
Abstract
Purpose
The quadrant method was described by Bernard et al. and it has been widely used for postoperative evaluation of anterior cruciate ligament (ACL) reconstruction. The purpose of this research is to further develop the quadrant method measuring four points, which we named four-point quadrant method, and to compare with the quadrant method.
Methods
Three-dimensional computed tomography (3D-CT) analyses were performed in 25 patients who underwent double-bundle ACL reconstruction using the outside-in technique. The four points in this study’s quadrant method were defined as point1—highest, point2—deepest, point3—lowest, and point4—shallowest, in femoral tunnel position. Value of depth and height in each point was measured. Antero-medial (AM) tunnel is (depth1, height2) and postero-lateral (PL) tunnel is (depth3, height4) in this four-point quadrant method. The 3D-CT images were evaluated independently by 2 orthopaedic surgeons. A second measurement was performed by both observers after a 4-week interval. Intra- and inter-observer reliability was calculated by means of intra-class correlation coefficient (ICC). Also, the accuracy of the method was evaluated against the quadrant method.
Results
Intra-observer reliability was almost perfect for both AM and PL tunnel (ICC > 0.81). Inter-observer reliability of AM tunnel was substantial (ICC > 0.61) and that of PL tunnel was almost perfect (ICC > 0.81). The AM tunnel position was 0.13% deep, 0.58% high and PL tunnel position was 0.01% shallow, 0.13% low compared to quadrant method.
Conclusions
The four-point quadrant method was found to have high intra- and inter-observer reliability and accuracy. This method can evaluate the tunnel position regardless of the shape and morphology of the bone tunnel aperture for use of comparison and can provide measurement that can be compared with various reconstruction methods. The four-point quadrant method of this study is considered to have clinical relevance in that it is a detailed and accurate tool for evaluating femoral tunnel position after ACL reconstruction.
Level of Evidence
Case series, Level IV.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Accurate and appropriate tunnel position in anterior cruciate ligament (ACL) reconstruction plays an important role in postoperative knee joint function [21, 31]. Tunnel position influences tibial anterior translation and rotation and postoperative clinical outcomes. Tunnel malposition causes recurrence of knee instability and increased risk of osteoarthritis after ACL reconstruction [1]. Specifically, the femoral tunnel position affects graft tension and isometricity more significantly than the tibial tunnel position [6, 19, 34]. Incorrect femoral tunnel position is a frequent cause of failed ACL reconstruction [8]. Recently, more anatomical reconstruction techniques have been developed in ACL reconstruction [20, 29, 31, 32]. Bernard et al. [2] developed the quadrant method to distinguish the femoral tunnel position on a true lateral plain radiographs using a quadrant consisting of a Blumensaat’s line as a roof and a lateral condyle. Since the quadrant method is simple and easy to understand, it has been widely used for postoperative evaluation of ACL reconstruction. However, a true lateral plain radiograph is necessary for accurate measurement. Tunnel location is often difficult to evaluate on a plain radiograph and, therefore, computed tomography (CT) is more commonly used to provide better visualization of bony structure [5, 7]. Furthermore, three-dimensional (3D) CT scans can provide an excellent perspective of the tunnel aperture and bony morphology after ACL reconstruction, making it a preferred tool today [5, 12]. There are many reports using this quadrant method to evaluate tunnel position reconstructed by different femoral bone tunnel preparation method, but it is difficult to compare between different groups of reconstruction method using quadrant method as measurement [17, 22, 25, 26]. In this study, quadrant method has been further developed which measures four points to describe the femoral tunnel position using 3DCT. We call it as four-point quadrant method. The purpose of this study is to introduce this new method and evaluate its intra- and inter-observer reliability against the quadrant method to determine its accuracy. We hypothesized that the four-point quadrant method is as highly reliable and as accurate as the quadrant method.
