
Abstract
Background
Several studies have stated that TNF-α participates in the pathogenesis of scleritis, but also in several systemic autoimmune diseases and vasculitis, of which some are associated with scleritis. Earlier GWAS and SNP studies have confirmed that multiple SNPs of TNF related genes are associated with many immune-mediated disorders. The purpose of this study was to examine the association of TNF related gene polymorphisms with scleritis in Chinese Han. A case-control study was carried out in 556 non-infectious scleritis cases and 742 normal controls. A total of 28 single-nucleotide polymorphisms (SNPs) were genotyped by the iPLEXGold genotyping assay.
Results
No significant correlations were seen between the individual SNPs in the TNF related genes and scleritis. Haplotype analysis showed a significantly decreased frequency of a TNFAIP3 TGT haplotype (order of SNPs: rs9494885, rs3799491, rs2230926) (Pc = 0.021, OR = 0.717, 95% CI = 0.563–0.913) and a significantly increased frequency of a TNFSF4 GT haplotype (order of SNPs: rs3850641, rs704840) (Pc = 0.004, OR = 1.691, 95% CI = 1.205–2.372) and TNFSF15 CCC haplotype (order of SNPs: rs6478106, rs3810936, rs7865494) (Pc = 0.012, OR = 1.662, 95% CI = 1.168–2.363) in patients with scleritis as compared with healthy volunteers.
Conclusions
This study reveals that a TGT haplotype in TNFAIP3 may be a protective factor for the development of scleritis and that a GT haplotype in TNFSF4 and a CCC haplotype in TNFSF15 may be risk factors for scleritis in Chinese Han.
Similar content being viewed by others


Background
Scleritis is a relatively uncommon and heterogeneous ocular disorder which is clinically characterized by the insidious onset of ocular redness, pain, and tenderness [1]. According to the anatomic location, it is usually classified into anterior, posterior, or pan-scleritis [2]. Scleritis is an inflammation of the stroma of the sclera. The inflammatory process of the sclera may extend to adjacent tissues if not treated adequately, possibly causing several ocular complications and even blindness [3, 4]. However, the precise etiologic pathways or mechanisms of scleritis are not yet clear and a number of studies have indicated that an immune imbalance triggered by environmental factors may contribute to chronic inflammation of the sclera in genetically predisposed individuals [5, 6].
Several studies have stated that TNF-α participates in the pathogenesis of scleritis [7,8,9], but also in several systemic autoimmune diseases and vasculitis [10,11,12], of which some are associated with scleritis [1, 13, 14]. Earlier GWAS and SNP studies have confirmed that multiple SNPs of TNF related genes are associated with many immune-mediated disorders, including ankylosing spondylitis (AS) [15], rheumatoid arthritis (RA) [16,17,18], multiple sclerosis (MS) [19], inflammatory bowel disease (IBD) [20,21,22,23], psoriasis [24], systemic sclerosis (SSc) [25,26,27], and systemic lupus erythematosus (SLE) [28,29,30]. Whether TNF related gene polymorphisms are associated with scleritis has not yet been reported and was therefore the subject of the study reported here. A case-control study was made to investigate the association of genetic polymorphisms in TNF related genes with scleritis, whereby we included 28 SNPs that had previously been demonstrated to be related with autoimmune or autoinflammatory diseases.
Results
Clinical features of the enrolled cases and controls
The demographic and clinical characteristics of the 556 scleritis cases and 742 included volunteers are shown in Table 1.
