
Abstract
This review is a summary of factors affecting the drug pharmacokinetics (PK) of dogs versus humans. Identifying these interspecies differences can facilitate canine-human PK extrapolations while providing mechanistic insights into species-specific drug in vivo behavior. Such a cross-cutting perspective can be particularly useful when developing therapeutics targeting diseases shared between the two species such as cancer, diabetes, cognitive dysfunction, and inflammatory bowel disease. Furthermore, recognizing these differences also supports a reverse PK extrapolations from humans to dogs. To appreciate the canine-human differences that can affect drug absorption, distribution, metabolism, and elimination, this review provides a comparison of the physiology, drug transporter/enzyme location, abundance, activity, and specificity between dogs and humans. Supplemental material provides an in-depth discussion of certain topics, offering additional critical points to consider. Based upon an assessment of available state-of-the-art information, data gaps were identified. The hope is that this manuscript will encourage the research needed to support an understanding of similarities and differences in human versus canine drug PK.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
BACKGROUND
The dog is not only a preclinical species for human medicine but also a potential patient, presenting with numerous analogues of human diseases. This includes cancer, inflammatory bowel disease (IBD), diabetes, and cognitive dysfunction (1). In fact, because of the numerous homologous cancers occurring in dogs and humans, the National Cancer Institute established the Comparative Oncology Program (https://ccr.cancer.gov/comparative-oncology-program) (2). Similarly, canine cognitive dysfunction mimics Alzheimer’s disease (3, 4), containing spontaneously deposited human-type amyloid-β that shows 98% homology with that of the human protein (3).
To support these important interspecies extrapolations, there is a need to understand the respective physiological differences that can exist in drug absorption, distribution, metabolism, and elimination. Such information can also help predict interspecies differences in drug toxicity (5,6,7,8,9). Therefore, this review provides a comparison of canine vs. human physiological characteristics, transporter abundance, activity and location, and enzyme abundance, activity, and location. In some cases, this information is derived from studies conducted in the individual species. In other situations, data are from studies where both species were simultaneously assessed and compared.
Since most canine studies employ healthy adult Beagles or purpose bred mongrels, this review focuses on information generated in individuals assumed to represent a wild-type population (i.e., without genetic mutations identified in the study reports). Population variability known to exist in humans (10,11,12) and dogs (13,14,15) is not covered.
The main body of the manuscript provides a high-level comparison of the canine versus human differences impacting drug PK. A more in-depth discussion of some of the topics covered in the manuscript can be found in the Supplemental material. To further support an examination of the points covered in this review, an extensive list of references is provided.
COMPARISON OF CANINE VS. HUMAN PHYSIOLOGY, INCLUDING TRANSPORTER ABUNDANCE, ACTIVITY AND LOCATION, AND ENZYME ABUNDANCE, ACTIVITY, AND LOCATION
Gastrointestinal (GI) Physiology
Gastric Crushing Force
Dogs and humans exhibit similar area-normalized torque (approximately 3700 dynes/cm2), reflecting comparable 2-dimensional rotational force, but very different 3-dimensional crushing force (8). Using identical pressure sensitive pills in dogs and humans, the area-normalized gastric emptying force (dynes/cm2) was 606 and 962 in fasted and fed humans and was 3858 and 3639 dynes/cm2 for fasted and fed dogs (16). Similar relative differences were observed using the destructive force dependent release system (DDRS) (17, 18). This difference in crushing force can render the dog a poor model for testing human oral modified release dosage forms.
Pylorus Restrictions
The dog pylorus tends to be more restrictive than that of humans, with beads of 17 mm diameter passing through the human pylorus (fasted state, 6 ounces of water), but the dog stomach retaining particles of 5–10 mm for up to about 1.5 h (19, 20). In the fed state, particles greater than 5 mm in diameter in the dog stomach were retained for over 7.5 h (19). The corresponding timeframe in humans was more difficult to define because of its dependence on meal composition (21).
The Interdigestive Migrating Motor Complex (IMMC)
The IMMC both of humans and dogs is characterized by 4 phases. However, while phase 3 of the IMMC (rapid peristaltic contractions) is similar in both species under fasted conditions (approximately every 120 min in humans and 100 min in dogs), the time to phase 3 activity following a meal is 2.6 to 5 h in humans and 5–13 h in dogs (22, 23).
Gastric Emptying Time
The estimation of gastric emptying time can be highly dependent upon the experimental method employed (20). Using the SmartPillR GI Monitoring system, (24) observed a mean gastric emptying time of 34 min in fasted dogs and a median of 30 min (min/max = 7 to 202 min) in fasted humans (25). Species differences emerged in the fed state. While in (Beagle) dogs, the duration ranged from 1.11 to 4.53 h, it ranged from 3.08 to 19.20 h in humans (Fig. 1). Similarly, when considering those cases where the SmartPillR exited the stomach at the time of the first meal, GET estimated obtained across several canine breeds was comparable to estimates found in humans (24, 26, 27). Contrasting this to what was discussed for the IMMC, these results may reflect temporary entrapment of the SmartPillR within the human (25) and canine (28) stomach after a solid meal. Since the SmartPillR is in fact a capsule, the dimensions of this device may influence estimates of gastric emptying time and small intestinal residence time in humans (26) and dogs (27). Despite this problem, these devices are routinely used for monitoring local pH and formulation release mechanisms (26).

Mean, minimum, and maximum GI transit time measured via a SmartPill swallowed in 19 fed humans and 6 fed Beagle dogs. Meals were of comparable caloric value but differed in terms of consistency (pureed for dogs but not for humans). Graph is based upon digitized values (GetDataGraph Digitizer, version 2.6, Softnews Net SRL, SOFTPEDIAR, Sectorul 3, Romania) derived from information presented by Koziolek et al. (2015 and 2019) (24, 25). Key (based on terms used in the referenced citation): GET = gastric emptying time, SITT = small intestinal transit time, CTT = colon transit time, WGTT = whole gut transit time. Patterned columns = dog; solid columns = humans
Small Intestinal Transit Time
Most studies indicate a faster and more variable small intestinal transit time in dogs (1–2 h and not affected by the food intake) versus humans (24, 29) (Fig. 1).
Gastric pH Under Fasted and Fed Conditions
Fasted State
Given the large variability that can occur within the canine fasted stomach, the United States Pharmacopoeia (USP) recommends that drug gastric solubility in the dog be evaluated over a pH range of 1.2–6.5 (24, 29). In contrast, a single pH value (1.6) is recommended for testing in human fasted simulated gastric fluid (USP General Chapter <1236>).
Fed State
The USP General Chapter <1236> includes a description of gastric fluids for the fed state for humans but describes only the fasted state for dogs. Under fed conditions, humans tend to exhibit an initial rise in pH due to the buffering effect of food, but pH slowly returns to pre-meal conditions in a period of 60–90 min. In contrast, the dog does not exhibit this initial rise due to the buffering effect, which may be attributable to a higher basal acid secretion (29), the amount (grams) of food consumed (30), and to housing conditions [using Bravo capsules, there tended to be a slightly more acidic postprandial gastric pH when dogs were fed under home cage versus study cage conditions (31)].
Intestinal Fluid Composition
Weak acids are typically more soluble in the canine vs human fasted intestinal fluids. For neutral molecules and for weak bases with a pKa of less than 3, the difference was largely a function of the species-specific extent of bile micellization. Above pH 4, the solubility differences for weak acids were associated both with ionized and unionized drug solubilization (32).
Although the USP Chapter <1236> describes human fed and fasted intestinal and colonic fluids, only fasted small intestinal fluids are described for dogs (33,34,35). Recommended fasted state small intestinal pH is 6.5 and 7.5 for humans and dogs, respectively (where the intestinal segment is not identified for either species). These values are consistent with reports for dogs (Heidelberg capsule), where intestinal pH under fasted conditions ranged from around 6.0 immediately after gastric emptying and progressively increased to pH 7.5 at 120 min after gastric emptying (29), and for humans (IntelliCap® system) where the proximal small intestinal pH was around 6 and increased to about 7–8 in the more distal regions (36). Additional information is available in Supplemental Section 1, Table 1S.
Canine-Human Differences in Bile Composition
The impact of bile salts on drug absorption may be drug and animal species specific (32, 37). The recommended composition of canine fasted state simulated intestinal fluids (FaSSIFc) includes 5 mM sodium taurocholate and sodium taurodeoxycholate (34), while for humans, the recommendation is only 3 mM sodium taurocholate (38). The numerous canine-human differences in primary and secondary bile abundance and type (from fecal samples) (39, 40) are provided in Fig. 2. While the ratio of human bile acid conjugation to glycine (primary) versus taurine (glycine/taurine) is 3, there is negligible conjugation to glycine in dogs, with nearly all conjugation being to taurine.

Relative fecal composition of bile salts in dogs (a) versus humans (b). Note that the dog relative amounts are based upon average of individual dog values estimated across all diets studied. Values are based upon information provided by Bazzoli et al. (1982) (39) and Herstad et al. (2018) (40). Key: CA = cholic acid, CDCA = chenodeoxycholic acid, DCA = deoxycholic acid, LCA = lithocholic acid, UDCA = ursodeoxycholic acid
The largest canine-human differences in pH and bile salt content occur during the postprandial state. For example, in a study comparing the bile salt and phospholipid content in the mid-jejunum of four Labradors and in the duodenal segment of healthy human adults following a 500-mL meal of Ensure PlusR (41), the bile salt content was 18 mM and 11.8 mM in dogs and humans, respectively, at 60 min following the meal. The corresponding phospholipid content (mM) was 19.4 mM and 4.31 mM in dogs and humans, respectively.
The bile salt composition in dogs varies as a function of diet, a result believed to be linked to diet-induced modification of the gut microflora (42, 43), and potentially reflecting similar diet-associated variation in bile salt composition in humans.
