
Abstract
The tumour necrosis factor receptor OX40 (CD134) is activated by its cognate ligand OX40L (CD134L, CD252) and functions as a T cell co-stimulatory molecule. OX40-OX40L interactions have been proposed as a potential therapeutic target for treating autoimmunity. OX40 is expressed on activated T cells, and in the mouse at rest on regulatory T cells (Treg). OX40L is found on antigen-presenting cells, activated T cells and others including lymphoid tissue inducer cells, some endothelia and mast cells. Expression of both molecules is increased after antigen presentation occurs and also in response to multiple other pro-inflammatory factors including CD28 ligation, CD40L ligation and interferon-gamma signaling. Their interactions promote T cell survival, promote an effector T cell phenotype, promote T cell memory, tend to reduce regulatory function, increase effector cytokine production and enhance cell mobility. In some circumstances, OX40 agonism may be associated with increased tolerance, although timing with respect to antigenic stimulus is important. Further, recent work has suggested that OX40L blockade may be more effective than OX40 blockade in reducing autoimmunity. This article reviews the expression of OX40 and OX40L in health, the effects of their interactions and insights from their under- or over-expression. We then review OX40 and OX40L expression in human autoimmune disease, identified associations of variations in their genes (TNFRSF4 and TNFSF4, respectively) with autoimmunity, and data from animal models of human diseases. A rationale for blocking OX40-OX40L interaction in human autoimmunity is then presented along with commentary on the one trial of OX40L blockade in human disease conducted to date. Finally, we discuss potential problems with clinical use of OX40-OX40L directed pharmacotherapy.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
There is increasing interest in the role of the T cell co-stimulatory tumour necrosis factor receptor (TNFR) OX40 and its cognate ligand, OX40L, in immunoregulation, and especially as a therapeutic target. Capacity exists both to enhance immune activity to promote immune responses in vaccination and to break tolerance in cancer immunotherapy, and also to reduce immune activity in hypersensitivity, atherosclerosis, sepsis and autoimmunity. This review considers autoimmunity.
Autoimmunity may be considered as a ‘clinical syndrome caused by the activation of T cells or B cells, or both, in the absence of an ongoing infection or other discernible cause’ [1] and is typically associated with autoantibodies reactive against self antigens [2]. Autoimmune disease, where there is also a negative effect on health in addition to autoimmunity, affects some 3 % of the US population. It may cause long-term morbidity compounded by side effects from untargeted immunosuppressive therapy [3]. In addition, several autoimmune diseases are not responsive to standard immunosuppressants and there is a need for effective but targeted and tolerable therapy. This review focuses on the logical and experimental evidence for the potential of OX40-L manipulation to treat autoimmunity.
OX40 and OX40 Ligand
The tumour necrosis factor receptor OX40 was first identified on activated rat lymphocytes: The first murine OX40 antibody was raised in mice immunized with phytohemagluttinin-activated rat lymph node. The antibody bound exclusively to activated CD4+ T cells and increased their proliferation after standardized stimulation in culture [4]. The identifier CD134 has since been allocated to the target receptor with its single transmembrane domain and cysteine-rich extracellular domain, but the name OX40 remains more common and is used in this review [5]. OX40’s cognate ligand is variously described as OX40L, CD134L, CD252 and gp34; OX40L will be used hereafter.
In 1994, OX40L was identified on an EBV-transformed B cell line with low-level expression on activated T cells [6]. This ligand for OX40 is a type II transmembrane protein and both mRNA and protein are markedly induced in human T cell leukaemia virus 1-infected cells. OX40L is expressed in trimeric form and binds three OX40 molecules with high affinity and slow dissociation [7, 8]. After it was cloned, OX40L was shown to increase T cell proliferation in response to a variety of standard stimuli [6].
OX40 and OX40L are encoded by TNFRSF4 and TNFSF4 on chromosome 1, where they are in close proximity to other TNF family molecules. The ligand-receptor pair is only present in the mammalian lineage and has been proposed as having evolved to permit the fine-tuning of memory and high-affinity antibody production to allow continued reproductive success after placentation [9]. Initial cloning and first sequencing revealed similarities to CD40L and CD40 (TNFSF5/TNFSFR5), and they were later established as members of the TNF and TNF receptor superfamilies [5].
Expression of OX40
Since its identification, the expression profile of OX40 has been confirmed as being predominantly on activated lymphocytes, and amongst these predominantly CD4+ T cells. On human CD4+ T cells, there is no expression of OX40 at rest, although in murine regulatory T cells (Treg) constitutive expression is reported [10]. Expression is seen on activated, memory and regulatory CD4+ T cells [11, 8, 12], at lower levels on activated CD8+ cells [13] but not on naïve cells. OX40 expression is also a marker of thymic T cells receiving positive selection signals [14]. Further, lower level OX40 expression is seen on NKT cells [15], NK cells [16] and neutrophils [17]. Reports on the function of OX40 other than on T cells are limited and the remainder of this article considers T cell OX40 alone.
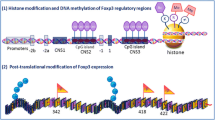
T cell receptor ligation alone is sufficient to drive OX40 expression on CD4 + T cells, but co-stimulatory ligation of CD28 by CD80 and CD86 (together B7) augments expression, as does CD40-CD40L ligation [18, 19]. IL-2 may induce OX40 on both CD4 and CD8 T cells [20, 21] and IL-1 and TNF also contribute. Further, the proteins Roquin 1 and 2 act as posttranscriptional regulators of protein expression and appears to act to degrade OX40 mRNAs: deficiency in functional Roquin results in increased expression [22] (see Fig. 1).

OX40 and OX40L expression, interaction and molecular consequences. At rest, no or minimal OX40 and OX40L is expressed. Expression of both is increased by antigen presentation to the T cell receptor and the engagement of co-stimulatory molecules (CD28 with CD80 and CD86, and CD40L with CD40) in a mechanism that involves the influx of calcium. OX40L is expressed on both APC and T cell; OX40 expression is limited to the T cell. Expression on naïve cells occurs after 24 to 72 h. Factors affecting expression are highlighted. Arrows denote positive effects; barred lines denote negative effects. APC = antigen-presenting cell; IFN-γ = interferon gamma; TLR = toll-like receptor; PGE2 = prostaglandin E2; IL = interleukin; mRNA = messenger ribonucleic acid; MHC II = major histocompatibility complex class II; TCR = T cell receptor; TNF = tumour necrosis factor
Reports on the time-course of OX40 expression vary, but in general expression on previously unstimulated CD4+ T cells reaches maximal 48 h after T cell receptor stimulation in both mouse [23] and human [24]. Murine memory T cells will re-express OX40 within 4 h of re-stimulation [23]. Such rapid re-expression of OX40 appears to be partly regulated by Sp1/Sp3, YY1 and NFκB. NFκB histone acetylation has been demonstrated in memory T cells, which express OX40 in a few hours on stimulation [25].
Consistent with observations that it restricted to activated T cells, OX40 expression is often confined to sites of inflammation and immune activation in human disease and this is reviewed below [26, 27]. In myelin-immunized rats, which go on to develop experimental allergic encephalomyelitis (EAE), OX40 denoted those T cells that were specific for myelin [28] and OX40 demarcation of antigen specificity is also true after Th1-type response promoting Listeria infection [29]. In humans, OX40 expression on T cells has been reported to demarcate autoreactive cells in type 1 diabetes mellitus [30].
Expression of OX40 Ligand
As with OX40, OX40L expression is upregulated in response to antigen presentation on multiple antigen-presenting cells: these include B cells [31], macrophages [32] and dendritic cells [33]. The repertoire of cells that can be induced to express OX40L is broader than for OX40 and reports exist of expression on mast cells [34, 35], bronchial smooth muscle [36], malignancies [37], vascular endothelial cells [38] and Langerhans cells [39]. There is constitutive expression on lymphoid tissue inducer cells [40]. Activated CD4+ and CD8+ T cells may also express OX40L and this may be enhanced by IL-12 exposure, with CD4+ cells showing greater expression than CD8+ [41, 42].
Factors promoting OX40L expression other than antigen presentation and accompanying co-stimulation include interferon gamma (IFNγ), in an IFNγ-receptor-dependent mechanism [43, 44], prostaglandin E2 [45], TSLP [46] and IL-18 [47]. Finally, human serum soluble OX40L increases with age [48].
Functions of OX40-OX40 Ligand Interactions
OX40 Engagement Expands Effector T cells and Prolongs Their Survival
Experiments with a soluble form of OX40L have shown that its engagement amplifies T cell proliferative responses to a range of stimuli [6]. Activation does not affect early proliferation and activation but controls late proliferation and activation states [41, 19]. Figure 2 summarizes the effects of OX40 ligation.

