
Abstract
Purpose
This pilot study was designed to describe the technical details and to present the preliminary outcome of autologous matrix-induced chondrogenesis (AMIC) combined with platelet-rich plasma gel, the so called AMIC plus technique, for the treatment of patellar cartilage defects in the knee.
Methods
The AMIC plus technique was used for the treatment of (osteo) chondral patellar lesions in the knee. The surgical technique is extensively described. Five patients were clinically prospectively evaluated during 2 years. MRI data were analysed based on the original MOCART (Magnetic Resonance Observation of Cartilage Repair Tissue) and modified MOCART scoring system.
Results
A clinical improvement became apparent after 24 months of follow-up. Both MOCART scoring systems revealed no significant deterioration or improvement of the repair tissue between one and 2 years of follow-up. However, all cases showed subchondral lamina and bone changes. The formation of intralesional osteophytes was observed in 3 of the 5 patients during the 2 years of follow-up.
Conclusions
AMIC plus is feasible for the treatment of symptomatic patellar cartilage defects and resulted in a clinical improvement in all patients. The favourable clinical outcome of the AMIC plus technique was not confirmed by the MRI findings.
Level of evidence
IV.
Similar content being viewed by others



Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Surgical treatment for articular cartilage injury is of major interest to orthopaedic surgeons because most lesions of articular cartilage do not heal spontaneously and may predispose the joint to the subsequent development of secondary osteoarthritis [5, 33]. Various techniques have been used to treat this injury with variable success rates. The ultimate aim of treatment is the restoration of normal knee function by regenerating hyaline cartilage in the defect and complete integration of the regenerated cartilage with the surrounding cartilage and underlying bone. Several marrow-stimulating procedures directed at the recruitment of bone marrow cells have been widely used to treat local cartilage defects. In this type of procedures, mesenchymal stem cells (MSCs) migrate in the fibrin network of the blood clot [6]. However, the fibrin clot is not mechanically stable to withstand the tangential forces [8]. As described by Gille et al. [12], an implanted exogenous scaffold (e.g. a collagen matrix) may improve the mechanical stability and durability for endogenous cells and may provide a proper stimulus for chondrogenic differentiation and cartilage regeneration. The original AMIC (autologous matrix-induced chondrogenesis) procedure provides two major advantages; on the one hand, it is a one-step procedure with no need of cartilage harvesting potentially leading to donor site morbidity, and on the other hand, it is cost-effective with no need of in vitro cell expansion [3].
Articular cartilage disease of the patella is still a challenging problem in orthopaedic surgery. In the present pilot study, the AMIC procedure using a collagen I/III scaffold combined with platelet-rich plasma gel (AMIC plus) is used for the treatment of chondral and osteochondral patellar lesions in the knee. The technique is extensively described in this paper. Platelet-rich plasma (PRP) is a general term for new technologies that are focused on enhancing the healing response after injury of different tissue types and may have certain applications that will speed recovery in cases of tendon, ligament, muscle and cartilage disorders [18]. PRP has already shown to have a positive effect on cartilage [21]. We therefore hypothesized that with the help of PRP in a gel form and the collagen I/III scaffold, bone marrow cells can be guided to the cartilage defect and enhance the induction of chondrogenic cells. We report in this pilot study, the clinical and magnetic resonance imaging (MRI) outcome of the first 5 patients treated with the AMIC plus technique in the Ghent University Hospital since January 2008. The goal of this short-term pilot study was to determine whether the AMIC plus technique is suitable for the treatment of patellar cartilage defects in the knee.
Materials and methods
Patients with focal cartilage defects involving the patella and with clinical symptoms (pain, swelling, locking and “giving away”) were eligible for treatment. Exclusion criteria were age under 18 and over 50 years, untreatable tibiofemoral or patellofemoral malalignment or instability, diffuse osteoarthritis or bipolar “kissing” lesions, major meniscal deficiency and other general medical conditions such as diabetes or rheumatoid arthritis. Clinical experimentation was approved by the Hospital Ethics Committee. Informed consent to participate in the study and to comply with the postoperative regimen was obtained from all patients. The patients included in this pilot study were treated between January and April 2008.