There also appears to be a difference in the canine vs human bile associated ratios (μM/μM) of phospholipid (cytoprotective) to bile acid (0.19 dog vs 0.3 humans) and of cholesterol (prevents phospholipid cytoprotection) to phospholipid (0.044 vs 0.2 for dog and humans, respectively) (44). Thus, although the relative amount of phospholipid may be lower in dogs as compared to humans, the markedly higher content of cholesterol in humans relative to dogs may have implications regarding differences in hepatotoxicity in the presence of elevated bile acid concentrations (45).
Unstirred Boundary Layer (UBL)
The UBL (the complex colloidal system that coats the intestinal mucosa) can create a barrier to the absorption of a number of compounds (46), particularly those which have low solubility and high permeability (47). Although its thickness has been estimated to be about 40 μm in dogs and humans (based upon intestinal perfusion studies involving glucose and warfarin) (47), its composition and thickness is recognized to vary as a function of intestinal segments (48). Unfortunately, there is not sufficient information describing the differences in the mucous layers in humans versus dogs or its relationship to diet, genetics, or disease (49).
GUT MICROBIOME
The gut microbiota has been implicated as a potential source of population variability in human drug PK (50,51,52) and for drugs undergoing enterohepatic circulation in dogs (52, 53). Alterations in gut microbiome have also been implicated in a number of pathologies, including irritable and IBD and psychiatric disorders in humans (54,55,56) and dogs (57).
The dog gut anatomy, physiology, and diet have adapted to that of humans during domestication (58, 59). Consequently, a 60% taxonomic and functional overlap was identified between the gut microbiota of dogs and humans, in contrast to only 33% and 10–20% similarity observed between humans versus pigs and mice, respectively [based upon short sequencing reads from each host associated gut microbiome (57)]. Furthermore, the gut microbial changes observed in the presence of colorectal cancer (40), IBD (60, 61), and diabetes mellitus (62) are comparable between humans and dogs. This makes health and drug-specific PK consequences that may accompany changes in the canine microflora relevant not only from a veterinary perspective but also in terms of its potential extrapolation to humans.
The predominant fecal bacteria both in humans and dogs are Firmicutes, Bacteroidetes, and Clostridium but unlike humans, Fusobacteria also appears to be abundant in dog feces. However, the microbiome captured in the feces (luminal microflora) may not fully correlate with the microbiome adhering onto the gut wall (63,64,65).
COMPARISON OF DRUG PERMEABILITY AND ABSORPTION
The interrelationship of factors influencing effective permeability (Peff) is provided in Supplement Section 1.
Membrane Passive Intrinsic Transcellular Permeability (P trans,0)
Although Ptrans,0 tends to be similar in humans and dogs, the overall Peff needs to be considered from the perspective of absorptive surface area. In terms of intestinal length, unlike the human small intestine (cadaver) which is largely comprised of the ileum (66), the predominant segment of the canine cadaver GI tract is the jejunum (67). The shorter canine small intestine segments and rapid intestinal transit time can lead to challenges in optimizing drug product dissolution and subsequent absorption (68). In contrast, although the canine small intestinal length is about half that of humans, the long and slender villi of the canine small intestine enhances absorptive surface area, providing at least partial compensation for the shorter intestinal length (69, 70). However, the surface area in humans is further increased by the presence of the plicae circularis, which is not present in the dog (71). This additional component needs to be factored into the differences in absorptive surface area between the two species.
Paracellular Absorption
Based upon an in vitro permeability study using Caco-2 cells (which are reflective of immature small intestinal enterocytes), human intestinal pore diameter was estimated to include a restriction component of 4.3–4.5 Angstroms, Å (71). As indicated by bioavailability studies of both drugs and polyethylene glycol oligomers of varying molecular mass (Daltons, Da), the intestinal pore diameter and abundance in dogs exceeds that of humans (72, 73), leading to a tendency for greater canine paracellular drug absorption (Supplemental Section 1, Table 2S). Generating a semi-log plot of these values, we estimated that 50% polyethylene glycol bioavailability via the paracellular pathway occurs at a pore radius of 6 Å in humans (R2 for regression = 0.97; ~PEG350) and 7.14 Å in dogs (R2 for regression = 0.88; ~PEG700).
This difference in pore radius may also affect the magnitude of bioavailability enhancement associated with absorption-modifying excipients (74, 75).
Active Transport (See Intestinal Transporter Section Below)
Lymphatic Absorption
Data pertaining to lymphatic uptake in humans are not available because such investigations necessitate invasive and non-reversible surgery of the intestinal and/or thoracic lymphatic duct. (76, 77). Nevertheless, such data are available in lymph-cannulated dogs, showing that food increases the cumulative amount of triglycerides in lymph from 0.3 to 18.4 g during the first 4 h and cumulative lymph flow (g) from 174 (fasted) to 483 (fed). The impact of prandial state is even greater 8–12 h after meal (78).
While qualitatively similar effects of food on the absorption and metabolism of drugs such as halofantrine (Hf) have been reported in humans and dogs (79, 80), when administered as an amorphous solid dispersion, the fed state increased canine Hf lymphatic transport from 1.3% in the fasted state to 54% in the fed state (79). Postprandial administration increased Hf oral bioavailability by 3-fold in humans and 12-fold in Beagles and reduced the hepatic Hf metabolism by 2.4-fold in humans and by 6.8-fold in dogs (79). Similar findings of meal-enhanced lymphatic absorption and oral bioavailability were observed when the antiparasitic agent, moxidectin, was administered via intragastric lavage to lymph-cannulated dogs (81).
The canine-human comparison of lymphatic uptake and its relationship to drug physicochemical characteristics remains a topic for additional investigation.
EXTRAPOLATING DRUG CLASSIFICATION BETWEEN DOGS AND HUMANS
To better understand the impact of the differences described above, the appropriateness of extrapolating drug classifications developed for humans to dogs was explored using either the Biopharmaceutics Classification System (BCS), the Biopharmaceutics Drug Disposition Classification System (BDDS), or the Extended Clearance Classification System (ECCS) (82,83,84). While none of these systems could reliably predict human vs dog differences in drug oral bioavailability, the ECCS suggested greater canine-human correlations for weak acids, zwitterions, and compounds not undergoing pre-systemic metabolism (82).
DRUG DISTRIBUTION
Interspecies Differences in Organ-Specific Distribution of Cardiac Output (CO)
The CO (in L/h/kg body weight) is much higher in the Beagle dog as compared to that of the human [e.g., one estimate is 12.3 and 4.54 for the dog and human, respectively (Supplemental Tables 3S and 4S)]. The dog CO values exceed that predicted on the basis of allometric scaling (see Supplemental material for further discussion). The brain receives about 15–20% of the CO in young adult humans but this decreases with age (cerebral blood flow/CO ratio decreased by 1.3% per decade due to changes in cerebral blood flow) (85). In contrast, canine cerebral blood flow comprises only about 2–3% of the CO (86). Other than the brain (and possibly muscle), the Beagle-human CO distribution to all other organ systems is similar (85 and Supplemental Section 2, Table 3S).
Interspecies Differences in Steady State Volume of Distribution (Vdss)
Using data published on 152 marketed compounds covering a range of physicochemical characteristics, only 57% of the Vdss values (L/kg body weight) measured in dogs were within 2-fold that of humans (87). Plasma protein binding could not explain this disparity (88). It was concluded that species variation in Vdss reflected the tissue composition (protein vs lipid) and pH (for ionizable compounds).
Alternatively, differences in resting potential (mV) across the tissue membranes could be an indicator of possible canine-human differences influencing the diffusion of ionized drug molecules across cell membranes which, in turn, could contribute to differences in the Vdss for certain drugs. However, reported canine-human tissue-specific resting membrane potentials tended to be similar [e.g., red blood cells (− 9, − 11), muscle (− 90, − 80), and gut tissue (− 58, − 44) for dog and humans, respectively] (89,90,91,92,93). With regard to pH differences, an attempt to compare the intracellular pH of canine versus human healthy tissues revealed the sparseness of data contained within the published literature. Available data (brain, lung, muscle, red blood cells, plasma) indicate similar intracellular pH values (i.e., within a range of 7.0–7.4). Assessments of small differences in tissue intracellular pH and its impact on drug Vdss would need to consider the drug pKa, Log P, blood-plasma ratio, plasma protein binding, intracellular tissue binding, and finally the relative proportion of that particular tissue within the given species.
Given the likelihood that pH differences have negligible influence on the Vdss of most drugs, the primary cause of observed species inconsistencies appears to be differences in species tissue composition. To that end, additional insights into factors influencing canine versus human drug Vdss values were obtained from the work of Ruark et al. (94). These investigators conducted a meta-analysis of tissue composition and organ characteristics. Using a bottom-up approach, they evaluated the passive tissue/plasma water partition coefficient (\( {K}_{t:p}^{passive} \)) as a function of compound characteristic and species. The predicted \( {K}_{t:p}^{passive} \) for neutral substances with low Log PO:W was greater in dogs than humans, similar at Log PO:W ~ 2, but much greater in humans than dogs for Log PO:W > 3. As compound lipophilicity increased, the \( {K}_{t:p}^{passive} \) of all organs examined tended to be substantially higher in humans than dogs. These differences are consistent with that reported by others (87, 95). Nevertheless, similar canine-human binding to brain tissue homogenates is observed, which has been attributed to the markedly higher lipid vs. protein content of the brain and therefore higher non-specific binding to the lipid in the dog brain versus the potential for specific binding to proteins (96).
