
Abstract
Eliminating all external incisions would be a significant step in reducing the invasiveness of surgical procedures. Accessing the peritoneal cavity through a natural orifice, as in Natural Orifice Translumenal Endoscopic Surgery (NOTES), promises distinct patient advantages, but is surgically challenging. Performing laparoscopic surgeries through a single transumbilical incision is also gaining renewed interest as a potential bridge to enabling NOTES. Both of these types of surgical procedures are inherently limited by working with multiple instruments through a constrained insertion point. New technologies are necessary to overcome these limitations and provide the surgeon with adequate visual feedback and triangulation. Miniature in vivo robots provide a unique approach by providing a platform that is completely inserted into the peritoneal cavity to enable minimally invasive surgery. This chapter describes the design and feasibility testing of miniature in vivo robots that can provide stable visualization and manipulation platforms for NOTES and single incision surgery.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Cholecystectomy
- In vivo
- Laparoscopy
- LESS
- Miniature
- Minimally invasive surgery
- Natural orifice
- NOTES
- Robot
- Single incision
1 Introduction
Performing surgical procedures using minimally invasive approaches is well established, with laparoscopy now being the standard of care for many routinely performed surgical procedures. While replacing a large open incision with three to five small incisions offers significant advantages, focus remains on further reducing the invasiveness of these procedures. Natural Orifice Translumenal Endoscopic Surgery (NOTES) is a new approach to abdominal surgery that promises to reduce the invasiveness of surgical procedures by accessing the surgical target through a natural orifice. Theoretically, the elimination of external incisions avoids wound infections, further reduces pain, and improves cosmetics and recovery times [1, 2]. While NOTES may be the ultimate goal of minimally invasive surgery, significant surgical challenges have led to an increased interest in Laparoendoscopic Single-Site (LESS) surgery as an important step, and possibly a bridge to NOTES [3].
Accessing the peritoneal cavity through a natural orifice or a single abdominal incision are appealing methods from the perspective of the patient. However, both methods are surgical challenging. It is difficult to have multiple instruments passing simultaneously through a natural orifice or an incision while maintaining adequate manipulation and visualization capabilities. Current endoscopic and laparoscopic instrumentation are inadequate for NOTES and LESS procedures. New technologies are necessary that can overcome these challenges and provide the surgeon with adequate visual feedback and triangulation. This chapter describes the design and in vivo feasibility testing of miniature in vivo robots that are a novel approach to overcoming the current instrumentation limitations for NOTES and LESS.
2 Background
Accessing the surgical environment through small incisions, such as in laparoscopy, is inherently limited in scope as compared to open procedures where the surgeon can directly view and manipulate within the surgical environment. Working with long, rigid tools through access ports in the abdominal wall limits the motion of the tools and provides only a two dimensional image of the surgical environment [4, 5]. While laparoscopy is the preferred intervention for many routine interventions, such as cholecystectomy, these constraints have contributed to the limited application of laparoscopic techniques to more complex procedures.
2.1 Robotic Assistances for Minimally Invasive Surgery
Visualization and dexterity limitations for minimally invasive surgery are being addressed through the application of robotics. The Automated Endoscopic System for Optimal Positioning (AESOP) was the first robotic device to receive Food and Drug Administration approval for direct surgical manipulation in laparoscopy and was introduced in the mid-1990s for controlling a laparoscopic camera for surgical procedures [6]. The daVinci® (Intuitive Surgical, Sunnyvale, CA) system is a more advanced tele-robotic device that enables a surgeon located at a remote workstation to control robotic arms that hold the laparoscopic instruments. The surgical dexterity is enhanced through capabilities including wristed action, motion scaling, and tremor reduction. Further, a stereoscopic image of the surgical environment is displayed at the hands of the surgeon, creating the illusion that the surgical tools are extensions of the surgeon’s hands [6]. However, the universal use of the daVinci® system has remained limited primarily due to its large size, high cost, and the diminished impact of the dexterous improvements for performing less complex surgical procedures.
