
Abstract
Introduction
Quantitative ultrasound (QUS) assessment at the calcaneus, as a safe and reliable method for evaluating skeletal status, is rapidly gaining in popularity. Assessment by QUS provides three parameters of skeletal status: broadband ultrasound attenuation (BUA), speed of sound (SOS) and derived data-stiffness index (STI). The objective of the present study was firstly to determine the normative QUS data on healthy Chinese mainland men and women and secondly to investigate the effects of sex, age and body size on these three QUS parameters.
Methods
A study cohort consisting of 725 healthy Chinese women and 568 men aged 10–83 years participated in this investigation. The three QUS parameters all exhibited a characteristic mild rise-then-fall pattern with increasing age in both sexes. Younger men and women had similar QUS values, while older women had lower values than older men. Age-related differences were more pronounced among females. Pearson’s correlation and regression analysis showed that weight was a major determinant of QUS in both sexes, along with age.
Results
There were some discrepancies between our data and results from other populations, even when the same type of QUS instrument was used, probably as a result of various factors, including ethnic, life-style environment and diet, among others.
Conclusions
These normative data will be useful for comparing the results of individual studies, predicting fracture risk of Chinese men and women and determining diagnostic criteria of osteoporosis by QUS.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
With the rapid aging of the world's population, osteoporosis is increasingly becoming a global public health problem. Osteoporosis is a systemic skeletal disease characterized by low bone density and the microarchitectural deterioration of bone tissue. The deterioration of skeletal status may result in osteoporotic fractures. Several methods are currently used to determine bone status, of which the most common are dual-energy X-ray absorptiometry (DXA) and quantitative ultrasound (QUS). DXA, the most common method, predicts fracture risk by measuring bone mineral density (BMD), and the World Health Organization (WHO) has established diagnostic criterion for osteoporosis based on the measurement of the BMD using DXA. However, recent research indicates that the biomechanical and structural properties of bone tissue (such as elasticity, anisotropy, geometry and lamellar orientation, among others) are also involved in the occurrence of fractures [1–3]. There is ample evidence [4–7] documenting that QUS reflects not only the BMD but also the structural properties of bone as predictors of bone strength. Moreover, compared with DXA, QUS provides a radiation-free, fast and low-cost method, all factors which greatly increase its availability. Many studies suggest that QUS is also an accurate and reliable method of monitoring skeletal status changes [5, 8–11]. It is also of great utility in clinical practice for fracture risk discrimination [8] and/or prediction [9, 10], particularly for large-scale investigations.
The parameters of QUS measurement include broadband ultrasound attenuation (BUA) and speed of sound (SOS), of which BUA is a reflection of the scattering of the ultrasound signal in trabecular bone and SOS is the speed of sound transmission. These parameters are associated with the quality or material properties of bone, particularly in trabecular bone such as the calcaneus [7, 12, 13]. The Stiffness index (STI) is a third parameter of QUS and is derived from the combination of BUA and SOS. Hans et al. [9] reported a better correlation between QUS STI and DXA BMD than between the latter and BUA and SOS.
Much effort is currently being expended to establish normative data of calcaneus QUS in Caucasian populations, especially for females, while research on male individuals and adolescents, especially those of the Chinese mainland, is less frequent [14–31]. One Chinese investigating team, Wu et al. [31], performed tibial QUS measurements in native Chinese women, but the results only contained data for SOS. The aim of the present study was to obtain reference values for three calcaneal QUS parameters (BUA, SOS and STI) in adolescents, adults and elderly individuals of both sexes of the mainland Chinese population. A second objective was to examine the age- or body size-dependence of possible gender differences.
Subjects and methods
Subjects
A random stratified sample of 725 Chinese females (mean age: 34.9±18.6 years; range: 10–83 years) and 568 males (mean age: 34.6±19.1 years; range: 10–82 years) was obtained from the Zhejiang and Guangxi areas between September 2003 and September 2004. All subjects were screened by means of a detailed questionnaire, history and physical examination. These subjects included military officers, employees, farmers, teachers and students, among others. Subjects with major systemic disorders or diseases affecting bone metabolism, such as diseases of the heart, kidney, liver, thyroid, parathyroid, adrenal, diabetes mellitus, haematologic diseases or a history of malignant tumor, etc., were excluded. None of the subjects were taking any agent known to affect bone metabolism, such as steroids, vitamin D, calcium, calcitonin, thiazides, thyroid hormone, biphosphonate, barbiturates or anti-convulsant medication. All subjects gave informed consent.
