
Abstract
Pharmaceuticals, a group of emerging contaminants (ECs), have aroused serious concern owing to their detection at levels threatening to the health of the ecosystem. India is one of the top producers and consumers of pharmaceuticals in the world. Recent studies conducted on pharmaceutical residues in the Indian environmental matrices reported unsurpassed levels of antibiotics and nonsteroidal anti-inflammatory drugs (NSAIDs). Reports submit the fact that India carries the largest burden of drug-resistant pathogens with anti-resistant genes (ARGs) in river water of India. Despite posing potential risk to the public health, pharmaceuticals still stand unregulated. Several advanced wastewater treatment technologies such as the photodegradation, adsorption, membrane filtration, catalytic oxidation, etc. have been devised for efficient removal of this special class of chemical compounds. A comprehensive documentation has been provided in the chapter as an attempt to acquire state of knowledge on occurrence, ecological risks, and possible decontamination techniques with respect to pharmaceuticals in the Indian environment.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Pharmaceutical residue
- Emerging contaminant
- Indian waters
- Antibiotic resistance
- Environmental risk
- Risk quotient
- Remediation techniques
1 Introduction
Although the use of pharmaceuticals is inevitable in our daily lives, the amount of chemicals discharged into the environment is voluminous and is reported to be at par with the amount of pesticides used annually (Daughton and Ternes 1999). As a result of their continuous use and discharge into the environment, pharmaceutical compounds accumulate in the environment. PPCPs gained considerable attention as environmental pollutants when the US Geological Survey between 1992 and 2000 reported 82 chemicals, including a variety of PPCPs in 139 waterways (Kolpin et al. 2002). One research revealed 713 pharmaceuticals (142 as transformation products) in the environment (IWW 2014). These organic pollutants are considered a part of emerging contaminants (ECs), which enter the aquatic systems from various point and non-point sources (Archer et al. 2017).
The emerging risks associated with the use of pharmaceuticals were recognized when studies linked their effects with the biological activity in organisms such as feminization of fish, induction of vitellogenin synthesis in male aquatic organisms, and acute renal failure in white-backed vultures (Santos et al. 2010). The pollution of the environment resulting from increased use and discharge of human and veterinary medicines in parent or metabolite form poses a threat to the health of the ecosystem including humans through drinking water supplies and contaminated food products. Their overuse may induce resistance in humans and animals through prolonged exposure.
Although the presence of pharmaceuticals in the environment is an emanating threat to the health of the ecosystem, these groups of chemicals do not face any regulatory guideline on their discharge limits at present. There are no specific legal requirements to monitor the levels of pharmaceuticals even in drinking water on a global scale. Hence, it is important to identify the problems associated with their use and residual effects on the environment so that necessary remedial measures may be adopted.
2 Major Classes of Pharmaceuticals
In the year 2008, United States Environmental Protection Agency (US EPA) proposed the universal waste rule and defines pharmaceutical as any chemical product, vaccine or allergen, not containing a radioactive component, that is intended for use in the diagnosis, cure, mitigation, treatment, or prevention of disease or injury in man or other animals (US EPA 2012). Today, pharmaceuticals are not only used for treating human and veterinary medical ailments but are also actively engaged in aquacultural practices and used as herbicides and as growth promoters in animal husbandry. They include a vast group of chemical compounds having different structures, chemical properties, and therapeutic modes of action. Depending on their intended use, pharmaceuticals can be categorized to include the following groups of compounds shown in Table 1. Table 2 shows the physicochemical properties along with the chemical structures of some representative compounds of pharmaceuticals from different groups.
2.1 Nonsteroidal Anti-inflammatory Drugs (NSAIDs)
NSAIDs are mostly carboxylic acid derivatives attached to planar aromatic functionalities, which act by reversible and irreversible inhibition of enzymes involved in stimulus of pain. They are used as mild analgesics, antipyretics, and anti-inflammatories. Out of the diverse pool of pharmaceuticals, such types of over-the-counter (OTC) drugs are extensively consumed due to their quick relief action in pain and easy availability of non-prescription drugs in the market. Approximately 90% of them belong to the commonly administered therapeutic group of nonsteroidal anti-inflammatory drugs (Crouse et al. 2012). Major types of NSAIDs include phenylpyrazolones (e.g., phenylbutazone), oxicams/enol acids (e.g., meloxicam), propionic acid derivatives (e.g., ibuprofen), fenamates (e.g., diclofenac), anilides (e.g., paracetamol), and salicylic acid derivatives (e.g., acetylsalicylic acid).
2.2 Antibiotics
Some major classes of antibiotics include the quinolones, tetracyclines, and sulfonamides. Antibiotics belonging to the class of quinolones are recommended for acute cases of bacterial prostatitis and in sickle cell disease patients where there is a risk of developing osteomyelitis from Salmonella. Tetracyclines are broad-spectrum antibiotics primarily used for treatment of various infections and also as growth promoter in animal husbandry. The basic structure of tetracyclines consists of a hydro naphthacene backbone containing four (tetra) fused rings, and the analogs vary primarily by substitutions of the fifth, sixth, or seventh position on the backbone rings. Examples include tetracyclines, chlortetracycline, oxytetracycline, doxycycline, etc. Sulfa drugs are N-substituted derivatives of p-aminobenzene sulfonamide (sulfanilamide) that vary in the amide substitution (R-group) to give analogs (e.g., sulfamethoxazole, sulfamerazine, sulfamethazine, sulfachloropyridazine, etc.). They are used against bacterial, protozoal, parasitic, and even fungal infections in human and animal systems and sometimes as herbicides too. Other subclasses of antibiotics include aminoglycosides, lincosamides, macrolides, and glycopeptides, which are complex molecules exhibiting bulky structure and are bactericidal but slow in action.
2.3 Cardiovascular Drugs
Beta-blockers are particularly used to prevent cardiac arrhythmias and myocardial infarction. They are also widely used to treat hypertension in some cases. The chemical structure of beta-blockers comprises of an aromatic ring structure attached to a side alkyl chain possessing a secondary hydroxyl and amine functional group. Some pharmaceuticals belonging to the class of beta-blockers are propranolol, metoprolol, atenolol, etc.
2.4 Anti-ulcer Drugs
These drugs are used to treat and reduce peptic ulcers and irritation of the gastrointestinal tract. These may include antibiotics to cure helicobacter infections, histamine H2 antagonists to reduce gastric acid secretion, and antacids for symptomatic relief. Examples include omeprazole, famotidine, ranitidine hydrochloride, etc.
2.5 Antihistamines
Antihistamines are used to treat allergies, cold, and flu symptoms by blocking the release of histamine from histamine-1 receptors located in the airways, blood vessels, and gastrointestinal tract. They are taken as inexpensive, generic, and OTC drugs for getting relief from nasal congestion and sneezing, caused due to pollen, dust mites, or animal allergy. Examples of antihistamines are cetirizine, fexofenadine, chlorpheniramine, and diphenhydramine.
2.6 Antidepressant
Antidepressant drugs work by acting on the chemical imbalances of neurotransmitters (serotonin, dopamine, and noradrenaline) in the brain, which are responsible for changes in mood and behavior, thereby reducing symptoms of depressive disorders. They include but are not limited to depression, anxiety, agitation, obsessive-compulsive disorders, major depressive disorder, diabetic peripheral neuropathic pain, neuropathic pain, social anxiety disorder, post-traumatic stress disorder, etc. Examples of antidepressants are amitriptyline, amoxapine, clomipramine, desipramine, doxepin, imipramine, nortriptyline, protriptyline, etc.