2.2 Natural Orifice Translumenal Endoscopic Surgery and Laparoendoscopic Single-Site Surgery
Accessing the abdominal viscera through a natural orifice may be the ultimate goal in reducing the invasiveness of surgical procedures. Natural Orifice Translumenal Endoscopic Surgery (NOTES) can be performed as a pure procedure using a single opening or as a combined procedure using multiple orifices. Hybrid procedures can also be performed using a natural orifice in conjunction with conventional transabdominal ports [7]. The feasibility of NOTES was initially demonstrated in multiple animal model studies including peritoneal exploration with liver biopsy, gastrojejunal anastomosis, organ resection, and transvesical thoracoscopy [8–11]. NOTES procedures have also been performed with success in humans including appendectomy and cholecystectomy [12–15].
Laparoendoscopic Single-Site (LESS) surgery, is another type of procedure closely related to NOTES that is gaining renewed interest. LESS procedures are performed using multiple instruments introduced though a single small transabdominal incision. LESS has been reported for cholecystectomy and appendectomy since 1998 [16, 17], but with limited momentum due to technical limitations of conventional instrumentation [18]. With recent advances in instrumentation and access methods, there is a renewed interest in single small incision surgery, with multiple procedures being performed in humans including simple nephrectomy [19, 20], pyeloplasty [19], and cholecystectomy [21, 22]. For LESS, the surgical target is often accessed using a specialized port, such as the Uni-X single Port Access System (Pnavel Systems, Cleveland, OH) or the QuadPort (Advanced Surgical Concepts, Bray, Ireland) that are introduced through a transumbilical incision. These systems incorporate individual ports for a laparoscope, insufflation, and specialized instruments.
2.3 Robotic Assistants and Instrumentation for NOTES and LESS
There is great potential for new NOTES and LESS approaches, but the technology remains in evolution [7]. Much of the work for addressing the visualization and manipulation limitations for NOTES is based on the flexible endoscopy platform. Some work focuses on developing locomotion systems for navigation of hollow cavities, such as the colon and esophagus, using methods including inchworm devices [23], rolling stents [24], and adhesion [25]. Other work is focused on improving distal tip dexterity. For example, master-slave robotic systems are being developed that use long-shafted flexible instruments with multiple degrees of freedom with standard gastroscopes or endoscopes to improve distal tip maneuverability [26, 27]. Also, the TransPort EndoSurgical Operating Platform (USGI Medical, San Clemente, CA), is a commercially available four-channel platform scope that uses ShapelockTM technology to lock the base of the endoscope for stability while also allowing for distal tip maneuverability [28].
The need for adequate triangulation for LESS is currently being addressed primarily through the use of bent or articulating instruments. However, bent tools necessitate that tissue dissection, retraction, and cautery be performed with the contralateral hand as compared to laparoscopic surgery [18] and often results in tool collisions. Alternatively, articulating tools such as RealHand (Novare Surgical Systems, Inc., Cupertino, CA) and Autonomy Laparo-Angle (Cambridge Endoscopic Devices, Inc., Framingham, MA) provide a seven degree of freedom maneuverability allowing for easier tissue manipulation. The daVinci S (Intuitive Surgical, Sunnyvale, CA) system has also been used to perform transumbilcial single port radical prostatectomy, dismembered pyeloplasty, and right side radical nephrectomy [29]. These procedures were performed using a multi-channel single access port. These studies described limited intracorporeal tool collisions and improved surgical dexterity.
While these specialized instruments and robotic systems mitigate the constraints of working through a single incision or natural orifice, limitations are inherent in approaches that require working with multiple instruments in a confined space. Even with specialized tools for LESS, instrument collisions internally and externally remain problematic. Also, flexible endoscopy approaches to NOTES instrumentation remain limited by the size and geometry of the natural orifice. An advanced laparoscopic skill set is requisite to the continued advancement of LESS and NOTES using existing instrumentation and robotic systems [18]
Novel approaches to instrumentation are necessary for the universal adoption of NOTES and LESS for performing minimally invasive surgery. One method is the use of miniature robots that are completely inserted into the peritoneal cavity through a natural orifice or a single incision. Unlike the externally actuated devices discussed previously, these robots are not constrained by the entrance incision once inserted into the peritoneal cavity. A transabdominal Magnetic Anchoring and Guidance System (MAGS) including intra-abdominal cameras and retraction instruments are currently being developed to assist in NOTES and LESS procedures [30, 31]. Once inserted into the peritoneal cavity, these devices are attached and positioned within the peritoneum using magnetic interactions with external handheld magnets. Similarly, insertable monoscopic and stereoscopic imaging devices with multiple degrees of freedom are also being developed for minimally invasive surgery [32, 33].