Five patients (3 men and 2 women) were treated consecutively and followed for 24 months. The right-to-left side ratio was 3:2. The lesions were focal in all cases and were located all on the patella. All lesions were International Cartilage Repair Society grade III–IV [14] and had a median size of 2 cm2 (range, 1–3 cm2). The cause of injury was focal nontraumatic (focal degenerative lesions) in all 5 cases. The median age of the patients was 27 years (range, 24–45 years). The median duration of symptoms before surgery was 4 months (range, 1–10 months). Associated procedures were performed in 3 patients: 3 Fulkerson osteotomies and 1 medial patellofemoral ligament reconstruction.
Surgical procedure
A miniarthrotomy in a tourniquet-controlled bloodless surgical field was performed to allow access to the defect. The lesion was measured after the bottom of the cartilage defect was freshened, and the edges of the defect were trimmed back to stable walls of healthy cartilage. Microfracturing is performed with slow speed drilling (drill bit diameter 1.2 mm). When the size of the defect is evaluated, the collagen membrane is measured. The collagen I/III membrane (Chondro-Gide®) should be slightly undersized to avoid dislocation after movement and was fixated with sutures (Vicryl 6/0) (Fig. 1). Before the defect was sealed completely, a small opening was left unsutured for the application of platelet-rich plasma (PRP) gel (GPS® III System Advantages, Biomet). The platelet-rich plasma gel was inserted manually and applied beneath the membrane. The remaining opening was closed entirely after the application of the PRP gel beneath the collagen membrane (Fig. 2). The joint was then gently moved intraoperatively to evaluate whether the membrane remained in place.

The collagen membrane is fixated with sutures, and the platelet-rich plasma gel is applied beneath the membrane

Schematic illustrations of the performed procedure:1 Schematic drawing of a cartilage lesion. 2 Debridement of the cartilage defect until stable walls of healthy cartilage and microfracturing of the cartilage lesion. 3 Suturing of the collagen I/III membrane, leaving a small opening for the application of the PRP gel. 4 Application of the PRP gel beneath the collagen I/III membrane and closing the remaining opening with sutures (corresponds with the photograph)
The postoperative regimen was as follows: nonweightbearing during 2 weeks. Achieving a normal gait pattern was advised at 10 weeks postoperatively. An extension brace was prescribed for the first 4 weeks after surgery. Maximum active flexion did not exceed 15° for the first 2 weeks of rehabilitation. Full range of motion was allowed 8 weeks postoperatively. Isometric quadriceps training, straight length raising and hamstrings isometrics were advised during the first 2 weeks. Return to low impact sports was allowed 12 months after surgery.
Clinical evaluation
All 5 patients were clinically prospectively evaluated with use of the Knee injury and Osteoarthritis Outcome Score (KOOS) [2, 28–30], the Tegner activity scale [35, 36], Kujala patellofemoral score [17] and the visual analogue scale (VAS) [4, 10] for pain preoperatively and at 12 and 24 months of follow-up.
MRI technique
All MRI examinations before the operation and at 12 and 24 months of follow-up were performed on a 1.5 T or a 3 T MR unit (Either a Magnetom Avanto, a Magnetom Symphony Tim or Magnetom Trio, Siemens Medical Solutions, Erlangen, Germany). All five patients had consented to follow the postoperative MRI evaluation protocol. We performed a standard knee MRI protocol including proton-density- and T2-weighted turbo spin echo (TSE) acquisitions using a dedicated send-receive eight channel knee coil. Imaging parameters of the sequences were as follows:
-
Sagittal proton-density- and T2-weighted turbo spin echo (TSE) images (TE: 24/96 ms TR: 4,000 ms on 1.5 T; TE: 22/101 ms TR: 4,662 ms on 3T; slice thickness: 3 mm with a 0.3 mm intersection gap; field of view (FOV): 180 mm; matrix size: 512 × 307 on 1.5 T MR unit, 448 × 246 on 3T MR unit) (Fig. 3).