Effects of OX40 ligation on T cells. Major effects of OX40 ligation are highlighted in bold with effector mechanisms below. Note that in some situations, OX40 ligation promotes a regulatory rather than effector phenotype: see text. Molecular mechanisms are described in more detail in Fig. 4. Arrows denote positive effects; barred lines denote negative effects; dashed lines show relations. APC = antigen-presenting cell, IL: interleukin; IL2Rα = IL-2 receptor alpha; IL-12R = IL-12 receptor; IFN-γ = interferon gamma; CXCR5 = C-X-C chemokine receptor type 5; Th1 = T-helper cell type 1; Th2 = T-helper cell type 2; Th17 = T-helper cell type 17; CTLA-4 = cytotoxic T-lymphocyte associated protein 4; TGF-β = transforming growth factor beta; FoxP3 = Forkhead box p3; Bcl-2 = B cell lymphoma 2; Bcl-xL = B cell lymphoma-extra large; BCL2A1 = Bcl-2-related protein A1; FAS = Fas cell surface death receptor; TRAF = TNF receptor-associated factor; NFκB = nuclear factor kappa-light-chain-enhancer of activated B cells; ERK = extracellular-signal-regulated kinases; PI3K = Phosphatidylinositol-4,5-bisphosphate 3-kinase; AKT = protein kinase B
In vivo work has shown that OX40 ligation preferentially expands the antigen-specific T cell pool [49, 50]. Correspondingly, there is reduced CD4+ expansion in OX40- or OX40L-deficient mice and constitutive OX40L expression by either dendritic cells (DCs) [51] or T cells [52] results in a greater numbers of activated CD4+ T cells, and transfecting DCs with OX40L mRNA increases their CD4+ T cell stimulatory potency and increases T cell polarization [53].
OX40 ligation results in augmentation of effector cytokine production [23] and prolongation of activation, and this is partially mediated through stabilization of mRNA [54]. The cytokines produced appear dependent on other factors: see below. An important mechanism by which T cells may prolong activation is through T cell-T cell interactions: by expression of both OX40L and OX40 on activation, T cells may stimulate other T cells, so sustaining activation [41]. Thus, proliferation is reduced in stimulated pure T cell cultures by OX40L blockade. An intriguing observation with relevance to autoimmunity is that T cells activated through OX40 become resistant to subsequent regulation by Treg [10].
The direction of T cell polarization is dependent on the cytokine milieu and may favour Th1, Th2 [33, 46], Th9 [55] or Th17 [56] cytokine production depending on circumstances; naïve T cells predominantly produce IL-4 [57]. OX40 ligation’s general net effect of promoting immune activation was demonstrated in a landmark experiment where a single dose of agonistic OX40 antibody was demonstrated to break tolerance that had been induced to an exogenous peptide [58].
OX40 and T cell Regulation
Both mice and humans lacking OX40 have reduced numbers of natural Treg alongside a reduction in other non-naïve T cell subtypes [10, 37]. Correspondingly, mice that constitutively express OX40L on T cells have increased numbers of Treg in their spleens alongside autoimmunity (see below; [52]). OX40, together with the other TNFRSF members, appears to couple the signal strength of TCR signals and fine-tune sensitivity to IL-2 [59]. Given that both TCR signal strength and IL-2 receptor signaling contribute to thymic Treg selection, this is consistent with the observation that OX40 marks thymic T cells receiving signals of positive selection [14].
OX40 agonists can drive Treg expansion in TGFβ-treated cultures, although the cytokine milieu is key. If IFNγ and IL-4 are present, there is preferential expansion of effector CD4+; with blockade of IL-4 and IFNγ, there is Treg expansion [60]. However, OX40 stimulation without IL-2 produces weakly proliferating, poorly suppressive Treg whilst exogenous IL-2 is sufficient to correct this [61]. Further experiments in lymphocyte cultures treated with the combination of anti-CD3 and anti-CD28 antibodies with exogenous IL-2 have suggested a Treg inhibiting role of OX40: in vitro TGFβ-driven conversion to Treg is reduced by OX40 in both mouse and human [62, 63]. In a variety of carcinoma models, agonistic anti-OX40 injected into tumours causes Treg deactivation and depletion, and also mediated tumour regression [64]. Similarly, the expansion and regulatory capability of established ‘ICOS + IL-10’ Tregs is inhibited by OX40 [63, 65].
OX40-deficient Treg appear to have reduced suppressive function. In a study of transfer colitis, Treg lacking OX40 were ineffective at correcting disease whereas their replete counterparts were effective [66], and in an allograft model, OX40 treated Treg were less able to suppress rejection, effector T cell proliferation or interferon-γ production [67].
OX40 Promotes and Sustains CD4+ T cell Memory
Numbers of memory cells are increased after administration of OX40 agonists in a TRAF2-dependent manner in an antigen-specific mouse model [68] and OX40 is required for both maintenance and effective reactivation in memory T cell-mediated allograft rejection [69]. Similarly, OX40 signals are required for appropriate expansion of a memory T cell pool. Appropriately, fewer memory T cells are seen in OX40 deficiency [49, 70] and numbers are increased in mice with constitutive OX40L expression on either DC [51] or CD4+ T cells [52] or with OX40L antibody ligation [49]. These findings are supported by the observation that OX40 signals permit and sustain the acquired response to vaccination [13].
OX40 Promotes Generation of Memory CD8+ T cells
OX40-L interactions appear to have an analogous role in cytotoxic CD8+ T cells to that in CD4+ cells: initial activation is not inhibited by their absence and initial responses to viral infection are maintained [71]. However, OX40 promotes CD8+ T cell survival [72] and the generation and maintenance of antigen-specific cells [73]. CD8-mediated allograft rejection is impaired in the absence of OX40-L interactions [74] and anti-tumour immunity is improved after treatment with OX40 agonists in a number of models [75], and this may be in part by forcing CD8+ T cells out of senescence [76].
Ligated OX40 Forms a Signaling Complex Which Alters Transcription Through Multiple Pathways
The molecular events that follow OX40 engagement by OX40L are incompletely described although there is interaction with a number of established pro-inflammatory mediators. Molecular pathways are summarized as Fig. 3.

Signaling pathways after OX40 stimulation. OX40L is trimeric and each trimer associates with three OX40 molecules. The signaling complex alters transcription through multiple pathways: a signaling complex involving TNF receptor associated factor 2 and 6, and possibly TRAF5, and IKKα, IKKβ, IKKγ is formed, IκB is phosphorylated and degraded and the NFκB sub-unit RelA, along with p50 is then able to enter the nucleus [167, 168, 68]; in a TRAF6-dependent process, IKKα acts to permit RelB nuclear entry [55]; the OX40 signaling complex phosphorylates STAT5 permitting nuclear entry [61]; OX40 permits the intracellular entry of calcium, this then activates calcineurin via calmodulin resulting in the dephosphorylation and nuclear entry of NFAT [8]; PI3K complexed to activated OX40 increases phosphorylation of AKT (also known as a PKB) in a PDK-dependent manner, this in turn amplifies signaling through the IKK complex [100]. The NFAT and PI3K pathways amplify signals from antigen-stimulated T cell receptors. There are multiple transcriptional effects including suppression of FoxP3 [67] and increased transcription of BLIMP-1 [169] tending to promote an overall effector phenotype. Cytokine transcription is dependent on pre-existing polarization state: e.g. IL-9 in Th9 cells [55]. Note that a number of these pathways are shared with other TNFRs and T cell receptor stimulation itself. TRAF = Tumour Necrosis Factor (TNF) receptor associated factor; STAT = Signal Transducer and Activator of Transcription; PI3K = phosphatidylinositol 3-kinase; PDK = phosphoinositide-dependent kinase; AKT = protein kinase B; IKK = IκB kinase; NFAT = nuclear factor of activated T cells; RelA and RelB V-rel avian reticuloendotheliosis viral oncogene homolog A and B; FoxP3 = Forkhead box P3; CTLA4 = cytotoxic T lymphocyte antigen-4; TGFβ = transforming growth factor beta; BLIMP-1 = PR domain zinc finger protein 1; Bcl-2 and Bcl-XL = B cell lymphoma 2 and XL; Bcl-XL; Bfl-1 = Bcl-2 related protein A1; IL = interleukin; IL-12Rβ2 = IL-12 receptor β2 sub-unit
OX40 Interactions Facilitate Adhesion and Migration
OX40-OX40L interactions facilitate the adhesion of activated T cells to endothelia and their subsequent transmigration. Blockade of OX40L has been demonstrated to reduce T cell adhesion to cultured vascular endothelial cells [38]. In mice with constitutive OX40L expression on dendritic cells, there is greater accumulation of CD4+ T cells in stimulated lymphoid tissue and this has been interpreted as evidence of increased migration, although increased proliferation cannot be excluded [51]. OX40-deficient T cells proliferate faster in vitro than OX40-sufficient T cells but survive less well. OX40-L interactions upregulate a number of molecules implicated in migration: CXCR5, which is associated with trafficking to germinal follicles [18] but also sites on inflammation [77]; CXCR4 [78]; and RANTES/CCL5 [79]. In animals, there is evidence that OX40-deficient T cells may be impaired from reaching sites of inflammation in addition to their reduced effector function [80, 66, 77].