3 In Vivo Robots for Visualization
Miniature in vivo robots provide a platform for visualization that is completely inserted into the peritoneal cavity through a single incision or a natural orifice approach. In contrast to existing flexible endoscopy tools used as the primary visualization for many NOTES procedures, in vivo robots provide visual feedback for the surgeon that is not constrained by the axis of the endoscope or the insertion point. Further the surgeon can reposition the robot throughout a procedure to provide visualization from arbitrary orientations within each quadrant of the peritoneal cavity. Two basic designs of in vivo robots for minimally invasive surgery have been developed, as shown in Fig. 6.1. The first is a mobile in vivo platform that provides a remotely controlled movable platform for visualization and task assistance. The second is a peritoneum-mounted robot that provides visualization from a birds-eye perspective.

3.1 Mobile Camera Robot
The basic design of a mobile camera robot, shown in Fig. 6.1 left, consists of two wheels that are driven independently using permanent magnet direct current motors that provide forward, reverse, and turning motions. A tail prevents counter-rotation and allows the robot to reverse directions. A helical design for the wheel profile was developed based on viscoelastic modeling together with benchtop and in vivo testing results [34, 35]. A helical wheel profile has demonstrated maneuverability on all of the pelvic organs, including the liver, spleen, small and large bowels, as well as capabilities of climbing deformable surfaces that are two to three times its height. No visible tissue damage has resulted from the in vivo testing with this robot. Various designs of the mobile robot incorporate on-board cameras for visualization and can also include end effectors, such as a biopsy grasper, to provide task assistance capabilities.
3.2 Peritoneum-Mounted Imaging Robot
Peritoneum-mounted robots provide primary visualization for minimally invasive procedures [36]. The robot contains an external housing with magnets used for fixation to the interior abdominal wall. These magnets interact with an external magnetic handle to hold the robot to the internal abdominal wall. A schematic of the external magnetic handle, the internal imaging robot, and the abdominal wall is shown in Fig. 6.1 right. Once attached, the robot can be grossly repositioned by maneuvering the magnetic handle along the exterior surface of the abdomen, with the robot being repositioned correspondingly below. The inner housing of the robot contains a camera and two ultra-bright LEDs for lighting. The camera can be rotated to provide a tilting action using a permanent magnet direct current motor that is also contained in the inner housing of the robot. This robot is tethered for power and communications.
3.3 In Vivo Results
The in vivo robots for visualization have been demonstrated in multiple survival and non-survival procedures in a porcine model. These procedures were all performed at the University of Nebraska Medical Center with experimental protocols approved by the institutional review committee.
Mobile Camera Robot. The mobile robot platform has been used to provide the sole visualization for performing a laparoscopic cholecystectomy in a porcine model [34]. For this procedure, the robot was introduced into the peritoneal cavity through a specialized trocar. After the robot was completely inserted, this port could then be used with a standard laparoscopic tool to provide additional task assistance capabilities, such as retraction. The mobile robot with a biopsy end effector has also demonstrated the feasibility of performing a single port biopsy using a mobile robot platform, as shown in Fig. 6.2.

Mobile biopsy robot performing liver biopsy as viewed from laparoscope. (With kind permission from Springer Science+Business Media: [42])
A mobile robot has also been inserted into the peritoneal cavity using a transgastric approach [37]. For this procedure, the robot was advanced into the gastric cavity through an overtube with the assistance of an endoscope. The robot then maneuvered within the gastric cavity and was advanced into the peritoneal cavity. The robot demonstrated abilities to explore the peritoneal cavity and was removed through the esophagus using its tether.