Interspecies Differences in Free Drug Concentrations
In humans, albumin comprises 50–60% of blood plasma proteins, translating to about 3.5–5.5 g/dL (https://emedicine.medscape.com/article/2054430-overview). Normal amounts of albumin in dogs range from 2.5 to 4.3 g/dL (http://webcanine.com/category/health/lab-normal-values/). The alpha1-acid glycoprotein (AAG) in healthy humans and Beagle dogs range from 0.45–1.12 mg/mL and 0.25 to 0.5 mg/mL, respectively (97). While human AAG has a wide drug binding region for basic, acidic, and neutral compounds, dogs have basic and steroid binding sites that overlap and affect each other. The dog does not appear to contain an acidic ligand binding region (98).
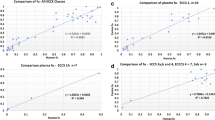
Colclough et al. (2014) evaluated the plasma protein binding of 574 compounds (acids, bases, neutral compounds, and zwitterions) (99). The ratio of % drug unbound in dog to human ranged from 0.065 to 122, with the majority of ratios between 0.5 and 5 (Fig. 3a, b).

Boxplot of ratio of % unbound drug in dogs versus humans as a function of drug acid/base properties. a Full range of values. b Y-axis truncated to define mean, median, and quartiles. Where X = mean, upper and lower limits of box are the 25 and 75 percentiles of values. Line in the middle = median. Whiskers are Q1 + 1.5 interquartile range, and points = outliers. Based upon data by Colclough et al. (2014) (99)
The authors concluded that for the given dataset, although on average, plasma protein binding in dogs was 1.5 times lower than to that of humans, there were also some drugs where the binding in dogs exceeded human plasma protein binding. The authors acknowledged that they did not distinguish between the different plasma proteins and assumed serum albumin to be the major binding protein.
With regard to binding to serum albumin, acidic drugs exhibit the largest differences in dog versus human protein binding while that of bases and possibly zwitterions are the most consistent. Potential reasons for this observation include interspecies differences in the amino acid composition of serum albumin and drug binding sites. For example, despite high levels of binding to human Sudlow site I (by hydrophobic or by static interactions) for warfarin and phenylbutazone, similar Sudlow site I binding for both compounds appeared to be absent in dogs. This was attributed to canine-human difference in the microenvironment of the binding site and its effects on the size and/or hydrophobicity of the binding pocket (100). In contrast, for drugs like diazepam and ibuprofen, Sudlow site II binding kinetics, appeared to be similar in dogs and humans (100, 101).
Drug binding sites (Sudlow sites I and II) are located within subdomains IIA and IIIA (102). Although human and canine albumin share 79.8% amino acid sequence homology, there are critical differences in the helical domains (102). As compared to human albumin, canine serum albumin exhibits an expansion of Sudlow site I, leading to both greater space and water accessibility within that binding site, thereby interfering with albumin binding to warfarin and phenylbutazone (102). It is the Sudlow site I that appears to exhibit the greatest magnitude of dissimilarity in drug binding in dogs as compared to that seen in humans.
Species differences in globulins, free fatty acids, bilirubin, or metabolites can either competitively displace drugs from albumin binding sites and/or induce conformational changes (98). Moreover, albumin can also undergo posttranslational modifications affecting its ability to interact with some drugs (103).
Species differences in drug distribution can occur due to differences in plasma constituent fractions, such as proportion of plasma lipoprotein, cholesterol, triglycerides, and apolar lipids (104). This can influence drug distribution characteristics within the blood. For example, as compared to humans, dogs have a significantly higher proportion of intravenously administered free and liposomal nystatin carried within the high-density lipoproteins, potentially influencing drug PK, toxicity, and activity (104).
METABOLISM
Humans possess N-acetyltransferase 1 (NAT1) in all tissues, and N-acetyltransferase 2 (NAT2) in the liver and intestine. In contrast, dogs do not express the NAT enzymes, thereby affecting their ability to activate or deactivate carcinogenic metabolites via this pathway (105, 106). Similarly, while humans are capable of synthesizing a single functional aldehyde oxidase (AOX1), the dog does not produce hepatic aldehyde oxidase (107).
Dog liver microsomes are about 55-fold more efficient than human in the conversion of cyclophosphamide (CP, a prodrug) to 4OHCP, the cytotoxic metabolite (108). In humans, this conversion is primarily a function of CYP2B6, with a far smaller involvement by the CYP2C subfamily (where the role of CYP2C19 exceeds that of CYP2C9) (109, 110). In dogs, Cyp2c21 and Cyp2c41 are the isoforms primarily responsible for this enzymatic conversion (108).
Rifampin is a strong inducer of CYP3A4 in humans. While induction of canine Cyp3a12 does occur (111), it is far less potent than in humans (based upon changes in mRNA levels observed in human hepatocytes versus canine liver slices) (112). Furthermore, for 22 xenobiotics (including nicardipine, rifampin, clotrimazole, and nifedipine), there was a lack of correlation between the resulting fold change in mRNA expression levels in the human (> 30-fold induction) versus canine (approximately 8-fold induction) gene. To understand the reason for this difference, the amino acid sequence of the dog and human pregnane X receptor (PXR), the predominant nuclear receptor responsible for CYP3A expression, was compared. Despite 86% homology, existing amino acid differences may cause a slight reduction in the hydrophobic region of PXR, which in turn, may impact its interaction with an inducer (112).
Metabolism Enzyme Abundance
A comparison of the fractional total composition of the various CYPs in dog versus human liver (113, 114) and intestine (113, 115) is shown in Fig. 4a and b, respectively. Human liver and intestinal cytochrome P450 distributions are provided by Paine et al. (2006) (113) and Ho et al. (2017) (117).

Comparison of cytochrome P450 composition (expressed as fraction of total CYPs) in the liver and intestine of dogs and humans. a Comparison in canine (116) versus human liver (Paine et al. (2006) (113); Shimada et al. (1994) (114). b Comparison of dog (digitized values estimated from Heikkinen et al. (2015) (115) versus those of humans (113) as a function of intestinal segment and cytochrome P450
Liver Enzymes
Human
The percent contribution, based on total immunoquantified P450 content, is 40% CYP3A, 25% CYP2C, 18% CYP1A2, 9% CYP2E1, 6% CYP2A6, 2% CYP2D6, and < 1% CYP2B6 (114). Similar values were reported by Achour et al. (2014) (118), who examined the pmol CYP enzymes/mg hepatic microsomal protein.
Dog
Considering the average protein abundance of 11 cytochrome P-450 isoforms and 2 accessory proteins across 59 dogs of varied breeds (14, 119):
-
a)
the most highly expressed enzymes (> 120 pmol/mg microsomal protein) are Cyb5a > Cyp2d15 > Cyp3a12.
-
b)
intermediately expressed (40–89 pmol/mg microsomal protein) are Cyp1a2 = Cyp2b11 = Cyp2e1 > Cyp2c21 > P450 oxidoreductase (POR)
-
c)
poorly expressed (< 12 pmol/mg microsomal protein): Cyp2a13 = Cyp2a25 = Cyp2c41 (the latter absent in the livers of many dogs) > Cyp3a26 = Cyp1a1.
In terms of interindividual variability in protein abundance:
-
a)
high = Cyp1a1 > Cyp1a2 (%CV = 105–276%).
-
b)
intermediate = Cyp2c41 = Cyp2a13 > Cyp2b11 = Cyp3a26 = Cyp2a25 > Cyp3a212 = Cyp2c21; (%CV = 36 to 67%)
-
c)
low = POR = Cyp2e1 = Cyp2d15 > Cyb5a (%CV = 16–28%).
Intestinal Enzymes
The abundance and diversity of the cytochrome P450’s is far greater in the liver than in the intestine of dogs and humans (Fig. 4a, b).
While Cyp3a and 2b11 provide the largest contribution in dogs, in humans, CYP2C9, 2C19, 2D6 (detected in most but not all individuals), and 2J2 have also been identified (113). The canine equivalent of CYP2J2 has not as yet been identified, although we have reason to believe that low levels may also be present in the canine upper small intestine (120).
The most abundant canine (Beagle) intestinal enzymes are Cyp3a12 (primary) and Cyp2b11 (secondary), with abundance and activity declining from small intestine to colon (based on enterocytes lining the intestinal villi) (121). Cyp3a12 and Cyp2b11 represent 90 and 10%, respectively, of the intestinal cytochrome P450’s in the upper small intestine (duodenum and upper jejunum), changing to 70 vs 30%, respectively, in the lower portions of the jejunum and below (116, 122). Despite the importance of intestinal drug metabolism on limiting the fraction of drug making it through the gut into the portal circulation, the same enzymes represent only a fraction of the pmol amount of expressed enzyme in the liver (116). For example, assuming 0.88 μmol and 1.45 μmol for Cyp2b11 and Cyp3a12, respectively, in Beagle whole liver, the relative expression levels across the small intestinal segments ranged from 1.59 × 10−4 (ileum) to 5.76 × 10−3 (duodenum/upper jejunum) for Cyp2b11 and from 2.92 × 10−4 (ileum) to 6.59 × 10−3 (duodenum/upper jejunum) for Cyp3a12. Similarly, activities of testosterone 6β- and 16α-hydroxylation (6β- and 16α-OHT), a marker of Cyp3a12 activity was markedly higher in the liver as compared to the small intestine, and this activity decreased along the length of the small intestine (123).
In contrast to the availability of human abundances and activities of uridine 5′-diphospho-glucuronosyltransferases (UGTs) in the literature, these data are sparse in dogs. In humans, the most abundant intestinal UGT is UGT2B17, followed by UGT1A1 and UGT1A7. In terms of canine Ugts, Ugt1a11 is the most abundant in the intestine, but also present is 1a1, 1a2, 1a3, 1a4, and 1a9 (115, 124). We are not aware of a human orthologue of Ugt1a11.
TRANSPORTERS
A summary of the assorted influx and efflux transporters found throughout the human body has been published in the 2019 international transporter consortium report (125). A synopsis of the various human and canine transporters involved in intestinal absorption (126,127,128), hepatic metabolism (10, 129), biliary secretion (130), renal elimination (131), and the blood-brain barrier (132,133,134,135,136,137) is provided in Fig. 5.