Fig. 3 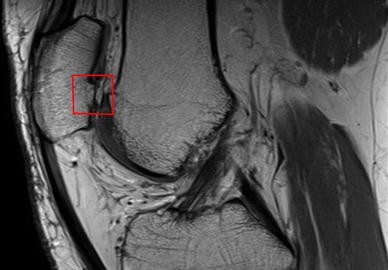
Sagittal proton-density- and T2-weighted turbo spin echo (TSE) image on 3 T MR unit. The red square shows an upcoming subchondral bone plate with thinning of the covering cartilage, resulting in the formation of an intralesional osteophyte 2 years after surgery
-
Coronal proton-density-weighted images with fat saturation (TE: 43 ms TR: 4,400 ms on 1.5 T; TE: 44 ms TR: 3,140 ms on 3T; slice thickness: 3 mm; FOV: 180 mm, matrix size: 512 × 240 on 1.5 T MR unit, 448 × 218 on 3T MR unit).
-
Transverse 3D dual echo steady state (DESS 3D) images, a gradient echo (GRE) sequence (TE: 5.5 ms TR: 19 ms; flip angle: 25°; slice thickness: 3 mm, FOV: 160 mm; matrix size: 256 × 156).
-
Sagittal 3D fast low-angle shot images with water excitation images (Flash 3Dwe) (only on 1.5 T MR unit): spoiled GRE. (TE: 27.0 ms; TR: 13.7 ms; flip angle: 30°; slice thickness: 1 mm consecutively; FOV: 180 mm; matrix size: 512 × 240).
-
Sagittal 3D proton-density SPACE images with fat saturation (only on 3 T MR unit) (TE: 43 ms TR: 1,100 ms; slice thickness 0.6 mm, FOV: 160 mm, matrix size: 320 × 269).

Original and modified MOCART system
For the description of the repair tissue, we used the original MOCART system previously published by Marlovits et al. [19, 20]. Nine variables were used to describe the morphology and signal intensity of the repair tissue compared to the adjacent native cartilage. Besides the original MOCART system, we also used a modification of this system previously published by Dhollander et al. [7]. Both morphological MRI classification systems were applied to the MRI images taken at 12 and 24 months of follow-up. All MR images were evaluated by a senior musculoskeletal radiologist. Both the original and modified MOCART scores were expressed as a percentage of the maximum score [7].
Statistical analysis
All data are expressed in terms of medians and ranges. Descriptive statistical analysis was performed using PASW statistics 18 (SPSS Inc, Chicago, Illinois).
Results
During the follow-up period, the VAS scores for pain indicated by the patients improved markedly. Preoperatively, the median VAS score was 52 mm (range, 14–86 mm) at 1-year follow-up 36 mm (range, 11–51 mm) and at 2 years of follow-up 14 mm (5–19 mm). According to the Tegner activity scale, no obvious differences were observed during the 24-month follow-up period. Before the operation, the median Tegner score was 2 (range, 1–3), 1 year after surgery 2 (range, 1–3) and at 2 years of follow-up, the median Tegner score was 3 (range, 2–3). Kujala patellofemoral scores revealed an obvious improvement between preoperative and 24 months of follow-up [medians preoperatively: 38 (range, 30–55), at 1 year of follow-up: 64 (range 38–67), and at 2 years of follow-up: 71 (range, 53–82)]. All KOOS subscale scores (ADL, Pain, Symptoms/Stiffness, QoL, and Sports and Recreational Activities) improved when preoperative and postoperative values were compared (Fig. 4).

Median values of the KOOS subscales. Pain: preoperative (pre; 64) (range, 39–92) and postoperative: 12 months (78) (range, 50–86) and 24 months (92) (range, 61–97). Symptoms/Stiffness: preoperative (pre; 39) (range, 36–86) and postoperative: 12 months (82) (range, 43–86) and 24 months (82) (range, 75–100). Activities of Daily Living: preoperative (pre; 65) (range, 38–76) and postoperative: 12 months (82) (range, 34–96) and 24 months (93) (range, 62–97). Sports and Recreational Activities: preoperative (pre; 15) (range, 0–20) and postoperative: 12 months (50) (range, 5–50) and 24 months (40) (range, 10–45). Quality of Life: preoperative (pre; 25) (range, 19–31) and postoperative: 12 months (25) (range, 13–69) and 24 months (50) (range, 38–56)
No infections occurred in the postoperative period. One patient underwent a second-look arthroscopy because of catching, revealing hypertrophy of the regenerated tissue, which was adequately treated by shaving.