Materials and methods
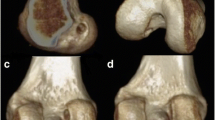
There were thirty seven knees in 37 patients who had undergone a double-bundle (DB) ACL reconstruction with hamstrings at Toho University Ohashi Medical Center from April 2015 to December 2016. Twenty-five knees that excluded single-bundle reconstruction, re-reconstruction and multi-ligament injury were included in the current study. Computed tomography analyses were performed in 25 patients who underwent DB-ACL reconstruction using the outside-in technique. Computed tomography analyses were done in all knees. Multislice CT system Aquilion (Toshiba Medical Systems®) with 4-slice multidetector helical acquisition in 1.25-mm sections and pitch 3.0 and spacing of 0.5 mm was used. Initially, the distal femur model was positioned horizontally in the true lateral position, where both femoral condyles were superimposed as Bernard et al. [2] described for the lateral radiograph of the knee. The image was then rotated to a distal view, and the medial femoral condyle was virtually removed at the highest point of the anterior aperture of the intercondylar notch leaving the lateral femoral condyle. Finally, the model was rotated back to the true lateral position, which was confirmed by superimposing a full distal femur model onto the lateral femoral condyle model. The medial–lateral (M–L) view of the lateral femoral condyle was applied to 4 by 4 grid in this lateral position (Fig. 1) [11, 15]. The image of 3DCT was downloaded to a personal computer and measured with Microsoft PowerPoint for Mac software (Redmond, WA, USA). 2 orthopaedic surgeons measured the central point of AM and PL tunnel by the quadrant method and measured the deep1, high2, deep3 and high4 of the point1–4 by the four-point quadrant method. The measurement was repeated after a 4-week interval by both observers.

The M–L view of the lateral femoral condyle was obtained from the 3DCT of the distal femur in the strictly lateral position, where both condyles were superimposed. 3DCT of the medial–lateral (M–L) view was applied to 4 by 4 grid based on the quadrant method. M–L, medial–lateral
The four-point quadrant method
3DCT of the medial–lateral (M–L) view was applied to 4 by 4 grid based on the quadrant method. In case of DB-ACL reconstruction, the central point of AM and PL tunnel was measured in ratio to depth and height by the quadrant method.
The four-point quadrant method in this study was defined as point1—highest, point2—deepest, point3—lowest, and point4—shallowest, in femoral tunnel position.
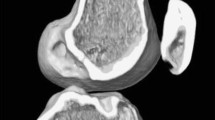
Also, in this method, point1 was positioned above the AM tunnel, point 2 was positioned behind the AM tunnel, point 3 was positioned below the PL tunnel, and point 4 was positioned in front of the PL tunnel on the 4 × 4 grid. Value of depth and height was measured in each point. To compare with the quadrant method, AM tunnel was prescribed as (depth1, height2) and PL tunnel as (depth3, height4) in the four-point quadrant method (Fig. 2). This study was approved by the Ethics Committee of Toho University Ohashi medical Center (no. H16110).

Measurements of femoral tunnel positioning. a Four-point quadrant method. b Quadrant method
Statistical analysis
Twenty-five patients’ CT after DB-ACL reconstruction was used for analysis. Intra- and inter-observer reliability was calculated by means of intra-class correlation coefficient (ICC). Test–retest reliability was determined with the intra-observer ICC of measurements obtained on two occasions by each observer. Also, the accuracy was evaluated to calculate the mean difference of tunnel position between the four-point quadrant method and the quadrant method. The average of the four measurements of each observer was used for analysis. A post hoc power analysis was performed to determine whether the sample size had sufficient power to detect significant differences in femoral tunnel position. The power was between 81.5 and 99.9% for a sample with 25 cases in each method. The α-level was 0.05. The results of the two methods were evaluated using paired t test. Values of P < 0.05 were considered statistically significant. The value of the ICC was in the range of 0–1 and was applied to the criterion of Landis [13]. The reliability was considered to be almost perfect if the ICC was greater than 0.81, substantial between 0.61 and 0.80, moderate between 0.41 and 0.60, fair between 0.21 and 0.40, and slight 0.0 and 0.20. All statistical analyses were performed using SPSS software, version 24.0 (SPSS, Chicago, IL, USA).
Result
Intra-observer reliability by two orthopaedic surgeons was almost perfect in both depth and height of AM and PL tunnel position (observer1 ICC: AM depth = 0.990, AM height = 0.969, PL depth = 0.995, PL height = 0.979, observer2 ICC: AM depth = 0.968, AM height = 0.988, PL depth = 0.995, PL height = 0.990). Inter-observer reliability of AM tunnel was substantial (ICC: AM depth = 0.730, AM height = 0.729) and that of PL tunnel was almost perfect (ICC: PL depth = 0.895, PL height = 0.859) (Table 1). There were no significant differences in both depth and height of AM and PL tunnel position between the four-point quadrant method and the quadrant method (P value: AM depth = 0.407, AM height = 0.807, PL depth = 0.917, PL height = 0.538). Mean difference was calculated as AM depth1-AM depth, AM height2-AM height, PL depth3-PL depth, PL height4-PL height. Compared with the quadrant method, this study was 0.13% deep and 0.58% high in AM tunnel, 0.01% shallow and 0.13% low in PL tunnel on average (Table 2).