2.7 Antiepileptics
Antiepileptics also known as anticonvulsant/antiseizure drugs are used in the treatment of epileptic seizures and bipolar disorders and also used as mood stabilizers. Antiepileptic drugs act in the central nervous system by reducing the overall neuronal activity. This can be achieved either by blocking voltage-dependent sodium channels (e.g., carbamazepine) or by enhancement of the inhibitory effects of the gamma-aminobutyric acid neurotransmitter (e.g., benzodiazepines).
2.8 Hormones
There are two groups of hormones (estrogens and progesterone), which are responsible for development of female secondary sexual characteristics. Small quantities are also produced in males. As drugs, female sex hormones are used to treat menstrual and menopausal disorders and are used as oral contraceptives. Estrogens may be used to treat cancer of the breast or prostate, and progestin (synthetic progesterone) is used to treat endometriosis. Examples include 17β-estradiol, 17α-ethynylestradiol, and estrogen.
All of these compounds have their own chemical structure and properties, which decides their behavior in sorption, elimination, degradation, and other associated fate in the environment. The common classes of pharmaceuticals with their generic names, common uses, possible side effects, and mode of action are presented in Table 3.
3 Pharmaceuticals in Indian Scenario
The Indian pharmaceutical industry boasts an aggressive growth in market size from USD 12.6 billion in 2009 to a projected value of USD 55 billion by 2020 (McKinsey and Company, Inc.). For instance, the potential of Indian pharmaceutical industry can be assessed by the fact that 80% of the antiretroviral drugs used to combat AIDS (acquired immune deficiency syndrome) are supplied globally. More than 50% of the global demand for pharmaceuticals used in vaccination, 40% of generic demand in the USA, and 25% of all the drugs used in the UK are also supplied by the Indian pharmaceutical companies (IBEF 2019). The industry’s primary focus has been manufacturing of generic medicines and export of bulk drugs. As per the Department of Pharmaceuticals, Government of India (2018), the growth of the Indian pharmaceutical industry is such that it ranks third by volume on a global basis today, accounting for 10% of global pharmaceutical production (Sharma et al. 2019). With such fast growth and an unprecedented expansion of the pharmaceutical sector, India is bound to be an active hotspot of pharmaceuticals in the environment.
4 Fate of Pharmaceuticals in Aquatic Ecosystem
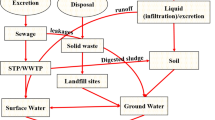
After consumption or direct discharge of expired pharmaceuticals, they are eliminated as active metabolites and parent compounds into waste streams to surface waters to contaminate the environment. Drugs discarded in municipal solid wastes and dumped in landfills could undergo degradation or adsorption or leach into water bodies. A study reported drugs in solid waste at levels of 7.4 to 45 mg/kg (Musson and Townsend 2009). Large quantities of veterinary pharmaceutical compounds (VPCs) are used worldwide in the form of feed additives and growth promoters and for prophylactic purposes. After administration of VPCs, they are not completely metabolized inside animal body. As a result, a portion of them is released to the environment in feces and urine. They also enter the environment from spills generated by anaerobic manure storage lagoons, manure fertilization of farm fields, runoff from farm fields, and discharge from aquaculture operations. As these compounds are quite resistant to existing elimination processes, once disposed of in the environment, they are easily transported to different environmental compartments in a pathway similar to human pharmaceuticals. Therefore, VPCs were reported in surface waters, groundwaters, soil, and air, and they carry their own potential for contaminating these environmental sinks.
The hospitals and drug manufacturing units ought to be the most obvious and impressive discharge units of pharmaceuticals. However, the waste streams from such sources rarely undergo any specialized treatment at the conventional WWTPs. The elimination rate of pharmaceuticals in WWTPs has been reported to vary up to 99% depending on the technology applied and the properties of pharmaceutical compounds. This may result in their tendency to (i) mineralize to low molecular weight compounds (CO2 and H2O) and (ii) simply resist elimination due to low adsorption coefficients and hydrophobicity, resulting in entrapment by suspended solids and sewage sludge, (iii) or these compounds may also convert into the parent compound in the final effluent from conjugated metabolite resulting from microbial enzymatic cleavage in wastewater and sewage sludge. Thus, WWTPs have been termed as hotspots of pharmaceutical contamination in the overall environment. The effluents loaded with pharmaceuticals are discharged into rivers, lakes, and estuaries. Once pharmaceuticals reach surface water bodies, they may undergo natural attenuation processes such as photolysis or sorption by sediments. The pharmaceuticals retained by sewage sludge may also reach the environment when used as fertilizers on agricultural lands. Hence, a potential source of pharmaceuticals in the environment is agricultural runoff, which leads them into nearby water bodies by runoff during rainfall, or even worse, they may seep into groundwater. The concentration levels of pharmaceuticals most commonly detected in the Indian aquatic environment are discussed in the following section.
5 Pharmaceuticals in the Aquatic Environment
5.1 Surface Water
Several studies have reported pharmaceuticals in surface waters around the world. Mutiyar and Mittal (2012) reported traces of NSAIDs and other pharmaceuticals in the Yamuna river. High level of caffeine has been reported in several surface waters from India, including Yamuna river (0.808 μg/L) (Mutiyar and Mittal 2012), Ganga river (0.743 μg/L) (Sharma et al. 2019), and lakes of Nagpur, Maharashtra (46.97 μg/L) (Archana et al. 2016). Ketoprofen was also found at the highest level of 107 ng/L in the Ganga river (Sharma et al. 2019). The Kaveri and Tamiraparani rivers of South India have also been found to be contaminated by carbamazepine at an average concentration of 28.3 ng/L and triclosan at 944 ng/L (Ramaswamy et al. 2011). In other countries, carbamazepine levels have been reported to be up to 48 ng/L in river waters of France (Bouissou-Schurtz et al. 2014), 11.47 ng/L in China (Zhang et al. 2018), and 0.22 ng/L in the USA (Archer et al. 2017). The Musi river, a tributary of the Krishna river, was detected with a host of fluoroquinolone antibiotics (ciprofloxacin, lomefloxacin, ofloxacin, norfloxacin, enrofloxacin, pefloxacin, and difloxacin) with ciprofloxacin, ofloxacin, and norfloxacin reportedly present at the highest concentrations, up to 5015, 542.4, and 251 μg/L, respectively (Gothwal and Shashidhar 2016). The Kaveri, Vellar, and Tamiraparani rivers were also found to contain NSAIDs (naproxen, diclofenac, ibuprofen, ketoprofen, and acetylsalicylic acid) at maximum concentrations of 28, 103, 200, 100, and 660 ng/L, respectively (Shanmugam et al. 2014). Comparatively, the Sindian river in Taiwan was found to contain NSAIDs including naproxen (270 ng/L), diclofenac (56.5 ng/L), ibuprofen (4350 ng/L), and ketoprofen (45 ng/L) (Lin et al. 2010). The Tiber river in Italy was also contaminated by these NSAIDs at higher level of 264, 120, 210, and 150 ng/L (in the same order) (Patrolecco et al. 2013). In Tehran, the river water contents of NSAIDs were reported to be 0.037 μg/L (ibuprofen), 0.041 μg/L (naproxen), 0.025 μg/L (diclofenac), and 0.041 μg/L (indomethacin) (Eslami et al. 2015). Most of the studies have reported the source of pharmaceutical contamination in the surface water to be wastewater discharge either as effluent from STPs or from drug manufacturing units. However, seasonal variation was also observed in the concentration of sulfamethoxazole during monsoon (0.9 μg/L) and post-monsoon (0.16 μg/L) seasons in the Kaveri river (Iyanee et al. 2013). Mutiyar and Mittal (2014b) reported ampicillin (13.74 μg/L), ciprofloxacin (1.4 μg/L), gatifloxacin (0.48 μg/L), sparfloxacin (2.1 μg/L), and cefuroxime (1.7 μg/L) in effluent from STPs discharging into Yamuna river in Delhi. Fick et al. (2009) reported high level of ciprofloxacin up to 6.5 mg/L in lakes receiving WWTPs in Patancheru, Hyderabad. The Cooum river flowing through the Chennai city was reported to be contaminated with triclocarban (6.18 μg/L), ibuprofen (2.32 μg/L), an antiplatelet metabolite carboxylic acid (1.37 μg/L), atenolol (3.18 μg/L), and amphetamine (0.98 μg/L) (Subedi et al. 2015).