Peritoneum-Mounted Imaging Robot. The peritoneum-mounted imaging robot has been demonstrated in multiple survival and non-survival procedures in a porcine model in cooperation with other in vivo robots and endoscopic and laparoscopic tools [36]. In the first procedure, the peritoneum-mounted imaging robot and a mobile robot were inserted into the peritoneal cavity through a standard trocar. The robots provided remotely repositionable platforms to provide visual feedback to the surgeon for the performance of a laparoscopic cholecystectomy, as shown in Fig. 6.3. A subsequent series of three survival cholecystectomies were successfully performed in a porcine model using a similar mobile camera robot and a peritoneum-mounted imaging robot.

In the third cooperative robot procedure, a peritoneum-mounted imaging robot, a lighting robot, and a retractor robot demonstrated the feasibility of inserting multiple robots with differing capabilities into the peritoneal cavity using a transgastric approach. For this procedure, the imaging robot was advanced into the peritoneal cavity through an overtube with the assistance of an endoscope. The robot was then magnetically coupled to the interior upper abdominal wall to provide visualization from an upper perspective. The retractor robot and the lighting robot were then inserted and demonstrated imaging and task assistance capabilities.
4 In Vivo Robots for Manipulation
4.1 Design Constraints
Definition of the forces, velocities, and workspace required for performing laparoscopic surgical procedures are necessary for the successful design of a manipulator robot for minimally invasive surgery. Available data for laparoscopic procedures are given almost exclusively for the forces applied by the surgeon at the tool handle instead of the actual forces applied to the tissues. Work by the BioRobotics Lab at the University of Washing uses a device called the BlueDRAGON to measure forces and motions applied by surgeons while performing various laparoscopic procedures [38, 39]. The raw data from these procedures provides useful information for determining the design requirements for a dexterous robot for manipulation. Based on this work, it was determined that the robot should be able to apply forces along and perpendicular to the tool axis of 10 and 5 N, respectively. Also, the angular velocities about the tool axis and the perpendicular axes should be on the order of 1 and 0.4 rad/s, respectively [40]
4.2 Conceptual Designs
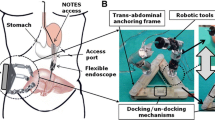
A dexterous in vivo robot for manipulation is designed to be analogous to the use of standard laparoscopic tools for performing minimally invasive the surgery. The basis of the robot design is to replace two laparoscopic tools with dexterous arms that have similar linear and angular velocity capabilities, and the ability to apply sufficient forces and torques as described above. The robot system, shown in Fig. 6.4, consists of the in vivo robot that is completely inserted into the peritoneal cavity and an external surgical control console. The robot must be flexible for insertion into the peritoneal cavity through the complex geometry of the natural lumen, and once inserted provide a stable platform for tissue manipulation and visualization.

Conceptual design of in vivo manipulator robot system for NOTES and LESS
4.3 Prototype Robot Designs
Prototypes of the dexterous manipulator robot have two prismatic arms that are each connected to a central body at a rotational shoulder joint. Each forearm has either a grasper or a cautery end effector for tissue manipulation. The body contains a stereo camera pair to provide visual feedback and an ultrabright LED for lighting. Magnets contained in the central body of the robot interact with magnets in the surgical control console to attach the robot to the interior of the abdomen and allow for gross positioning of the robot internally. This method of attachment to the abdominal wall enables the surgeon to arbitrarily position the robot throughout a surgery to provide improved visualization and manipulation capabilities within each quadrant of the peritoneal cavity [41].
The robot has two configurations to allow flexibility for insertion and also to provide stability for tissue manipulation. The robot can be changed from an articulation configuration to an insertion configuration, as shown in Fig. 6.5, by disconnecting the shoulder joint linkages. In the insertion configuration, the shoulder joints freely rotate allowing for natural orifice insertion. Once the robot has fully entered the peritoneal cavity, the shoulder linkages are reconnected allowing articulation.