a Influx and efflux transporters in the human and canine liver, kidney, and intestine (based upon figures provided by Lai 2009 (130), Pan 2019 (10), Basit et al. (2019) (131), Estuadante et al. (2013) (126), the US FDA/University of Southern California collaborative transporter portal http://transportal.compbio.ucsf.edu/organs/small-intestine/, Burt et al. (2016) (129), Harwood et al. (2019) (128), Giacomini et al. (2010) (127), and Morris et al. (2017) (134). b Influx and efflux transporters in the humans and dogs at the blood-brain barrier (135,136,137,138,139,140). The authors also wish to express our appreciation to Dr. Matthew Harwood for conducting the meta-analysis of dog brain transporters (see Supplemental Section 6, Table 7S). Abbreviations: apical sodium-dependent bile acid transporter (ABST), breast cancer resistance protein (BCRP), bile salt efflux transporter (BSEP), equilibrative nucleoside transporter (ENT), L-amino acid transporters (LAT), multi-antimicrobial extrusion protein (MATE), monocarboxylate transporter (MCT), multidrug resistance proteins (MRP), organic anion transporter (OAT), solute carrier organic anion transporter protein (OATP), organic cationic transporter (OCT), sodium/bile acid cotransporter (NCTP), organic solute transporter (OST), peptide transporter (PEPT), P-glycoprotein (P-gp, also known as multidrug resistance protein 1, MDR1), plasma membrane monoamine transporter (PMAT). Greyed out canine transporters have not been investigated to date. # not detected * <LLOQ (below the lower limit of quantification of the analytical method)
For the sake of brevity, our discussion will focus primarily on transporters of the liver and kidney. Data on the brain can be found in the Supplement Section 6.
Liver
Published reports need to be interpreted with caution, because the interspecies comparisons are frequently based upon levels of mRNA, even though mRNA levels are often poorly correlated with the abundance of expressed protein or of transporter activity (121, 138).
In contrast to the human liver, where Solute Carrier Organic Anion Transporter Polypeptide (OATP) OATP1B1 and OATP1B3 are the most abundant transporters (about 29% of the hepatobiliary transporters), the most abundant canine transporter is Oatp1b4 (about 50% of the canine hepatobiliary transporters) (138). Using plated hepatocytes, Matsunaga et al. (139) observed that while the intracellular protein binding in humans and dogs was similar, transporter activity was not. Estimates of cell to medium concentration ratio for unbound drug (Kpuu), which reflects the interplay of active uptake, passive diffusion, and metabolism/biliary secretion, were markedly different in dogs and humans (corrected for species hepatocellularity, refer to Table 10S). Moreover, the relationship between human vs. canine uptake efficiency was compound specific. Although Wilby et al. (2011) observed somewhat greater similarity in the activity of Oatp1b4 and OATP1B3, they too found this to be substrate specific (140).
Interference in bile salt transport can result in drug-induced liver injury (DILI). Inhibition of bile salt export protein (BSEP) activity (in vitro hepatocyte assay of 24 compounds) also showed species differences, with 7 compounds having much lower IC50 values in dogs than humans, 10 of similar sensitivity (dog/human IC50 ratios ranging between 0.60 and 4.4), 3 being somewhat less sensitive in dogs (IC50 dog/human ratios of 7.39–24), and 3 compounds for which the dog failed to reflect compound’s ability to inhibit human BSEP (141).
In order of abundance, after the OATPs, the next most abundant family of transporters in the human liver are the organic cation transporters (specifically hepatic OCT1) and the multidrug resistance protein 2 (Mrp2) in dogs. In terms of the sinusoidal efflux transporters, the MRP/Mrp 3-6 were typically present in relatively small amounts in the healthy liver both of dogs and humans (138). Although this cited study did not account for transporter losses due to tissue digestion and membrane extraction [e.g., see (142)], it did provide one of the few reports containing a within-study canine-human transporter comparison.
The relative expression estimated between species provides the basis of comparisons of human versus dog as shown in Fig. 6b. Although the dog data were obtained from Wang et al. (2015) (138), the human data were taken from the meta-analysis results included in the Simcyp Simulator, Version 19. The human data provided in Fig. 6 represents data for healthy humans (adult, 20–50 years, Caucasian).

Relative contribution of hepatic transporter in the dog (a) and humans (b). The data for dogs are from Wang et al. (2015) (138). The data for humans were extracted from the figure captions
Further discussions of the relative abundance of the hepatic transporters in dogs and humans are provided in Supplemental Section 3, Table 5S. In addition, Supplemental Section 4 describes how two hepatic transporters (BSEP/Bsep and MDR3/Mdr3) can interact in the formation of bile micelles.
Kidney
The toxicity for certain renally eliminated compounds in dogs, such as the phenoxyacetic acids and related organic acids (143), has been linked with the lower capacity of dogs to secrete organic acids from the kidney. Conversely, for the acyclic nucleoside phosphonates, lower OAT-associated accumulation of these compounds in the kidney of dogs versus humans has been implicated in the corresponding lower renal toxicity of these compounds in dogs (144). This dissimilarity likely reflects the deficiency of transporters in the SLC22 family in dogs [e.g., including Oat 2, 3, 4, Oct1 (present, but at very low quantities), Oct2, Oct3, and Octn1]. Also absent in the dog is Oatp4c1 (145). Conversely, the higher affinity (lower Km value) of human vs canine OAT1 for acyclic nucleoside phosphates was responsible for renal accumulation and nephrotoxicity of many antiviral compounds in humans but not in dogs (144).
In terms of the ABC transporters, although Basit et al. (2019) concluded that breast cancer resistance protein (Bcrp) is not conserved in the canine proximal tubule (131), Wittenburg et al. (2019) were able to quantify this transporter using LC/MS/MS in the canine renal cortex (137).
A comparison of the human and canine renal transporter abundance data based upon the findings of Basit et al. (2019) is provided in Table I (131).
Scaling of the renal transporter abundance to amount per gram of dog or human kidney is provided in Supplemental Section 5 and Tables 6S and 7S.
Other Tissues
Dog
Tissues from healthy dogs were obtained during necropsies conducted at Colorado State University (breed not indicated) (145). In the canine brain (Supplemental Table 8S), the most abundant cortical ABC transporter is Bcrp, followed by P-gp. Bcrp was present in the liver, renal cortex, duodenum, and jejunum (none in the ileum). Mdr2 was found in low amounts in dog brain and liver. Mrp 6 and 7 were seen only in the liver and duodenal samples, respectively. P-gp was in the brain, liver, renal cortex, duodenum, and jejunum (duodenum higher than jejunum) and Mrp2 was only found in the renal cortex. Among the ATP-binding cassette transporters evaluated in canine tissues, the MRP family had the lowest expression in most dogs, being either present or not identified in some animals. However, tissue transporter content was based on an assumption of a linear relationship between the amount of signature peptide whose reference sequence was derived from a single boxer dog, leading to potential bias if signature peptide sequences contain variants from that of the boxer.
Human
The relevance of tissue transporter function was underscored by statin movement into cultured human skeletal muscle fibers transfected with adenovirus to over-express several transporters (146). Incubation of these in vitro muscle fibers in statin-containing media led to an association between OATP2B1 expression and muscle toxicity while MRP1 expression tended to be cytoprotective. Benet et al. (2019) further expand upon the importance of understanding transporter function in interpreting potential population variability both in terms of clearance and Vdss (147).
Using data generated on the basis of either protein or mRNA expression, a wide array of transporters were identified on the blood-brain barrier (BBB) and in the blood cerebrospinal fluid barrier (BCSFB) (134). The suggested arrangement in the human brain is included in Fig. 5b and Supplement Section 6, Table 8S.
USE OF IN SILICO PHYSIOLOGICALLY BASED PK MODELS TO SUPPORT INTERSPECIES EXTRAPOLATION
The interspecies PK extrapolation from preclinical species to humans using physiologically based pharmacokinetic (PBPK) models has gained much traction in recent years. Despite successes, as shown in Supplemental Section 7, Table S9, challenges remain regarding the extrapolation of drug metabolism or transport between the dog. A comparison of hepatic and intestinal scaling factors of dogs versus humans is provided in Supplemental Section 7, Table S10 (120, 148,149,150,151,152).
FUTURE TECHNOLOGIES TO SUPPORT INTERSPECIES EXTRAPOLATIONS
Consistent with efforts to streamline methods for characterizing candidate drugs, there is increasing interest in the development and use of miniature organs (so-called 3D organoids) derived from stem cells collected in animal or human patients (153). The goal is that through the use of these in vitro systems, it may be possible to increase our understanding of the species-specific differences in drug transport and metabolism that can influence systemic and local exposure to both parent drug and its metabolites. This information, when used to inform our PBPK models, could greatly improve our interspecies predictions.
Recent research has demonstrated that 3D intestinal organoids can be successfully maintained from healthy dogs and from dogs with naturally occurring IBD (154,155,156,157). Organoids have also been developed from dogs with urothelial carcinoma (158). These 3D systems have the potential to positively impact healthcare (e.g., in patients with bladder cancer) and streamline the development of new therapeutic strategies in humans and dogs.
CONCLUDING COMMENTS
This review reflects an effort to provide a broad overview of the factors that can lead to differences in the drug PK characteristics in dogs and humans. Despite recognized population variability that can occur in both species, an appreciation of where the greatest degree of similarities exist can support a determination of when dog-human interspecies extrapolations may be most appropriate.
One of the challenges is the proportionally small amount of information on canine enzymes and transporters as compared to that in humans. Furthermore, a major drawback is the frequent reliance on mRNA for identification of location and changes in transporters and drug-metabolizing enzymes (159). It is difficult to compare human and canine enzyme and transporter activity on the basis of anything other than expressed activities.
