
Abstract
Purpose
A modified quadrant method was developed for description of femoral tunnel aperture positions on the sagittal plane after double-bundle anterior cruciate ligament (ACL) reconstruction, which can be measured by using two-view radiographs. The purpose of the study is to provide a new measurement method and to evaluate the reproducibility and accuracy of the method.
Methods
Forty-one patients who had undergone a double-bundle ACL reconstruction were investigated. Two-view plain radiographs, a 45-degree-flexion posterior–anterior standing (Rosenberg) and a lateral view, were taken at 1 year postoperatively, and the femoral tunnel positions were measured. Intra- and inter-observer reproducibility was calculated by means of intra-class correlation coefficient (ICC). Also, the accuracy of the method was evaluated by comparing the measurement from three-dimensional computed tomography (3D-CT).
Results
Intra-observer reproducibility was excellent (ICC > 0.9). Inter-observer reproducibility of antero-medial (AM) tunnel position was almost perfect (ICC > 0.8) and that of postero-lateral (PL) tunnel was substantial (ICC > 0.7). The accuracy of the method was assessed by comparing the measurement from 3D-CT and was found to be almost perfect (ICC > 0.8). With the modified quadrant method, the average height of AM and PL tunnels were 17.8 and 44.4 %, respectively, and the depth of AM and PL tunnels were 25.5 and 36.7 %, respectively.
Conclusions
A modified quadrant method was found to have acceptable reproducibility and accuracy. The method is useful for describing the femoral tunnel aperture positions in ACL reconstruction because of its easiness and simplicity. By using this method, it is possible to analyse the femoral tunnel position even in the cases without CT analysis.
Level of evidence
IV.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The importance of femoral tunnel aperture positions has been emphasized in anterior cruciate ligament (ACL) reconstruction. The femoral tunnel position affects graft tension and isometricity more significantly than the tibial tunnel position [5, 17, 27]. A significant amount of experimental studies suggest that the femoral tunnel positioning would be correlated with the clinical outcome of ACL reconstruction [1, 7, 14, 24].
Recently, anatomic anterior cruciate ligament (ACL) reconstruction has attracted attention among knee ligament surgeons [10, 16, 20, 23, 25]. To evaluate the aperture position of the femoral tunnel is technically more difficult than determining those of tibial tunnel, especially in double-bundle (DB) ACL reconstructions. Controversies still remain regarding the optimal femoral aperture position and anatomic placement. One of the reasons for this is due to the lack of a proper evaluation method for femoral tunnel position in respect of cost and ease of implementation.
Bernard et al. [3] developed a “quadrant method” to identify the femoral tunnel position on the sagittal plain radiographs using a quadrant consisting of a Blumensaat’s line as a roof and a lateral condyle. By using this quadrant method, the femoral tunnel position is indicated by percentage from the posterior tangential line and from the distal tangential line [4, 9, 26]. This method is very simple and easy; however, an image intensifier would be necessary to take a true lateral view, and it often happens that the tunnel positions are invisible on the plain radiographs, especially in the early period after double-bundle ACL reconstruction. Three-dimensional computed tomography (3D-CT) analysis [11] for determining the tunnel aperture position would be one of the preferable measurement methods; however, radiographic analysis has the advantages in terms of cost and radiation exposure for the daily medical practice.
In the present study, “a modified quadrant method” was developed for description of femoral tunnel aperture positions on the sagittal plane after double-bundle ACL reconstruction, which can be measured by using two-view radiographs. The purpose of the study is to introduce a modified quadrant method, and to evaluate the reproducibility and accuracy of the method. We hypothesized that the reproducibility and accuracy of the radiographic measures for ACL tunnel aperture position would be acceptable.
Materials and methods
Forty-one knees in 41 patients who had undergone a double-bundle ACL reconstruction with hamstrings at Tokyo Medical and Dental University Hospital between 2004 and 2008 were randomly picked up and investigated for the current study. Four hundred and six ACL reconstructions were performed during these 5 years. Two-view radiographs, a 45-degree-flexion posterior–anterior standing (Rosenberg) view [19] and a lateral view [15], were routinely taken at 1 year after the surgery. Lateral radiographs of the knee were taken with the patient lying supine. The patient’s foot was elevated on a 25-cm high wedge-shaped bolster, with other bolsters used if necessary, to satisfactorily adjust leg rotation while maintaining the leg muscles in a relaxed state [15]. The leg rotation was controlled by skeletal radiological technicians. In case of unacceptable rotational control, a lateral radiograph in extension was taken again before sending the final radiographs to the outpatient office. Then, the femoral tunnel aperture positions were measured with the following method (modified quadrant method). For evaluation of the reproducibility and accuracy of the method, 20 knees were randomly picked up among the 41 patients and examined.