Design of prototype dexterous manipulator robot in articulation (a) and insertion (b) configurations (©2008 IEEE)
4.4 Kinematic Models and Analysis
The dexterous manipulator robot is represented with the kinematic model of a two degree-of-freedom planar robot with a rotational shoulder joint and a prismatic arm joint [40]. The prototype NOTES robot is shown overlaid on the robot schematic with details of the shoulder joint expanded in Fig. 6.6. The joint variables are pitch, yaw, and lower arm extension, denoted by α 1, θ 3, and a 3, respectively. A universal frame {0} is aligned with the gravity gradient, and the parameter, α 0, defines the rotation of the robot with respect to the universal frame. The parameter, α 1, defining the angle of rotation of the robot cameras with respect to frame {1}, is zero for this robot. The constants, a 2 and a 4, define the half body width and the end effector offset with respect to the shoulder joint, respectively.

Kinematic model of the dexterous robot (left) and shoulder joint (right) (©2008 IEEE)
The necessary joint torques were determined assuming a half body width, a 2, of 40 mm, a prismatic link mass of 30 g, a workplane, α 0, of 40° below level, and lower extension, a 3, and shoulder yaw, θ 3, ranges of 64–93 mm and 75–154°, respectively. The maximum joint torque necessary at full extension of the lower arm was determined to be 522 mNm. The necessary input force, F s , to apply the necessary joint torque within the dexterous workspace defined as the range of joint angle, α 3, from 110–154°, was then determined. The shoulder joint articulation method for this robot uses a slider mechanism constrained to move in the x-direction that is coupled to the robotic arm, a 3, by a link L 1, with rotational degrees of freedom at each end. The maximum slider input force required was determined to be 67 N, assuming an overall efficiency of 50%.
4.5 User Interfaces
One version of the user interface for the dexterous miniature robot consists of two joystick controls that provide control for rotation of the shoulder joint and forearm extension, as shown in Fig. 6.7 [41]. Two pushbuttons on the left joystick are used to open and close the grasper jaws. The cautery is activated using a foot pedal. The video from one of the robot cameras is displayed on the LCD screen located between the two joysticks. The back of the control console contains magnets that interact with magnets in the body of the robot to hold the robot to the interior abdominal wall directly below the screen on the user interface. This provides for an intuitive understanding of the robot position within the peritoneal cavity. Moving the control console along the exterior surface of the abdomen effectively repositions the robot internally.

User interface for dexterous manipulator robot. (With kind permission from Springer Science+Business Media: [41])
An alternative design for the user interface uses two modified laparoscopic tools in place of the joysticks. In this design, the robot arms located internally act as extensions of the external laparoscopic handles. This interface also includes an LCD display for video feedback and a foot pedal for cautery activation. This user interface is currently used to provide on-off control of the degrees of freedom for the robot.
4.6 In Vivo Results
Multiple non-survival procedures in a porcine model have been performed using iterations of this prototype dexterous manipulator robot design [41]. The basic surgical procedure initiated with accessing the peritoneal cavity through the upper gastrointestinal tract. An overtube was inserted through a transesophageal incision and advanced through the esophagus and into through a transgastric incision made using an endoscope. The robot was then configured for insertion and advanced through the overtube and into the peritoneal cavity using a standard therapeutic endoscope. The endoscope provided supplementary visualization and observation of the robot throughout the procedure. The focus of two of the procedures was to evaluate robot functionality. For these surgeries, the robots were inserted into the peritoneal cavity through a single transabdominal incision with supplementary visualization and retraction being provided by laparoscopic tools.
For each procedure, the robot was lifted from the floor of the abdomen following insertion using the interaction of magnets embedded in the robot and in the external surgical control console. The robot was then grossly maneuvered in the proper orientation for manipulation of the gallbladder. Once in position, the grasper end effector was used to grasp the cystic duct. The cautery end effector was next moved into position to begin the dissection and the cautery was activated. The procedure continued through iterations of this stretch and dissect task with repositioning of the robot as necessary throughout to perform a cholecystectomy. Views of the robot from a laparoscope used to observe the operation of the robot and from the on-board robot cameras are shown in Figs. 6.8 and 6.9, respectively. At the end of each procedure the robot was retrieved by its tether.

