina P, Schott AM, Sebert JL, Cormier C, Kotzki PO, Delmas PD, Pouilles JM, Breart G, Meunier PJ (1996) Ultrasonographic heel measurements to predict hip fracture in elderly women: the EPIDOS prospective study. Lancet 348:511–514
Mughal MZ, Ward K, Qayyum N, Langton CM (1997) Assessment of bone status using the contact ultrasound bone analyser. Arch Dis Child 76:535–536
Alenfeld FE, van de Loo I, Diessel E, Felsenberg D (1997) Influence of factors on quantitative ultrasound measurements at the calcaneus in children in a German reference population. Bone 20:37S
Carr AJ, Thompson PW, Jones C, Jenkins EJE (1995) Heel ultrasound measurements on 244 peri menarchal schoolgirls. Am Coll Rheum 38:S358
Lum CK, Wang MC, Moore E, Wilson DM, Marcus R, Bachrach LK (1999) A comparison of calcaneus ultrasound and dual X-ray absorptiometry in healthy North American youths and young adults. J Clin Densitom 2:403–411
Lappe JM, King SA, Lypaczewski MG (1999) Normative values for quantitative ultrasound at the os calcis in children and adolescents. J Bone Miner Res 14(Suppl 1):S256
Sundberg M, Gardsell P, Johnell O, Ornstein E, Sernbo I (1998) Comparison of quantitative ultrasound measurements in calcaneus with DXA and SXA at other skeletal sites: a population-based study on 280 children aged 11–16 years. Osteoporos Int 8:410–417
van den Bergh JP, Noordam C, Ozyilmaz A, Hermus AR, Smals AG, Otten BJ (2000) Calcaneal ultrasound imaging in healthy children and adolescents: relation of the ultrasound parameters BUA and SOS to age, body weight, height, foot dimensions and pubertal stage. Osteoporos Int 11:967–976
Salle A, Aubry C, Pascal-Bigneron V, Kuntz C, Locuty J, Leclere J, Weryha G (1998) Age-related changes in SOS and BUA during children, using SAHARA ultrasound bone densitometer. Bone 23:S318
Schonau E, Radermacher A, Wentzlik U, Klein K, Michalk D (1994) The determination of ultrasound velocity in the os calcis, thumb and patella during childhood. Eur J Pediatr 153:252–256
Suwa S, Tachibana K, Maesaka H, Tanaka T, Yokoya S (1992) Longitudinal standards for height and height velocity for Japanese children from birth to maturity. Clin Pediatr Endocrinol 1:5–13
Bailey DA (1997) The Saskatchewan Pediatric Bone Mineral Accrual Study. Bone mineral acquisition during the growing years. Int J Sports Med 18:191–194
Wu XP, Yang YH, Zhang H, Yuan LQ, Luo XH, Cao XZ, Liao EY (2005) Gender differences in bone density at different skeletal sites of acquisition with age in Chinese children and adolescents. J Bone Miner Metab 23:253–260
Baroncelli GI, Federico G, Bertelloni S, de Terlizzi F, Cadossi R, Saggese G (2001) Bone quality assessment by quantitative ultrasound of proximal phalanxes of the hand in healthy subjects aged 3–21 years. Pediatr Res 49:713–718
Matkovic V, Jelic T, Wardlaw GM, Ilich JZ, Goel PK, Wright JK, Andon MB, Smith KT, Heaney RP (1994) Timing of peak bone mass in Caucasian females and its implication for the prevention of osteoporosis. J Clin Invest 93:799–808
Bonjour JP, Theintz G, Buchs B, Slosman D, Rizzoli R (1991) Critical years and stages of puberty for spinal and femoral bone mass accumulation during adolescence. J Clin Endocrinol Metab 73:555–563
Liu W, Xu CL, Zhu ZQ, Wang W, Han SM, Zu SY, Zhu GJ (2006) Characteristics of calcaneus quantitative ultrasound normative data in Chinese mainland men and women. Osteoporos Int 17:1216–1224
Theintz G, Buchs B, Rizzoli R, Slosman D, Clavien H, Sizonenko PC, Bonjour JP (1992) Longitudinal monitoring of bone mass accumulation in healthy adolescents: evidence for a marked reduction after 16 years of age at the levels of lumbar spine and femoral neck in female subjects. J Clin Endocrinol Metab 75:1060–1065
Takahashi Y, Minamitani K, Kobayashi Y, Minagawa M, Yasuda T, Niimi H (1996) Spinal and femoral bone mass accumulation during normal adolescence: comparison with female patients with sexual precocity and with hypogonadism. J Clin Endocrinol Metab 81:1248–1253
Recker RR, Davies KM, Hinders SM, Heaney RP, Stegman MR, Kimmel DB (1992) Bone gain in young adult women. JAMA 268:2403–2408
Novotny R, Daida YG, Grove JS, Acharya S, Vogt TM, Paperny D (2004) Adolescent dairy consumption and physical activity associated with bone mass. Prev Med 39:355–360
Acknowledgments
This study was supported by the Special Fund for Key Basic Research Project of the Ministry of National Science and Technology China (2001DEA30031, 2002DIA40018). The authors express special appreciation for the support of all the school principals and teachers involved, and the excellent cooperation of all the participating students and their parents in Zhejiang, Hebei, and Guangxi provinces.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Zhu, ZQ., Liu, W., Xu, CL. et al. Ultrasound bone densitometry of the calcaneus in healthy Chinese children and adolescents. Osteoporos Int 18, 533–541 (2007). https://doi.org/10.1007/s00198-006-0276-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-006-0276-x