Anthropometry
All subjects had their body height and weight measured using a stadiometer and standardized balance-beam scale, respectively, without shoes and in light clothing. Body mass index (BMI) was calculated according to the following formula: BMI (kg/m2)=body weight (kg)/(body height×body height) (m2).
QUS measurements
QUS examination of the right calcaneal bone was performed by measuring BUA (in decibels/megahertz), SOS (in meters/second) and STI (expressed as the percentage of young adults; STI = 0.67×(BUA)+ 0.28×(SOS)−420 [28]) using the Achilles device (Lunar, Madison, Wis.) operated by two technicians who had received the same training. The Achilles system consists of two transducers (emitting and receiving). Contact between the heel and the emitting and receiving transducers of ultrasound was achieved with ultrasound gel. The ultrasound signal is emitted from one transducer and transmitted to the second transduce. After the signal is digitized and stored, the data are sent to a computer for automated analysis. A quality control procedure using the standard phantom was performed daily before the measurements.
In the present study, in-vivo short-term precision as represented by the coefficient of variation (CV) was calculated from four repeated measurements by the same operator, with repositioning, on ten healthy volunteers (age range: 25–37 years). The CVs for SOS, BUA and STI were 0.2, 1.8 and 1.3%, respectively. Inter-observer precision was 0.3% as assessed by comparing the SOS values of ten measurements obtained by two independent operators on two healthy persons.
Statistics
All subjects were divided into seven groups based on age, with a 10-year span in each group (except for the group over 69 years). Data on height, weight, BMI and QUS are expressed as mean values ± standard deviation (SD). Subjects greater than 3 SD were examined and then excluded from this series. Normal distribution was confirmed in all age groups of both sexes. One-way analysis of variance was used to examine the mean differences of QUS between different age groups. Differences in the basic characteristics and QUS in males and females were determined by an independent-samples t-test. The most appropriate model for age-related changes of QUS was determined according to the highest coefficient of determination ®2) after comparing linear, logarithmic, quadratic, cubic, compound, power, growth and exponential regression models. The peak QUS and the age at which the peak QUS was reached were estimated by two different methods. In the first method, the peak QUS was determined from the age group with the highest QUS mean value; in the second method, the peak QUS and its corresponding age were calculated from the cubic equations of the best regression models. The annual decline in QUS parameters after the peak age was calculated using a linear regression model. Pearson’s correlation and stepwise multiple linear regression analysis were conducted to estimate the variation of QUS explained by age, body weight, height and BMI. In addition, Pearson’s correlation coefficient was also computed between BUA, SOS and STI. The statistic significance level was set at p<0.05. The SPSS ver. 11.0 statistic program (SPSS, Chicago, Ill.) for Windows was used for data analysis.
Results
Demographic characteristics
Table 1 shows the general and anthropometric characteristics of the study subjects. Men were significantly heavier and were significantly longer than women (p<0.001 in both cases), however, there was no significant difference in age and BMI between the women and men (p>0.05). There is a trend for the subjects’ height, weight and BMI to initially increase and then progressively decrease with increasing age in both men and women.
Ultrasound values
The results of BUA, SOS and STI for the female and male subjects across different age groups are summarized in Table 2. The three QUS parameters exhibited a characteristic mild rise-then-fall pattern with increasing age in both sexes. In males, the highest mean SOS, BUA and STI values all occurred at the age of 20–29 years. In females, SOS, BUA and STI peaked at 20–29, 40–49 and 20–29 years of age, respectively. In males, there were no statistically significant changes between most adjacent age groups, except that the SOS value at 30–39 years of age was significantly lower than that at the age of 20–29 years (p<0.05) and that the BUA and STI values at the 20–29 years of age were higher than those at 10–19 years (p<0.001 and p<0.05, respectively). However, in the female subjects, age-related differences were very pronounced. There were significant changes in SOS and STI between the age groups of 40–49, 50–59, 60–69 and over 69 years, and in BUA between the age groups of 50–59 and 60–69 years.