Views of the robot in the peritoneal cavity from the laparoscope. (With kind permission from Springer Science+Business Media: [41])

Dissection of cystic duct as viewed from robot camera. (With kind permission from Springer Science+Business Media: [41])
These procedures demonstrated the feasibility of using a dexterous in vivo robot platform to perform LESS or NOTES from essentially a laparoscopic platform. The configurations of the robot provided sufficient flexibility for insertion through a natural orifice or a transabdominal incision. Further, the placement of the robot cameras improved tool triangulation and the surgeon’s understanding of the surgical environment. The robot design also enabled the application of sufficient off-axis forces for tissue retraction and dissection.
5 Conclusions and Future Work
Central to the widespread conversion of many surgeries in the peritoneal cavity to a less invasive NOTES or LESS approach is the further development of devices that provide the surgeon with a stable multi-tasking platform for visualization and dexterous tissue manipulation. Many of the instruments that are currently being developed are based on the design of existing laparoscopic or flexible endoscopy tools. However, these instruments remain limited by working simultaneously through a confined entrance point.
Miniature in vivo robots that are completely inserted into the peritoneal cavity through a natural orifice or a single incision provide a novel approach for addressing the constraints of LESS and NOTES. These devices can be used inside the peritoneum without the typical constraints of the access point. Miniature robots can provide the surgeon with a repositionable visualization platform using peritoneum-mounted or mobile camera robots. Also, miniature robots with dexterous end effectors, including cautery and grasping, can provide a stable platform for off-axis tissue manipulation and visualization. Further, multiple devices can be inserted through the same incision without being limited by simultaneously working through a natural orifice or single incision.
Although barriers remain to the universal application of the NOTES and LESS approaches for performing abdominal procedures, continued developments in robotic technologies promise to provide an improved platform for intuitive visualization and dexterous tissue manipulation to better enable complex procedures using these less invasive approaches. Continuing work to the miniature in vivo robotic platform includes improving robot dexterity and speed while also reducing the size of the robot.
References
Kalloo, A.N., Rattner, D., Brugge, W. et al.: ASGE/SAGES working group on natural orifice translumenal endoscopic surgery white paper. Gastrointest. Endosc. 62, 199–203 (2005)
Ko, C.W., Kalloo, A.N.: Per-oral transgastric abdominal surgery. Chin. J. Dig. Dis. 7, 67–70 (2006)
Tracy, C.R., Raman, J.D., Cadeddu, J.A., Rane, A.: Laparoendoscopic single-site surgery in urology: where have we been and where are we heading? Nat. Clin. Pract. Urol. 5, 561–568 (2008)
Tendick, F., Jennings, R., Tharp, G., Stark, L.: Perception and manipulation problems in endoscope surgery. In: Taylor, R.H., Lavallee, S., Burdea, G.C., Mosges, R. (eds.) Computer Integrated Surgery: Technology and Clinical Applications. MIT Press, Cambridge (1996)
Treat, M.: A surgeon’s perspective on the difficulties of laparoscopic surgery. In: Taylor, R.H., Lavallee, S., Burdea, G.C., Mosges, R. (eds.) Computer Integrated Surgery: Technology and Clinical Applications. MIT Press, Cambridge (1996)