OX40-L Interaction also Promotes Activity of the Cell Expressing OX40L
The effects of OX40L ligation on the expressing cell are less well studied than those of OX40 ligation and are summarized in Fig. 4.

Effects of OX40L ligation on non T cells. In addition to effects on T cells as summarized in Fig. 2, OX40-OX40L ligation has a number of effects on the cell expressing OX40L. These are highlighted in bold by cell type. See text for further details. References: Dendritic cells [170], B cells [171, 172], endothelia [79], mast cells [173]. Ig = immunoglobulin; BSAP = B cell specific activator protein; RANTES/CCL5 = regulated on activation, normal T cell expressed and secreted/chemokine (C-C motif) ligand 5; IL: Interleukin, IgE = immunoglobulin E; TNFα = Tumour necrosis factor alpha
OX40 and OX40 Ligand Aberrations in Transgenic Mice
A key study highlighting OX40-OX40L interactions’ role in autoimmunity was performed in 2002 when Murata and co-workers generated mice transgenic for TNFSF4 with the transgene under the control of the lck promoter [52]. This resulted in the constitutive expression of OX40L on all T cells. Phenotypically, these mice had greatly elevated numbers of CD4+ T cells of which an increased proportion were of a memory phenotype, greatly enlarged lymphoid organs, enhanced antigen-specific T cell responses as measured by proliferation and cytokine production, increased serum antibody concentrations and Th2-type cytokines prior to stimulation and—perhaps most interestingly—multi-lineage infiltrates of both lung and colon; these changes were prevented by the administration of a blocking OX40L antibody. A further interesting observation from the study was that autoimmunity was only induced in C57BL/6 mice and not BALB/c: perhaps related to the former’s greater tendency to produce Th1-type immune responses. Of note, autoimmunity may be similarly induced with constitutive expression of other TNFR ligands such as LIGHT [81].
If OX40L is constitutively expressed on dendritic cells, numbers of CD4+ T cells are increased seen in B-follicles and these cells are of a more activated phenotype after immunization with an antigenic nitrophenol conjugate but not at rest or after lipopolysaccharide alone. In contrast with mice with over-expression of OX40L on T cells, there was no overt autoimmunity [51].
Mice deficient in OX40 were generated in the late 1990s [7, 71]. Such mice breed normally and appear able to generate both IgM and IgG subclass responses to pathogens such as vesicular stomatitis virus and also to haptenized proteins with maintained germinal centre formation. CD8+ cytotoxic lymphocyte responses are maintained, but stimulated CD4+ T cells show reduced proliferation and IFNγ responses to viruses. However, viral response in OX40 deficiency appears variable and numbers of infiltrating cells on bronchoalveolar lavage in response to influenza virus were reduced in OX40-deficient animals [71]. Similarly, the generation of CD4 memory is greatly impaired in OX40 deficiency [49]. Haplosufficiency of OX40 appears sufficient for a phenotypically normal CD4+ response.
Human OX40 Deficiency
A single human with homozygous recessive missense mutations in TNFRSF4 has been reported. She had reduced surface T cell OX40 expression and poor OX40L binding [37]. The patient was identified through exome sequencing of cases of classic Kaposi’s sarcoma (KS): a disease usually confined to the immunosuppressed, especially in conditions where there is CD4+ T cell dysfunction such as HIV/AIDS [82]. This patient’s CD4+ T cells showed minimal OX40 staining after stimulation in contrast to controls. Transfection of Jurkat cells with vectors carrying the mutant gene demonstrated greatly reduced OX40 staining in comparison with control. Phenotypically, there was treatment-responsive visceral leishmaniasis (in which clearance is associated with strong Th1–IFNγ responses [83]), an absence of non-naïve T cells in her peripheral circulation, reduced IFNγ responses after in vitro stimulation of peripheral CD4+ T cells to commonly encountered antigens and preserved proportions of class-switched antibody with reduced numbers of memory B cells. There was no evidence of the infectious diseases usually associated with antibody deficiency or CD4+ T cell deficiency. Also despite evidence of contact with EBV and CMV, she lacked recall responses to these pathogens although also lacked evidence of related disease.
OX40 and OX40L with Relation to Specific Diseases and Disease Models
Polymorphisms in TNFSF4 are Associated with SLE and Systemic Sclerosis with Associations With Sjögren Syndrome and Narcolepsy
An important early study assessing TNFSF4’s link to autoimmunity examined both families and case-controls study in SLE patients from both the USA and UK. OX40L variants were both over- and under-transmitted in SLE [84]. The group went on to demonstrate increased relative OX40L expression in comparison to other markers on stimulation of peripheral blood mononuclear cells and a greater proportion of cells positive for OX40L in those with disease-associated variants.
Genome-wide association studies have confirmed linkage with TNFSF4 polymorphisms in both European [85] and Han Chinese [86] populations. Candidate gene work has confirmed that several European risk variants are also significantly associated with disease amongst Mestizo or mixed heritage European-AmerIndian peoples [87], with the unconfirmed suggestion that OX40L variants may be linked with developing renal manifestations of the disease in Chinese [88]. Multi-population meta-analyses have confirmed linkage of numerous TNFSF4 variants with SLE [89] and have also suggested relative specificity to SLE rather than other autoimmune conditions. The use of fine-mapping of TNFSF4 in SLE and control subjects from multiple ancestries has confirmed that the phenomenon is not a manifestation of linkage disequilibrium and also linked the rs2205960-T variant with specific autoantibodies and lymphopenia [90].
Two separate candidate gene studies have demonstrated associations of polymorphisms with systemic sclerosis [91, 92]. Both protective and at risk variants were identified as well as specific association with limited—rather than diffuse—disease. Later meta-analysis of several large GWAS studies confirmed the association of several TNFSF4 and also identified an association with anti-centromere antibodies [93].
The sleep disorder narcolepsy has been considered autoimmune because of its strong associations with specific HLA variants and that similar disease is induced by serum transfer in animals; autoreactive T cells and autoantibodies are not yet identified. A role for OX40L is suggested in narcolepsy following a significant association with TNFSF4 polymorphism in an ImmunoChip® study involving some 1,886 patients [94]. No studies assessing protein expression or function are yet reported.
A link between variants in TNFSF4 and Sjögren syndrome has been suggested by a candidate gene study in a Scandinavian cohort of 540 patients, but validatory studies are required [95].
OX40 is Expressed at Sites of Autoimmune Inflammation
In autoimmunity, OX40 is typically upregulated at sites of inflammation (summarized in Table 1). Consistent with its known expression pattern, OX40 is identifiable on infiltrating lymphocytes in multi-system diseases such as vasculitis but staining is only seen in affected organs; in non-confluent colitis, staining is only seen in biopsies from affected areas, and in rheumatoid arthritis, OX40 upregulation is particularly pronounced on synovial lymphocytes from inflamed joints [96, 27, 26]. In more localized diseases such as colitis, colonic OX40+ expression is not associated with increased systemic expression as assessed in peripheral blood; in more systemic conditions, there is a typically a peripheral increase (see below).
OX40 is Upregulated on Peripheral Circulating Lymphocytes in Autoimmunity
In systemic diseases, there is commonly an increase in the number of peripheral CD4+ T cells expressing OX40. Consistent with observations from conditions where there is site-specific autoimmunity, in systemic autoimmunity there is often a correlation of expression and disease severity e.g. in SLE [97–103]. Disease-ameliorating interventions can reduce proportions of circulating lymphocytes expressing OX40 such as natalizumab in multiple sclerosis or may correlate with other measures of severity: in myasthenia gravis there is a correlation with acetylcholine receptor antibody titer [104, 105].