Genotyping results of tested SNPs
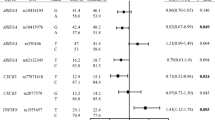
In total, 28 SNPs of 556 scleritis patients and 742 healthy individuals were genotyped and analyzed. None of SNPs deviated from HWE in the healthy volunteers, and the call rate of all SNPs tested was above 90%. Two SNPs, rs9494885 and rs2230926 in TNFAIP3, were correlated with scleritis. Lower frequencies of the T allele and TT genotype of rs9494885 (P = 0.047, OR = 0.727, 95% CI = 0.530–0.997; P = 0.042, OR = 0.710, 95% CI = 0.510–0.989, respectively) and higher frequencies of the C allele and TC genotype (P = 0.047, OR = 1.376, 95% CI = 1.003–1.886; P = 0.045, OR = 1.406, 95% CI = 1.007–1.965, respectively) were observed in scleritis patients as compared to the controls (Table 2). Regarding rs2230926, we found that the frequencies of the TT genotype and T allele were decreased in scleritis patients (P = 0.037, OR = 0.660, 95% CI = 0.446–0.997; P = 0.040, OR = 0.675, 95% CI = 0.464–0.984, respectively), while the G allele and GT genotype frequencies were increased (P = 0.040, OR = 1.481, 95% CI = 1.016–2.157; P = 0.039, OR = 1.519 95% CI = 1.020–2.263, respectively; Table 2). However, the statistical significance of the weak associations with scleritis was lost after Bonferroni correction (Table 2). As for the remaining 26 SNPs, we did not observe any association with scleritis (Supplementary Table S2).
Age effects
Due to the significant difference between the average age of the scleritis patients and normal controls, and to exclude the influence of age on the results, we divided the patients and healthy controls into young and old age groups, based on the average age, and then performed statistical analysis to determine whether age affects genotype and allele frequency. The results show that there were no significant differences in genotype and allele frequencies between younger and older people either in patients or healthy controls (Table 3).
Stratified analysis
To further confirm whether anatomical location and associated systemic diseases could affect the frequencies of genotypes and alleles in scleritis, we performed a stratified study of the two SNPs described above in various scleritis subgroups compared to normal controls, including patients with anterior, posterior, and pan-scleritis and in patients with or without related systemic diseases. No statistical differences were found in the subgroups of scleritis with the two SNPs after Bonferroni correction (Supplementary Table S3).
Haplotype analysis
The haplotypes of TNFAIP3 (tumor necrosis factor alpha-induced protein 3), TNFRSF1A (tumor necrosis factor receptor superfamily member 1A), TNFSF4 (tumor necrosis factor ligand superfamily member 4), and TNFSF15 (tumor necrosis factor ligand superfamily member 15) having more than one SNP were analyzed on the SHEsis online platform in our scleritis patients [31]. Haplotypes were not included in the analysis if the frequency was below 3%. A TNFAIP3 TGT haplotype (order of SNPs: rs9494885, rs3799491, rs2230926), a TNFSF4 GT haplotype (order of SNPs: rs3850641, rs704840), and a TNFSF15 CCC haplotype (order of SNPs: rs6478106, rs3810936, rs7865494) showed significant associations with scleritis (Pc = 0.021, OR = 0.717, 95% CI = 0.563–0.913; Pc = 0.004, OR = 1.691, 95% CI = 1.205–2.372; Pc = 0.012, OR = 1.662, 95% CI = 1.168–2.363, respectively) (Tables 4, 5, and 6). On the basis of anatomical location subgroups, stratified analysis showed that the TNFSF4 GC haplotype frequency was increased in the anterior and generalized (pan) scleritis group in comparison with the healthy volunteers group (Pc = 0.022, OR = 1.636, 95% CI = 1.117–2.396; Pc = 4.38 × 10−4, OR = 3.744, 95% CI = 1.772–7.910, respectively) (Table 5). The TNFSF15 CCC haplotype frequency was significantly increased in the anterior scleritis group (Pc = 0.003, OR = 1.860, 95% CI = 1.267–2.730), but this was not seen in the other scleritis groups (Table 6). Dividing patients into subgroups with or without systemic diseases, decreased frequency of TNFAIP3 TGT haplotype was observed, whereas elevated frequency of TNFSF4 GT haplotype was found in patients without systemic diseases (Pc = 0.024, OR = 0.715, 95% CI = 0.558–0.916; Pc = 0.004, OR = 1.719, 95% CI = 1.216–2.430, respectively) (Tables 4 and 5). The TNFSF15 CCC haplotype frequency was discovered to be significantly increased in scleritis cases without as well as with systemic diseases, as compared with healthy volunteers (Pc = 0.039, OR = 1.579, 95% CI = 1.096–2.274; Pc = 0.027, OR = 2.496, 95% CI = 1.229–5.067, respectively) (Table 6). The TNFRSF1A haplotype was not significantly correlated with scleritis or its subgroups (Supplementary Table S4).