Discussion
The most important finding of this study was that the four-point quadrant method was as highly reliable and as accurate as the quadrant method in the evaluation of femoral tunnel position after anterior cruciate ligament reconstruction. Furthermore, there were no significant differences between the two groups in the AM and PL tunnel position. Bernard et al. [2] developed the quadrant method to identify the femoral tunnel position on a plain lateral radiograph using the quadrant consisting of the Blumensaat’s line as the roof and the outlines of the lateral femoral condyle as the other rectangular borders. Kim et al. [11] described that the Blumensaat’s line is not a single line with a clear boundary but rather a 3- to 5-mm-thick line with blurred boundaries on a simple radiograph, and that it is difficult to discern a reproducible superior border of the lattice on a simple radiograph. Furthermore, important osseous landmarks, such as the lateral intercondylar ridge or the lateral bifurcate ridge, are not visible on conventional radiographs [10]. Therefore, compared with a simple radiograph, 3DCT provides more detailed osseous landmarks, and there is an advantage to accurately visualizing the center of the bone tunnel. Also, Iriuchishima et al. [9] reported that Blumensaat’s line exhibited three types; straight type, small hill type and large hill type. A straight type was observed in only 37%. In this study, the problem was addressed by defining the Blumensaat’s line as the most anterior straight part of the distal femoral condyle. Compared with the quadrant method, this study was 0.13% deep and 0.58% high in AM tunnel, 0.01% shallow and 0.13% low in PL tunnel on average. This is because there were some cases which the tunnel aperture was not a circle but an oval. When the bone tunnel is oval, point1 is deeper, point2 is higher, point3 is shallower, and point4 is lower than when the bone tunnel is circle. The center point of the bone tunnel is measured in the quadrant method, but the tunnel aperture is not always a circle but an oval in some cases [4, 18, 27]. Since the four-point quadrant method is an equivalent method that has no significant differences and is as reliable as the quadrant method, it can be compared with previous studies using the quadrant method. In the previous studies using the quadrant method, the average position of AM depth and height of femoral tunnel were 23.1 and 22.7%, and that of PL depth and height of femoral tunnel were 31.9 and 48.3% (Table 3) [3, 5, 8, 14, 16, 23, 28, 30, 33]. When compared with the previous studies, our AM and PL tunnel position was placed deeper-lower.
In the four-point quadrant method, there is an advantage that measurement can be taken regardless of the shape of the bone tunnel. Although a demerit exists in that the four-point quadrant method needs two more points of measurement, the greatest merit of this method is that it can provide measurement that can be compared with various reconstruction methods such as single-bundle reconstruction, double-bundle reconstruction using hamstring and single-bundle reconstruction using BTB. In particular, comparison between the anatomical rectangular tunnel double-bundle (DB) ACL reconstruction with bone–patellar tendon–bone graft designed by Shino et al. [24] and DB-ACL reconstruction using hamstring tendon will be possible, since varying shapes of each bone tunnel would no longer be problematic with this new method. The four-point quadrant method of this study has clinical relevance in that it is a detailed and accurate tool for evaluating femoral tunnel position after ACL reconstruction.
This study had some limitations. Firstly, compared to the quadrant method by Bernard et al. using standard lateral radiographs, medical costs and radiation exposure will be higher with this method since it uses CT. Secondly, this study has not been compared with various reconstruction methods such as single-bundle reconstruction, double-bundle reconstruction using hamstring and single-bundle reconstruction using BTB.
Conclusion
The four-point quadrant method was found to have high intra- and inter-observer reliability and accuracy. This method can evaluate the tunnel position regardless of the shape and morphology of the bone tunnel aperture for use of comparison. This method is a postoperative evaluation method applicable to various ACL reconstruction methods.