Given the utility of parallel drug product development, particularly as it comes to shared diseases, our goal is to encourage research efforts that fill remaining data gaps using technologies such as (but not limited to) human or canine organoids that can support use of PBPK models to accelerate veterinary and human drug development. With increased harmonization between human and animal drug development, there will be expanded opportunities to address the therapeutic needs both of humans and dogs.
GAP ANALYSIS—QUESTIONS FOR FUTURE RESEARCH
Based upon our analysis, these are the current gaps where additional research is needed:
-
Bile salts in dog intestinal fluids under fed and fasted conditions.
-
Factors that can affect canine GI fluid volumes and composition under fasted and fed conditions and how these fluids may be altered by experimental conditions.
-
Mucous layer thickness and composition in dog and humans.
-
Speciation of canine regional gut microflora, the impact of diet on gut microflora, and how changes in this microbial population can influence drug PK and health.
-
UGT expression and activity in dogs.
-
Species differences in drug-associated nuclear receptor (e.g., PXR) activation.
-
Information on canine transporter across the various tissues and their abundance and activity relative to that in humans.
-
Canine-specific organ scalars (e.g., MPPGL, HPGL, PTCPGK)
-
Quantitative information on the lymphatic pathway in humans and dogs.
Lastly, there is the need to develop reproducible and easy to use organoid assays that are linked via in vivo-in vitro extrapolation to PBPK models. If we can address these gaps, then organoids and PBPK modeling will be better suited to address the 3R’s and will indeed reduce, refine, and replace studies in animal and humans equally.
References
Schneider B, Balbas-Martinez V, Jergens AE, Troconiz IF, Allenspach K, Mochel JP. Model-based reverse translation between veterinary and human medicine: the one health initiative. CPT Pharmacometrics Syst Pharmacol. 2018;7(2):65–8.
Gordon I, Paoloni M, Mazcko C, Khanna C. The Comparative Oncology Trials Consortium: using spontaneously occurring cancers in dogs to inform the cancer drug development pathway. PLoS Med. 2009;6(10):e1000161.
Ambrosini YM, Borcherding D, Kanthasamy A, Kim HJ, Willette AA, Jergens A, et al. The gut-brain axis in neurodegenerative diseases and relevance of the canine model: a review. Front Aging Neurosci. 2019;11:130.
Schutt T, Helboe L, Pedersen LO, Waldemar G, Berendt M, Pedersen JT. Dogs with cognitive dysfunction as a spontaneous model for early Alzheimerʼs disease: a translational study of neuropathological and inflammatory markers. J Alzheimers Dis. 2016;52(2):433–49.
Bailey J, Thew M, Balls M. An analysis of the use of dogs in predicting human toxicology and drug safety. Alternatives to laboratory animals : ATLA. 2013;41(5):335–50.
Bentley RT, Ahmed AU, Yanke AB, Cohen-Gadol AA, Dey M. Dogs are manʼs best friend: in sickness and in health. Neuro Oncol. 2017;19(3):312–22.
Leenaars CHC, Kouwenaar C, Stafleu FR, Bleich A, Ritskes-Hoitinga M, De Vries RBM, et al. Animal to human translation: a systematic scoping review of reported concordance rates. Journal of Translational Medicine. 2019;17(1):223.
Martinez MN, Mochel JP, Pade D. Considerations in the extrapolation of drug toxicity between humans and dogs. Current Opinion in Toxicology. 2020;23-24:98–105.
Monticello TM, Jones TW, Dambach DM, Potter DM, Bolt MW, Liu M, et al. Current nonclinical testing paradigm enables safe entry to first-in-human clinical trials: the IQ consortium nonclinical to clinical translational database. Toxicol Appl Pharmacol. 2017;334:100–9.
Pan G. Roles of hepatic drug transporters in drug disposition and liver toxicity. Adv Exp Med Biol. 2019;1141:293–340.
Yee SW, Brackman DJ, Ennis EA, Sugiyama Y, Kamdem LK, Blanchard R, et al. Influence of transporter polymorphisms on drug disposition and response: a perspective from the International Transporter Consortium. Clin Pharmacol Ther. 2018;104(5):803–17.
Zhou SF, Liu JP, Chowbay B. Polymorphism of human cytochrome P450 enzymes and its clinical impact. Drug Metab Rev. 2009;41(2):89–295.
Martinez MN, Court MH, Fink-Gremmels J, Mealey KL. Population variability in animal health: influence on dose-exposure-response relationships: part I: drug metabolism and transporter systems. J Vet Pharmacol Ther. 2018;41(4):E57–67.
Martinez SE, Shi J, Zhu HJ, Perez Jimenez TE, Zhu Z, Court MH. Absolute quantitation of drug-metabolizing cytochrome P450 enzymes and accessory proteins in dog liver microsomes using label-free standard-free analysis reveals interbreed variability. Drug Metab Dispos. 2019;47(11):1314–24.
Mealey KL, Martinez SE, Villarino NF, Court MH. Personalized medicine: going to the dogs? Hum Genet. 2019;138(5):467–81.
Laulicht B, Tripathi A, Schlageter V, Kucera P, Mathiowitz E. Understanding gastric forces calculated from high-resolution pill tracking. Proc Natl Acad Sci U S A. 2010;107(18):8201–6.
Kamba M, Seta Y, Kusai A, Ikeda M, Nishimura K. A unique dosage form to evaluate the mechanical destructive force in the gastrointestinal tract. Int J Pharm. 2000;208(1-2):61–70.
Kamba M, Seta Y, Kusai A, Nishimura K. Evaluation of the mechanical destructive force in the stomach of dog. Int J Pharm. 2001;228(1-2):209–17.
Itoh T, Higuchi T, Gardner CR, Caldwell L. Effect of particle size and food on gastric residence time of non-disintegrating solids in Beagle dogs. J Pharm Pharmacol. 1986;38(11):801–6.
Martinez MN, Papich MG. Factors influencing the gastric residence of dosage forms in dogs. J Pharm Sci. 2009;98(3):844–60.
Mojaverian P, Ferguson RK, Vlasses PH, Rocci ML Jr, Oren A, Fix JA, et al. Estimation of gastric residence time of the Heidelberg capsule in humans: effect of varying food composition. Gastroenterology. 1985;89(2):392–7.
Code CF, Marlett JA. The interdigestive myo-electric complex of the stomach and small bowel of dogs. J Physiol. 1975;246(2):289–309.
Itoh Z, Aizawa I, Sekiguchi T. The interdigestive migrating complex and its significance in man. Clin Gastroenterol. 1982;11(3):497–521.
Koziolek M, Grimm M, Bollmann T, Schafer KJ, Blattner SM, Lotz R, et al. Characterization of the GI transit conditions in Beagle dogs with a telemetric motility capsule. Eur J Pharm Biopharm. 2019;136:221–30.
Koziolek M, Schneider F, Grimm M, Modebeta C, Seekamp A, Roustom T, et al. Intragastric pH and pressure profiles after intake of the high-caloric, high-fat meal as used for food effect studies. J Control Release. 2015;220(Pt A):71-8.
Harwood M, Neuhoff S. Establishing the colonic mean residence time for different physical drug entities in Caucasians: a meta-analysis. Simcyp Consortium Meeting; Sheffield, UK2016.
Warrit K, Boscan P, Ferguson LE, Bradley AM, Dowers KL, Rao S, et al. Minimally invasive wireless motility capsule to study canine gastrointestinal motility and pH. Vet J. 2017;227:36–41.
Boscan P. Investigating a noninvasive, at-home diagnostic technique for gastrointestinal disorders. Circle of Discovery [Internet]. 2016. Available from: https://www.pwdfoundation.org/wp-content/uploads/2016/01/D10CA-016-Boscan-FINAL-GI-disorders.pdf.
Dressman JB. Comparison of canine and human gastrointestinal physiology. Pharm Res. 1986;3(3):123–31.
Sagawa K, Li F, Liese R, Sutton SC. Fed and fasted gastric pH and gastric residence time in conscious Beagle dogs. J Pharm Sci. 2009;98(7):2494–500.
Mahar KM, Portelli S, Coatney R, Chen EP. Gastric pH and gastric residence time in fasted and fed conscious Beagle dogs using the Bravo pH system. J Pharm Sci. 2012;101(7):2439–48.
Walsh PL, Stellabott J, Nofsinger R, Xu W, Levorse D, Galipeau K, et al. Comparing dog and human intestinal fluids: implications on solubility and biopharmaceutical risk assessment. AAPS PharmSciTech. 2017;18(4):1408–16.
Akiyama Y, Kimoto T, Mukumoto H, Miyake S, Ito S, Taniguchi T, et al. Prediction accuracy of mechanism-based oral absorption model for dogs. J Pharm Sci. 2019;108(8):2728–36.
Arndt M, Chokshi H, Tang K, Parrott NJ, Reppas C, Dressman JB. Dissolution media simulating the proximal canine gastrointestinal tract in the fasted state. Eur J Pharm Biopharm. 2013;84(3):633–41.
Vertzoni M, Fotaki N, Kostewicz E, Stippler E, Leuner C, Nicolaides E, et al. Dissolution media simulating the intralumenal composition of the small intestine: physiological issues and practical aspects. J Pharm Pharmacol. 2004;56(4):453–62.
Koziolek M, Grimm M, Becker D, Iordanov V, Zou H, Shimizu J, et al. Investigation of pH and temperature profiles in the GI tract of fasted human subjects using the Intellicap((R)) system. J Pharm Sci. 2015;104(9):2855–63.
Xiao J, Tran D, Zhang X, Zhang T, Seo S, Zhu H, et al. Biliary excretion-mediated food effects and prediction. AAPS J. 2020;22(6):124.
Kimura T, Inui K, Sezaki H. Differences in effects on drug absorption between dihydroxy and trihydroxy bile salts. J Pharmacobiodyn. 1985;8(7):578–85.