Satava, R.M.: Surgical robotics: the early chronicles. Surg. Laparosc. Endosc. Percutan. Tech. 12, 6–16 (2002)
Gettman, M.T., Box, G., Averch, T. et al.: Consensus statement on natural orifice transluminal endoscopic surgery and single-incision laparoscopic surgery: heralding a new era in urology? Eur. Urol. 53, 1117–1120 (2008)
Bergstrom, M., Ikeda, K., Swain, P., Park, P.O.: Transgastric anastomosis by using flexible endoscopy in a porcine model (with video). Gastrointest. Endosc. 63, 307–312 (2006)
Kalloo, A.N., Singh, V.K., Jagannath, S.B., Niiyama, H., Hill, S.L., Vaughn, C.A., Magee, C.A., Kantsevoy, S.V.: Flexible transgastric peritoneoscopy: a novel approach to diagnostic and therapeutic interventions in the peritoneal cavity. Gastrointest. Endosc. 60, 114–117 (2004)
Lima, E., Henriques-Coelho, T., Rolanda, C., Pego, J.M., Silva, D., Carvalho, J.L.: Transvesical thoracoscopy: a natural orifice translumenal endoscopic approach for thoracic surgery. Surg. Endosc. 21, 854–858 (2007)
Merrifield, B.F., Wagh, M.S., Thompson, C.C.: Peroral transgastric organ resection: a feasibility study in pigs. Gastrointest. Endosc. 63, 693–697 (2006)
Bessler, M., Stevens, P.D., Milone, L., Parikh, M., Fowler, D.: Transvaginal laparoscopically assisted endoscopic cholecystectomy: a hybrid approach to natural orifice surgery. Gastrointest. Endosc. 6, 1243–1245 (2007)
Rao, G.V., Reddy, D.N., Banerjee, R.: NOTES: human experience. Gastrointest. Endosc. Clin. N. Am. 18, 361–370 (2008)
USGI Medical (2007) USGI announces first NOTES transgastric cholecystectomy procedures using the USGI endosurgical operating system performed by Dr. Lee Swanstrom at Legacy Hospital in Portland, OR. Updated 2007. http://www.usgimedical.com/news/releases/062507.htm. Retrieved 17 Sep 2007
Zorron, R., Filgueiras, M., Maggioni, L.C., Pombo, L., Carvalho, G.L., Oliveira, A.L.: NOTES transvaginal cholecystectomy: report of the first case. Surg. Innov. 14, 279–283 (2007)
Esposito, C.: One-trocar appendectomy in pediatric surgery. Surg. Endosc. 12, 177–178 (1998)
Piskun, G., Rajpal, S.: Transumbilical laparoscopic cholecystectomy utilizes no incisions outside the umbilicus. J. Laparoendosc. Adv. Surg. Tech. A 9, 361–364 (1999)
Kommu, S.S., Rane, A.: Devices for laparoendoscopic single-site surgery in urology. Expert Rev. Med. Devices 6, 95–103 (2009)
Desai, M.M., Rao, P.P., Aron, M. et al.: Scarless single port transumbilical nephrectomy and pyeloplasty: first clinical report. BJU Int. 101, 83–88 (2008)
Rane, A., Rao, P., Rao, P.: Single-port-access nephrectomy and other laparoscopic urologic procedures using a novel laparoscopic port (R-port). Urology 72, 260–263 (2008)
Gumbs, A.A., Milone, L., Sinha, P., Bessler, M.: Totally transumbilical laparoscopic cholecystectomy. J Gastrointest. Surg. 13, 533–534 (2009)
Hodgett, S.E., Hernandez, J.M., Morton, C.A., et al.: Laparoendoscopic single site (LESS) cholecystectomy. J Gastrointest. Surg. 13, 188–192 (2009)
Phee, L., Accoto, D., Menciass, A. et al.: Analysis and development of locomotion devices for the gastrointestinal tract. IEEE Trans. Biomed. Eng. 49, 613–616 (2002)
Breedveld, P., van der Kouwe, D.E., van Gorp, M.A.J.: Locomotion through the intestine by means of rolling stents. In: ASME Design Engineering Technical Conference, Salt Lake City, UT, pp. 963–969 (2004)
Menciassi, A., Dario, P.: Bio-inspired solutions for locomotion in the gastrointestinal tract: background and perspectives. Philos. Trans. R. Soc. Lond. 361, 2287–2298 (2003)