Figures 1 and 2 show the scatter plot and cubic regression curves of BUA, SOS and STI against the age of the subjects for both males and females. Based on the cubic regression equations, we calculated the exact peak QUS and corresponding peak age in men and women. Men and women reached the peak SOS levels (1585.4 and 1581.2 m/s, respectively) at 23.9 and 22.6 years, respectively. The peak BUA levels in men and women were 116.6 dB/MHz at 33.6 years and 118.0 dB/MHz at 33.3 years, respectively. The peak STI was 100.8% at 28.4 years in men and 100.5% at 28.3 years in women.

Scatter plots and fitting curves for age-related changes of QUS in the Chinese women of the study cohort. The regression equations between SOS (a), BUA (b) or STI (c) and age are as follows: SOS=1540.867267+4.101489(age)−0.109240(age)2+0.000654(age)3 (R=0.50872; p=0.0000); BUA=89.079325+1.812413(age)−0.034729(age)2+0.000154(age)3(R=0.31632;p=0.0000);STI=70.738572+2.347 549(age)−0.053497(age)2+0.000285(age)3(R=0.44337; p=0.0000)

Scatter plots and fitting curves for age-related changes of QUS in the Chinese men of the study cohort. For the regression equations between SOS (a), BUA (b) or STI (c) and age are as follows: SOS=1540.975262+3.997796(age)−0.117268(age)2+0.000848(age)3 (R=0.34896; p=0.0000); BUA=79.786613+2.732267(age)−0.060234(age)2+0.000384(age)3(R=0.30227;p=0.0000);STI=64.573674+2.931958(age)−0.072729(age)2+0.000492(age)3 (R=0.28877; p=0.0000)
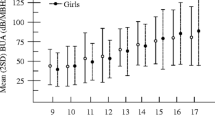
To enable a visual representation of age- and gender-related differences in this population, we plotted BUA, SOS, and STI values (Fig. 3). In the 30–39 and 40–49 age groups, SOS, BUA and STI values were higher in the female subjects than in the male subjects, but without statistical significance. However, men aged 60 years or older had significantly higher values of BUA, SOS and STI than their female counterparts (p<0.05 or p<0.01). In addition to this, the BUA of the men was also significantly higher than that of the women in the 20–29 age group (p<0.05).

Sex differences in SOS (a), BUA (b) and STI (c) values based on age. Significant sex differences were recognized. * p<0.05, ** p<0.01
Table 3 lists linear regression equations between QUS and age in Chinese men and women before and after 40 years of age. The mean decreasing rate of the QUS parameters was significantly different in men (0.702 m/s per year for SOS, and 0.156% per year for STI) (no significant linear correlation between BUA and age in men) and women (0.064 dB/MHz per year for BUA, 0.961 m/s per year for SOS, and 0.310% per year for STI), being more pronounced in women. According to Table 2, the total age-related decrease was 10.2% for BUA, 3.0% for SOS and 20.8% for STI in men; 17.1% for BUA, 5.2% for SOS and 35.7% for STI in women.
Relationship between QUS and age, weight, height and BMI
Correlation analysis revealed the presence of significant relationships between the measured QUS variables. The correlation coefficients between STI and SOS (r=0.871; p=0.000) or BUA (r=0.846; p=0.000) were higher than those between SOS and BUA (r=0.475; p=0.000).
Table 4 shows a Pearson correlation between the ultrasound parameters and age, weight, height or BMI. No significant correlations were found between STI and BMI, and BUA and age in both men and women. In addition, there were also no significant correlations between SOS and height.
In the stepwise multiple linear regression analyses (Table 5), height and BMI were less important factors for QUS in both men and women. In men, SOS was significantly dependent only on age (β=−0.317; p=0.000) and BUA was a function of weight (β=0.299; p=0.000). However, in women, SOS and BUA were both dependent on age (β=−0.493; p=0.000 and β=−0.204; p=0.000 respectively) and weight (β=0.110; p=0.003 and β=0.313; p=0.000, respectively). STI was dependent on age and weight in both men and women. β for age, and weight in men were −0.235 (p=0.000) and 0.195 (p=0.000), respectively. In women, β for age, and weight were −0.410 (p=0.000) and 0.245 (p=0.000), respectively.