Discussion
In this study, haplotype analysis showed that a TNFAIP3 TGT haplotype, a TNFSF4 GT haplotype, and a TNFSF15 CCC haplotype were significantly associated with scleritis. Any individual SNPs did not show a statistically significant association with scleritis.
Only few studies have analyzed genetic associations with uveitis. A significantly increased frequency of the GG genotype and G allele of rs3087243 in CTLA4 has been reported in scleritis [6]. Haplotype analysis showed a significantly increased prevalence of the TTATACGCG haplotype in PTPN22 and a decreased prevalence of the TCAA haplotype in CTLA4 (order of SNPs: rs3789604, rs150426536, rs1746853, rs12174003, rs1217406, rs3789609, rs1217414, rs3789612, rs2488457; order of SNPs: rs733618, rs5742909, rs231775, rs3087243, respectively) [6].
We made several efforts to validate the experimental data and guarantee the correctness of our experimental results [32]. Firstly, our scleritis patients were selected on the basis of well-defined criteria including the engorgement of the vascular plexus in the superficial and deep episclera and swelling and edema in the scleral tissues. Second, we excluded scleritis patients with a definite infectious etiology. Third, to avoid ethnic bias, only Chinese Han patients and controls were included. Furthermore, to avoid confounding by genetic ancestry, the healthy volunteers were matched according to the geographical regions of the patients.
TNFAIP3 encodes a ubiquitin-editing enzyme A20, working downstream of TNF-α [24]. It inhibits the NF-kB signaling pathway and thus prevents overstimulation of the immune response [24, 33]. In our study, weak associations were detected between two SNPs in the TNFAIP3 gene and scleritis. We found an increased prevalence of the TC genotype and a decreased frequency of the TT genotype in rs9494885 among scleritis patients. This trend has also been reported in Behcet’s disease (BD) [34], allergic rhinitis (AR) [35], and Vogt-Koyanagi-Harada syndrome (VKH) [36] in Chinese Han populations. This variant does not have a direct biological function, since the TNFAIP3 expression was not obviously different in TC genotype as compared to TT genotype carriers of rs9494885 in BD [34]. Moreover, we observed that the TT genotype frequency was lower, while the GT genotype frequency was higher in rs2230926, which is a nonsynonymous variant and leads to a change of the A20 protein at residue 127 from phenylalanine to cysteine [37]. Previous studies also reported similar observations concerning the risk association of scleritis with the G allele and GT genotype, such as RA [38], SLE [28, 39], and primary immune thrombocytopenia (IPT) [40]. Furthermore, the expression of A20 mRNA was higher in rs2230926 GT genotype as compared to TT genotype carriers [41]. GT genotype carriers were more likely to have a poor treatment outcome in RA patients [41]. On the basis of the research findings referred above, we hypothesized that the genotypes that showed an association with other autoimmune disorders might also play a role in the development of scleritis.
Haplotype analysis allows a joint estimation of the role of multiple SNPs in a gene, and it may be more effective than the one-SNP-at-a-time approach to tag uncommon associated variants in catching genetic associations by reducing dimensionality [42]. We observed that one TNFAIP3 haplotype TGT was protective for developing scleritis, and this specific association has to our knowledge not been found in other diseases. The response to TNF blockers has been reported to be significantly associated with the TNFAIP3 TG haplotype (order of SNPs: rs2230926, rs610604) in psoriasis [43]. Additional studies are necessary to investigate whether TNFAIP3 haplotypes might also have an impact on the therapeutic response of scleritis patients to biological agents.
We also found a higher frequency of the TNFSF4 GT haplotype in scleritis patients. The tumor necrosis factor ligand superfamily member 4 (TNFSF4, OX40L) encodes a type II transmembrane protein which can interact with TNFRSF4 (OX40) leading to a costimulatory signal for various immune responses, and which has been put forward as a potential therapeutic target to control autoimmunity [44]. In earlier reports, the GT haplotype of the TNFSF4 gene (order of SNPs: rs844648, rs704840) played a protective role in neuromyelitis optica spectrum disorders in Chinese [45]. The AA haplotype of TNFSF4 (order of SNPs: rs844648, rs10912580) has been shown to be correlated with the occurrence of breast cancer [46]. The biological function of the GT haplotype described in our study has not yet been reported, and its exact role in the pathogenesis of scleritis therefore remains unclear.