Bazzoli F, Fromm H, Sarva RP, Sembrat RF, Ceryak S. Comparative formation of lithocholic acid from chenodeoxycholic and ursodeoxycholic acids in the colon. Gastroenterology. 1982;83(4):753–60.
Herstad KMV, Moen AEF, Gaby JC, Moe L, Skancke E. Characterization of the fecal and mucosa-associated microbiota in dogs with colorectal epithelial tumors. PLoS One. 2018;13(5):e0198342.
Kalantzi L, Persson E, Polentarutti B, Abrahamsson B, Goumas K, Dressman JB, et al. Canine intestinal contents vs. simulated media for the assessment of solubility of two weak bases in the human small intestinal contents. Pharm Res. 2006;23(6):1373–81.
Fiamoncini J, Curi R, Daniel H. Metabolism of bile acids in the post-prandial state. Essays in biochemistry. 2016;60(5):409–18.
Jantratid E, Janssen N, Reppas C, Dressman JB. Dissolution media simulating conditions in the proximal human gastrointestinal tract: an update. Pharm Res. 2008;25(7):1663–76.
Moschetta A, Xu F, Hagey LR, van Berge-Henegouwen GP, van Erpecum KJ, Brouwers JF, et al. A phylogenetic survey of biliary lipids in vertebrates. J Lipid Res. 2005;46(10):2221–32.
Ikeda Y, Morita SY, Terada T. Cholesterol attenuates cytoprotective effects of phosphatidylcholine against bile salts. Sci Rep. 2017;7(1):306.
Sugano K. Aqueous boundary layers related to oral absorption of a drug: from dissolution of a drug to carrier mediated transport and intestinal wall metabolism. Mol Pharm. 2010;7(5):1362–73.
Levitt MD, Furne JK, Strocchi A, Anderson BW, Levitt DG. Physiological measurements of luminal stirring in the dog and human small bowel. J Clin Invest. 1990;86(5):1540–7.
Macierzanka A, Mackie AR, Krupa L. Permeability of the small intestinal mucus for physiologically relevant studies: impact of mucus location and ex vivo treatment. Sci Rep. 2019;9(1):17516.
Herath M, Hosie S, Bornstein JC, Franks AE, Hill-Yardin EL. The role of the gastrointestinal mucus system in intestinal homeostasis: implications for neurological disorders. Front Cell Infect Microbiol. 2020;10:248.
Colotti G, Rinaldi T. The central role of gut microbiota in drug metabolism and personalized medicine. Future Med Chem. 2020;12(13):1197–200.
Li H, He J, Jia W. The influence of gut microbiota on drug metabolism and toxicity. Expert Opin Drug Metab Toxicol. 2016;12(1):31–40.
Xie Y, Hu F, Xiang D, Lu H, Li W, Zhao A, et al. The metabolic effect of gut microbiota on drugs. Drug Metab Rev. 2020;52(1):139–56.
Zhou X, Cassidy KC, Hudson L, Mohutsky MA, Sawada GA, Hao J. Enterohepatic circulation of glucuronide metabolites of drugs in dog. Pharmacol Res Perspect. 2019;7(4):e00502.
Baj A, Moro E, Bistoletti M, Orlandi V, Crema F, Giaroni C. Glutamatergic signaling along the microbiota-gut-brain axis. Int J Mol Sci. 2019;20(6).
Kelly JR, Kennedy PJ, Cryan JF, Dinan TG, Clarke G, Hyland NP. Breaking down the barriers: the gut microbiome, intestinal permeability and stress-related psychiatric disorders. Front Cell Neurosci. 2015;9:392.
Vandana UK, Barlaskar NH, Gulzar ABM, Laskar IH, Kumar D, Paul P, et al. Linking gut microbiota with the human diseases. Bioinformation. 2020;16(2):196–208.
Coelho LP, Kultima JR, Costea PI, Fournier C, Pan Y, Czarnecki-Maulden G, et al. Similarity of the dog and human gut microbiomes in gene content and response to diet. Microbiome. 2018;6(1):72.
Alessandri G, Milani C, Mancabelli L, Mangifesta M, Lugli GA, Viappiani A, et al. Metagenomic dissection of the canine gut microbiota: insights into taxonomic, metabolic and nutritional features. Environ Microbiol. 2019;21(4):1331–43.
Lyu T, Liu G, Zhang H, Wang L, Zhou S, Dou H, et al. Changes in feeding habits promoted the differentiation of the composition and function of gut microbiotas between domestic dogs (Canis lupus familiaris) and gray wolves (Canis lupus). AMB Express. 2018;8(1):123.
Vazquez-Baeza Y, Hyde ER, Suchodolski JS, Knight R. Dog and human inflammatory bowel disease rely on overlapping yet distinct dysbiosis networks. Nat Microbiol. 2016;1:16177.
White R, Atherly T, Guard B, Rossi G, Wang C, Mosher C, et al. Randomized, controlled trial evaluating the effect of multi-strain probiotic on the mucosal microbiota in canine idiopathic inflammatory bowel disease. Gut Microbes. 2017;8(5):451–66.
Jergens AE, Guard BC, Redfern A, Rossi G, Mochel JP, Pilla R, et al. Microbiota-related changes in unconjugated fecal bile acids are associated with naturally occurring, insulin-dependent diabetes mellitus in dogs. Front Vet Sci. 2019;6:199.
Barko PC, McMichael MA, Swanson KS, Williams DA. The gastrointestinal microbiome: a review. J Vet Intern Med. 2018;32(1):9–25.
Eckburg PB, Bik EM, Bernstein CN, Purdom E, Dethlefsen L, Sargent M, et al. Diversity of the human intestinal microbial flora. Science. 2005;308(5728):1635–8.
Pilla R, Suchodolski JS. The role of the canine gut microbiome and metabolome in health and gastrointestinal disease. Front Vet Sci. 2019;6:498.
Hounnou G, Destrieux C, Desme J, Bertrand P, Velut S. Anatomical study of the length of the human intestine. Surg Radiol Anat. 2002;24(5):290–4.
DeSesso JM, Jacobson CF, Williams AL. Anatomical and physiological parameters that influence gastrointestinal absorption. Encyclopedia of Drug Metabolism and Interactions. 2012:1–35.
Martinez MN, Mistry B, Lukacova V, Lentz KA, Polli JE, Hoag SW, et al. Exploring canine-human differences in product performance. Part II: use of modeling and simulation to explore the impact of formulation on ciprofloxacin in vivo absorption and dissolution in dogs. AAPS J. 2017;19(3):712–26.
Hatton GB, Yadav V, Basit AW, Merchant HA. Animal farm: considerations in animal gastrointestinal physiology and relevance to drug delivery in humans. J Pharm Sci. 2015;104(9):2747–76.
Kararli TT. Comparison of the gastrointestinal anatomy, physiology, and biochemistry of humans and commonly used laboratory animals. Biopharm Drug Dispos. 1995;16(5):351–80.
Watson CJ, Rowland M, Warhurst G. Functional modeling of tight junctions in intestinal cell monolayers using polyethylene glycol oligomers. Am J Physiol Cell Physiol. 2001;281(2):C388–97.
He YL, Murby S, Warhurst G, Gifford L, Walker D, Ayrton J, et al. Species differences in size discrimination in the paracellular pathway reflected by oral bioavailability of poly(ethylene glycol) and D-peptides. J Pharm Sci. 1998;87(5):626–33.
van De Waterbeemd H, Smith DA, Beaumont K, Walker DK. Property-based design: optimization of drug absorption and pharmacokinetics. J Med Chem. 2001;44(9):1313–33.
Dahlgren D, Roos C, Johansson P, Tannergren C, Lundqvist A, Langguth P, et al. The effects of three absorption-modifying critical excipients on the in vivo intestinal absorption of six model compounds in rats and dogs. Int J Pharm. 2018;547(1-2):158–68.
Legen I, Kracun M, Salobir M, Kerc J. The evaluation of some pharmaceutically acceptable excipients as permeation enhancers for amoxicillin. Int J Pharm. 2006;308(1-2):84–9.
Trevaskis NL, Shackleford DM, Charman WN, Edwards GA, Gardin A, Appel-Dingemanse S, et al. Intestinal lymphatic transport enhances the post-prandial oral bioavailability of a novel cannabinoid receptor agonist via avoidance of first-pass metabolism. Pharm Res. 2009;26(6):1486–95.
Yanez JA, Wang SW, Knemeyer IW, Wirth MA, Alton KB. Intestinal lymphatic transport for drug delivery. Adv Drug Deliv Rev. 2011;63(10-11):923–42.
Khoo SM, Edwards GA, Porter CJ, Charman WN. A conscious dog model for assessing the absorption, enterocyte-based metabolism, and intestinal lymphatic transport of halofantrine. J Pharm Sci. 2001;90(10):1599–607.
Humberstone AJ, Porter CJ, Charman WN. A physicochemical basis for the effect of food on the absolute oral bioavailability of halofantrine. J Pharm Sci. 1996;85(5):525–9.
Milton KA, Edwards G, Ward SA, Orme ML, Breckenridge AM. Pharmacokinetics of halofantrine in man: effects of food and dose size. Br J Clin Pharmacol. 1989;28(1):71–7.
Lespine A, Chanoit G, Bousquet-Melou A, Lallemand E, Bassissi FM, Alvinerie M, et al. Contribution of lymphatic transport to the systemic exposure of orally administered moxidectin in conscious lymph duct-cannulated dogs. Eur J Pharm Sci. 2006;27(1):37–43.
Martinez MN, El-Kattan A, Awji E, Papich M. Reconciling human-canine differences in oral bioavailability: looking beyond the Biopharmaceutics Classification System. AAPS J. 2019;21(5):99.