Discussion
At the present time, the most common skeletal site for ultrasonometry is the calcaneus, whose bone is 90% greater than the trabecular bone on a volume basis [32] and whose changes are thought to manifest earlier than those of compact bone [30]. In addition, this is a very common form of ultrasonometry for which data are available worldwide, thereby enabling us to compare our data with other those obtained from reference populations. Consequently, we chose the calcaneus as the measurement site to investigate the QUS distribution in a sample cohort of a normal Chinese mainland population. Our study also included some subjects aged between 10 and 20 years, which sets it apart from most other QUS normative studies (generally only including subjects over 20 years of age). This will help us understand the skeletal status of adolescents in the growing state.
The demographic results presented in the preceding section reveal statistically significant differences in weight and height, and a similarity in age distribution and BMI between men and women, which are similar to those reported by Sosa et al. [29]. These parameters are known to be influencing factors on bone mass [33, 34] and are also one of causal factors of sex differences in QUS.
We found a very high correlation between QUS parameters and age in both sexes (except between BUA and age). The QUS values initially increased and then gradually decreased with age in men and women. This trend is consistent with most reports on QUS or BMD. However, due to differences in intrinsic factors (including race, heredity, height, weight, muscle power, fat mass, among others), extrinsic factors (including habitation, diet, lifestyle and others) and the measurement system [35, 36] used, the absolute values of QUS in the different age groups and the decline rates in QUS with age by gender in this study were not completely identical with those in other study groups.
The peak values of SOS, BUA and STI in the Chinese male subjects that we calculated from fittest regression equations occurred at 23.9, 33.6 and 28.4 years, respectively. In the Chinese female subjects, the peak ages of these three QUS parameters were 22.6, 33.3 and 28.3 years, respectively, which are very close to those of the male subjects. Relative to the peak SOS, there was an approximate 10-year delay in the attainment of peak BUA, perhaps due to a delayed mineralization effect and different representations of SOS and BUA (untrasound speed and attenuation, respectively). Since STI was a combination of SOS and BUA, the intermediate peak age was attained. However, the results are also not completely consistent with those of other reports. Thuy et al. [37] found that the BUA peaked around the age of 27 years in Vietnamese men and around 32 years in women. In a study of Estonian women [38], BUA and STI values were found to peak at the age of 30–39 years, while in several other population studies, the ultrasonographic parameter values peaked before the age of 30 years [15, 26, 27, 29, 39].
In accordance with some reports [22, 40, 41] but at odds with others [21], we detected no major differences between adolescent boys and girls. Theoretically, adults should have higher QUS than adolescents because adolescents are in a growth state. In our study, adult men did have higher BUA and STI values than adolescent boys (p<0.001 and p<0.05, respectively). However, there was no statistically significant difference between adult women and adolescent girls. This kind of sex difference may be partly due to the absence of synchronization in growth between adolescent boys and girls. Additionally, our age range was probably too large to manifest the age trend. Faidon et al. [40] was able to show the age trend owing to more detailed age grouping in youngsters. Many investigators have reported that adult men have a higher BUA value than adult women [16, 23, 29, 40, 42], but in our study the SOS and STI values were similar. Among the elderly of our study cohort, all of the QUS variables for men were significantly higher than those for women, which is in agreement with results reported in the literature [16, 23, 24, 29, 30, 40]. The gradually increasing difference between the two genders may result from the double effects of aging and estrogen withdrawal in older women.