Abbott, D.J., Becke, C., Rothstein, R.I., Peine, W.J.: Design of an endoluminal NOTES robotic system. In: IEEE/RSJ International Conference on Intelligent Roots and Systems, San Diego, CA (2007)
Phee, S.J., Low, S.C., Sun, Z.L. et al.: Robotic system for no-scar gastrointestinal surgery. Int. J. Med. Robot. Comput. Assist. Surg. 4, 15–22 (2008)
Swanstrom, L.L., Whiteford, M., Khajanchee, Y.: Developing essential tools to enable transgastric surgery. Surg. Endosc. 22, 600–604 (2008)
Kaouk, J.H., Goel, R.K., Haber, G.P. et al.: Robotic single-port transumbilical surgery in humans: initial report. BJU Int. 103, 366–369 (2009)
Park, S., Bergs, R.A., Eberhart, R., et al.: Trocar-less instrumentation for laparoscopy: magnetic positioning of intra-abdominal camera and retractor. Ann. Surg. 245, 379–384 (2007)
Scott, D.J., Tang, S.J., Fernandez, R. et al.: Completely transvaginal NOTES cholecystectomy using magnetically anchored instruments. Surg. Endosc. 21, 2308–2316 (2007)
Hogle, N.J., Hu, T., Allen, P.K., Fowler, D.L.: Comparison of monoscopic insertable, remotely controlled imaging device with a standard laparoscope in a porcine model. Surg. Innov. 15, 271–276 (2008)
Hu, T., Allen, P.K., Nadkami, T., et al.: Insertable stereoscopic 3D surgical imaging device with pan and tilt. In: 2nd Biennial IEEE?RAS-EMBS International Conference on Biomedical Robotics and Biomechantronics, Scottsdale, AZ, pp. 311–317 (2008)
Rentschler, M.: In vivo abdominal surgical robotics: tissue mechanics modeling, robotic design, experimentation and analysis. University of Nebraska-Lincoln thesis, Biomedical Engineering (2006)
Rentschler, M., Dumpert, J., Platt, S. et al.: Modeling, analysis, and experimental study of in vivo wheeled robotic mobility. IEEE Trans. Robot. 22, 308–321 (2006)
Lehman, A.C., Berg, K.A., Dumpert, J. et al.: Surgery with cooperative robots. Comput. Aided Surg. 13, 95–105 (2008)
Rentschler, M.E., Dumpert, J., Platt, S.R. et al.: Natural orifice surgery with an endoluminal mobile robot. Surg. Endosc. 21, 1212–1215 (2006)
Lum, M.J.H., Trimble, D., Rosen, J., et al.: Multidisciplinary approach for developing a new minimally invasive surgical robotic system. In: The first IEEE/RAS-EMBS International Conference on Biomedical Robotics and Biomechatronics, pp. 841–846 (2006)
Rosen, J., Brown, J.D., Chang, L., et al.: The BlueDRAGON – a system for measuring the kinematics and dynamics of minimally invasive surgical tools in vivo. In: IEEE International Conference on Robotics and Automation, Washington DC, pp. 1876–1881 (2002)
Lehman, A.C., Wood, N.A., Dumpert, J., et al.: Dexterous miniature in vivo robot for NOTES. In: 2nd Biennial IEEE/RAS-EMBS Conference on Biomedical Robotics and Biomechatronics, Scottsdale, AZ, pp. 244–249 (2008)
Lehman, A.C., Dumpert, J., Wood, N.A. et al.: Natural orifice cholecystectomy using a miniature robot. Surg. Endosc. 23, 260–266 (2009)
Lehman, A.C., Rentschler, M.E., Farritor, S.M., Oleynikov, D.: The current state of miniature in vivo laparoscopic robotics. J. Robot. Surg. 1, 45–49 (2007)
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2011 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Farritor, S.M., Lehman, A.C., Oleynikov, D. (2011). Miniature In Vivo Robots for NOTES. In: Rosen, J., Hannaford, B., Satava, R. (eds) Surgical Robotics. Springer, Boston, MA. https://doi.org/10.1007/978-1-4419-1126-1_6
Download citation
DOI: https://doi.org/10.1007/978-1-4419-1126-1_6
Published:
Publisher Name: Springer, Boston, MA
Print ISBN: 978-1-4419-1125-4
Online ISBN: 978-1-4419-1126-1
eBook Packages: EngineeringEngineering (R0)