Our results showed that a TNFSF15 CCC haplotype was associated with an increased susceptibility to develop scleritis. TNFSF15 encodes the tumor necrosis factor-like ligand 1a (TL1A), which acts as a costimulatory molecule regulating T cell-mediated immunity [47]. The local and systemic levels of TLA1 were significantly increased in scleritis related systemic diseases, such as RA [48], psoriasis [49], IBD [50], AS [51], and SLE [52]. TL1A serum levels were significantly decreased in patients with RA [48] after treatment with an anti-TNF agent and AS patients [51]. Similar results of TNFSF15 haplotype analysis were discovered in IBD [20], breast cancer [53], SLE [54], CD [21], and UC [55], although the composition of the haplotypes was different from that found in our study. How these haplotypes affect the function of TNF related pathways is unclear and deserves further investigation.
Conclusions
In conclusion, we identified the association of various TNF gene related haplotypes with scleritis in Chinese Han, including TGT in TNFAIP3, GT in TNFSF4, and CCC in TNFSF15.
Materials and methods
Subjects
For this project, we recruited 556 patients with scleritis and 742 matched healthy controls at the Department of Ophthalmology of the First Affiliated Hospital of Zhengzhou University (Zhengzhou, China, from May 2017 to November 2019) and the Department of Ophthalmology of the First Affiliated Hospital of Chongqing Medical University (Chongqing, China, from May 2009 to November 2019). The patients with the presence of swelling and edema in the scleral tissues and engorgement of the superficial and deep vascular plexus of the episclera were diagnosed as scleritis, as shown in an earlier paper [1, 2]. Anterior, posterior, and generalized (pan) scleritis were defined following published classification schemes [1, 2]. Fourteen cases were excluded because they were caused by an infection (13 tuberculosis, 1 leprosy). Patients with an unclear diagnosis due to lack of sufficient clinical details, such as a satisfactory B-scan or UBM data, were excluded. All participants were Han Chinese. The 742 enrolled healthy controls were matched with regard to ethnicity, sex, and age.
SNP selection
A thorough search was performed through a combination of different search terms in the Medline, PubMed, and Ensembl databases, which includes polymorphisms, single-nucleotide polymorphisms (SNPs), genetic polymorphisms, gene polymorphism, TNFAIP3, TNFRSF1A, TNFSF4, TNFSF15, and all the aliases for these four genes. In the end, an aggregate of 405 articles and 49 SNPs were screened (Supplementary Table S5), which were revealed to have a significant association with one or more inflammatory and autoimmune disorders. Using the Han Chinese HapMap database, we checked the linkage disequilibrium (LD) between certain SNPs (r2 threshold of 0.8) and a known polymorphism in Chinese populations, which resulted in the exclusion of 21 SNP sites, despite the fact that these SNPs have been reported to be associated with the susceptibility of several immune-mediated disorders in other ethnic groups. Seven SNPs lacked a polymorphism in the Chinese population, and 14 SNPs showed a linkage disequilibrium with other SNPs (Supplementary Table S6). After using these criteria, we ended up with a total of 28 SNPs, which included TNFAIP3 (rs7753873, rs5029928, rs9494885, rs610604, rs2230926, rs3799491), TNFRSF1A (rs4149577, rs1800693, rs767455, rs2234649, rs1800692, rs4149570, rs4149578, rs12426675), TNFSF4 (rs12039904, rs1234315, rs2205960, rs704840, rs1234314, rs3850641, rs3861950), and TNFSF15 (rs6478106, rs4979462, rs3810936, rs6478108, rs11554257, rs7865494, rs10817669).