Twenty-four month longitudinal follow-up of the repair tissue with the original and MOCART system
At the 24-month follow-up, it was shown that the original MOCART score remains stable over time [medians at 1 year of follow-up: 53% (range, 47–59%) and at 2 years of follow-up: 53% (range, 47–59%)]. As with the original MOCART system, a higher modified MOCART system score signified a more cartilage-like aspect of the repair tissue on MRI and a more complete filling of the defect, without it being overfilled. The percentages also remained stable over time [medians at 1 year of follow-up: 38% (range, 38–45%) and at 2 years of follow-up: 38% (range, 33–45%)].
MRI data evaluated with the original MOCART system at 12 and 24 months of follow-up
One and two years after the AMIC plus procedure, the MRI data were analysed according to original MOCART system [28]. At 12 months of follow-up, complete filling of the defect was not seen. Incomplete filling was observed in 3 cases (60%). Hypertrophy of the repair tissue was seen in 2 patients (40%). Complete integration of the border zone with the adjacent cartilage was observed in all patients. The surface of the repair tissue was irregular and had an inhomogeneous structure in all patients. An intact subchondral lamina and an intact subchondral bone were not seen. Adhesions and effusions were absent in all cases. The signal intensities were described as isointense in none of the patients. For all variables of the original MOCART, except for the variable ‘integration to the border zone’, the same results were obtained 2 years postoperatively. With one patient, we observed the occurrence of a split between the repair tissue and adjacent cartilage at 24 months of follow-up. In general, the formation of intralesional osteophytes was observed in 3 of the 5 patients during the 2 years after surgery.
Discussion
The most important finding of the present study is that the AMIC plus procedure is feasible for the treatment of patellar cartilage defects in the knee. In general, bone marrow stimulation techniques produce similar results in comparison with autologous chondrocyte implantation [15]. Although the treatment of patellar chondral lesions seems uncommon in some countries such as the United States, using cartilage repair techniques for patellar lesions has become more and more accepted [9]. This is represented by some studies exclusively dealing with the issue of Autologous Chondrocyte Implantation (ACI) for patellar defects [13, 22, 24]. Nevertheless, clinical results still seem inferior to those of defects located on the femoral condyles [16, 24, 27, 32]. We report in this pilot study, the clinical results obtained of the first five patients treated with the AMIC plus technique for patellar cartilage lesions. The patients who participated in this study showed a gradual clinical improvement after surgery. No decline in clinical outcome was observed. The clinical results are similar to those of other techniques, taking into account this small and challenging patient cohort [12, 26].
In the present study, both the original and the modified MOCART system were used in a longitudinal fashion to evaluate the repair tissue. Both scores were moderate and remained stable over time. The MRI findings of the repair tissue showed no signs of deterioration or improvement during the 24 months of follow-up.
Based on the original MOCART system, we analysed our patient group 12 and 24 months after the AMIC plus procedure. The majority of the chondral repair tissue filled the defect depth sufficiently. In contrast to the findings of Gille et al. [12], we observed an irregular surface of the repair tissue in most of the cases and neither was the repair tissue isointense to the surrounding cartilage. We found subchondral lamina and bone changes in all patients at each follow-up moment. Moreover, the formation of intralesional osteophytes was observed in 3 of the 5 patients during the 2 years of follow-up. Two patients developed hypertrophy of the repair tissue observed on MRI. One patient underwent a second-look arthroscopy because of catching due to this finding. We observed a high incidence of hypertrophy of the repair tissue (40%), but a good integration with adjacent cartilage (80%) at 24 months of follow-up on MRI. These findings are comparable with those published by Niemeyer et al. [25].