Lymphocyte OX40 Expression may Correlate with Pathogenicity in Human Autoimmunity
In an observation that mirrors experimental animal work, OX40 expression on circulating lymphocytes predicts pathogenic antigen specificity in T1DM [106]. Similarly, OX40 and CD25 (IL2Rα) co-expression is strongly predictive of identifying autoreactive T cells in patients with T1DM and also pre-diabetic probands, suggesting a role in disease initiation [30]. The association of OX40 expression with increased lymphocyte activity lends interest to the finding that OX40 mRNA in sorted Treg is reduced in T1DM [107]. By contrast, mRNA for OX40 and TRAF2 were both upregulated in purified CD4+ cells from patients with active SLE [108]. Unfortunately, no protein correlate was examined in either study.
OX40L Expression is Upregulated in a Site-Specific Manner in Autoimmunity
Similar to OX40, OX40L is expressed in a site-specific manner in autoimmune disease (Table 1). This appears to be most marked in autoimmune-mediated inflammation than other causes: for example, it is maximal in immune-mediated nephritides as compared with other etiologies [97].
Systemically, mRNA for OX40L was increased in the serum of SLE patients with concurrent increases in TRAF2 [108]. TRAF2 is activated through ligation of TNF receptors, and OX40 in particular. A correlation between more severe clinical manifestations and serum OX40L mRNA was also demonstrated.
Serum Soluble OX40L
Soluble OX40L is readily assessable in serum by ELISA and elevations that correlate with disease severity have been identified in a number of conditions (Table 1). Some studies may be confounded by the observation that sOX40L tends to increase with age although in active Graves’ thyroiditis at least, there is a correlation in disease state with increased sOX40L expression [48].
Serum Soluble OX40 Alterations Vary Between Autoimmune Diseases
Examination of serum soluble OX40 concentrations in a cohort of unimmunosuppressed Japanese patients with systemic sclerosis revealed significant elevations as compared with both healthy controls and patients with SLE [109]. sOX40 is not however consistently elevated in autoimmunity: the reverse occurs in rheumatoid arthritis [110] and in SLE, there is no difference from controls [109].
OX40-L Blockade has Variable Anti-Inflammatory Effects in Vitro
OX40-L blockade may reduce disease-associated characteristics in leucocyte cultures. Perforin-mediated hemolysis by lymphocytes from SLE patients is reduced by OX40 blockade, alongside NFκB activation and hemolytic activity [111]. Similarly, the prolonged activation and reduced apoptosis seen in T cells isolated from donors with thyroiditis is reversed, an anti-OX40L [112]. Continued OX40 agonism may be necessary to maintain a disease-associated phenotype too: for example, it was necessary to cause proliferation in response to an otherwise sub-mitogenic dose of anti-CD3 on an MBP-reactive cell line derived from EAE [113]. OX40+ cells isolated from a mouse colitis model showed increased IFNγ and TNFα production in culture that was inhibited in vitro with neutralizing OX40L [114]. In partial contrast, a Chinese group has examined PBMCs from a small number of lupus nephritis patients and the effects of an OX40 on them in culture with exogenous IL-2 [103]. Production of IL-4 and IL-10 was reduced but IFNγ increased, suggesting a predominant anti-Th2 effect.
Expression of OX40 is Specific to Sites of Autoimmunity and Correlates with Disease Severity in Animal Models
Consistent with observations in humans, OX40 expression is limited to sites of immune activation in models of autoimmunity. For example, OX40 (and OX40L) mRNA is increased in the spleen, lymph node and nervous tissue of EAE rats with non-significant changes in peripheral blood [115]. T cell OX40 is seen in the thyroids and spleens of mice with thyroiditis [116], the joints of animals with collagen-induced arthritis (CIA) [117], the eyes of mice with intravitreal ovalbumin-induced uveitis [56] and on infiltrating T cells in hapten-induced colitis [80].
Groups examining the effects of other disease-ameliorating interventions have reported a correlation of reduced OX40 expression with lessened severity: in both a CIA model and a human T cell leukaemia virus type I transgenic mouse model, arthritis severity was reduced by interleukin-1 deficient and this correlated with reduced T cell OX40 expression [117]. In IL- receptor antagonist deficient mice, there is IL-17 dependent arthritis: OX40 expression on synovium infiltrating T cells is reduced in ameliorated disease and the IL-17 production induced by stimulation of CD4+ T cells from these mice was markedly enhanced by a stimulatory OX40 antibody in culture [118].
OX40L Expression in Animal Models is Specific to Sites of Autoimmunity
Similar to OX40, OX40L expression is consistent with clinically apparent sites of inflammation: for example, diabetes-prone non-obese diabetic (NOD) mice show OX40L in their pancreases and secondary lymphoid organs [119]; lupus-like nephritis prone BXSB mice express OX40L in renal lesions, which correlate with disease severity [120]; OX40L and OX40 protein expression in homogenized brain correlates with disease severity in EAE [121]; and in CD4 + CD45RB+ transfer colitis, infiltrating lymphocyte in the colon frequently express OX40L [122]. The major source of OX40L expression in EAE is on CD11b + dendritic cells with data on antigen-presenting cells incomplete in other models [123].
A further animal study has considered the role of investigating the relative expression of a number of TNF ligands between MRL/MpJ-lpr/lpr mice, which develop sialadenitis and controls [124]. Although this study demonstrated variable expression of TNFR ligands GITR-L and 41BB-L, OX40L expression did not vary significantly with the degree of inflammation illustrating that OX40L expression is not an inevitably consequence of murine autoimmunity.
The H-24 derivative of the NOD mouse has a tendency to autoimmune thyroiditis exacerbated by iodinated drinking water. Such inflammation is T cell dependent and is likened to Hashimoto’s thyroiditis [116]. Histological scores correlate with thyroid OX40 and OX40L mRNA levels; OX40L positivity is seen on intrathyroid B cells with similar changes in the spleen.
OX40 Expression in Animal Models of Autoimmunity Correlates with an Early Initiating Event
Rats treated with Mycobacterium tuberculosis and adjuvant predictably develop polyarthritis. In this model, OX40 expression is increased in the draining lymph nodes of inflamed joints and expression increases before clinical signs appear [125]. In rat EAE, there was analogous early OX40 activation on antigen-specific lymphocytes before the onset of clinical signs [126].
OX40 Appears to Identify Activated, Antigen-Specific Cells
Variations on the EAE model provided further insights into the role of OX40/OX40L interactions. Recently activated T cells autoreactive to components of nervous tissues are OX40+ in the irises of EAE rats [127]. Expression of OX40 appears to define cells that are reactive to the myelin basic protein antigen used to induced EAE [128], as above, cells specific to listeria expressing a particular peptide are OX40-positive [29] and OX40-positive circulating T cells precede diabetes onset in NOD mice [119].
OX40 and OX40L Ameliorate Autoimmunity in Vivo
OX40L blockade in vivo generally ameliorates autoimmunity, with strong experimental support for efficacy in most major disease models (summarized in Table 2). Two studies have however shown the reverse: in mice given sheep anti-glomerular basement membrane antibodies, the resultant nephritis is exacerbated by blocking OX40L antibody with increased IFNγ + T cell infiltration [129]. A second study reported in abstract form only reports exacerbation of EAU with OX40L blockade, although this is in contrast to other EAU and EAE studies [130–133].
The effect of OX40L blockade may be time-dependent. Using the NOD mouse, Pakala and colleagues showed that OX40 is expressed on circulating CD4+ T cells prior to the onset of overt diabetes and that OX40L is expressed in both secondary lymphoid tissue and the pancreas [119]. Intriguingly, the group demonstrated a reduction in the incidence of diabetes in their study population when blocking antibody to OX40L was given at 12 weeks from birth but not earlier or later; this contrasts with results showing that CD28 blockade prevents diabetes in a window up to 4 weeks and is complementary to the sequential checkpoint theory of autoimmunity proposed by Croft [134]. Similar data are lacking for OX40 blockade.
The effects of OX40-L blockade in ameliorating autoimmunity include preventing proliferation of active CD4+ T cells, altering cytokine production, preventing migration and affecting T cell polarization. In mice with dextran sulfate sodium-induced enteritis, OX40-IgG fusion protein reduces histological severity and reduces the production of T-bet mRNA, suggesting reduced Th1 polarization [77]. Disease amelioration appeared to be partly IL-10 mediated: IL-10 was increased by agonistic OX40 IgG and IL-10 blocking antibodies reduced OX40-IgG efficacy. After OX40-IgG administration, lymphocyte infiltration reduced. CXCR5 was less expressed, suggesting one possible mechanism. In transfer colitis, OX40-deficient T cells are unable to reach the colon [66]. A third colitis model has confirmed reduction in Th1 type cytokines with OX40 blockade [80], a similar picture is seen in inflammatory arthritis [123] and in EAE IL-2 and IL-6 [131]: all had reduced severity of tissue T cell infiltrate.