5.2 Groundwater/Drinking Water
Sharma et al. (2019) reported caffeine, ibuprofen, carbamazepine, and ketoprofen levels of 262 ng/L, 49.4 ng/L, 27.2 ng/L, and 23.4 ng/L, respectively, in the groundwater of the Ganga river basin. Jindal et al. (2015) reported diclofenac concentrations at 48 ng/mL and pitavastatin at 0.48 ng/mL in the groundwater sample of Mohali, Punjab. The well waters used for drinking purposes in close proximity to a WWTP of drug manufacturing units in Patancheru, Hyderabad, were detected with antibiotics such as cetirizine (28 μg/L), ciprofloxacin (14 μg/L), enoxacin (1.9 μg/L), and terbinafine (0.055 μg/L) (Fick et al. 2009). NSAIDs such as diclofenac and ibuprofen at 120 and 250 ng/L, respectively, have been reported in groundwater at a depth of 0.5 m below the main trench sewer pipe in London (Ellis et al. 2003). Olaitan et al. (2014) reported average concentrations of diclofenac, chloroquine, paracetamol, and ciprofloxacin at 17.0, 5.0, 3.0, and 1.0 μg/L, respectively, in several wells in a pharmaceutical industrial area of Sango Ota, Ogun State of Nigeria. Benotti et al. (2009), in other countries, detected sulfamethoxazole (0.32 ng/L) and carbamazepine (6800 ng/L) in finished water from drinking water treatment plants in the USA, while energy drinks in China were reported with diclofenac at 8310 ng/L (Zhang et al. 2013).
5.3 Sewage Treatment Plants
Some of the most commonly detected pharmaceuticals reported to occur in the wastewater from Indian sewage treatment plants are carbamazepine (a psychoactive), atenolol (antihypertensive), triclocarban and triclosan (antimicrobials), trimethoprim and sulfamethoxazole (antibacterials), ibuprofen and acetaminophen (analgesics), and caffeine (stimulant). Mutiyar and Mittal (2013) reported amoxicillin in the influent and effluent samples of a STP in Delhi at 172.6 ng/L (influent) and 62.5 ng/L (effluent). In another study by Mutiyar and Mittal (2014b), the influent samples of STP in Okhla, New Delhi, were highly contaminated with antibiotics such as ampicillin, ciprofloxacin, gatifloxacin, sparfloxacin, and cefuroxime at the mean concentration levels of 104.2, 20.1, 2.7, 22.5, and 3.4 μg/L, respectively. The levels of these antibiotics (in the same order) were found to occur at 12.68, 8.0, 1.22, 0.14, and 0.22 μg/L in the effluent samples after the treatment (Subedi et al. 2015). The concentration of sulfamethoxazole in wastewater effluent was 0.23 μg/L (Subedi et al. 2015), 0.63 μg/L (Akiba et al. 2016), and 1.02 μg/L (Prabhasankar et al. 2016). Amoxicillin was also detected in a WWTP of Japan at levels of 100–2000 ng/L (Matsuo et al. 2011). The average concentration of sulfamethoxazole in the WWTPs was similar to the concentrations obtained in a WWTP outlet in Spain (Carballa et al. 2004), while it is lower than the average for Europe (1.7 μg/L, Loos et al. 2013) and Canada (1.8 μg/L, Guerra et al. 2014). Forty-three pharmaceutical compounds along with their 13 metabolites including psychoactives, illicit drugs, and artificial sweeteners were reported in 5 STPs of India (Subedi et al. 2015). The NSAIDs constitute a major portion of the pharmaceuticals consumed, and apart from their extensive usage, NSAIDs are frequently encountered in the environment as these acidic molecules are negatively charged at near neutral pH of wastewater, which escape sorption by sewage sludge and remain at dissolved phase in wastewater (Fent et al. 2006). Ibuprofen, ketoprofen, and diclofenac have been detected at 26.45, 16.21, and 25.68 μg/L levels, respectively, in the wastewater drains of India (Singh et al. 2014). Comparatively, NSAIDs in WWTP effluents of Tehran have been detected at levels of 0.045, 0.054, 0.033, and 0.057 μg/L for ibuprofen, naproxen, diclofenac, and indomethacin, respectively (Eslami et al. 2015).
5.4 Pharmaceutical from Production Facilities and Hospital Wastewater
Wastewater discharges from pharmaceutical production facilities and hospitals are the major potent source of environmental contamination by pharmaceuticals. The levels of ciprofloxacin, cetirizine, metoprolol, enrofloxacin, citalopram, norfloxacin, lomefloxacin, enrofloxacin, and ofloxacin in effluent of bulk drug manufacturers near Hyderabad were up to 31000, 1400, 950, 900, 840, 420, 300, 300, and 160 μg/L, respectively (Larsson et al. 2007). The level of ciprofloxacin in similar wastewater of other countries has been 0.6 μg/L in Canada (Guerra et al. 2014), 1.4 μg/L in Portugal (Santos et al. 2013), 3.7 μg/L in Italy (Verlicchi et al. 2012), and 6.9 μg/L in Australia (Pal et al. 2010). In wastewater from hospital in Ujjain, Madhya Pradesh, were found concentrations of ofloxacin, levofloxacin, ceftriaxone, ciprofloxacin, tinidazole, sulfamethoxazole, metronidazole, and norfloxacin at 73, 81, 60, 237, 88, 81, 3.8, and 23 μg/L, respectively (Diwan et al. 2010). In southern India, two sewage treatment plants (STPs) receiving hospital effluent were also reported to have chloramphenicol (Akiba et al. 2016). They also reported concentrations of trimethoprim (103–285 ng/L), ofloxacin (1715–2469 ng/L), and sulfamethoxazole (207–637 ng/L) in the wastewater from one STP, and from another STP, concentrations were 43–46 ng/L, 500–537 ng/L, and 40–50 ng/L, respectively. Higher concentrations of sulfamethoxazole (307–8714 ng/L) and ofloxacin (3135–24,811 ng/L) have been reported to occur in the hospital effluents of Coimbra, Portugal (Santos et al. 2013). Prabhasankar et al. (2016) reported presence of sulfamethoxazole, trimethoprim, erythromycin, chloramphenicol, naproxen, bezafibrate, and ampicillin in the samples of STP receiving hospital wastewater in Karnataka. Comparatively, higher concentrations of pharmaceuticals from hospital wastewaters in Portugal were reported as 8714 ng/L for sulfamethoxazole, 3963 ng/L for trimethoprim, 7545 ng/L for erythromycin, 6042 ng/L for naproxen, and 1359 ng/L for bezafibrate (Santos et al. 2013).