Modified quadrant method
On the Rosenberg view, the tangential line connecting the posterior margin of both medial and lateral posterior condyles was drawn (PC line). The parallel line to PC line running through the highest point of posterior condylar notch was drawn (Roof line). The midlines of the AM/PL tunnel were drawn and extended to the intercondylar notch. Then, the points of intersection between the posterior intercondylar notch and AM or PL tunnel lines were identified, and the parallel line to PC line was drawn through these points (A line/P line). The distance between PC line to Roof line (x), PC line to A line (y), and PC line to P line (z) were measured, and the ratio of y/x and z/x were calculated as height ratio (Fig. 1a).

Measuring steps for the modified quadrant method. a Step 1—Detection of tunnel aperture centres on the Rosenberg view. PC line, Roof line, A line, and P line were drawn. The distance between PC line to Roof line (x), PC line to A line (y), and PC line to P line (z) were measured, and the ratio of y/x and z/x were calculated as height ratio (see “Materials and methods” in detail). b Step 2—Detection of tunnel aperture centres on the lateral view. The four lines obtained from the Rosenberg view (Roof line, A line, P line, and PC line) were put onto the lateral view with keeping the same height ratio (y/x and z/y). Then, AM/PM tunnel lines were drawn, and the points of intersection between AM/PM tunnel lines and A/P lines were considered as tunnel aperture centres on the sagittal plane (AM aperture centre: black circle, PL aperture centre: white circle). c Step 3—Measurement of tunnel aperture centres on the lateral view by quadrant method. The marked AM and PL aperture centres were expressed as percentages from the Blumensaat’s line (height) and from the posterior line (depth) according to the quadrant method
Next, the four lines obtained from the Rosenberg view (Roof line, A line, P line, and PC line) were put onto the lateral view with keeping the same height ratio. At that time, Roof line was considered to be equivalent to Blumensaat’s line on the lateral view, and PC line was considered to be equivalent to the tangential line connecting to the posterior margin of the condyle. Then, AM/PM tunnel lines were drawn on the lateral view and the points of intersection between AM/PM tunnel lines and A/P lines were marked (Fig. 1b). The marked AM and PL aperture centres were expressed as percentages from the Blumensaat’s line (height) and from the posterior line (depth) according to the quadrant method (Fig. 1c).
Statistical analysis
Twenty patients were randomly selected among the 41 patients and two examiners independently measured the femoral tunnel aperture positions twice by the modified quadrant method. Intra- and inter-observer reproducibility was evaluated by means of the intra-class correlation coefficient (ICC) using SPSS. Also, the accuracy of the method was evaluated by comparing the measurement by quadrant method from the images of three-dimensional computed tomography (3D-CT) [11], which were taken at 1 year postoperatively. Test–retest reliability was determined with the ICC, which measures the correlation between the results of the aperture positions obtained by the same observer on two separate occasions (intra-observer ICC). ICCs ranged from 0 to 1. The reliability was considered to be excellent if the ICC was greater than 0.91, almost perfect between 0.9 and 0.81, substantial between 0.61 and 0.80, and moderate between 0.41 and 0.60 [12].
Results
The reproducibility of the modified quadrant method is shown in Tables 1 and 2. Intra-observer reproducibility was excellent in both height and depth of AM and PL tunnel aperture positions (ICC: AM height = 0.99, AM depth = 0.95, PL height = 0.96, PL depth = 0.95). Inter-observer reproducibility of AM tunnel aperture positions was almost perfect (ICC: AM height = 0.97, AM depth = 0.90) and that of PL tunnel was substantial (ICC: PL height = 0.85, PL depth = 0.74).
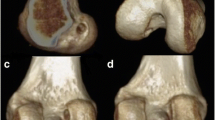
The accuracy of the method was assessed by comparing the measurement by quadrant method from the images of 3D-CT (Fig. 2) and was found to be almost perfect (ICC: AM height = 0.84, AM depth = 0.82, PL height = 0.85, PL depth = 0.82) (Table 3). The hypothesis was supported by our results.

Image of 3D-CT for measurement of the femoral tunnel position by quadrant method
The femoral tunnel aperture positions of 41 cases were examined by the modified quadrant method. The results are shown in Table 4. With the modified quadrant method, the height of the antero-medial (AM) and postero-lateral (PL) tunnels were 17.8 ± 5.1 % and 44.4 ± 7.6 %, respectively, from the roof of the intercondylar notch, and the depth of the AM and PL tunnels were 25.5 ± 7.3 % and 36.7 ± 8.1 %, respectively, from the posterior line of the quadrant.