In contrast to other cartilage repair procedures, the AMIC procedure is quite easy to handle and can be done in a one-step surgery. There is no need for harvesting autologous cartilage. In this way, in vitro propagation of chondrocytes and the concomitant dedifferentiation issues are avoided. Therefore, this technique is less expensive, less time intensive and offers availability to all patients. In the original AMIC procedure published by Benthien et al., the collagen membrane is fixed with commercial fibrin glue [3]. In the series published by Gille et al., a semiautologous fibrin glue was used [12]. This type of fibrin glue is believed to offer superior properties than the commercial fibrin glue [11]. In the described AMIC plus technique, we used sutures the fixation of the collagen membrane to ensure a secure fixation. We did not observe transplant loosening, debonding of the graft or ablation and in turn clinical complications and reoperations.
In previous studies, the hypothesis was verified that perforation of the subchondral bone plate gives rise to the stem cell pool of the bone marrow and leads to release of further marrow elements as growth factors and cytokines [34]. The original AMIC procedure combines microfracture with a collagen I/III membrane (Chondro-Gide®) and fibrin glue. The AMIC plus procedure combines microfracture with the same collagen membrane type and platelet-rich plasma gel (PRP). Collagen scaffolds have already been used in many studies that have loaded chondrocytes or MSCs to build cartilage in vitro and in vivo [1, 23, 31]. These membranes allow cell growth and seem to improve the mechanical stability of the initially formed fibrin clot. We hypothesized that the combination of PRP gel and a collagen membrane would enhance the formation of hyaline-like repair tissue. Platelet-rich plasma (PRP) therapy is a simple, low cost and minimally invasive method that allows a natural concentrate of autologous growth factors to be obtained from the blood. PRP has shown to stimulate cartilage repair after microfracture in a sheep model. The procedure was more effective when PRP was used in a gel form [21]. The preliminary results of this pilot study did not confirm the hypothesis that the combination of PRP gel and a collagen membrane enhances the formation of hyaline-like repair tissue. In other words, the supplemental use of PRP gel did not seem to have obvious beneficial effects on the cartilage repair process.
It must be emphasized that the small sample size lacked the necessary statistical power, that the follow-up period was limited to 24 months and that all MR images were evaluated by only one musculoskeletal radiologist. An important drawback of this pilot study population is the fact that associated procedures were performed in 3 patients: 3 Fulkerson osteotomies and 1 medial patellofemoral ligament reconstruction. These limitations do not allow a broad generalization of the findings observed in this study, but can be seen as an incentive for future research under the same theme.
Conclusion
This pilot study—with a combination of microfracture, PRP and collagen membrane—used in cartilage repair, which is the first to be described in the literature—allows us to present the first clinical and MRI outcome at 2 years postsurgery and now serves as a control for future studies with modified protocols. The key finding in this pilot study is that the AMIC plus procedure is feasible for the treatment of patellar cartilage defects in the knee. The patients who participated in this study showed a gradual clinical improvement during 24 months of follow-up. However, the gradual short-term clinical improvement of AMIC plus procedure was not confirmed by the MRI data. All cases showed subchondral lamina and bone changes. Moreover, the formation of intralesional osteophytes was observed in 3 of the 5 patients during the 2 years of follow-up. Long-term and randomized controlled studies are mandatory to confirm the initial results and the reliability of this procedure.