6 Toxicity of Pharmaceuticals
6.1 Toxicity of Anti-cancer (Antineoplastic) Compounds
Individual and combinations of anti-cancer compounds at varying concentrations are reported to have organism-specific toxicity (Toolaram et al. 2014). For example, EC50 of cisplatin and 5-fluorouracil for algae Pseudokirchneriella subcapitata is 1.52 mg/L and 0.13 mg/L, respectively, and 0.67 mg/L and 1.20 mg/L, respectively, for cyanobacteria Synechococcus leopoliensis (Brezovsek et al. 2014). However, EC50 for 5-fluorouracil and cytarabine were reported for P. putida is 0.044 mg/L and 17 mg/L, respectively, and 0.1 mg/L and 10 mg/L for D. magna, respectively (Zounkova et al. 2010).
6.2 Toxicity of Beta-Blocker Compounds
Beta-blockers act by inhibiting beta-adrenergic receptors, which are a class of receptors critical for normal functioning in the sympathetic branch of the autonomic nervous system in vertebrates. Fishes like other vertebrates possess β-receptors in the heart, liver, and reproductive system, and prolonged exposure to drugs belonging to this therapeutic class may cause deleterious effects in vertebrates. Drugs belonging to this class such as propranolol reduced growth rate of Japanese medaka fish in 2 weeks at 500 μg/L, while exposure to concentration of 0.5–1 μg/L resulted in a decrease of egg production (Huggett et al. 2002). Serotonin is an important neurotransmitter in hormonal and neuronal mechanisms, which is responsible for different regulatory and endocrine functions in vertebrates and invertebrates. Alterations in its levels may cause changes in appetite, immune system, reproduction, and other behavioral functions. In therapeutics, the selective serotonin reuptake inhibitors such as fluoxetine, fluvoxamine, paroxetine, and sertraline are the most widely used synthetic antidepressants (Santos et al. 2010).
6.3 Toxicity of NSAIDs (Nonsteroidal Anti-inflammatory Drugs)
NSAIDs act mainly by suppressing the cyclooxygenase (COX) enzyme responsible for synthesis of prostaglandins. Chronic toxicity test on the rainbow trout showed cytological changes in the liver, kidneys, and gills after 28 days of exposure to diclofenac at concentration of 1 μg/L (Triebskorn et al. 2004). They also reported concentration of 5 μg/L of diclofenac resulted in renal lesions and bioaccumulation in the liver, kidneys, gills, and muscles. Among all the NSAIDs, diclofenac is the most studied analgesic compound often detected at trace level in the environmental samples and possesses the highest acute toxicity on aquatic organisms. It was suggested that diclofenac is the most toxic analgesics with commonly reported lowest observed effect concentration (LOEC) of below 100 mg/L (Fent et al. 2006). Diclofenac has also been proven to be acutely toxic to vultures, decimating populations in the Indian subcontinent due to its ubiquitous use in cattle. This drug gained notorious popularity, and the manufacture of diclofenac for veterinary formulations was banned in 2006 after it was known to cause renal lesions in vultures (Gyps bengalensis, Gyps indicus, and Gyps tenuirostris) which scavenged on treated livestock bodies. Phytoplankton was found to be highly sensitive to diclofenac in acute, high-level exposure with an EC50 value of 14.5 mg/L in 96 h (Ferrari et al. 2004).
6.4 Toxicity of Hormones
Hormones, specifically estrogen compounds are some of the earliest pharmaceutical compounds reported to be present in the environment. Their presence has been linked with abnormal reproductive conditions in aquatic organisms, especially fishes. Ethynylestradiol (EE2) is a synthetic estrogen found in oral contraceptive pills with marked estrogenic effects in fish. Very low concentrations <1 ng/L were enough to give rise to an increased female population, and for EE2 concentrations above 3.5 ng/L, fish became completely feminized. The chronic exposure of fathead minnow to concentrations of EE2 at 5–6 ng/L led to feminization of male fish, through production of vitellogenin and disruption in gonadal development, causing intersex, and altered oogenesis in female fishes (Kidd et al. 2007). Such reproductive alterations led to the collapse of the fathead minnow population due to the loss of the young generations, which almost brought this species from the lake near to extinction.
6.5 Toxicity of Antibiotics
Bialk-Bielinska et al. (2011) carried out a systematic analysis of the ecotoxicological potential of many sulfonamide antibiotics on aquatic microorganisms including bacteria and algae. They estimated EC50 values of 0.02 mg/L for sulfadimethoxine in the inhibition of duckweed growth to >250 mg/L for 12 sulfonamides in enzyme inhibition assays. Additionally, the presence of elements in environment can potentially increase the toxicity of antibiotic contaminants (Zhang et al. 2012). Antibiotics such as tetracyclines and quinolones in association with copper, zinc, and cadmium, may result in more toxicity. The major concern with regard to the presence of antibiotics in the environment is the prevalence of antibiotic residues, which can result in the development of antibiotic-resistant strains of both environmental and pathogenic bacteria (Martinez 2009; Hong et al. 2013). A positive correlation has been found between antibiotic-resistant microorganisms and concentrations of aquatic antibiotic (Novo et al. 2013). This unwilling or unintentional resistance among commensal organisms is due to mutation in common genes and transfer of antibiotic-resistant genes (ARGs). Some ARGs has been detected in the clinical and non-clinical samples including drinking water (Jiang et al. 2011). With reference to antibiotic resistance, antimicrobial resistance (AMR) is another synonym which can be summed up to be antibiotic, antiviral, antiprotozoal, and antifungal resistance altogether.
Based on the economist from the UK, the impact of AMR is such that currently 700,000 deaths occur globally, and it has been estimated that by 2050, 10 million deaths/year are projected to occur (O’Neill 2016). In India, antibiotic-resistant neonatal infections cause the deaths of nearly 60,000 newborns each year (Laxminarayan et al. 2013). As per the scoping report on antimicrobial resistance in India, more than 70% isolates of Gram-negative bacteria Escherichia coli, Klebsiella pneumoniae, and Acinetobacter baumannii and nearly half of all Pseudomonas aeruginosa were resistant to antibiotics of fluoroquinolones set and third-generation cephalosporins. Among the Gram-positive organisms, 42.6% of Staphylococcus aureus were methicillin-resistant, and 10.5% of Enterococcus faecium were vancomycin-resistant. AMR challenges in India include the uncontrolled use of antibiotics in human as well as veterinary sectors; increased use of antibiotics as growth promoters in animals; inadequate implementation of regulations; limited or no regulations for food and non-food animals, respectively; and, importantly, inadequate interaction among clinicians and lab experts.
The World Health Organization (WHO) (WHO 2017) experts agreed on grouping the pathogens according to the species and the type of resistance and then stratifying the results in three priority tiers, critical, high, and medium, depicted below.
Priority 1: Critical |
Acinetobacter baumannii, carbapenem-resistant Pseudomonas aeruginosa, carbapenem-resistant Enterobacteriaceae, carbapenem-resistant, cephalosporin-resistant |
Priority 2: High |
Enterococcus faecium, vancomycin-resistant Staphylococcus aureus, methicillin-resistant, vancomycin-resistant Helicobacter pylori, clarithromycin-resistant Campylobacter, fluoroquinolone-resistant Salmonella spp., fluoroquinolone-resistant Neisseria gonorrhoeae, cephalosporin-resistant, fluoroquinolone-resistant |
Priority 3: Medium |
Streptococcus pneumoniae, penicillin-non-susceptible Haemophilus influenzae, ampicillin-resistant Shigella spp., fluoroquinolone-resistant |
7 Environmental Risk Assessment (ERA)
The European Commission (Directive 92/18/EEC) specified that the medicinal product for human use must be accompanied by an environmental risk assessment. For this purpose, the European Medicines Agency (EMA) introduced “Note for Guidance” which included the guidelines for assessing the environmental risks of veterinary medicines only to be extended later to pharmaceuticals for human use by Directive 2001/83/EC (Santos et al. 2010). The guidelines recommend a stepwise procedure using acute toxicity tests on model organisms belonging to different phyla such as algae, zooplanktons, fish, and other invertebrates.