Discussion
The most important finding for the current study was that a newly developed measurement with the use of two-view plain radiographs to provide femoral tunnel positions on the sagittal plane after double-bundle ACL reconstruction was found to have acceptable reproducibility and accuracy. It made it possible to identify the femoral tunnel aperture position on the lateral view with the use of tunnel height information, which was obtained from 45-degree-flexion posterior–anterior standing (Rosenberg) view. The modified quadrant method has an advantage in its easiness, simplicity, cost, and radiological exposure compared with CT assessment. Simple methods would be preferable for surgeons to evaluate femoral tunnel aperture position after ACL reconstruction postoperatively in the daily medical practice. In our hospital, we routinely take these two-view radiographs after the ACL reconstruction at each follow-up time point. Therefore, by using the modified quadrant method, it made it possible to analyse the femoral tunnel aperture position even in the cases without CT retrospectively.
With respect to the reproducibility, the inter-observer reproducibility of PL tunnel positions was slightly lower than that of AM tunnel position. One of the reasons was thought that there is some minor deviation between the observers when they determine the points of intersection between the posterior intercondylar notch and PL tunnel lines. However, this kind of measurement problem is not easily resolved even with the use of CT or MRI [2, 6, 8, 13, 21]. Moreover, the determination of the tunnel aperture position is thought to be difficult even with the use of CT and MRI. With regard to the use of the Rosenberg view for assessing the tunnel height, it will be simple and appropriate because the height of the anterior and posterior intercondylar notches was identical in most cases, that is, the radiographic beam was parallel to the Blumensaat’s line in our Rosenberg view.
Colombet et al. [4] indicated the centre of AM bundle of the normal ACL is positioned about 1/4 height from the Blumensaat’s line and 1/4 depth from the posterior side, and that of PL bundle is about 50 % height and 1/3 depth, respectively, based on the quadrant method. Zantop et al. [26] described the central position of AM bundle and PL bundle of the normal ACL using the quadrant method as 18.5 % height and 22.3 % depth for the centre of normal AM bundle and 53.6 % height and 29.3 % depth for normal PL bundle. In the present study, the average aperture centre of AM tunnel was described as 17.8 % height and 25.5 % depth and that of PL tunnel as 44.4 % height and 36.7 % depth with the modified quadrant method. The tunnel position of our DB reconstruction was thought to be close to the centre of AM bundle and PL bundle of the normal ACL; nevertheless, the femoral tunnel placement was performed by transtibial approach [18, 22].
One limitation of the modified quadrant method is that the accuracy would basically depend on the accuracy and repeatability of each radiographic image. Also, in some radiographic images, there is difficulty in plotting the central position of the femoral aperture on Rosenberg view. Other disadvantages might involve tracing the contour of the posterior intercondylar notch.
Conclusion
A modified quadrant method was found to have acceptable intra-observer/inter-observer reproducibility and the accuracy. The method is useful for describing the femoral tunnel aperture positions in ACL reconstruction because of its easiness and simplicity with the use of two-view radiographs. With the modified quadrant method, the average height of AM and PL aperture positions were 17.8 and 44.4 %, respectively, and the depth of AM and PL tunnels were 25.5 and 36.7 %, respectively, in our 41 cases of a double-bundle ACL reconstruction.
References
Abebe ES, Kim JP, Utturkar GM et al (2011) The effect of femoral tunnel placement on ACL graft orientation and length during in vivo knee flexion. J Biomech 44:1914–1920
Basdekis G, Christel P, Anne F (2009) Validation of the position of the femoral tunnels in anatomic double-bundle ACL reconstruction with 3-D CT scan. Knee Surg Sports Traumatol Arthrosc 17:1089–1094
Bernard M, Hertel P, Hornung H, Cierpinski T (1997) Femoral insertion of the ACL. Radiographic quadrant method. Am J Knee Surg 10: 14–21; discussion 21-12
Colombet P, Robinson J, Christel P et al (2006) Morphology of anterior cruciate ligament attachments for anatomic reconstruction: a cadaveric dissection and radiographic study. Arthroscopy 22:984–992
Giron F, Cuomo P, Aglietti P, Bull AM, Amis AA (2006) Femoral attachment of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc 14:250–256