References
Behrens P, Bitter T, Kurz B, Russlies M (2006) Matrix-associated autologous chondrocyte transplantation/implantation (MACT/MACI)–5-year follow-up. Knee 13:194–202
Bekkers JE, de Windt TS, Raijmakers NJ, Dhert WJ, Saris DB (2009) Validation of the knee injury and osteoarthritis outcome score (KOOS) for the treatment of focal cartilage lesions. Osteoarthr Cartil 17:1434–1439
Benthien JP, Behrens P (2010) Autologous matrix-induced chondrogenesis (AMIC) combining microfracturing and a collagen I/III matrix for articular cartilage resurfacing. Cartilage 1:65–68
Bijur PE, Silver W, Gallagher EJ (2001) Reliability of the visual analog scale for measurement of acute pain. Acad Emerg Med 8:1153–1157
Buckwalter JA, Lane NE (1997) Athletics and osteoarthritis. Am J Sports Med 25:873–881
Cerynik DL, Lewullis GE, Joves BC, Palmer MP, Tom JA (2009) Outcomes of microfracture in professional basketball players. Knee Surg Sports Traumatol Arthrosc 17:1135–1139
Dhollander AAM, Huysse WCJ, Almqvist KF, Verdonk PCM, Verstraete KL, Verdonk R, Verbruggen G (2010) MRI evaluation of a new scaffold-based allogenic chondrocyte implantation for cartilage repair. Eur J Radiol 75:72–81
Dorotka R, Windberger U, Macfelda K, Bindreiter U, Toma C, Nehrer S (2005) Repair of articular cartilage defects treated by microfracture and a three-dimensional collagen matrix. Biomaterials 26:3617–3629
Farr J (2007) Autologous chondrocyte implantation improves patellofemoral cartilage treatment outcomes. Clin Orthop Relat Res 463:187–194
Gallaher EJ, Bijur PE, Laimer C, Silver W (2002) Reliability and validity of a visual analog scale for acute abdominal pain in the ED. Am J Emerg Med 20:287–290
Gille J, Meisner U, Ehlers EM, Muller A, Russlies M, Behrens P (2005) Migration pattern, morphology and viability of cells suspended in or sealed with fibrin glue: a histomorphologic study. Tissue Cell 37:339–348
Gille J, Schuseil E, Wimmer J, Gellissen J, Schulz AP, Behrens P (2010) Mid-term results of autologous matrix-induced chondrogenesis for treatment of focal cartilage defects in the knee. Knee Surg Sports Traumatol Arthrosc 18:1456–1464
Gobbi A, Kon E, Berruto M, Francisco R, Filardo G, Marcacci M (2006) Patellofemoral full-thickness chondral defects treated with Hyalograft-C: a clinical, arthroscopic, and histologic review. Am J Sports Med 34:1763–1773
Hjelle K, Soljeim E, Strand T, Muri R, Brittberg M (2002) Articular cartilage defects in 1,000 knee arthroscopies. Arthroscopy 18:730–734
Knutsen G, Drogset JO, Engebretsen L, Grontvedt T, Isaksen V, Ludvigsen TC, Roberts S, Solheim E, Strand T, Johansen O (2007) A randomized trial comparing autologous chondrocyte implantation with microfracture. Findings at five years. J Bone Joint Surg Am 89:2105–2112
Kreuz PC, Steinwachs M, Erggelet C, Krause SJ, Ossendorf C, Maier D, Ghanem N, Uhl M, Haag M (2007) Classification of graft hypertrophy after autologous chondrocyte implantation of full-thickness chondral defects in the knee. Osteoarthritis Cart 15:1339–1347
Kujala UM, Jaakkola LH, Koskinen SK, Taimela S, Hurme M, Nelimarkka O (1993) Scoring of patellofemoral disorders. Arthroscopy 9:159–163
Lopez-Vidriero E, Goulding KA, Simon DA, Sanchez M, Johnson DH (2010) The use of platelet-rich plasma in arthroscopy and sports medicine: optimizing the healing environment. Arthroscopy 26:269–278
Marlovits S, Singer P, Zeller P, Mandl I, Haller J, Trattning S (2006) Magnetic resonance observation of cartilage repair tissue (MOCART) for the evaluation of autologous chondrocyte transplantation: determination of interobserver variability and correlation to clinical outcome after 2 years. Eur J Radiol 57:16–23
Marlovits S, Striessnig G, Resinger CT, Aldrian SM, Vecsei V, Imhof H, Trattnig S (2004) Definition of pertinent parameters for the evaluation of articular cartilage repair tissue with high-resolution magnetic resonance imaging. Eur J Radiol 52:310–319