The age-related decrease in QUS also revealed differences between the sexes. Calculated with the linear regression equation, the mean decreasing rate of SOS in women was 1.4-fold that of men (0.961 m/s per year, and 0.702 m/s per year, respectively), and the mean decreasing rate of STI in women was twofold that of men (0.310% per year, and 0.156% per year, respectively). In older Chinese men (over 50 years), the average decline in SOS was 0.8 m/s per year; BUA declined about 0.2 dB/MHz annually and STI about 0.4%. However, the average decreases in SOS, BUA and STI in older Chinese women were 2.0 m/s, 0.7 dB/MHz, and 1.0%, respectively. These results are not consistent with those obtained from some studies using the Achilles [15, 20, 27, 28, 43–46]. For example, in Japanese women, BUA was found to decline by about 0.4 dB/MHz annually, the average SOS decrease was 1.5 m/s per year and the resulting annual decline in STI was about 0.6–0.8% [40, 47]. In German women over age 50 years, BUA was found to decline annually by only 0.3 dB/MHZ, and SOS by less than 1 m/s. However, when the total percentages of age changes were examined, the changes are similar to those of other populations [23, 26, 27, 38]. For example, the total age-related decreases in females were 17.1% for BUA, 5.2% for SOS and 35.7% for STI in our population; in German women these were 15% for BUA, 5% for SOS and 31% for STI; in Estonian women, these were14.8% for BUA, 3% for SOS and 29% for STI.
An overview of the results for calcaneus QUS using the same measurement instrument (Achilles) in different ethnic groups (including Estonian, Japanese and German) with similar age groupings is given in Table 6. We can see that the SD of QUS in our study is comparatively greater. A large SD reflects that there is a wide QUS distribution range between each individual of each age group, or an increased coefficient of variation. It can be a result of large differences in the standard of living in China. At the same time, we can also observe that the mean values for SOS and STI (not BUA) in Chinese men are higher than those in Japanese men. In addition, the mean values for SOS and STI in Chinese women are also higher than those in women from other countries, with the exception of the older age groups. It is hard to explain why our data on bone quality are better than those of the populations presented in Table 6. This phenomenon may arise from ethnic differences or other, yet unexplainable, reasons.
We also observed the effect of body size (height, weight and BMI) on QUS as a variable of gender. In the Pearson correlation analysis, no correlation was revealed between STI and BMI in both sexes, or between SOS and height in males. The multiple linear regression analysis (including age) provided further information. SOS, BUA and STI in the female subjects were significantly positively correlated with age and weight. However, in the male subjects, SOS had a stronger correlation only with age, and BUA was related only to weight. Comparatively, height and BMI were not effective influencing factors on QUS. Weight appeared to be the more important influencing factor of QUS than height and BMI, which is in agreement with many reports, including studies on BMD [7, 31, 43, 48–51]. This may be explained by the fact that these parameters express features of weight-bearing bone. The fact that the QUS was influenced by weight could also explain why demineralization occurs under the conditions of long-term bed-rest. If middle-aged and elderly men and women maintain a appropriate weight and actively exercise, the balance between bone absorption and bone formation may be maintained. However, there are also a few reports which have shown that there is no correlation between weight and QUS [38, 52] and, instead, a correlation between height [31] or obesity (BMI) [51, 53–55] and QUS. The reason for this discrepancy is not completely clear, but may possibly be related to different subjects being measured and the instruments.
As mentioned above, many factors affect bone formation and bone loss, such as lifestyle, body composition, muscle power, fat mass, daily calcium intake, and many more. The effect of these factors on QUS in a normal Chinese population need to be investigated, but were not considered in the present investigation. Moreover, in the comparison analysis between different ethnic groups, we did not eliminate effects resulting from differences in height and weight, etc, which is a limitation in the present study.
We also investigated the correlation between SOS, BUA and STI. Our results show that the correlation between BUA or SOS and STI was higher than that between SOS and BUA in both sexes. These results are similar to those of Sosa et al. [29] and may be due to different representations of SOS and BUA and the derivation of STI from a formula based on SOS and BUA. Accordingly, this also can partly explain why the changes in the three QUS parameters with age and the relationships with body size were not completely identical. However, it must be pointed out that the correlation between BUA and SOS in a Spanish population [29] is higher than that in the Chinese population. The reason is unclear.
In conclusion, we established reference data for three calcaneus QUS parameters in Chinese mainland women and men aged between 10 and 83 years. We also investigated the effect of age and body size on QUS and their sexual and ethnic differences. Given the worldwide popularity of QUS parameters, these normative data will be useful for predicting fracture risk in Chinese men and women and determining diagnostic criteria of osteoporosis by QUS.