Hoser C, Tecklenburg K, Kuenzel KH, Fink C (2005) Postoperative evaluation of femoral tunnel position in ACL reconstruction: plain radiography versus computed tomography. Knee Surg Sports Traumatol Arthrosc 13:256–262
Hosseini A, Lodhia P, Van de Velde SK et al (2012) Tunnel position and graft orientation in failed anterior cruciate ligament reconstruction: a clinical and imaging analysis. Int Orthop 36:845–852
Inoue M, Tokuyasu S, Kuwahara S et al (2010) Tunnel location in transparent 3-dimensional CT in anatomic double-bundle anterior cruciate ligament reconstruction with the trans-tibial tunnel technique. Knee Surg Sports Traumatol Arthrosc 18:1176–1183
Iriuchishima T, Ingham SJ, Tajima G et al (2010) Evaluation of the tunnel placement in the anatomical double-bundle ACL reconstruction: a cadaver study. Knee Surg Sports Traumatol Arthrosc 18:1226–1231
Kawaguchi Y, Kondo E, Kitamura N, Kai S, Inoue M, Yasuda K (2011) Comparisons of femoral tunnel enlargement in 169 patients between single-bundle and anatomic double-bundle anterior cruciate ligament reconstructions with hamstring tendon grafts. Knee Surg Sports Traumatol Arthrosc 19:1249–1257
Kawakami Y, Hiranaka T, Matsumoto T et al (2012) The accuracy of bone tunnel position using fluoroscopic-based navigation system in anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 20:1503–1510
Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data. Biometrics 33:159–174
Lorenz S, Elser F, Mitterer M, Obst T, Imhoff AB (2009) Radiologic evaluation of the insertion sites of the 2 functional bundles of the anterior cruciate ligament using 3-dimensional computed tomography. Am J Sports Med 37:2368–2376
Markolf KL, Hame S, Hunter DM et al (2002) Effects of femoral tunnel placement on knee laxity and forces in an anterior cruciate ligament graft. J Orthop Res 20:1016–1024
Muneta T, Ezura Y, Sekiya I, Yamamoto H (1996) Anterior knee laxity and loss of extension after anterior cruciate ligament injury. Am J Sports Med 24:603–607
Muneta T, Koga H, Mochizuki T et al (2007) A prospective randomized study of 4-strand semitendinosus tendon anterior cruciate ligament reconstruction comparing single-bundle and double-bundle techniques. Arthroscopy 23:618–628
Muneta T, Yamamoto H, Sakai H, Ishibashi T, Furuya K (1993) Relationship between changes in length and force in in vitro reconstructed anterior cruciate ligament. Am J Sports Med 21:299–304
Piasecki DP, Bach BR Jr, Espinoza Orias AA, Verma NN (2011) Anterior cruciate ligament reconstruction: can anatomic femoral placement be achieved with a tarsotibial technique? Am J Sports Med 39:1306–1315
Rosenberg TD, Paulos LE, Parker RD, Coward DB, Scott SM (1988) The forty-five-degree posteroanterior flexion weight-bearing radiograph of the knee. J Bone Jt Surg Am 70:1479–1483
Shino K, Nakata K, Nakamura N et al (2008) Rectangular tunnel double-bundle anterior cruciate ligament reconstruction with bone-patellar tendon-bone graft to mimic natural fiber arrangement. Arthroscopy 24:1178–1183
Steckel H, Musahl V, Fu FH (2010) The femoral insertions of the anteromedial and posterolateral bundles of the anterior cruciate ligament: a radiographic evaluation. Knee Surg Sports Traumatol Arthrosc 18:52–55
Strauss EJ, Barker JU, McGill K, Cole BJ, Bach BR Jr, Verma NN (2011) Can anatomic femoral tunnel placement be achieved using a tarsotibial technique for hamstring anterior cruciate ligament reconstruction? Am J Sports Med 39:1263–1269
van Eck CF, Schreiber VM, Mejia HA et al (2010) “Anatomic” anterior cruciate ligament reconstruction: a systematic review of surgical techniques and reporting of surgical data. Arthroscopy 26:S2–S12
Xu Y, Ao Y, Wang J, Yu J, Cui G (2011) Relation of tunnel enlargement and tunnel placement after single-bundle anterior cruciate ligament reconstruction. Arthroscopy 27:923–932
Yasuda K, Kondo E, Ichiyama H et al (2004) Anatomic reconstruction of the anteromedial and posterolateral bundles of the anterior cruciate ligament using hamstring tendon grafts. Arthroscopy 20:1015–1025
Zantop T, Wellmann M, Fu FH, Petersen W (2008) Tunnel positioning of anteromedial and posterolateral bundles in anatomic anterior cruciate ligament reconstruction: anatomic and radiographic findings. Am J Sports Med 36:65–72
Zavras TD, Race A, Amis AA (2005) The effect of femoral attachment location on anterior cruciate ligament reconstruction: graft tension patterns and restoration of normal anterior–posterior laxity patterns. Knee Surg Sports Traumatol Arthrosc 13:92–100
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Horie, M., Muneta, T., Yamazaki, J. et al. A modified quadrant method for describing the femoral tunnel aperture positions in ACL reconstruction using two-view plain radiographs. Knee Surg Sports Traumatol Arthrosc 23, 981–985 (2015). https://doi.org/10.1007/s00167-013-2781-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-013-2781-8