An ERA consists of two phases: Phase I, which is a screening phase, and Phase II, a testing phase, which may be conducted based on the results of Phase I. Firstly, Phase I includes calculation of the predicted environmental concentration (PEC) of the compound in surface water (PECsurface water), an assessment of the mode of action, and results from toxicological tests. A predicted environmental concentration calculation of the compound is restricted to the aquatic compartment (PECsurface water). In case the PECsurface water is less than 0.01 μg/L and no other environmental factors are taken into account, it is assumed that the pharmaceutical is unlikely to pose a risk to the environment. However, if the PECsurface water is above 0.01 μg/L, a Phase II assessment is required to be performed. In Phase II, it is required to make all information about the physical, chemical, or toxicological properties of the compound available to the investigator. A tiered approach involving two steps – Step A and Step B – is involved in Phase II. In Step A, an evaluation of the possible fate and effects of the compound is done. If no risk is found during this step, there is no requirement of Step B. If a risk is detected, then the fate and effects of the active substance in the relevant compartment are tested by determination of certain toxicological end points on test organisms using standardized test protocols. Using the results generated from the effect studies performed in Step A, the predicted no-effect concentrations (PNECs) are derived for environmental compartments such as surface water, groundwater, and sewage treatment plants and compared with calculated PEC values. The predicted no-effect concentration was determined by dividing the EC50 by an uncertainty factor which is typically set equal to 1000 (Sanderson et al. 2004). If one or more of the PEC/PNEC ratios or hazard quotient (HQ) exceeds the predefined trigger values (1 for surface water and groundwater compartments and 0.1 for the STP), a Step B assessment should be conducted. Environmental fate studies in Step B may include a bioconcentration study in fish and/or degradation in soil, while effect studies may include testing with terrestrial organisms such as soil microflora, earthworms, springtails, and plants.
In a case study, Sharma et al. (2019) estimated the worst-case scenario of potential health risk of some pharmaceuticals in drinking water (groundwater) along the Ganga river in India. An age-dependent risk quotient (RQ) for each detected compound was calculated by dividing the maximum measured concentration in the groundwater (MCGW) by the corresponding age-dependent drinking water equivalent level (DWEL).
The DWEL values were taken from literature and estimated for seven age categories using different parameters such as the acceptable daily intake or risk-specific dose (RSD) for non-carcinogenic and carcinogenic effects, respectively, age-specific body weights (BW) in kg, daily drinking water intake, etc. The DWELs for all age groups ranged from 4.8 μg/L (for carbamazepine, 1–2 year’s age group) to 12.8 mg/L (for acetaminophen, 16–21 year’s age group). The RQ >1 indicated the possibility of human health risk, while its value between 0.2 and 1 called for more detailed assessment, whereas RQ ≤0.2 was considered of no appreciable concern to human health. For all detected pharmaceuticals, RQs ranged from 1.5 × 10−7 (for acetaminophen, 16–21 year’s age group) to 0.0021 (for carbamazepine, 16–21 year’s age group). Among different age groups, children (1–11 years) had higher RQs than adolescents (11–21 years) and adults (>21 years).
In the same study, the ecological risk assessment was also performed by calculating RQ (some studies use the term hazard quotient (HQ)) for the detected pharmaceuticals where the RQ was calculated by dividing the maximum river water concentration (MCRW) for each compound by the PNEC for three classes of aquatic organisms, i.e., algae, Daphnia magna (a crustacean), and fish. The PNEC values were estimated by dividing the EC50 (effective concentration, reducing a biological process by 50%) or LC50 (lethal concentration, killing 50% of the organisms) obtained from the literature or by using the US EPA Ecological Structure Activity Relationship (ECOSAR v1.10) model by an assessment factor of 1000. Results of ecological risk assessment showed that the risks were comparatively higher for algae. For example, the RQ of caffeine was as high as 49.5, which was observed for three different aquatic organisms. Similarly, the RQs of triclocarban and triclosan ranged from 0.03 to 0.3 and 0.01 to 3.9, respectively. The RQs for freshwater invertebrates (except for Daphnia from triclocarban) and fish were generally lower than 0.1, implying negligible risk of acute/chronic toxicity to these aquatic organisms. An account of the risk quotients for different pharmaceuticals in water matrices has been given in Table 4.
8 Treatment Process for Pharmaceuticals
8.1 Microbial Degradation
In case of long and highly branched pharmaceuticals, the biodegradation is least effective in comparison to molecules with short and unbranched chemical structure (e.g., paracetamol, salicylic acid, diclofenac, and carbamazepine). Saturated aliphatic and aromatic compounds containing sulfur and halogen substituents showed resistance to microbial degradation. Apart from bacteria, white-rot fungus has been reported to be effective in the degradation of pharmaceuticals. In one study, two white-rot fungi Trametes versicolor and Ganoderma lucidum were used in the removal of a mixture of 13 pharmaceuticals while generating biodiesel from the sludge (Vasiliadou et al. 2016). The removal rates of clofibric acid, atenolol, caffeine, carbamazepine, hydrochlorothiazide, sulfamethoxazole, and sulpiride degradation were below 40%, while diclofenac, gemfibrozil, ibuprofen, progesterone, and ranitidine showed complete removal.
8.2 Phytoremediation
Phytoremediation technique utilizes plants and associated microorganisms in the rhizospheres to transform, remediate, or accumulate toxic environmental contaminants present in ground and surface waters, sediments, and soil. The natural wetlands act as transitional zones between the land and water system and, in the course, improve the water quality in terms of biological oxygen demand, total suspended solids, metal ions, phosphates, and other organic contaminants such as pesticides and pharmaceuticals. The mechanisms of the plant-based aquatic systems include sorption, sedimentation, volatilization, photodegradation, and microbial degradation. Depending on the mode of loading, depth of bed, soil matrix, presence of vegetation, types and number of plant species, organic and hydraulic loading rates, etc., the pharmaceutical degradation rate varies in a wetland system. In a review study done by Li et al. (2014), 115 pharmaceuticals were studied under 4 types of constructed wetland systems such as the free water surface constructed wetland, vertical subsurface flow constructed wetlands (VSSF CWs), horizontal subsurface flow constructed wetlands, and hybrid constructed wetlands. The VSSF CWs were most efficient in elimination of diclofenac, ibuprofen, naproxen, and salicylic acid, possibly due to higher oxygenations, shorter hydraulic retention time, and low sensitivity toward overloading conditions.
8.3 Membrane Process
Membrane-based removal techniques involve microfiltration (MF), ultrafiltration (UF), nanofiltration (NF), and reverse osmosis (RO) processes, where MF and UF are based on sieving mechanism, while RO and NF are pressure-driven membrane processes. The MF and UF are not considered as suitable pharmaceutical removal process (with the exception of hydrophobic compounds), because of their large pore size. In the case of RO, the pressure difference between filtrate and feed sites of the separation membrane is the driving force during reverse osmosis. High rejection efficiency (>85%) has been reported for diclofenac, ketoprofen, and carbamazepine using NF/RO technologies in a drinking water treatment plant (Radjenović et al. 2007). The main challenges posed by membrane-driven removal processes are clogging of membrane pores by larger molecules and suspended materials, disposal of brine, susceptibility of the membranes toward oxidizing agents, and easy fouling of the membranes. Some of these shortcomings may be improvised with advanced oxidation processes.