References
Ammann P, Rizzoli R (2003) Bone strength and its determinants. Osteoporos Int 14:S13–S18
Schnitzler CM (1993) Bone quality: a determinant for certain risk factors for bone fragility. Calcif Tissue Int 53:S27–S31
Faulkner KG (2000) Bone matters: are bone density increases necessary to reduce fracture risk? J Bone Miner Res 15:183–187
Heaney RP, Kanis JA (1996) The interpretation and utility of ultrasound measurements of bone. Bone 18:491–492
Gluer CC (1997) Quantitative ultrasound techniques for the assessment of osteoporosis: expert agreement on current status. J Bone Miner Res 12:1280–1288
Langton CM, Njeh CF (1998) Sound-tissue interaction: the physical basis of bone ultrasonometry and limitations of existing methods. J Clin Densitom 1:295–301
Njeh CF, Boivin CM, Langton CM (1997) The role of ultrasound in the assessment of osteoporosis: a review. Osteoporos Int 7:7–22
Lopez-Rodriguez F, Mezquita-Raya P, de Dios Luna J, Escobar-Jimenez F, Munoz-Torres M (2003) Performance of quantitative ultrasound in the discrimination of prevalent osteoporotic fractures in a bone metabolic unit. Bone 32:571–578
Hans D, Dargent-Molina P, Schott AM, Sebert JL, Cormier C, Kotzki PO, Delmas PD, Pouilles JM, Breart G, Meunier PJ (1996) Ultrasonographic heel measurements to predict hip fracture in elderly women: the EPIDOS prospective study. Lancet 348:511–514
Bauer DC, Gluer CC, Cauley JA, Vogt TM, Ensrud KE, Genant HK, Black DM (1997) Broadband ultrasound attenuation predicts fractures strongly and independently of densitometry in older women. A prospective study. Study of Osteoporotic Fractures Research Group. Arch Int Med 157:629–634
Frost ML, Blake GM, Fogelman I (2001) Quantitative ultrasound and bone mineral density are equally strongly associated with risk factors for osteoporosis. J Bone Miner Res 16:406–416
Hans D, Wu C, Njeh CF, Zhao S, Augat P, Newitt D, Link T, Lu Y, Majumdar S, Genant HK (1999) Ultrasound velocity of trabecular cubes reflects mainly bone density and elasticity. Calcif Tissue Int 64:18–23
Stewart A, Reid DM (2002) Quantitative ultrasound in osteoporosis. Semin Musculoskelet Radiol 6:229–232
Heldan de Moura Castro C, Medeiros Pinheiro M, Lucia Szejnfeld V (2000) Quantitative ultrasound of the calcaneus in Brazilian Caucasian women: normative data are similar to the manufacturer’s normal range. Osteoporos Int 11:923–928
Cepollaro C, Agnusdei D, Gonnelli S, Martini G, Pondrelli C, Borracelli D, Palmieri R, Parisi G, Gennari C (1995) Ultrasonographic assessment of bone in normal Italian males and females. Br J Radiol 68:910–914
Langton CM, Langton DK (1997) Male and female normative data for ultrasound measurement of the calcaneus within the UK adult population. Br J Radiol 70:580–585
Moris M, Peretz A, Tjeka R, Negaban N, Wouters M, Bergmann P (1995) Quantitative ultrasound bone measurements: normal values and comparison with bone mineral density by dual X-ray absorptiometry. Calcif Tissue Int 57:6–10
Pluskiewicz W (1998) Bone status assessed by quantitative ultrasound in healthy postmenopausal Polish women: normative data. Clin Rheumatol 17:40–43
Schott AM, Hans D, Sornay-Rendu E, Delmas PD, Meunier PJ (1993) Ultrasound measurements on os calcis: precision and age-related changes in a normal female population. Osteoporos Int 3:249–254
Truscott JG (1997) Reference data for ultrasonic bone measurement: variation with age in 2087 Caucasian women aged 16–93 years. Br J Radiol 70:1010–1016