Papich MG, Martinez MN. Applying biopharmaceutical classification system (BCS) criteria to predict oral absorption of drugs in dogs: challenges and pitfalls. AAPS J. 2015;17(4):948–64.
Wu CY, Benet LZ. Predicting drug disposition via application of BCS: transport/absorption/elimination interplay and development of a biopharmaceutics drug disposition classification system. Pharm Res. 2005;22(1):11-23, Predicting Drug Disposition via Application of BCS: Transport/Absorption/ Elimination Interplay and Development of a Biopharmaceutics Drug Disposition Classification System.
Xing CY, Tarumi T, Liu J, Zhang Y, Turner M, Riley J, et al. Distribution of cardiac output to the brain across the adult lifespan. J Cereb Blood Flow Metab. 2017;37(8):2848–56.
Smith KA, Meyer MW. Distribution of cardiac output in dogs during intravenous infusion of betahistine. Stroke. 1976;7(3):257–60.
Chan R, De Bruyn T, Wright M, Broccatelli F. Comparing mechanistic and preclinical predictions of volume of distribution on a large set of drugs. Pharm Res. 2018;35(4):87.
Berry LM, Li C, Zhao Z. Species differences in distribution and prediction of human V(ss) from preclinical data. Drug Metab Dispos. 2011;39(11):2103–16.
Bilbrey GL, Herbin L, Carter NW, Knochel JP. Skeletal muscle resting membrane potential in potassium deficiency. J Clin Invest. 1973;52(12):3011–8.
Chow E, Huizinga JD. Myogenic electrical control activity in longitudinal muscle of human and dog colon. J Physiol. 1987;392:21–34.
Lassen UV, Sten-Knudsen O. Direct measurements of membrane potential and membrane resistance of human red cells. J Physiol. 1968;195(3):681–96.
McComas AJ, Mrozek K, Gardner-Medwin D, Stanton WH. Electrical properties of muscle fibre membranes in man. J Neurol Neurosurg Psychiatry. 1968;31(5):434–40.
Parker JC, Castranova V, Goldfinger JM. Dog red blood cells: Na and K diffusion potentials with extracellular ATP. J Gen Physiol. 1977;69(4):417–30.
Ruark CD, Hack CE, Robinson PJ, Mahle DA, Gearhart JM. Predicting passive and active tissue:plasma partition coefficients: interindividual and interspecies variability. J Pharm Sci. 2014;103(7):2189–98.
Ward KW, Smith BR. A comprehensive quantitative and qualitative evaluation of extrapolation of intravenous pharmacokinetic parameters from rat, dog, and monkey to humans. II. Volume of distribution and mean residence time. Drug Metab Dispos. 2004;32(6):612–9.
Di L, Umland JP, Chang G, Huang Y, Lin Z, Scott DO, et al. Species independence in brain tissue binding using brain homogenates. Drug Metab Dispos. 2011;39(7):1270–7.
Smith SA, Waters NJ. Pharmacokinetic and pharmacodynamic considerations for drugs binding to alpha-1-acid glycoprotein. Pharm Res. 2018;36(2):30.
Otagiri M. A molecular functional study on the interactions of drugs with plasma proteins. Drug Metab Pharmacokinet. 2005;20(5):309–23.
Colclough N, Ruston L, Wood JM, MacFaul PA. Species differences in drug plasma protein binding. MedChemComm. 2014;5(7):963–7.
Kosa T, Maruyama T, Otagiri M. Species differences of serum albumins: I. Drug binding sites. Pharm Res. 1997;14(11):1607–12.
Kaneko K, Fukuda H, Chuang VT, Yamasaki K, Kawahara K, Nakayama H, et al. Subdomain IIIA of dog albumin contains a binding site similar to site II of human albumin. Drug Metab Dispos. 2008;36(1):81–6.
Ketrat S, Japrung D, Pongprayoon P. Exploring how structural and dynamic properties of bovine and canine serum albumins differ from human serum albumin. J Mol Graph Model. 2020;98:107601.
Lee P, Wu X. Review: modifications of human serum albumin and their binding effect. Curr Pharm Des. 2015;21(14):1862–5.
Ramaswamy M, Wallace TL, Cossum PA, Wasan KM. Species differences in the proportion of plasma lipoprotein lipid carried by high-density lipoproteins influence the distribution of free and liposomal nystatin in human, dog, and rat plasma. Antimicrob Agents Chemother. 1999;43(6):1424–8.
Trepanier LA. Idiosyncratic toxicity associated with potentiated sulfonamides in the dog. J Vet Pharmacol Ther. 2004;27(3):129–38.
Trepanier LA, Cribb AE, Spielberg SP, Ray K. Deficiency of cytosolic arylamine N-acetylation in the domestic cat and wild felids caused by the presence of a single NAT1-like gene. Pharmacogenetics. 1998;8(2):169–79.
Garattini E, Terao M. The role of aldehyde oxidase in drug metabolism. Expert Opin Drug Metab Toxicol. 2012;8(4):487–503.
Ramirez DA, Collins KP, Aradi AE, Conger KA, Gustafson DL. Kinetics of cyclophosphamide metabolism in humans, dogs, cats, and mice and relationship to cytotoxic activity and pharmacokinetics. Drug Metab Dispos. 2019;47(3):257–68.
Abbott JM, Calinski D, Hollenberg P. Metabolism of cyclophosphamide by CYP 2B6 and associated polymorphisms. The FASEB Journal. 2013;27(S1):1007.7-.7.
Griskevicius L, Yasar U, Sandberg M, Hidestrand M, Eliasson E, Tybring G, et al. Bioactivation of cyclophosphamide: the role of polymorphic CYP2C enzymes. Eur J Clin Pharmacol. 2003;59(2):103–9.
Graham RA, Downey A, Mudra D, Krueger L, Carroll K, Chengelis C, et al. In vivo and in vitro induction of cytochrome P450 enzymes in Beagle dogs. Drug Metab Dispos. 2002;30(11):1206–13.
Chen J, Tran C, Xiao L, Palamanda J, Klapmuts T, Kumari P, et al. Co-induction of CYP3A12 and 3A26 in dog liver slices by xenobiotics: species difference between human and dog CYP3A induction. Drug Metab Lett. 2009;3(1):61–6.
Paine MF, Hart HL, Ludington SS, Haining RL, Rettie AE, Zeldin DC. The human intestinal cytochrome P450 “pie”. Drug Metab Dispos. 2006;34(5):880–6.
Shimada T, Yamazaki H, Mimura M, Inui Y, Guengerich FP. Interindividual variations in human liver cytochrome P-450 enzymes involved in the oxidation of drugs, carcinogens and toxic chemicals: studies with liver microsomes of 30 Japanese and 30 Caucasians. J Pharmacol Exp Ther. 1994;270(1):414–23.
Heikkinen AT, Friedlein A, Matondo M, Hatley OJ, Petsalo A, Juvonen R, et al. Quantitative ADME proteomics—CYP and UGT enzymes in the Beagle dog liver and intestine. Pharm Res. 2015;32(1):74–90.
Heikkinen AT, Fowler S, Gray L, Li J, Peng Y, Yadava P, et al. In vitro to in vivo extrapolation and physiologically based modeling of cytochrome P450 mediated metabolism in Beagle dog gut wall and liver. Mol Pharm. 2013;10(4):1388–99.
Ho MD, Ring N, Amaral K, Doshi U, Li AP. Human enterocytes as an in vitro model for the evaluation of intestinal drug metabolism: characterization of drug-metabolizing enzyme activities of cryopreserved human enterocytes from twenty-four donors. Drug Metab Dispos. 2017;45(6):686–91.
Achour B, Barber J, Rostami-Hodjegan A. Expression of hepatic drug-metabolizing cytochrome p450 enzymes and their intercorrelations: a meta-analysis. Drug Metab Dispos. 2014;42(8):1349–56.
Funk-Keenan J, Sacco J, Wong YY, Rasmussen S, Motsinger-Reif A, Trepanier LA. Evaluation of polymorphisms in the sulfonamide detoxification genes CYB5A and CYB5R3 in dogs with sulfonamide hypersensitivity. J Vet Intern Med. 2012;26(5):1126–33.
Pade D, Jamei M, Turner DB, Mistry B, Martinez MN. Danazol oral absorption modelling in the fasted dog: an example of mechanistic understanding of formulation effects on drug pharmacokinetics. Eur J Pharm Biopharm. 2019;141:191–209.
Yague E, Armesilla AL, Harrison G, Elliott J, Sardini A, Higgins CF, et al. P-glycoprotein (MDR1) expression in leukemic cells is regulated at two distinct steps, mRNA stabilization and translational initiation. J Biol Chem. 2003;278(12):10344–52.
Heikkinen AT, Friedlein A, Lamerz J, Jakob P, Cutler P, Fowler S, et al. Mass spectrometry-based quantification of CYP enzymes to establish in vitro/in vivo scaling factors for intestinal and hepatic metabolism in Beagle dog. Pharm Res. 2012;29(7):1832–42.
Kyokawa Y, Nishibe Y, Wakabayashi M, Harauchi T, Maruyama T, Baba T, et al. Induction of intestinal cytochrome P450 (CYP3A) by rifampicin in Beagle dogs. Chem Biol Interact. 2001;134(3):291–305.
Court MH. Feline drug metabolism and disposition: pharmacokinetic evidence for species differences and molecular mechanisms. Vet Clin North Am Small Anim Pract. 2013;43(5):1039–54.
Alexander SPH, Kelly E, Mathie A, Peters JA, Veale EL, Armstrong JF, et al. THE CONCISE GUIDE TO PHARMACOLOGY 2019/20: introduction and other protein targets. Br J Pharmacol. 2019;176(Suppl 1):S1–S20.
Estudante M, Morais JG, Soveral G, Benet LZ. Intestinal drug transporters: an overview. Adv Drug Deliv Rev. 2013;65(10):1340–56.