8.4 Advanced Oxidation Process
Oxidation reactions involve generation of free radicals, mainly hydroxyl radical, which facilitate conversion of the pharmaceuticals into more biodegradable compounds (Deegan et al. 2011) or simple mineralization into smaller molecules by use of oxidants such as ozone or hydrogen peroxide, catalysts (Fe and TiO2), and energy source such as ultraviolet-visible radiation, electric current, and ultrasound irradiation. The high reactivity of these free radicals promotes oxidation of organic and inorganic pollutants with high reaction rate constants. Ozonation has been very successful in removal of pharmaceuticals with removal efficiency >90% for some antibiotics (Ternes et al. 2003; Dantes et al. 2008) but <50% for some beta-blockers (Ternes et al. 2003). The electrophilic ozone reacts with electron-rich molecules and hence can directly attack compounds having carbon-carbon double or triple bonds and aromatic groups or at certain oxygen-, nitrogen-, phosphorus-, or sulfur-containing functional group. Fenton reactions involving H2O2 in presence of Fe and UV light showed that diclofenac could be completely mineralized by photo-Fenton reactions within 50 min (Ravina et al. 2002). TiO2 is a promising alternative due to its inert nature, cost-effectiveness, and photostability. The semiconductor oxide such as TiO2 is excited by photoexcitation of a valence-shell electron generating an electron-hole pair. These holes have high oxidation potential and can generate hydroxyl radicals from water at the particle surface. TiO2-based photo-oxidations under both simulated light and sunlight conditions led to complete removal of oxytetracycline with 90% mineralization (Zhao et al. 2013).
8.5 Adsorption
Adsorption is the process through which a substance/adsorbate, originally present in one phase is removed from that phase by accumulation at the interface between that phase and a separate solid/adsorbent phase, usually activated carbons. The accumulation may result from physical interactions (e.g., van der Waals forces) or chemical reaction (e.g., sharing of electrons). Ruiz et al. (2010) obtained >90% removal for paracetamol by a commercial activated carbon. The US EPA identifies granular activated carbon as the “best available technology” for treating various organic pollutants (Westerhoff et al. 2005).
8.6 Ionizing Radiation
Wang et al. (2019) reported progress of pharmaceutical degradation by ionizing radiation. Ionizing irradiation of antibiotics is effective for their degradation, resulting in complete removal. They reported that during the process of radiation, with increasing absorbed dose and decreasing initial concentration of pharmaceuticals, the degradation efficiency of pharmaceuticals increases. To improve their removal efficiency, several advanced oxidation processes (AOPs) such as H2O2, Fe2+, and Fe2+/H2O2, as well as biological treatment processes, are combined with ionizing radiation.
9 Recommendations
One of the most effective ways to reduce the load of pharmaceuticals into the environment is by reducing their consumption. Complementary strategies such as improved sanitation, nutrition, and access to general health care are recommended in order to avoid the use of medicines. Prudent use of veterinary drugs in the agriculture sector is one of the wisest approaches in combating pollution by pharmaceuticals. This consists essentially of implementing various management practices to minimize the use of antibiotics, which are consumed by humans. This reduces the occurrence of cross-resistance toward antibiotics in humans and animals. Product take-back programs by pharmaceutical producers have been particularly active in setting up programs, which allow consumers to return their residual medications to pharmacies at no cost. It is a very effective measure to reduce the disposal of unused pharmaceuticals to municipal sewage systems and private septic tanks. The proposed program includes voluntary or compulsory team for collecting the unused/expired pharmaceuticals to a collection point such as a pharmacy or municipal authority for disposal. However, there is a need for much involvement through research in order to assess the cost-effectiveness of these programs (e.g., types and amounts of medicine being collected, the participation rates, regulatory compliance issues, program costs, funding sources, and final disposal). However, the take-back programs do not come with complete reliance as such programs may increase the risk of accidental poisonings and drug abuse due to the stock piling of unused medications awaiting take-back. In general, the public who are the ultimate users should be aware of the consequences of improper disposal and overuse of pharmaceuticals in their day-to-day life. For this, awareness campaigns and workshops should be conducted for the public. Some of the awareness facts include completing the dosage or the full prescription even if the infection seems to have lessened down. Pharmaceutical companies and other providers should behave in a proactive manner and examine the pathway along with the potential impact of discharging wastewater containing such active pharmaceutical ingredients to the wastewater stream and finally into the downstream waterways.
There is an active research need for tracing the presence of pharmaceutical contaminants in the environment, which includes water, sediments, and biota. A robust detection method is required for determining the presence of pharmaceuticals and their metabolites in the environmental samples. Water monitoring network studies for early detection are essential. More information is needed about the possible negative effects that may occur after long-term environmental exposure to several pharmaceuticals both separately and simultaneously.
References
Akiba M, Sekizuka T, Yamashita A et al (2016) Distribution and relationships of antimicrobial resistance determinants among extended-spectrum-cephalosporin-resistant or carbapenem-resistant escherichia coli isolates from rivers and sewage treatment plants in India. Antimicrob Agents Chemother 60:2972–2980
Archana G, Dhodapkar R, Kumar A (2016) Offline solid-phase extraction for preconcentration of pharmaceuticals and personal care products in environmental water and their simultaneous determination using the reversed phase high-performance liquid chromatography method. Environ Monit Assess 188:1–10
Archer E, Petrie B, Kasprzyk-Hordern B, Wolfaardt GM (2017) The fate of pharmaceuticals and personal care products (PPCPs), endocrine disrupting contaminants (EDCs), metabolites and illicit drugs in a WWTW and environmental waters. Chemosphere 174:437–446
Benotti MJ, Trenholm RA, Vanderford BJ, Holady JC, Stanford BD, Snyder SA (2009) Pharmaceuticals and endocrine disrupting compounds in U.S. drinking water. Environ Sci Technol 43:597–603
Bialk-Bielinska A, Stolte S, Arning J, Uebers U, Boschen A, Stepnowski P, Matzke M (2011) Ecotoxicity evaluation of selected sulfonamides. Chemosphere 85(6):928–933
Blair BD, Crago JP, Hedman CJ, Klaper RD (2013) Pharmaceuticals and personal care products found in the Great Lakes above concentrations of environmental concern. Chemosphere 93:2116–2123