OX40L Blockade May Have More Potent Effects Than OX40 Blockade
Although OX40 is the only known receptor for OX40L, and OX40L is OX40’s only known natural ligand, there appears to be an increased effect of preventing OX40L signaling as compared with stopping OX40 signaling or anti T cell therapy. In CIA, an OX40-blocking FAb fragment which prevented reverse signaling was equaled in efficacy by an OX40L fusion protein previously shown to block OX40L but signal through OX40 [135]. Supporting this argument is the finding that in mice deficient in Treg, the resulting multi-system autoimmunity is more significantly attenuated by OX40 blockade or deficiency than CD4+ and/or CD8+ deficiency [136, 137]. Such findings may offer an alternative explanation for studies where apparent OX40 agonists have ameliorated autoimmune disease.
OX40 May Be Used to Target Depletion of Autoreactive T Cells
Two groups have demonstrated successfully used OX40 to target autoreactive cells. OX40 is a viable target for the delivery of liposomal drug 5′-fluoro-2′-deoxyuridine dipalmitate (a cytostatic agent), reducing proliferation in vitro and the severity of adjuvant-induced arthritis in vivo [125]. Similarly, a depleting immunotoxin specific to OX40 was able to ameliorate disease in a rat EAE model [28].
The Effects of OX40 Agonism Vary with Timing in Relation to Antigen Exposure and Inflammatory Milieu
An interesting and clinically relevant feature of OX40 stimulation has become apparent through work on EAE. Having confirmed others’ work that OX40 stimulation antagonized the Treg generation in TGFβ-treated culture, Weinberg et al. showed that blocking IL-4, IL-6 and IFNγ caused OX40 agonism to have a reverse effect and promote the generation of Treg. This was then translated to the EAE model: OX40 agonism during induction ameliorated disease; OX40 agonism after onset worsened disease [60]. Similar effects are reported in models of diabetes: in NOD mice immunized with intranasal insulin, agonistic anti-OX40 reduced the incidence of diabetes when given at immunization [138]. OX40 administration appeared to augment specific Treg numbers. These Treg populations appeared to mediate tolerance: SCID mice crossed onto the NOD background were protected when there was co-transfer of CD4+ cells from αOX40-treated mice. Further evidence of OX40 agonism enhancing the effects of the cytokine milieu include experiments that have shown promotion of a Th1, Th2 [33, 46], Th9 [55] or Th17 [56] type response depending on the microenvironment concerned.
The same group demonstrated that OX40 expression identified encephalitogenic autoreactive T cells [113] and transfer of these cells caused EAE after culture with stimulating OX40 but not without: suggesting that continued OX40 signaling was necessary for maintenance of pathogenic potential [113].
In contrast, in a model of intravitreal ovalbumin-induced uveitis in mice with ovalbumin-specific T cells, OX40 stimulating antibody worsened inflammation and augmented production of Th17 cytokines [56]. In interpreting this difference, it should be remembered that antigen-specific effector T cells were pre-formed not generated at the point of immunization. However in uveitis induced by injection of a photoreceptor protein peptide, agonistic OX40 ligation at immunization or afterwards worsened clinical scores and prolonged duration of inflammation [139]. There were increases in numbers of IFNγ and IL-17 positive effector CD4+ T cells and the quantity of IFNγ produced by cultures of splenocytes with retinal antigen was also increased. Thus, timing of OX40 agonism is critical in determining response.
There Is Redundancy in OX40 Co-Stimulatory Signaling
The EAE model has also highlighted OX40/L interaction’s auxiliary role in co-stimulation. The major, and constitutively expressed, T cell co-stimulatory molecule is CD28. In CD28-deficient mice, EAE manifests at reduced severity. However, when OX40L blocking antibody was co-administered, EAE could not be induced [140]. Similarly, in Treg-deficiency multi-system autoimmunity, combination blockade of OX40 and CD30 is sufficient to correct an otherwise lethal effector T cell driven phenotype; either alone prolongs life by weeks [136]. There was an additive effect of anti-OX40L and CTLA-4 Ig co-administration in ameliorating disease in a different EAE study [141].
OX40 is Necessary for Regulatory and Effector T cell Function and Migration
By transferring allotype marked Treg in colitis, it has been demonstrated that Tregs lacking OX40 are less able to localize to the gut than their intact counterparts. Importantly, these are then unable to control transfer colitis; co-transfer of intact Tregs reduces weight loss, histological scores, T cells gut infiltration, and cytokine levels but these improvements are not seen with OX40-deficient T cells despite normal in vitro proliferation. Intriguingly, OX40 on transferred effector cells was also a requirement for the development of colitis, highlighting its importance in both arms of the T cell response [66].
Conclusion
OX40 is predominantly expressed on activated T cells, and its cognate ligand OX40L is expressed on activated antigen-presenting cells, but also activated T cells, some endothelia and mast T cells. Their interaction serves to increase the proliferation and longevity of effector T cells, increase production of effector cytokines, (usually) suppress regulatory function, preserve cellular memory and facilitate migration. There is evidence for increased expression and signaling through the OX40-OX40L receptor-ligand pair in a wide variety of human autoimmune diseases and in several this correlates with established measures of disease severity.
In the majority of animal models of autoimmunity, OX40-OX40L inhibition ameliorates disease; OX40 agonism appears to be more time-specific with increased autoimmunity in some instances and amelioration in others. This difference may be due to differential expansion of regulatory or effector compartments, different cytokine milieu or variable blockade of reverse OX40L signaling.
OX40-OX40L inhibition is therefore a logical approach for the targeted treatment of human autoimmune disease (summarized in Box 1). Some recent work suggests that OX40L blockade may be more effective than OX40, but this requires further exploration. Questions regarding optimal timing of administration, off-target effects, the need for concurrent blockade of other co-stimulatory molecules and the possibility of malignant or infective complications with longer term use all warrant consideration when considering further trials (see also Box 2).
Box 1: Rationale for Targeting OX40-OX40L Interactions in Autoimmunity
-
OX40-OX40 ligand interactions form part of pathogenic pathway in a number of human diseases and animal models. Thus, whether aberrations in such interactions form part of etiopathogenesis of autoimmunity themselves as in constitutively OX40L expressing mice or whether they are resultant on other pathways, preventing their activation may ameliorate disease [52].
-
As identified above, in certain models the effect of OX40L blockade is superior to T cell specific therapies alone [136, 135]
-
A lack of severe side effects in the animal studies reported above and the long-term relative health of OX40-deficient mice and the single OX40-deficient human—with the caveat of HHV8 infection—suggest a low side effect burden [37, 71]. The one trial of humanized anti-OX40L did not cause significant side effects [142].
-
OX40-L should provide targeting to areas of immune activity. Expression is largely confined to activated cells and especially autoantigen-specific cells [28, 29]. Such site-specificity has been demonstrated clinically by OX40 upregulation on the T cells of inflamed tissue but not peripheral blood in human colitis and in rheumatoid arthritis [112, 26].
-
An ideal therapy in autoimmunity is the re-establishment of immune tolerance. The observation that activation through OX40L may render T cells resistance to regulatory signals makes this a logical target [10, 112]. Further, in systems such as CD40L-deficient islet cell allograft recipients, OX40 agonism or blockade alone is enough to determine graft tolerance [143].
-
Migration of activated T cells across endothelia appears to be at least partly dependent on OX40-OX40L [38, 144]. This observation, coupled with apparent selective tissue expression in certain autoimmune disease states (e.g. [97]) suggests that inhibition of the interaction might reduce migration into inflamed areas. Work in EAE mice suggests that pathogenic T cells persist after OX40 blockade, but do not migrate to target sites [132].
-
OX40-L blockade appears effective after disease onset—e.g. in a diabetes model [119]. Although several animal studies have demonstrated that OX40-L inhibition may ameliorate autoimmunity, many have used OX40/L blockade at, or before, disease onset: something that differs from the clinical situation in which a patient will present for treatment after symptom onset.
-
Topical therapy is feasible and effective in mouse models e.g. OX40-agonists intra-tumour [64] or intravitreal OX40L blockade in a uveitis model [56].
Box 2: Potential Problems with Human OX40-OX40L Therapy
-
The optimal timing of OX40 blockade remains unclear: it is proposed that OX40-L interaction is one a series of time-dependent checkpoints in the activation of CD4+ T cells [134]. In animal models of autoimmunity, timing of administration of OX40-L blockade can be critical and determine success [119].