Giacomini KM, Huang S-M, Tweedie DJ, Benet LZ, Brouwer KLR, Chu X, et al. Membrane transporters in drug development. Nature Reviews Drug Discovery. 2010;9(3):215–36.
Harwood MD, Zhang M, Pathak SM, Neuhoff S. The regional-specific relative and absolute expression of gut transporters in adult Caucasians: a meta-analysis. Drug Metab Dispos. 2019;47(8):854–64.
Burt HJ, Riedmaier AE, Harwood MD, Crewe HK, Gill KL, Neuhoff S. Abundance of hepatic transporters in Caucasians: a meta-analysis. Drug Metab Dispos. 2016;44(10):1550–61.
Lai Y. Identification of interspecies difference in hepatobiliary transporters to improve extrapolation of human biliary secretion. Expert Opin Drug Metab Toxicol. 2009;5(10):1175–87.
Basit A, Radi Z, Vaidya VS, Karasu M, Prasad B. Kidney cortical transporter expression across species using quantitative proteomics. Drug Metab Dispos. 2019;47(8):802–8.
Al-Majdoub ZM, Al Feteisi H, Achour B, Warwood S, Neuhoff S, Rostami-Hodjegan A, et al. Proteomic quantification of human blood-brain barrier SLC and ABC transporters in healthy individuals and dementia patients. Mol Pharm. 2019;16(3):1220–33.
Braun C, Sakamoto A, Fuchs H, Ishiguro N, Suzuki S, Cui Y, et al. Quantification of transporter and receptor proteins in dog brain capillaries and choroid plexus: relevance for the distribution in brain and CSF of selected BCRP and P-gp substrates. Mol Pharm. 2017;14(10):3436–47.
Morris ME, Rodriguez-Cruz V, Felmlee MA. SLC and ABC transporters: expression, localization, and species differences at the blood-brain and the blood-cerebrospinal fluid barriers. AAPS J. 2017;19(5):1317–31.
Nies AT. The role of membrane transporters in drug delivery to brain tumors. Cancer Lett. 2007;254(1):11–29.
Redzic Z. Molecular biology of the blood-brain and the blood-cerebrospinal fluid barriers: similarities and differences. Fluids and Barriers of the CNS. 2011;8(1):3.
Wittenburg LA, Ramirez D, Conger H, Gustafson DL. Simultaneous absolute quantitation of ATP-binding cassette transporters in normal dog tissues by signature peptide analysis using a LC/MS/MS method. Res Vet Sci. 2019;122:93–101.
Wang L, Prasad B, Salphati L, Chu X, Gupta A, Hop CE, et al. Interspecies variability in expression of hepatobiliary transporters across human, dog, monkey, and rat as determined by quantitative proteomics. Drug Metab Dispos. 2015;43(3):367–74.
Matsunaga N, Ufuk A, Morse BL, Bedwell DW, Bao J, Mohutsky MA, et al. Hepatic organic anion transporting polypeptide-mediated clearance in the Beagle dog: assessing in vitro-in vivo relationships and applying cross-species empirical scaling factors to improve prediction of human clearance. Drug Metab Dispos. 2019;47(3):215–26.
Wilby AJ, Maeda K, Courtney PF, Debori Y, Webborn PJ, Kitamura Y, et al. Hepatic uptake in the dog: comparison of uptake in hepatocytes and human embryonic kidney cells expressing dog organic anion-transporting polypeptide 1B4. Drug Metab Dispos. 2011;39(12):2361–9.
Zhang J, He K, Cai L, Chen YC, Yang Y, Shi Q, et al. Inhibition of bile salt transport by drugs associated with liver injury in primary hepatocytes from human, monkey, dog, rat, and mouse. Chem Biol Interact. 2016;255:45–54.
Harwood MD, Russell MR, Neuhoff S, Warhurst G, Rostami-Hodjegan A. Lost in centrifugation: accounting for transporter protein losses in quantitative targeted absolute proteomics. Drug Metab Dispos. 2014;42(10):1766–72.
Timchalk C. Comparative inter-species pharmacokinetics of phenoxyacetic acid herbicides and related organic acids. evidence that the dog is not a relevant species for evaluation of human health risk. Toxicology. 2004;200(1):1–19.
Zou L, Stecula A, Gupta A, Prasad B, Chien HC, Yee SW, et al. Molecular mechanisms for species differences in organic anion transporter 1, OAT1: implications for renal drug toxicity. Mol Pharmacol. 2018;94(1):689–99.
Neuhoff S, Gaohua L, Burt H, Jamei M, Li L, Tucker GT, et al. Accounting for transporters in renal clearance: towards a mechanistic kidney model (Mech KiM). In: Sugiyama Y, Steffansen B, editors. Transporters in drug development: discovery, optimization, clinical study and regulation. New York: Springer New York; 2013. p. 155–77.
Knauer MJ, Urquhart BL, Meyer zu Schwabedissen HE, Schwarz UI, Lemke CJ, Leake BF, et al. Human skeletal muscle drug transporters determine local exposure and toxicity of statins. Circ Res. 2010;106(2):297–306.
Benet LZ, Bowman CM, Sodhi JK. How transporters have changed basic pharmacokinetic understanding. AAPS J. 2019;21(6):103.
Abdulla T, Pade D, Neuhoff S, Jamei M. Propofol: a tail of drug disposition and dynamics in different dog breeds. San Antonio: American Association of Pharmaceutical Scientist - PharmSci 360; 2019.
Kimoto E, Bi YA, Kosa RE, Tremaine LM, Varma MVS. Hepatobiliary clearance prediction: species scaling from monkey, dog, and rat, and in vitro-in vivo extrapolation of sandwich-cultured human hepatocytes using 17 drugs. J Pharm Sci. 2017;106(9):2795–804.
Pade D, Neuhoff S, Mistry B, Jamei M, Myers M, Martinez MN. PBPK modelling of collie plasma and brain concentrations as impacted by P-gp to explore loperamide-induced CNS toxicity. Wroclaw: 14th International Congress of European Association for Veterinary Pharmacology and Toxicology; 2018.
Shida S, Yamazaki H. Human plasma concentrations of five cytochrome P450 probes extrapolated from pharmacokinetics in dogs and minipigs using physiologically based pharmacokinetic modeling. Xenobiotica. 2016;46(9):759–64.
Takano R, Furumoto K, Shiraki K, Takata N, Hayashi Y, Aso Y, et al. Rate-limiting steps of oral absorption for poorly water-soluble drugs in dogs; prediction from a miniscale dissolution test and a physiologically-based computer simulation. Pharm Res. 2008;25(10):2334–44.
Clevers H. Modeling development and disease with organoids. Cell. 2016;165(7):1586–97.
Ambrosini YM, Park Y, Jergens AE, Shin W, Min S, Atherly T, et al. Recapitulation of the accessible interface of biopsy-derived canine intestinal organoids to study epithelial-luminal interactions. PLoS One. 2020;15(4):e0231423.
Chandra L, Borcherding DC, Kingsbury D, Atherly T, Ambrosini YM, Bourgois-Mochel A, et al. Derivation of adult canine intestinal organoids for translational research in gastroenterology. BMC Biol. 2019;17(1):33.
Kingsbury DD, Mochel JP, Atherly T, Chandra LC, Phillips RL, Hostetter J, et al. Mo1059—comparison of endoscopically (Egd/Colo) procured enteroids and colonoids from normal dogs and dogs with naturally occurring chronic enteropathies (IBD). Gastroenterology. 2018;154(6, Supplement 1):S-686-S-7.
Mochel JP, Jergens AE, Kingsbury D, Kim HJ, Martin MG, Allenspach K. Intestinal stem cells to advance drug development, precision, and regenerative medicine: a paradigm shift in translational research. AAPS J. 2017;20(1):17.
Lennarella-Servantez C, Gabriel V, Atherly T, Minkler S, Thenuwara S, Mao S. Collection, culture, and characterization of canine healthy bladder and urothelial carcinoma organoids: reverse translational clinical research in the veterinary patient. Barcelona: European College of Veterinary Internal Medicine Annual Conference; 2020.
Martinez MN, Greene J, Kenna L, Kissell L, Kuhn M. The impact of infection and inflammation on drug metabolism, active transport, and systemic drug concentrations in veterinary species. Drug Metab Dispos. 2020;48(8):631–44.
Acknowledgements
The authors would like to express our appreciation to Drs. Yuching Yang and Xinyuan Zhang, Center for Drug Evaluation and Research, Office of Clinical Pharmacology, FDA, for providing a critique of this manuscript.
Funding
This collaboration is part of the Cooperative Research and Development Agreement (CRADA) between the US FDA Center for Veterinary Medicine and Certara UK Limited, Simcyp Division. No external funding was involved in the development of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics in Animal and Clinical Investigations
As only available study data were used in the development of this manuscript, no additional human or animal testing occurred for the purpose of generating this review.
Conflict of Interest
JPM is a founder and COO of 3D Health Solutions, Inc. SN and DP are employees and shareholders of Certara UK, Simcyp Division.
Additional information
Guest Editors: Diane Burgess, Marilyn Morris and Meena Subramanyam
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Marilyn N. Martinez communicating author
The information in these materials is not a formal dissemination of information by FDA and does not constitute an advisory opinion, does not necessarily represent the formal position of FDA, and does not bind or otherwise obligate or commit the agency to the views expressed. This collaboration should not be construed as FDA endorsement or preference for a company or specific modeling software.
Supplementary information
ESM 1
(DOCX 233 kb)
Rights and permissions
About this article

Cite this article
Martinez, M.N., Mochel, J.P., Neuhoff, S. et al. Comparison of Canine and Human Physiological Factors: Understanding Interspecies Differences that Impact Drug Pharmacokinetics. AAPS J 23, 59 (2021). https://doi.org/10.1208/s12248-021-00590-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1208/s12248-021-00590-0