DNA extraction and genotyping
The QIAamp DNA Blood Mini Kit (Qiagen, Valencia, CA, USA) was used to obtain genomic DNA from peripheral blood collected in EDTA tubes and stored at − 80 °C until used for genotype analysis. The primer sequences of iPLEX reactions were designed through Mass ARRAY® Assay design software (Supplementary Table S1). This experiment was performed strictly according to the guidelines of the manufacturer (Agena Bioscience, San Diego, CA, USA). The iPLEX Gold Assay and TYPER version 4.0.20 software was used to identify and analyze genotypes of patients and controls.
Statistical analysis
The significant deviation from the Hardy-Weinberg equilibrium (HWE) was calculated using chi-square (χ2) test in the healthy group. All experimental data concerning differences of candidate SNPs with respect to genotype and allele were evaluated using the χ2 or Fisher’s exact test by SPSS version 19.0 (SPSS, Chicago, IL, USA). Bonferroni correction was applied to account for multiple testing. This method multiplies the P value of the chi-square or Fisher’s exact test by the number of simultaneous tests (n = 28) in our study. A Pc (P value correction) less than 0.05 was taken as statistically significant.
Availability of data and materials
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Abbreviations
- GWAS:
-
Genome-wide association studies
- SNP:
-
Single-nucleotide polymorphism
- TNF:
-
Tumor necrosis factor
- TNFAIP3:
-
Tumor necrosis factor alpha-induced protein 3
- TNFSF4:
-
Tumor necrosis factor ligand superfamily member 4
- TNFSF15:
-
Tumor necrosis factor ligand superfamily member 15
- TNFRSF1A:
-
Tumor necrosis factor receptor superfamily member 1A
- AS:
-
Ankylosing spondylitis
- RA:
-
Rheumatoid arthritis
- MS:
-
Multiple sclerosis
- IBD:
-
Inflammatory bowel disease
- SSc:
-
Systemic sclerosis
- SLE:
-
Systemic lupus erythematosus
- BD:
-
Behcet’s disease
- AR:
-
Allergic rhinitis
- VKH:
-
Vogt-Koyanagi-Harada syndrome
- IPT:
-
Primary immune thrombocytopenia
- CD:
-
Crohn’s disease
- UC:
-
Ulcerative colitis
- HWE:
-
Hardy-Weinberg equilibrium
References
Yang P, Ye Z, Tang J, Du L, Zhou Q, Qi J, et al. Clinical features and complications of scleritis in Chinese patients. Ocul Immunol Inflamm. 2018;26:387–96.
Watson PG, Hayreh SS. Scleritis and episcleritis. Br J Ophthalmol. 1976;60:163–91.
Watson PG, Young RD. Scleral structure, organisation and disease. A review. Exp Eye Res. 2004;78:609–23.
Wieringa WG, Wieringa JE, ten Dam-van Loon NH, Los LI. Visual outcome, treatment results, and prognostic factors in patients with scleritis. Ophthalmology. 2013;120:379–86.
Wakefield D, Di Girolamo N, Thurau S, Wildner G, McCluskey P. Scleritis: immunopathogenesis and molecular basis for therapy. Prog Retin Eye Res. 2013;35:44–62.
Li F, Ma X, Du L, Shi L, Cao Q, Li N, et al. Identification of susceptibility SNPs in CTLA-4 and PTPN22 for scleritis in Han Chinese. Clin Exp Immunol. 2019;197:230–6.
Levy-Clarke G, Jabs DA, Read RW, Rosenbaum JT, Vitale A, Van Gelder RN. Expert panel recommendations for the use of anti-tumor necrosis factor biologic agents in patients with ocular inflammatory disorders. Ophthalmology. 2014;121:785–96 e3.
Ragam A, Kolomeyer AM, Fang C, Xu Y, Chu DS. Treatment of chronic, noninfectious, nonnecrotizing scleritis with tumor necrosis factor alpha inhibitors. Ocul Immunol Inflamm. 2014;22:469–77.
de Fidelix TS, Vieira LA, de Freitas D, Trevisani VF. Biologic therapy for refractory scleritis: a new treatment perspective. Int Ophthalmol. 2015;35:903–12.
Braun J, Sieper J. Ankylosing spondylitis. Lancet. 2007;369:1379–90.