Milano G, Passino ES, Deriu L, Careddu G, Manunta L, Manunta A, Saccomanno MF, Fabbriciani C (2010) The effect of platelet rich plasma combined with microfractures on the treatment of chondral defects. An experimental study in a sheep model. Osteoarthr Cartil 18:971–980
Minas T, Bryant T (2005) The role of autologous chondrocyte implantation in the patellofemoral joint. Clin Orthop Relat Res 436:30–39
Nehrer S, Breinan HA, Ramappa A, Shortkroff S, Young G, Minas T, Sledge CB, Yannas IV, Spector M (1997) Canine chondrocytes seeded in type I and type II collagen implants investigated in vitro. J Biomed Mater Res 38:95–104
Niemeyer P, Steinwachs M, Erggelet C, Kreuz PC, Kraft N, Köstler W, Mehlhorn A, Südkam NP (2008) Autologous chondrocyte implantation for the treatment of retropatellar cartilage defects: clinical results referred to defect localisation. Arch Orthop Trauma Surg 128:1223–1231
Niemeyer P, Petska JM, Kreuz PC, Erggelet C, Schmal H, Suedkamp NP, Steinwachs M (2008) Characteristic complications after autologous chondrocyte implantation for cartilage defects of the knee joint. Am J Sports Med 36:2091–2099
Pascual-Garrido C, Slabaugh MA, L’Heureux DR, Friel NA, Cole BJ (2009) Recommendations and treatment outcomes for patellofemoral articular cartilage defects with autologous chondrocyte implantation: prospective evaluation at average 4-year follow-up. Am J Sports Med 37:33–41
Peterson L, Minas T, Brittberg M, Nilsson A, Sjogren-Jansson E, Lindahl A (2000) Two- to 9-year outcome after autologous chondrocyte transplantation of the knee. Clin Orthop Relat Res 374:212–234
Roos EM, Roos HP, Ekdahl C, Lohmander LS (1998) Knee injury and osteoarthritis outcome score (KOOS): validation of a Swedish version. Scand J Med Sci Sports 8:439–448
Roos EM, Roos HP, Lohmander LS, Ekdahl C, Beynnon BD (1998) Knee injury and osteoarthritis outcome score (KOOS): development of a self-administered outcome measure. J Orthop Sports Phys Ther 28:88–96
Roos EM, Toksvig-Larsen S (2003) Knee injury and osteoarthritis outcome score (KOOS): validation and comparison to the WOMAC in total knee replacement. Health Qual Life Outcomes 1:17
Russlies M, Behrens P, Ehlers EM, Brohl C, Vindigni C, Spector M, Kurz B (2005) Periosteum stimulates subchondral bone densification in autologous chondrocyte transplantation in a sheep model. Cell Tissue Res 319:133–142
Saris DBF, Vanlauwe J, Victor J, Almqvist KF, Verdonk R, Bellemans J, Luyten FP (2009) Treatment of symptomatic cartilage defects of the knee: characterized chondrocyte implantation results in better clinical outcome at 36 months in a randomized trial compared to microfracture. Am J Sports Med 37:10–19
Shapiro F, Koide S, Glimcher MJ (1993) Cell origin and differentiation in the repair of full-thickness defects of articular cartilage. J Bone Joint Surg Am 75:532–553
Steadman JR, Rodkey WG, Briggs KK (2002) Microfracture to treat full-thickness chondral defects: surgical technique, rehabilitation, and outcomes. J Knee Surg 15:170–176
Tegner Y (1985) Cruciate ligament injuries in the knee: evaluation and rehabilitation [dissertation]. Linköping University, Linköping
Tegner Y, Lysholm J (1985) Rating systems in the evaluation of knee ligament injuries. Clin Orthop 198:43–49
Acknowledgments
The authors would like to thank K. Verstraete and W. Huysse of the Department of Radiology, Ghent University for their support concerning the application of the Magnetic Resonance Imaging facilities.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dhollander, A.A.M., De Neve, F., Almqvist, K.F. et al. Autologous matrix-induced chondrogenesis combined with platelet-rich plasma gel: technical description and a five pilot patients report. Knee Surg Sports Traumatol Arthrosc 19, 536–542 (2011). https://doi.org/10.1007/s00167-010-1337-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-010-1337-4