-
Agonism of OX40 can both ameliorate or exacerbate autoimmunity in animal models, and timing of administration can determine its effect [60, 138]. Whilst such timing is feasible in animal models, it is difficult to see its translation into human therapy; further, in contrast to mice, human Treg do not express OX40 at rest and it is therefore possible that a tolerogenic effect might not be seen at all.
-
OX40-L interactions represent but one of many co-stimulatory processes between T cells and antigen-presenting cells. In some animal models multiple blockade is required for a full protective effect e.g. OX40 and CD28 [140, 129] or OX40 and CD30 [136]. Whether multiple blockades would be required in human work remains uncertain but may underlie the failure of an anti-OX40L trial in asthma [142].
-
Host responses may develop against therapeutic antibodies, especially given a tendency to autoimmunity. Such problems have been reported in the development of agonistic OX40L fusion protein [145]. However, such antibodies were not generated in a trial of OX40L blockade [142]. Alternative approaches include small molecules [146] or targeting cytotoxic drugs through OX40 [125, 28].
-
Few studies have addressed the effects of OX40-L blockade withdrawal. A typical response would be for recurrence of the suppressed response: in one study that used OX40 blockade to prevent skin allograft rejection, graft loss occurred weeks after cessation [74]. Details are lacking in autoimmunity.
-
Recipients of OX40 blockade may become vulnerable to infection or malignancy. The recurrent Kaposi’s sarcoma and visceral leishmaniasis manifest in human OX40 deficiency are concerning [37]. However, in OX40L deficient mice, there is no increased susceptibility to Leishmania [147], no overt susceptibility to infection is seen in OX40-deficient mice [71], and infective complications were not reported in human OX40L blockade [142].
-
The typical net effect of OX40-L blockade is in a reducing T cell-mediated effector function, however there is a possibility of losing tolerance or exacerbating disease. In T cell transfer colitis, only intact, but not OX40-deficient, Treg cells could control inflammation [66]. Examples of unexpected disease exacerbation include in murine anti-GBM nephritis [129] and murine experimental autoimmune uveoretinitis [130].
-
Differences in OX40 expression between mouse and humans warrant caution in translating therapy. Expression of OX40 is constitutive on some populations of Treg in mice but is only induced in humans [8]. ‘Wildtype’ humans are also likely to be significantly more antigen-experienced than laboratory mice. Differences in prior antigen exposure were thought to have been behind the lethal idiosyncratic reactions that resulted in deaths in early human trials of the CD28 super-agonist TGN1412, though analogous problems are yet reported with OX40 agonists [148, 149].
-
The various genetics studies detailed above regarding TNFSF4 variants in SLE, and associated variable OX40L expression make variable responses to blockade likely, especially between different ethnic groups [84].
-
The full spectrum of functions of OX40-OX40L interactions is incompletely understood. Whilst of the molecules is not required for life, off-target effects of their blockade must be considered outside of known effects on atherosclerosis [150]. For example, OX40 blockade in CIA revealed reductions in osteoclastogenesis and that OX40L deficient mice have thinner, shorter bones than intact controls [135].
References
Davidson A, Diamond B (2001) Autoimmune diseases. N Engl J Med 345(5):340–350. doi:10.1056/NEJM200108023450506
Lleo A, Invernizzi P, Gao B, Podda M, Gershwin ME (2010) Definition of human autoimmunity — autoantibodies versus autoimmune disease. Autoimmun Rev 9(5):A259–A266. doi:10.1016/j.autrev.2009.12.002
Cooper GS, Stroehla BC (2003) The epidemiology of autoimmune diseases. Autoimmun Rev 2(3):119–125
Paterson DJ, Jefferies WA, Green JR, Brandon MR, Corthesy P, Puklavec M, Williams AF (1987) Antigens of activated rat T lymphocytes including a molecule of 50,000 Mr detected only on CD4 positive T blasts. Mol Immunol 24(12):1281–1290
Mallett S, Fossum S, Barclay AN (1990) Characterization of the MRC OX40 antigen of activated CD4 positive T lymphocytes--a molecule related to nerve growth factor receptor. EMBO J 9(4):1063–1068
Godfrey WR, Fagnoni FF, Harara MA, Buck D, Engleman EG (1994) Identification of a human OX-40 ligand, a costimulator of CD4+ T cells with homology to tumor necrosis factor. J Exp Med 180(2):757–762
Pippig SD, Pena-Rossi C, Long J, Godfrey WR, Fowell DJ, Reiner SL, Birkeland ML, Locksley RM, Barclay AN, Killeen N (1999) Robust B cell immunity but impaired T cell proliferation in the absence of CD134 (OX40). J Immunol 163(12):6520–6529
Croft M, So T, Duan W, Soroosh P (2009) The significance of OX40 and OX40L to T-cell biology and immune disease. Immunol Rev 229(1):173–191. doi:10.1111/j.1600-065X.2009.00766.x
Lane PJL, McConnell FM, Anderson G, Nawaf MG, Gaspal FM, Withers DR (2014) Evolving strategies for cancer and autoimmunity: back to the future. Front Immunol 5:154. doi:10.3389/fimmu.2014.00154
Takeda I, Ine S, Killeen N, Ndhlovu LC, Murata K, Satomi S, Sugamura K, Ishii N (2004) Distinct roles for the OX40-OX40 ligand interaction in regulatory and nonregulatory T cells. J Immunol 172(6):3580–3589
So T, Lee SW, Croft M (2008) Immune regulation and control of regulatory T cells by OX40 and 4-1BB. Cytokine Growth Factor Rev 19(3–4):253–262. doi:10.1016/j.cytogfr.2008.04.003
Calderhead DM, Buhlmann JE, van den Eertwegh AJ, Claassen E, Noelle RJ, Fell HP (1993) Cloning of mouse Ox40: a T cell activation marker that may mediate T-B cell interactions. J Immunol 151(10):5261–5271
Munks MW, Mourich DV, Mittler RS, Weinberg AD, Hill AB (2004) 4-1BB and OX40 stimulation enhance CD8 and CD4 T-cell responses to a DNA prime, poxvirus boost vaccine. Immunology 112(4):559–566. doi:10.1111/j.1365-2567.2004.01917.x
Klinger M, Kim JK, Chmura SA, Barczak A, Erle DJ, Killeen N (2009) Thymic OX40 expression discriminates cells undergoing strong responses to selection ligands. J Immunol 182(8):4581–4589. doi:10.4049/jimmunol.0900010
Zaini J, Andarini S, Tahara M, Saijo Y, Ishii N, Kawakami K, Taniguchi M, Sugamura K, Nukiwa T, Kikuchi T (2007) OX40 ligand expressed by DCs costimulates NKT and CD4+ Th cell antitumor immunity in mice. J Clin Invest 117(11):3330–3338. doi:10.1172/jci32693
Melero I, Hirschhorn-Cymerman D, Morales-Kastresana A, Sanmamed MF, Wolchok JD (2013) Agonist antibodies to TNFR molecules that costimulate T and NK cells. Clin Cancer Res: Off J Am AssocCancer Res 19(5):1044–1053. doi:10.1158/1078-0432.ccr-12-2065
Baumann R, Yousefi S, Simon D, Russmann S, Mueller C, Simon HU (2004) Functional expression of CD134 by neutrophils. Eur J Immunol 34(8):2268–2275. doi:10.1002/eji.200424863
Walker LS, Gulbranson-Judge A, Flynn S, Brocker T, Raykundalia C, Goodall M, Forster R, Lipp M, Lane P (1999) Compromised OX40 function in CD28-deficient mice is linked with failure to develop CXC Chemokine receptor 5-positive CD4 cells and germinal centers. J Exp Med 190(8):1115–1122