References
Ajuied A, Wong F, Smith C, Norris M, Earnshaw P, Back D, Davies A (2014) Anterior cruciate ligament injury and radiologic progression of knee osteoarthritis: a systematic review and meta-analysis. Am J Sports Med 42(9):2242–2252
Bernard M, Hertel P, Hornung H, Cierpinski T (1997) Femoral insertion of the ACL. Radiographic quadrant method. Am J Knee Surg 10:14–22
Colombet P, Robinson J, Christel P, Franceschi JP, Djian P, Bellier G, Sbihi A (2006) Morphology of anterior cruciate ligament attachments for anatomic reconstruction: a cadaveric dissection and radiographic study. Arthroscopy 22(9):984–992
Dugas JR, Pace JL, Bolt B, Wear SA, Beason DP, Cain EL Jr (2014) Evaluation and comparison of femoral tunnel placement during anterior cruciate ligament reconstruction using 3-dimensional computed tomography: effect of notchplasty on transtibial and medial portal drilling. Orthop J Sports Med. https://doi.org/10.1177/2325967114525572
Forsythe B, Kopf S, Wong AK, Martins CA, Anderst W, Tashman S, Fu FH (2010) The location of femoral and tibial tunnels in anatomic double-bundle anterior cruciate ligament reconstruction analyzed by three-dimensional computed tomography models. J Bone Jt Surg Am 92(6):1418–1426
Giron F, Cuomo P, Aglietti P, Bull AM, Amis AA (2006) Femoral attachment of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc 14(3):250–256
Hoser C, Tecklenburg K, Kuenzel KH, Fink C (2005) Postoperative evaluation of femoral tunnel position in ACL reconstruction: plain radiography versus computed tomography. Knee Surg Sports Traumatol Arthrosc 13(4):256–262
Iriuchishima T, Ingham SJ, Tajima G, Horaguchi T, Saito A, Tokuhashi Y, Van Houten AH, Aerts MM, Fu FH (2010) Evaluation of the tunnel placement in the anatomical double-bundle ACL reconstruction: a cadaver study. Knee Surg Sports Traumatol Arthrosc 18(9):1226–1231
Iriuchishima T, Ryu K, Aizawa S, Fu FH (2016) Blumensaat’s line is not always straight: morphological variations of the lateral wall of the femoral intercondylar notch. Knee Surg Sports Traumatol Arthrosc 24(9):2752–2757
Kamath GV, Redfern JC, Greis PE, Burks RT (2011) Revision anterior cruciate ligament reconstruction. Am J Sports Med 39(1):199–217
Kim DH, Lim WB, Cho SW, Lim CW, Jo S (2016) Reliability of 3-dimensional computed tomography for application of the Bernard quadrant method in femoral tunnel position evaluation after anatomic anterior cruciate ligament reconstruction. Arthroscopy 32(8):1660–1666
Kopf S, Forsythe B, Wong AK, Tashman S, Anderst W, Irrgang JJ, Fu FH (2010) Nonanatomic tunnel position in traditional transtibial single-bundle anterior cruciate ligament reconstruction evaluated by three-dimensional computed tomography. J Bone Jt Surg Am 92(6):1427–1431
Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data. Biometrics 33(1):159–174
Lee JK, Lee S, Seong SC, Lee MC (2015) Anatomy of the anterior cruciate ligament insertion sites: comparison of plain radiography and three-dimensional computed tomographic imaging to anatomic dissection. Knee Surg Sports Traumatol Arthrosc 23(8):2297–2305
Lertwanich P, Martins CA, Asai S, Ingham SJ, Smolinski P, Fu FH (2011) Anterior cruciate ligament tunnel position measurement reliability on 3-dimensional reconstructed computed tomography. Arthroscopy 27(3):391–398
Lorenz S, Elser F, Mitterer M, Obst T, Imhoff AB (2009) Radiologic evaluation of the insertion sites of the 2 functional bundles of the anterior cruciate ligament using 3-dimensional computed tomography. Am J Sports Med 37(12):2368–2376
Matassi F, Sirleo L, Carulli C, Innocenti M (2015) Anatomical anterior cruciate ligament reconstruction: transtibial versus outside–in technique. Joints 3(1):6–14
Miller CD, Gerdeman AC, Hart JM, Bennett CG, Golish SR, Gaskin C, Miller MD (2011) A comparison of 2 drilling techniques on the femoral tunnel for anterior cruciate ligament reconstruction. Arthroscopy 27(3):372–379
Muneta T, Yamamoto H, Sakai H, Ishibashi T, Furuya K (1993) Relationship between changes in length and force in in vitro reconstructed anterior cruciate ligament. Am J Sports Med 21(2):299–304