Wunsche K, Wunsche B, Fahnrich H, Mentzel HJ, Vogt S, Abendroth K, Kaiser WA (2000) Ultrasound bone densitometry of the os calcis in children and adolescents. Calcif Tissue Int 67:349–355
van den Bergh JP, Noordam C, Ozyilmaz A, Hermus AR, Smals AG, Otten BJ (2000) Calcaneal ultrasound imaging in healthy children and adolescents: relation of the ultrasound parameters BUA and SOS to age, body weight, height, foot dimensions and pubertal stage. Osteoporos Int 11:967–976
Landin-Wilhelmsen K, Johansson S, Rosengren A, Dotevall A, Lappas G, Bengtsson BA, Wilhelmsen L (2000) Calcaneal ultrasound measurements are determined by age and physical activity. Studies in two Swedish random population samples. J Intern Med 247:269–278
Adami S, Giannini S, Giorgino R, Isaia G, Maggi S, Sinigaglia L, Filipponi P, Crepaldi G, Di Munno O (2003) The effect of age, weight, and lifestyle factors on calcaneal quantitative ultrasound: the ESOPO study. Osteoporos Int 14:198–207
Ishikawa K, Ohta T (1999) Radial and metacarpal bone mineral density and calcaneal quantitative ultrasound bone mass in normal Japanese women. Calcif Tissue Int 65:112–116
Kung AW, Tang GW, Luk KD, Chu LW (1999) Evaluation of a new calcaneal quantitative ultrasound system and determination of normative ultrasound values in southern Chinese women. Osteoporos Int 9:312–317
Hadji P, Hars O, Bock K, Albert U, Beckmann MW, Emons G, Schulz K (1999) Age changes of calcaneal ultrasonometry in healthy German women. Calcif Tissue Int 65:117–120
Thompson P, Taylor J, Fisher A, Oliver R (1998) Quantitative heel ultrasound in 3180 women between 45 and 75 years of age: compliance, normal ranges and relationship to fracture history. Osteoporos Int 8:211–214
Sosa M, Saavedra P, Munoz-Torres M, Alegre J, Gomez C, Gonzalez-Macias J, Guanabens N, Hawkins F, Lozano C, Martinez M, Mosquera J, Perez-Cano R, Quesada M, Salas E (2002) Quantitative ultrasound calcaneus measurements: normative data and precision in the Spanish population. Osteoporos Int 13:487–492
Pluskiewicz W, Drozdzowska B (1999) Ultrasonic measurement of the calcaneus in Polish normal and osteoporotic women and men. Bone 24:611–617
Wu XP, Liao EY, Luo XH, Dai RC, Zhang H, Peng J (2003) Age-related variation in quantitative ultrasound at the tibia and prevalence of osteoporosis in native Chinese women. Br J Radiol 76: 605–610
Vogel JM, Wasnich RD, Ross PD (1988) The clinical relevance of calcaneus bone mineral measurements: a review. Bone Miner 5:35–58
National Institutes of Health (NIH) consensus development conference (1993) Diagnosis, prophylaxis, and treatment of osteoporosis. Am J Med 94:646–650
World Health Organization (WHO) study group (1994) Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Technical report series 843. WHO, Geneva
Njeh CF, Hans D, Li J, Fan B, Fuerst T, He YQ, Tsuda-Futami E, Lu Y, Wu CY, Genant HK (2000) Comparison of six calcaneal quantitative ultrasound devices: precision and hip fracture discrimination. Osteoporos Int 11:1051–1062
Tothill P, Fenner JA, Reid DM (1995) Comparisons between three dual energy X-ray absorptiometers used for measuring spine and femur. Br J Radiol 68:621–629
Thuy VT, Chau TT, Cong ND, De DV, Nguyen TV (2003) Assessment of low bone mass in Vietnamese: comparison of QUS calcaneal ultrasonometer and data-derived T-scores. J Bone Miner Metab 21:114–119
Maasalu K, Kirjanen K, Haviko T (2002) Bone status in healthy Estonian women assessed with quantitative ultrasonometry. Acta Orthop Scand 73:558–561
Yamazaki K, Kushida K, Ohmura A, Sano M, Inoue T (1994) Ultrasound bone densitometry of the os calcis in Japanese women. Osteoporos Int 4:220–225