Maki-Petaja KM, Elkhawad M, Cheriyan J, Joshi FR, Ostor AJ, Hall FC, et al. Anti-tumor necrosis factor-alpha therapy reduces aortic inflammation and stiffness in patients with rheumatoid arthritis. Circulation. 2012;126:2473–80.
Armstrong AW, Read C. Pathophysiology, clinical presentation, and treatment of psoriasis: a review. JAMA. 2020;323:1945–60.
Sainz de la Maza M, Foster CS, Jabbur NS. Scleritis associated with systemic vasculitic diseases. Ophthalmology. 1995;102:687–92.
Akpek EK, Thorne JE, Qazi FA, Do DV, Jabs DA. Evaluation of patients with scleritis for systemic disease. Ophthalmology. 2004;111:501–6.
Zinovieva E, Bourgain C, Kadi A, Letourneur F, Izac B, Said-Nahal R, et al. Comprehensive linkage and association analyses identify haplotype, near to the TNFSF15 gene, significantly associated with spondyloarthritis. PLoS Genet. 2009;5:e1000528.
Scherer HU, van der Linden MP, Kurreeman FA, Stoeken-Rijsbergen G, Cessie S, Huizinga TW, et al. Association of the 6q23 region with the rate of joint destruction in rheumatoid arthritis. Ann Rheum Dis. 2010;69:567–70.
Thomson W, Barton A, Ke X, Eyre S, Hinks A, Bowes J, et al. Rheumatoid arthritis association at 6q23. Nat Genet. 2007;39:1431–3.
Plenge RM, Cotsapas C, Davies L, Price AL, de Bakker PI, Maller J, et al. Two independent alleles at 6q23 associated with risk of rheumatoid arthritis. Nat Genet. 2007;39:1477–82.
Gregory AP, Dendrou CA, Attfield KE, Haghikia A, Xifara DK, Butter F, et al. TNF receptor 1 genetic risk mirrors outcome of anti-TNF therapy in multiple sclerosis. Nature. 2012;488:508–11.
Thiebaut R, Kotti S, Jung C, Merlin F, Colombel JF, Lemann M, et al. TNFSF15 polymorphisms are associated with susceptibility to inflammatory bowel disease in a new European cohort. Am J Gastroenterol. 2009;104:384–91.
Yang SK, Lim J, Chang HS, Lee I, Li Y, Liu J, et al. Association of TNFSF15 with Crohn’s disease in Koreans. Am J Gastroenterol. 2008;103:1437–42.
Wellcome Trust Case Control C. Genome-wide association study of 14,000 cases of seven common diseases and 3,000 shared controls. Nature. 2007;447:661–78.
Brant SR, Okou DT, Simpson CL, Cutler DJ, Haritunians T, Bradfield JP, et al. Genome-wide association study identifies African-specific susceptibility loci in African Americans with inflammatory bowel disease. Gastroenterology. 2017;152:206–17.e2.
Nair RP, Duffin KC, Helms C, Ding J, Stuart PE, Goldgar D, et al. Genome-wide scan reveals association of psoriasis with IL-23 and NF-kappaB pathways. Nat Genet. 2009;41:199–204.
Bossini-Castillo L, Broen JC, Simeon CP, Beretta L, Vonk MC, Ortego-Centeno N, et al. A replication study confirms the association of TNFSF4 (OX40L) polymorphisms with systemic sclerosis in a large European cohort. Ann Rheum Dis. 2011;70:638–41.
Dieude P, Guedj M, Wipff J, Ruiz B, Riemekasten G, Matucci-Cerinic M, et al. Association of the TNFAIP3 rs5029939 variant with systemic sclerosis in the European Caucasian population. Ann Rheum Dis. 2010;69:1958–64.
Gourh P, Arnett FC, Tan FK, Assassi S, Divecha D, Paz G, et al. Association of TNFSF4 (OX40L) polymorphisms with susceptibility to systemic sclerosis. Ann Rheum Dis. 2010;69:550–5.
Musone SL, Taylor KE, Lu TT, Nititham J, Ferreira RC, Ortmann W, et al. Multiple polymorphisms in the TNFAIP3 region are independently associated with systemic lupus erythematosus. Nat Genet. 2008;40:1062–4.