Rogers PR, Song J, Gramaglia I, Killeen N, Croft M (2001) OX40 promotes Bcl-xL and Bcl-2 expression and is essential for long-term survival of CD4 T cells. Immunity 15(3):445–455
Croft M (2010) Control of immunity by the TNFR-related molecule OX40 (CD134). Annu Rev Immunol 28:57–78. doi:10.1146/annurev-immunol-030409-101243
Redmond WL, Weinberg A (2008) Novel regulation of CD8 T cell-specific OX40 expression via an IL-2 and JAK3-dependent mechanism. FASEB J 22(1076):21
Vogel KU, Edelmann SL, Jeltsch KM, Bertossi A, Heger K, Heinz GA, Zoller J, Warth SC, Hoefig KP, Lohs C, Neff F, Kremmer E, Schick J, Repsilber D, Geerlof A, Blum H, Wurst W, Heikenwalder M, Schmidt-Supprian M, Heissmeyer V (2013) Roquin paralogs 1 and 2 redundantly repress the icos and Ox40 costimulator mRNAs and control follicular helper T cell differentiation. Immunity 38(4):655–668. doi:10.1016/j.immuni.2012.12.004
Gramaglia I, Weinberg AD, Lemon M, Croft M (1998) Ox-40 ligand: a potent costimulatory molecule for sustaining primary CD4 T cell responses. J Immunol 161(12):6510–6517
Sadler R, Bateman EA, Heath V, Patel SY, Schwingshackl PP, Cullinane AC, Ayers L, Ferry BL (2014) Establishment of a healthy human range for the whole blood “OX40” assay for the detection of antigen-specific CD4+ T cells by flow cytometry. Cytometry B Clin Cytom 86(5):350–361. doi:10.1002/cyto.b.21165
Tone Y, Kojima Y, Furuuchi K, Brady M, Yashiro-Ohtani Y, Tykocinski ML, Tone M (2007) OX40 gene expression is up-regulated by chromatin remodeling in its promoter region containing Sp1/Sp3, YY1, and NF-kappa B binding sites. J Immunol 179(3):1760–1767
Giacomelli R, Passacantando A, Perricone R, Parzanese I, Rascente M, Minisola G, Tonietti G (2001) T lymphocytes in the synovial fluid of patients with active rheumatoid arthritis display CD134-OX40 surface antigen. Clin Exp Rheumatol 19(3):317–320
Stuber E, Buschenfeld A, Luttges J, Von Freier A, Arendt T, Folsch UR (2000) The expression of OX40 in immunologically mediated diseases of the gastrointestinal tract (celiac disease, Crohn’s disease, ulcerative colitis). Eur J Clin Investig 30(7):594–599
Weinberg AD, Bourdette DN, Sullivan TJ, Lemon M, Wallin JJ, Maziarz R, Davey M, Palida F, Godfrey W, Engleman E, Fulton RJ, Offner H, Vandenbark AA (1996) Selective depletion of myelin-reactive T cells with the anti-OX-40 antibody ameliorates autoimmune encephalomyelitis. Nat Med 2(2):183–189
Marriott CL, Mackley EC, Ferreira C, Veldhoen M, Yagita H, Withers DR (2014) OX40 controls effector CD4(+) T-cell expansion, not follicular T helper cell generation in acute Listeria infection. Eur J Immunol 44(8):2437–2447. doi:10.1002/eji.201344211
Endl J, Rosinger S, Schwarz B, Friedrich SO, Rothe G, Karges W, Schlosser M, Eiermann T, Schendel DJ, Boehm BO (2006) Coexpression of CD25 and OX40 (CD134) receptors delineates autoreactive T-cells in type 1 diabetes. Diabetes 55(1):50–60
Linton PJ, Bautista B, Biederman E, Bradley ES, Harbertson J, Kondrack RM, Padrick RC, Bradley LM (2003) Costimulation via OX40L expressed by B cells is sufficient to determine the extent of primary CD4 cell expansion and Th2 cytokine secretion in vivo. J Exp Med 197(7):875–883. doi:10.1084/jem.20021290
Karulf M, Kelly A, Weinberg AD, Gold JA (2010) OX40 ligand regulates inflammation and mortality in the innate immune response to sepsis. J Immunol 185(8):4856–4862. doi:10.4049/jimmunol.1000404
Jenkins SJ, Perona-Wright G, Worsley AG, Ishii N, MacDonald AS (2007) Dendritic cell expression of OX40 ligand acts as a costimulatory, not polarizing, signal for optimal Th2 priming and memory induction in vivo. J Immunol 179(6):3515–3523
Kashiwakura J, Yokoi H, Saito H, Okayama Y (2004) T cell proliferation by direct cross-talk between OX40 ligand on human mast cells and OX40 on human T cells: comparison of gene expression profiles between human tonsillar and lung-cultured mast cells. J Immunol 173(8):5247–5257
Nakae S, Suto H, Iikura M, Kakurai M, Sedgwick JD, Tsai M, Galli SJ (2006) Mast cells enhance T cell activation: importance of mast cell costimulatory molecules and secreted TNF. J Immunol 176(4):2238–2248
Krimmer DI, Loseli M, Hughes JM, Oliver BG, Moir LM, Hunt NH, Black JL, Burgess JK (2009) CD40 and OX40 ligand are differentially regulated on asthmatic airway smooth muscle. Allergy 64(7):1074–1082. doi:10.1111/j.1398-9995.2009.01959.x
Byun M, Ma CS, Akcay A, Pedergnana V, Palendira U, Myoung J, Avery DT, Liu Y, Abhyankar A, Lorenzo L, Schmidt M, Lim HK, Cassar O, Migaud M, Rozenberg F, Canpolat N, Aydogan G, Fleckenstein B, Bustamante J, Picard C, Gessain A, Jouanguy E, Cesarman E, Olivier M, Gros P, Abel L, Croft M, Tangye SG, Casanova JL (2013) Inherited human OX40 deficiency underlying classic Kaposi sarcoma of childhood. J Exp Med 210(9):1743–1759. doi:10.1084/jem.20130592
Imura A, Hori T, Imada K, Ishikawa T, Tanaka Y, Maeda M, Imamura S, Uchiyama T (1996) The human OX40/gp34 system directly mediates adhesion of activated T cells to vascular endothelial cells. J Exp Med 183(5):2185–2195
Sato T, Ishii N, Murata K, Kikuchi K, Nakagawa S, Ndhlovu LC, Sugamura K (2002) Consequences of OX40-OX40 ligand interactions in Langerhans cell function: enhanced contact hypersensitivity responses in OX40L-transgenic mice. Eur J Immunol 32(11):3326–3335. doi:10.1002/1521-4141(200211)32:11<3326::aid-immu3326>3.0.co;2[-‐]9
Kim MY, Toellner K-M, White A, McConnell FM, Gaspal FMC, Parnell SM, Jenkinson E, Anderson G, Lane PJL (2006) Neonatal and adult CD4+ CD3- cells share similar gene expression profile, and neonatal cells up-regulate OX40 ligand in response to TL1A (TNFSF15). J Immunol 177(5):3074–3081
Soroosh P, Ine S, Sugamura K, Ishii N (2006) OX40-OX40 ligand interaction through T cell-T cell contact contributes to CD4 T cell longevity. J Immunol 176(10):5975–5987
Mendel I, Shevach EM (2006) Activated T cells express the OX40 ligand: requirements for induction and costimulatory function. Immunology 117(2):196–204. doi:10.1111/j.1365-2567.2005.02279.x
Wang Y, Li M, Song M, Xu X, Xiong J, Yang X, Tan J, Bai Y (2008) Expression of OX40 ligand in microglia activated by IFN-gamma sustains a protective CD4+ T-cell response in vitro. Cell Immunol 251(2):86–92. doi:10.1016/j.cellimm.2008.04.002
Kurche JS, Haluszczak C, McWilliams JA, Sanchez PJ, Kedl RM (2012) Type I IFN-dependent T cell activation is mediated by IFN-dependent dendritic cell OX40 ligand expression and is independent of T cell IFNR expression. J Immunol 188(2):585–593. doi:10.4049/jimmunol.1102550
Krause P, Bruckner M, Uermosi C, Singer E, Groettrup M, Legler DF (2009) Prostaglandin E2 enhances T-cell proliferation by inducing the costimulatory molecules OX40L, CD70, and 4-1BBL on dendritic cells. Blood 113(11):2451–2460. doi:10.1182/blood-2008-05-157123
Ito T, Wang YH, Duramad O, Hori T, Delespesse GJ, Watanabe N, Qin FX, Yao Z, Cao W, Liu YJ (2005) TSLP-activated dendritic cells induce an inflammatory T helper type 2 cell response through OX40 ligand. J Exp Med 202(9):1213–1223. doi:10.1084/jem.20051135
Maxwell JR, Yadav R, Rossi RJ, Ruby CE, Weinberg AD, Aguila HL, Vella AT (2006) IL-18 bridges innate and adaptive immunity through IFN-gamma and the CD134 pathway. J Immunol 177(1):234–245