Bottoni P, Caroli S, Caracciolo AB (2010) Pharmaceuticals as priority water contaminants. Toxicol Environ Chem 92(3):549–565
Bouissou-Schurtz C, Houeto P, Guerbet M et al (2014) Ecological risk assessment of the presence of pharmaceutical residues in a French national water survey. Regul Toxicol Pharmacol 69:296–303
Brezovsek P, Elersek T, Filipic M (2014) Toxicities of four anti-neoplastic drugs and their binary mixtures tested on the green alga Pseudokirchneriella subcapitata and the cyanobacterium Synechococcus leopoliensis. Water Res 52:168–177
Carballa M, Omil F, Lema J, Llompart M, Garcia-Jares C, Rodrıguez I, Gomez M, Ternes T (2004) Behavior of pharmaceuticals, cosmetics and hormones in a sewage treatment plant. Water Res 38:2918–2926
Crouse BA, Ghoshdastidar AJ, Tong AZ (2012) The presence of acidic and neutral drugs in treated sewage effluents and receiving waters in the Cornwallis and Annapolis River watersheds and the Mill Cove Sewage treatment plant in Nova Scotia, Canada. Environ Res 112:92–99
Dantes R, Contreras S, Sans C, Esplugas S (2008) Sulfamethoxazole abatement by means of ozonation. J Hazard Mater 150:790–794
Daughton CG, Ternes TA (1999) Pharmaceuticals and personal care products in the environment: agents of subtle change? Environ Health Perspect 107(suppl. 6):907–938
Deegan AM, Shaik B, Nolan K, Urell K, Oelgemöller M, Tobin J, Morrissey A (2011) Treatment options for wastewater effluents from pharmaceutical companies. Int J Environ Sci Technol 8:649–666
Diwan V, Tamhankar AJ, Khandal RK et al (2010) Antibiotics and antibiotic-resistant bacteria in waters associated with a hospital in Ujjain, India. BMC Public Health 10:1–8
Ellis JB, Revitt DM, Lister P, Willgress C, Buckley A (2003) Experimental studies of sewer exfiltration. Water Sci Technol 47:61–67
EMA (European Medicines Agency) (2019) Categorisation of antibiotics. Accessed 08 Apr 2021 at https://www.ema.europa.eu › documents › report
Eslami A, Amini MM, Yazdanbakhsh AR et al (2015) Occurrence of non-steroidal anti-inflammatory drugs in Tehran source water, municipal and hospital wastewaters, and their ecotoxicological risk assessment. Environ Monit Assess 187:734
Fent K, Weston AA, Caminada D (2006) Review Ecotoxicology of human pharmaceuticals. Aquat Toxicol 76:122–159
Ferrari B, Mons R, Vollat B, Fraysse B, Paxeaus N, Giudice RL (2004) Environmental risk assessment of six human pharmaceuticals: are the current environmental risk assessment procedures sufficient for the protection of the aquatic environment? Environ Toxicol Chem 23(5):1344–1354
Fick J, Söderström H, Lindberg RH, Phan C, Tysklind M, Larsson DG (2009) Contamination of surface, ground, and drinking water from pharmaceutical production. Environ Toxicol Chem 28:2522–2527
Gothwal R, Shashidhar T (2016) Occurrence of high levels of fluoroquinolones in aquatic environment due to effluent discharges from bulk drug manufacturers. J Hazard Toxic Radioact Waste 21(3):05016003
Guerra P, Kim M, Shah A, Alaee M, Smyth SA (2014) Occurrence and fate of antibiotic, analgesic/anti-inflammatory, and antifungal compounds in five wastewater treatment processes. Sci Total Environ 473–474:235–243
Hong P, Al-Jassim N, Ansari MI, Mackie RI (2013) Environmental and public health implications of water reuse: antibiotics, antibiotic resistant bacteria, and antibiotic resistance genes. Antibiotics 2(3):367–399
Huggett DB, Brooks BW, Peterson B, Foran CM, Schlenk D (2002) Toxicity of select beta adrenergic receptor-blocking pharmaceuticals (B-blockers) on aquatic organisms. Arch Environ Cotam Toxicol 43:229–235
IWW (2014) Resulst of a Global Database of Measured Environmental Concentrations (MEC), Geneva conference on Pharmaceuticals in the Environment, 8th–9th April 2014
Iyanee FS, Shimamura K, Prabhasankar VP et al (2013) Occurrence of antibiotics in river water – a case study of the Vrishabhavathi river near Bangalore, India. Symposium on Halogenated Persistent Organic Pollutants, DIOXIN 2013, Daegu, Korea
Jiang L, Hu X, Yin D, Zhang H, Yu Z (2011) Occurrence, distribution and seasonal variation of antibiotics in the Haungpu River, Shanghai, China. Chemosphere 82:822–828
Jindal K, Narayanam M, Singh S (2015) A systematic strategy for the identification and determination of pharmaceuticals in environment using advanced LC–MS tools: Application to ground water samples. J Pharm Biomed Anal 108:86–96
Kidd KA, Blanchfield PJ, Mills KH et al (2007) Collapse of a fish population after exposure to a synthetic estrogen. Proc Natl Acad Sci USA 104:8897–8901
Kolpin DW, Furlong ET, Meyer MT et al (2002) Pharmaceuticals, hormones, and other organic wastewater contaminants in US streams, 1999-2000: a national reconnaissance. Environ Sci Technol 36:1202–1211
Larsson DG, de Pedro C, Paxeus N (2007) Effluent from drug manufactures contains extremely high levels of pharmaceuticals. J Hazard Mater 148:751–755
Laxminarayan R, Duse A, Wattal C et al (2013) Antibiotic resistance-the need for global solutions. Lancet Infect Dis 13:1057–1098
Li Y, Zhu G, Ng WJ, Tan SK (2014) A review on removing pharmaceutical contaminants from wastewater by constructed wetlands: design, performance and mechanism. Sci Total Environ 468–469:908–932
Lin AYC, Panchangam SC, Chen HY (2010) Implications of human pharmaceutical occurrence in the Sindian river of Taiwan: a strategic study of risk assessment. J Environ Monit 12:261–270
Loos R, Carvalho R, António DC et al (2013) EU-wide monitoring survey on emerging polar organic contaminants in wastewater treatment plant effluents. Water Res 47:6475–6487
Martinez JL (2009) Environmental pollution by antibiotics and by antibiotic resistance determinants. Environ Pollut 157(11):2893–2902
Matsuo H, Sakamoto H, Arizono K, Shinohara R (2011) Behavior of pharmaceuticals in waste water treatment plant in Japan. Bull Environ Contam Toxicol 87:31–35
MSD Manual. Accessed 08 Apr 2021 at https://www.msdmanuals.com/en-in/home/infections/antibiotics/overview-of-antibiotics
Musson SE, Townsend TG (2009) Pharmaceutical compound content of municipal solid waste. J Hazard Mater 162:730–735
Mutiyar PK, Mittal AK (2012) Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) in river Yamuna, Delhi: emerging class of urban environmental pollutants. In: Proceeding of: Urban Environmental Pollution (UEP -2012) Conference, At Amsterdam, Netherlands
Mutiyar PK, Mittal AK (2013) Occurrences and fate of an antibiotic amoxicillin in extended aeration-based sewage treatment plant in Delhi, India: a case study of emerging pollutant. Desalination Water Treat 51:6158–6164
Mutiyar PK, Mittal AK (2014a) Risk assessment of antibiotic residues in different water matrices in India: key issues and challenges. Environ Sci Pollut Res Int 21:7723–7736
Mutiyar PK, Mittal AK (2014b) Occurrences and fate of selected human antibiotics in influents an effluents of sewage treatment plant and effluent-receiving river Yamuna in Delhi (India). Environ Monit Assess 186(1):541–557
Novo A, Andre S, Viana P, Nunes OC, Manaia CM (2013) Antibiotic resistance, antimicrobial residues and bacterial community composition in urban wastewater. Water Res 47(5):1875–1887