Magkos F, Manios Y, Babaroutsi E, Sidossis LS (2005) Quantitative ultrasound calcaneus measurements: normative data for the Greek population. Osteoporos Int 16:280–288
Brukx LJ, Waelkens JJ (2003) Evaluation of the usefulness of a quantitative ultrasound device in screening of bone mineral density in children. Ann Hum Biol 30:304–315
Welch A, Camus J, Dalzell N, Oakes S, Reeve J, Khaw KT (2004) Broadband ultrasound attenuation (BUA) of the heel bone and its correlates in men and women in the EPIC-Norfolk cohort: a cross-sectional population-based study. Osteoporos Int 15:217–225
Zerahn B, Borgwardt A, Hejsgard C, Lemser T (1996) Ultrasound and BMD measurements of the os calcis in normal Danish adults. Eur J Exp Musculoskel Res 4:154–159
van Daele PL, Burger H, Algra D, Hofman A, Grobbee DE, Birkenhager JC, Pols HA (1994) Age-associated changes in ultrasound measurements of the calcaneus in men and women: the Rotterdam study. J Bone Miner Res 9:1751–1757
Wendt B, Cornelius A, Otto R (1996) Diagnosis of osteoporosis with ultrasound densitometry of the calcaneus. Radiologe 36:58–63
Karlsson MK, Obrant KJ, Nilsson BE, Johnell O (1998) Bone mineral density assessed by quantitative ultrasound and dual energy X-ray absorptiometry. Acta Orthop Scand 69:189–193
Takeda N, Miyake M, Kita S, Tomomitsu T, Fukunaga M (1996) Sex and age patterns of quantitative ultrasound densitometry of the calcaneus in normal Japanese subjects. Calcif Tissue Int 59:84–88
Xu SZ, Zhou W, Mao XD, Xu J, Xu LP, Ren JY (2001) Reference data and predictive diagnostic models for calcaneus bone mineral density measured with single-energy x-ray absorptiometry in 7428 Chinese. Osteoporos Int 12:755–762
Pluskiewicz W, Drozdzowska B (2001) Quantitative ultrasound (QUS) at the calcaneus and hand phalanges in polish healthy postmenopausal women. Ultrasound Med Biol 27:373–377
Tromp AM, Smit JH, Deeg DJ, Lips P (1999) Quantitative ultrasound measurements of the tibia and calcaneus in comparison with DXA measurements at various skeletal sites. Osteoporos Int 9:230–235
Yeh LR, Chen CK, Lai PH (2004) Normal bone mineral density in anteroposterior, lateral Spine and hip of Chinese men in Taiwan: effect of age change, body weight and height. J Chin Med Assoc 67:287–295
Damilakis JE, Dretakis E, Gourtsoyiannis NC (1992) Ultrasound attenuation of the calcaneus in the female population: normative data. Calcif Tissue Int 51:180–183
Kirchengast S, Knogler W, Hauser G (2002) Protective effect of moderate overweight on bone density of the hip joint in elderly and old Austrians. Anthropol Anz 60:187–197
Kao CH, Chen CC, Wang SJ (1994) Normal data for lumbar spine bone mineral content in healthy elderly Chinese: influences of sex, age, obesity and ethnicity. Nucl Med Commun 15:916–920
Nishizawa Y, Koyama H, Shoji T, Aratani H, Hagiwara S, Miki T, Morii H (1991) Obesity as a determinant of regional bone mineral density. J Nutr Sci Vitaminol 37:S65–S70
Acknowledgements
This study was supported by the Special Fund for Key Basic Research Project of the Ministry of National Science and Technology China (200DA30031, 2002DIA40018). We express our heartfelt thanks to all participants for their helpful assistance.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Liu, W., Xu, C.L., Zhu, Z.Q. et al. Characteristics of calcaneus quantitative ultrasound normative data in Chinese mainland men and women. Osteoporos Int 17, 1216–1224 (2006). https://doi.org/10.1007/s00198-006-0081-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-006-0081-6