Graham RR, Cotsapas C, Davies L, Hackett R, Lessard CJ, Leon JM, et al. Genetic variants near TNFAIP3 on 6q23 are associated with systemic lupus erythematosus. Nat Genet. 2008;40:1059–61.
Cunninghame Graham DS, Graham RR, Manku H, Wong AK, Whittaker JC, Gaffney PM, et al. Polymorphism at the TNF superfamily gene TNFSF4 confers susceptibility to systemic lupus erythematosus. Nat Genet. 2008;40:83–9.
Li Z, Zhang Z, He Z, Tang W, Li T, Zeng Z, et al. A partition-ligation-combination-subdivision EM algorithm for haplotype inference with multiallelic markers: update of the SHEsishttp://analysis.bio-x.cn. Cell Res. 2009;19:519–23.
Yang P, Du L, Ye Z. How to deal with uveitis patients? Curr Mol Med. 2018;17:468–70.
Liu YC, Penninger J, Karin M. Immunity by ubiquitylation: a reversible process of modification. Nat Rev Immunol. 2005;5:941–52.
Li H, Liu Q, Hou S, Du L, Zhou Q, Zhou Y, et al. TNFAIP3 gene polymorphisms confer risk for Behcet’s disease in a Chinese Han population. Hum Genet. 2013;132:293–300.
Ke X, Yang Y, Shen Y, Wang X, Hong S. Association between TNFAIP3 gene polymorphisms and risk of allergic rhinitis in a Chinese Han population. Iran J Allergy Asthma Immunol. 2016;15:46–52.
Li H, Liu Q, Hou S, Du L, Zhou Q, Zhou Y, et al. TNFAIP3 gene polymorphisms in a Chinese Han population with Vogt-Koyanagi-Harada syndrome. PLoS One. 2013;8:e59515.
Odqvist L, Jevnikar Z, Riise R, Oberg L, Rhedin M, Leonard D, et al. Genetic variations in A20 DUB domain provide a genetic link to citrullination and neutrophil extracellular traps in systemic lupus erythematosus. Ann Rheum Dis. 2019;78:1363–70.
Shimane K, Kochi Y, Horita T, Ikari K, Amano H, Hirakata M, et al. The association of a nonsynonymous single-nucleotide polymorphism in TNFAIP3 with systemic lupus erythematosus and rheumatoid arthritis in the Japanese population. Arthritis Rheum. 2010;62:574–9.
Ciccacci C, Latini A, Perricone C, Conigliaro P, Colafrancesco S, Ceccarelli F, et al. TNFAIP3 gene polymorphisms in three common autoimmune diseases: systemic lupus erythematosus, rheumatoid arthritis, and primary Sjogren syndrome-association with disease susceptibility and clinical phenotypes in Italian patients. J Immunol Res. 2019;2019:6728694.
Zhou H, Yang J, Liu L, Zhang D, Zhou K, Li H, et al. The polymorphisms of tumor necrosis factor-induced protein 3 gene may contribute to the susceptibility of chronic primary immune thrombocytopenia in Chinese population. Platelets. 2016;27:26–31.
Zhu L, Wang L, Wang X, Zhou L, Liao Z, Xu L, et al. Characteristics of A20 gene polymorphisms and clinical significance in patients with rheumatoid arthritis. J Transl Med. 2015;13:215.
Clark AG. The role of haplotypes in candidate gene studies. Genet Epidemiol. 2004;27:321–33.
Tejasvi T, Stuart PE, Chandran V, Voorhees JJ, Gladman DD, Rahman P, et al. TNFAIP3 gene polymorphisms are associated with response to TNF blockade in psoriasis. J Invest Dermatol. 2012;132:593–600.
Webb GJ, Hirschfield GM, Lane PJ. OX40, OX40L and autoimmunity: a comprehensive review. Clin Rev Allergy Immunol. 2016;50:312–32.
Lian Z, Liu J, Shi Z, Chen H, Zhang Q, Feng H, et al. Association of TNFSF4 polymorphisms with neuromyelitis optica spectrum disorders in a Chinese population. J Mol Neurosci. 2017;63:396–402.