O’Neill J (2016) Tackling drug-resistant infections globally: final report and recommendations. Review on Antimicrobial Resistance. Accessed 20 Nov 2020 at: https://amrreview.org/sites/default/files/160518_Final%20paper_with%20cover.pdf
O’Rourke A, Beyhan S, Choi Y et al (2020) Mechanism-of-action classification of antibiotics by global transcriptome profiling. Antimicrob Agents Chemother 64:e01207–e01219
Olaitan J, Chimezie A, Bamiro T, Temitope A (2014) Determination of pharmaceutical compounds in surface and underground water by solid phase extraction-liquid chromatography. J Environ Chem Ecotoxicol 6:20–26
Pal A, Gin K, Lin A, Reinhard M (2010) Impacts of emerging organic contaminants on freshwater resources: review of recent occurrences, sources, fate and effects. Sci Total Environ 408:6062–6609
Patrolecco L, Ademollo N, Grenni P, Tolomei A, Barra A, Capri S (2013) Simultaneous determination of human pharmaceuticals in water samples by solid phase extraction and HPLC with UV-fluorescence detection. Microchem J 107:165–171
Prabhasankar VP, Dl J, Balakrishna K et al (2016) Removal rates of antibiotics in four sewage treatment plants in South India. Environ Sci Pollut Res Int 23:8679–8685
Radjenović J, Petrovic M, Barcelo D (2007) Analysis of pharmaceuticals in wastewater and removal using a membrane bioreactor. Anal Bioanal Chem 387:1365–1377
Ramaswamy BR, Shanmugam G, Velu G, Rengarajan B, Larsson DG (2011) GC–MS analysis and ecotoxicological risk assessment of triclosan, carbamazepine and parabens in Indian rivers. J Hazard Mater 186:1586–1593
Ravina M, Campanella L, Kiwi J (2002) Accelerated mineralisation of the drug diclofenac via Fenton reactions in a concentric photo-reactor. Water Res 36:3553–3560
Report on Indian Pharmaceuticals Industry Analysis August (2019). https://www.ibef.org/download/Pharmaceuticals-August-2019.pdf. Accessed 15 Nov 2019
Ruiz B, Cabrita I, Mestre AS, Parra JB, Pires J, Carvalho AP, Ania CO (2010) Surface heterogeneity effects of activated carbons on the kinetics of the paracetamol removal from aqueous solution. Appl Surf Sci 256:5171–5175
Sanderson H, Brain RA, Johnson DJ, Wilson CJ, Solomon KR (2004) Toxicity classification and evaluation of four pharmaceuticals classes: antibiotics, antineoplastics, cardiovascular, and sex hormones. Toxicology 203:27–40
Santos LHMLM, Araújo AN, FachiniA PA, Delerue-Mastos C, Montenegro MCBSM (2010) Ecotoxicological aspects related to the presence of pharmaceuticals in the aquatic environment. J Hazard Mater 175:45–95
Santos LH, Gros M, Rodriguez-Mozaz S et al (2013) Contribution of hospital effluents to the load of pharmaceuticals in urban wastewaters: identification of ecologically relevant pharmaceuticals. Sci Total Environ 461–462:302–316
Shanmugam G, Sampath S, Selvaraj K, Larsson DG, Ramaswamy BR (2014) Non-steroidal anti-inflammatory drugs in Indian rivers. Environ Sci Pollut Res Int 21:921–931
Sharma BM, Bečanová J, Scheringer M et al (2019) Health and ecological risk assessment of emerging contaminants (pharmaceuticals, personal care products, and artificial sweeteners) in surface and groundwater (drinking water) in the Ganges River Basin, India. Sci Total Environ 646:1459–1467
Singh KP, Rai P, Singh AK, Verma P, Gupta S (2014) Occurrence of pharmaceuticals in urban wastewater of north Indian cities and risk assessment. Environ Monit Assess 186:6663–6682
Subedi B, Balakrishna K, Sinha RK, Yamashita N, Balasubramanian VG, Kannan K (2015) Mass loading and removal of pharmaceuticals and personal care products, including psychoactive and illicit drugs and artificial sweeteners, in five sewage treatment plants in India. J Environ Chem Eng Part A 3(4):2882–2891
Ternes TA, Stüber J, Herrmann N, McDowell D, Ried A, Kampmann M, Teise B (2003) Ozonation: a tool for removal of pharmaceuticals, contrast media and musk fragrances from wastewater. Water Res 37:1976–1982
Toolaram AP, Kummerer K, Schneider M (2014) Environmental risk assessment of anti-cancer drugs and their transformation products: a focus on their genotoxicity characterization-state of knowledge and shortcomings. Mutat Res Rev Mutat Res 760:18–35
Triebskorn R, Casper H, Heyd A, Eikemper R, Kohler HR, Schwaiger J (2004) Toxic effects of the non-steroidal anti-inflammatory drug diclofenac. Part II. Cytological effects in liver, kidney, gills and intestine of rainbow trout (Oncorhynchus mykiss). Aquat Toxicol 68:151–166
US EPA (2012) Inaction in Identifying Hazardous Waste Pharmaceuticals May Result in Unsafe Disposal. Report No 12-P-0508. May 25, 2012
Vasiliadou IA, Sánchez-Vázquez R, Molina R et al (2016) Biological removal of pharmaceutical compounds using white-rot fungi with concomitant FAME production of the residual biomass. J Environ Manag 180:228–237
Verlicchi P, Al Aukidy M, Galletti A, Petrovic M, Barceló D (2012) Hospital effluent: investigation of the concentrations and distribution of pharmaceuticals and environmental risk assessment. Sci Total Environ 430:109–118
Wang JL, Zhuan R, Chu L (2019) The occurrence, distribution and degradation of antibiotics by ionizing radiation: An overview. Sci Total Environ 646:1385–1397
Westerhoff P, Yoon Y, Snyder S, Wert E (2005) Fate of endocrine-disruptor, pharmaceutical and personal care product chemicals during simulated drinking water treatment processes. Environ Sci Technol 39:6649–6663
WHO (2017) Global priority list of antibiotic-resistant bacteria to guide research, Discovery, and Development of New antibiotics. Accessed 20 May 2020 at http//:www.who.int
Zhang Y, Cai X, Lang X, Qiao X, Li X, Chen J (2012) Insights into aquatic toxicities of the antibiotics oxytetracycline and ciprofloxacin in the presence of metal: complexation versus mixture. Environ Pollut 166:48–56
Zhang H, Du Z, Ji Y, Mei M (2013) Simultaneous trace determination of acidic non-steroidal anti-inflammatory drugs in purified water, tap water, juice, soda and energy drink by hollow fiber-based liquid-phase micro extraction and ultra-high pressure liquid chromatography coupled to tandem mass spectrometry. Talanta 109:177–184
Zhang P, Zhou H, Li K, Zhao X, Liu Q, Li D, Zhao G (2018) Occurrence of pharmaceuticals and personal care products, and their associated environmental risks in a large shallow lake in north China. Environ Geochem Health 40:1525–1539
Zhao C, Pelaez M, Duan X et al (2013) Role of pH on photolytic and photocatalytic degradation of antibiotic oxytetracycline in aqueous solution under visible/solar light: kinetics and mechanism studies. Appl Catal B 134:83–92
Zounkova R, Kovalova L, Blaha L, Dott W (2010) Ecotoxicity and genotoxicity assessment of cytotoxic antineoplastic drugs and their metabolites. Chemosphere 81(2):253–260
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Kumar, B., Rai, P., Chakraborty, P. (2022). Pharmaceuticals in Indian Aquatic Environment: Risk and Implications for Management. In: Chakraborty, P., Snow, D. (eds) Legacy and Emerging Contaminants in Water and Wastewater. Emerging Contaminants and Associated Treatment Technologies. Springer, Cham. https://doi.org/10.1007/978-3-030-95443-7_3
Download citation
DOI: https://doi.org/10.1007/978-3-030-95443-7_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-95442-0
Online ISBN: 978-3-030-95443-7
eBook Packages: Earth and Environmental ScienceEarth and Environmental Science (R0)