Murawski CD, Wolf MR, Araki D, Muller B, Tashman S, Fu FH (2013) Anatomic anterior cruciate ligament reconstruction: current concepts and future perspective. Cartilage 4(3):27S-37S
Musahl V, Plakseychuk A, VanScyoc A, Sasaki T, Debski RE, McMahon PJ, Fu FH (2005) Varying femoral tunnels between the anatomical footprint and isometric positions: effect on kinematics of the anterior cruciate ligament-reconstructed knee. Am J Sports Med 33(5):712–718
Park JS, Park JH, Wang JH, Oh CH, Hwang MH, Lee SH, Kim JG (2015) Comparison of femoral tunnel geometry, using in vivo 3-dimensionalcomputed tomography, during transportal and outside-in single-bundle anterior cruciate ligament reconstruction techniques. Arthroscopy 31(1):83–91
Pietrini SD, Ziegler CG, Anderson CJ, Wijdicks CA, Westerhaus BD, Johansen S, Engebretsen L, LaPrade RF (2011) Radiographic landmarks for tunnel positioning in double-bundle ACL reconstructions. Knee Surg Sports Traumatol Arthrosc 19(5):792–800
Shino K, Nakata K, Nakamura N, Toritsuka Y, Horibe S, Nakagawa S, Suzuki T (2008) Rectangular tunnel double-bundle anterior cruciate ligament reconstruction with bone–patellar tendon–bone graft to mimic natural fiber arrangement. Arthroscopy 24(10):1178–1183
Sim JA, Kim JM, Lee S, Bae JY, Seon JK (2017) Comparison of tunnel variability between trans‑portal and outside‑in techniques in ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 25(4):1227–1233
Takeda Y, Iwame T, Takasago T, Kondo K, Goto T, Fujii K, Naruse A (2013) Comparison of tunnel orientation between transtibial and anteromedial portal techniques for anatomic double-bundle anterior cruciate ligament reconstruction using 3-dimensional computed tomography. Arthroscopy 29(2):195–204
Tashiro Y, Okazaki K, Uemura M, Toyoda K, Osaki K, Matsubara H, Hashizume M, Iwamoto Y (2014) Comparison of transtibial and transportal techniques in drilling femoral tunnels during anterior cruciate ligament reconstruction using 3D-CAD models. Open Access J Sports Med 5:65–72
Tsukada H, Ishibashi Y, Tsuda E, Fukuda A, Toh S (2008) Anatomical analysis of the anterior cruciate ligament femoral and tibial footprints. J Orthop Sci 13(2):122–129
Van Eck CF, Lesniak BP, Schreiber VM, Fu FH (2010) Anatomic single- and double-bundle anterior cruciate ligament reconstruction flowchart. Arthroscopy 26(2):258–268
Yamamoto Y, Hsu WH, Woo SL, Van Scyoc AH, Takakura Y, Debski RE (2004) Knee stability and graft function after anterior cruciate ligament reconstruction: a comparison of a lateral and an anatomical femoral tunnel placement. Am J Sports Med 32(8):1825–1832
Zantop T, Diermann N, Schumacher T, Schanz S, Fu FH, Petersen W (2008) Anatomical and nonanatomical double-bundle anterior cruciate ligament reconstruction: importance of femoral tunnel location on knee kinematics. Am J Sports Med 36(4):678–685
Zantop T, Petersen W, Sekiya JK, Muhsal V, Fu FH (2006) Anterior cruciate ligament anatomy and function relating to anatomical reconstruction. Knee Surg Sports Traumatol Arthrosc 14(10):982–992
Zantop T, Wellmann M, Fu FH, Petersen W (2008) Tunnel positioning of anteromedial and posterolateral bundles in anatomic anterior cruciate ligament reconstruction: anatomic and radiographic findings. Am J Sports Med 36(1):65–72
Zavras TD, Race A, Amis AA (2005) The effect of femoral attachment location on anterior cruciate ligament reconstruction: graft tension patterns and restoration of normal anterior–posterior laxity patterns. Knee Surg Sports Traumatol Arthrosc 13(2):92–100
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and publication of this article.
Ethical approval
The study was approved by the Ethics Committee of Toho University Ohashi Medical Center (No. H16110).
Informed consent
Patient were informed, and they consented to conduct the study.
Rights and permissions
About this article

Cite this article
Mochizuki, Y., Kaneko, T., Kawahara, K. et al. The quadrant method measuring four points is as a reliable and accurate as the quadrant method in the evaluation after anatomical double-bundle ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 26, 2389–2394 (2018). https://doi.org/10.1007/s00167-017-4797-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-017-4797-y