Weiguang Y, Dalin L, Lidan X, Yonggang C, Shuang C, Yanhong L, et al. Association of OX40L polymorphisms with sporadic breast cancer in northeast Chinese Han population. PLoS One. 2012;7:e41277.
Aiba Y, Nakamura M. The role of TL1A and DR3 in autoimmune and inflammatory diseases. Mediat Inflamm. 2013;2013:258164.
Bamias G, Siakavellas SI, Stamatelopoulos KS, Chryssochoou E, Papamichael C, Sfikakis PP. Circulating levels of TNF-like cytokine 1A (TL1A) and its decoy receptor 3 (DcR3) in rheumatoid arthritis. Clin Immunol. 2008;129:249–55.
Bamias G, Evangelou K, Vergou T, Tsimaratou K, Kaltsa G, Antoniou C, et al. Upregulation and nuclear localization of TNF-like cytokine 1A (TL1A) and its receptors DR3 and DcR3 in psoriatic skin lesions. Exp Dermatol. 2011;20:725–31.
Song L, Zhou R, Huang S, Zhou F, Xu S, Wang W, et al. High intestinal and systemic levels of interleukin-23/T-helper 17 pathway in Chinese patients with inflammatory bowel disease. Mediat Inflamm. 2013;2013:425915.
Konsta M, Bamias G, Tektonidou MG, Christopoulos P, Iliopoulos A, Sfikakis PP. Increased levels of soluble TNF-like cytokine 1A in ankylosing spondylitis. Rheumatology (Oxford). 2013;52:448–51.
Xu WD, Chen DJ, Li R, Ren CX, Ye DQ. Elevated plasma levels of TL1A in newly diagnosed systemic lupus erythematosus patients. Rheumatol Int. 2015;35:1435–7.
Han S, Liu L, Xu F, Chen S, Yuan W, Fu Z, et al. A case-control study about the association between vascular endothelial growth inhibitor gene polymorphisms and breast cancer risk in female patients in Northeast China. Chin J Cancer Res. 2016;28:435–43.
Wang XM, Tu JC. TNFSF15 is likely a susceptibility gene for systemic lupus erythematosus. Gene. 2018;670:106–13.
Baskaran K, Pugazhendhi S, Ramakrishna BS. Protective association of tumor necrosis factor superfamily 15 (TNFSF15) polymorphic haplotype with ulcerative colitis and Crohn’s disease in an Indian population. PLoS One. 2014;9:e114665.
Yang P, Gao Y, Du L, Li F, Ding J, Li G, et al. The association of TNF related gene polymorphisms with scleritis in Chinese Han. 2020.
Acknowledgements
We would like to express our sincere gratitude to all patients and volunteers who participated in this study. We previously submitted the manuscript as a preprint to Authorea (DOI: 10.22541/au.159541386.63678604) [56].
Funding
This work was supported by the Talent Development Program for the Medical College of Zhengzhou University, the “51282” Project for Henan Medical Science and Technology Innovative Talents, and the National Natural Science Foundation Project (81770914 and 81970729).
Author information
Authors and Affiliations
Contributions
PY, YG, LD, and FL conceptualized and designed the experiments. YG accomplished the experiments and wrote the original manuscript. YG, JD, and GL performed the initial statistical analysis. QC, NL, and GS collected the samples and prepared the materials and reagents. PY and AK reviewed the important intellectual content and revised the manuscript. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures were in line with the principles of the Declaration of Helsinki. Written informed consent was acquired from all participants; for children, it was obtained from their parents or guardians. The experimental protocol was given the approval by the Clinical Research Ethics Committee of the First Affiliated Hospital of Chongqing Medical University and the Medical Ethics Committee of the First Affiliated Hospital of Zhengzhou University.
Consent for publication
All patients consented to the publication of their data.
Competing interests
All authors have declared no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Gao, Y., Du, L., Li, F. et al. The haplotypes of various TNF related genes associated with scleritis in Chinese Han. Hum Genomics 14, 46 (2020). https://doi.org/10.1186/s40246-020-00296-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40246-020-00296-y