Wang Q, Chen Y, Xie F, Ge Y, Chen L, Wu H, Qu Q, Wang X, Zhang X (2006) Development of a sandwich ELISA for evaluating soluble OX40L (CD252) in human sera of different ages or with Graves’ disease. Cytokine 36(1–2):23–28. doi:10.1016/j.cyto.2006.10.006
Gramaglia I, Jember A, Pippig SD, Weinberg AD, Killeen N, Croft M (2000) The OX40 costimulatory receptor determines the development of CD4 memory by regulating primary clonal expansion. J Immunol 165(6):3043–3050
Maxwell JR, Weinberg A, Prell RA, Vella AT (2000) Danger and OX40 receptor signaling synergize to enhance memory T cell survival by inhibiting peripheral deletion. J Immunol 164(1):107–112
Brocker T, Gulbranson-Judge A, Flynn S, Riedinger M, Raykundalia C, Lane P (1999) CD4 T cell traffic control: in vivo evidence that ligation of OX40 on CD4 T cells by OX40-ligand expressed on dendritic cells leads to the accumulation of CD4 T cells in B follicles. Eur J Immunol 29(5):1610–1616. doi:10.1002/(sici)1521-4141(199905)29:05<1610::aid-immu1610>3.0.co;2[-‐]8
Murata K, Nose M, Ndhlovu LC, Sato T, Sugamura K, Ishii N (2002) Constitutive OX40/OX40 ligand interaction induces autoimmune-like diseases. J Immunol 169(8):4628–4636
Dannull J, Nair S, Su Z, Boczkowski D, DeBeck C, Yang B, Gilboa E, Vieweg J (2005) Enhancing the immunostimulatory function of dendritic cells by transfection with mRNA encoding OX40 ligand. Blood 105(8):3206–3213. doi:10.1182/blood-2004-10-3944
Mestas J, Crampton SP, Hori T, Hughes CC (2005) Endothelial cell co-stimulation through OX40 augments and prolongs T cell cytokine synthesis by stabilization of cytokine mRNA. Int Immunol 17(6):737–747. doi:10.1093/intimm/dxh255
Xiao X, Balasubramanian S, Liu W, Chu X, Wang H, Taparowsky EJ, Fu YX, Choi Y, Walsh MC, Li XC (2012) OX40 signaling favors the induction of T(H)9 cells and airway inflammation. Nat Immunol 13(10):981–990. doi:10.1038/ni.2390
Zhang Z, Zhong W, Hinrichs D, Wu X, Weinberg A, Hall M, Spencer D, Wegmann K, Rosenbaum JT (2010) Activation of OX40 augments Th17 cytokine expression and antigen-specific uveitis. AM J Pathol 177(6):2912–2920. doi:10.2353/ajpath.2010.100353
Ohshima Y, Yang LP, Uchiyama T, Tanaka Y, Baum P, Sergerie M, Hermann P, Delespesse G (1998) OX40 costimulation enhances interleukin-4 (IL-4) expression at priming and promotes the differentiation of naive human CD4(+) T cells into high IL-4-producing effectors. Blood 92(9):3338–3345
Bansal-Pakala P, Jember AG, Croft M (2001) Signaling through OX40 (CD134) breaks peripheral T-cell tolerance. Nat Med 7(8):907–912. doi:10.1038/90942
Mahmud SA, Manlove LS, Schmitz HM, Xing Y, Wang Y, Owen DL, Schenkel JM, Boomer JS, Green JM, Yagita H, Chi H, Hogquist KA, Farrar MA (2014) Costimulation via the tumor-necrosis factor receptor superfamily couples TCR signal strength to the thymic differentiation of regulatory T cells. Nat Immunol 15(5):473–481. doi:10.1038/ni.2849
Ruby CE, Yates MA, Hirschhorn-Cymerman D, Chlebeck P, Wolchok JD, Houghton AN, Offner H, Weinberg AD (2009) Cutting Edge: OX40 agonists can drive regulatory T cell expansion if the cytokine milieu is right. J Immunol 183(8):4853–4857. doi:10.4049/jimmunol.0901112
Xiao X, Gong W, Demirci G, Liu W, Spoerl S, Chu X, Bishop DK, Turka LA, Li XC (2012) New insights on OX40 in the control of T cell immunity and immune tolerance in vivo. J Immunol 188(2):892–901. doi:10.4049/jimmunol.1101373
So T, Croft M (2007) Cutting edge: OX40 inhibits TGF-beta- and antigen-driven conversion of naive CD4 T cells into CD25 + Foxp3+ T cells. J Immunol 179(3):1427–1430
Voo KS, Bover L, Harline ML, Vien LT, Facchinetti V, Arima K, Kwak LW, Liu YJ (2013) Antibodies targeting human OX40 expand effector T cells and block inducible and natural regulatory T cell function. J Immunol 191(7):3641–3650. doi:10.4049/jimmunol.1202752
Piconese S, Valzasina B, Colombo MP (2008) OX40 triggering blocks suppression by regulatory T cells and facilitates tumor rejection. J Exp Med 205(4):825–839. doi:10.1084/jem.20071341
Ito T, Wang YH, Duramad O, Hanabuchi S, Perng OA, Gilliet M, Qin FX, Liu YJ (2006) OX40 ligand shuts down IL-10-producing regulatory T cells. Proc Natl Acad Sci U S A 103(35):13138–13143. doi:10.1073/pnas.0603107103
Griseri T, Asquith M, Thompson C, Powrie F (2010) OX40 is required for regulatory T cell-mediated control of colitis. J Exp Med 207(4):699–709. doi:10.1084/jem.20091618
Vu MD, Xiao X, Gao W, Degauque N, Chen M, Kroemer A, Killeen N, Ishii N, Li XC (2007) OX40 costimulation turns off Foxp3+ Tregs. Blood 110(7):2501–2510. doi:10.1182/blood-2007-01-070748
Prell RA, Evans DE, Thalhofer C, Shi T, Funatake C, Weinberg AD (2003) OX40-mediated memory T cell generation is TNF receptor-associated factor 2 dependent. J Immunol 171(11):5997–6005
Vu MD, Clarkson MR, Yagita H, Turka LA, Sayegh MH, Li XC (2006) Critical, but conditional, role of OX40 in memory T cell-mediated rejection. J Immunol 176(3):1394–1401
Soroosh P, Ine S, Sugamura K, Ishii N (2007) Differential requirements for OX40 signals on generation of effector and central memory CD4+ T cells. J Immunol 179(8):5014–5023
Kopf M, Ruedl C, Schmitz N, Gallimore A, Lefrang K, Ecabert B, Odermatt B, Bachmann MF (1999) OX40-deficient mice are defective in Th cell proliferation but are competent in generating B cell and CTL Responses after virus infection. Immunity 11(6):699–708
Bansal-Pakala P, Halteman BS, Cheng MH, Croft M (2004) Costimulation of CD8 T cell responses by OX40. J Immunol 172(8):4821–4825
Salek-Ardakani S, Moutaftsi M, Crotty S, Sette A, Croft M (2008) OX40 drives protective vaccinia virus-specific CD8 T cells. J Immunol 181(11):7969–7976
Kinnear G, Wood KJ, Marshall D, Jones ND (2010) Anti-OX40 prevents effector T-cell accumulation and CD8+ T-cell mediated skin allograft rejection. Transplantation 90(12):1265–1271. doi:10.1097/TP.0b013e3181fe5396
Moran AE, Kovacsovics-Bankowski M, Weinberg AD (2013) The TNFRs OX40, 4-1BB, and CD40 as targets for cancer immunotherapy. Curr Opin Immunol 25(2):230–237. doi:10.1016/j.coi.2013.01.004
Buchan SL, Manzo T, Flutter B, Rogel A, Edwards N, Zhang L, Sivakumaran S, Ghorashian S, Carpenter B, Bennett CL, Freeman GJ, Sykes M, Croft M, Al-Shamkhani A, Chakraverty R (2014) OX40- and CD27-mediated costimulation synergizes with anti-PD-L1 blockade by forcing exhausted CD8+ T cells to exit quiescence. J Immunol 194(1):125–133. doi:10.4049/jimmunol.1401644
Obermeier F, Schwarz H, Dunger N, Strauch UG, Grunwald N, Scholmerich J, Falk W (2003) OX40/OX40L interaction induces the expression of CXCR5 and contributes to chronic colitis induced by dextran sulfate sodium in mice. Eur J Immunol 33(12):3265–3274. doi:10.1002/eji.200324124
Jourdan P, Vendrell JP, Huguet MF, Segondy M, Bousquet J, Pene J, Yssel H (2000) Cytokines and cell surface molecules independently induce CXCR4 expression on CD4+ CCR7+ human memory T cells. J Immunol 165(2):716–724
Kotani A, Hori T, Matsumura Y, Uchiyama T (2002) Signaling of gp34 (OX40 ligand) induces vascular endothelial cells to produce a CC Chemokine RANTES/CCL5. Immunol Lett 84(1):1–7
Higgins LM, McDonald SA, Whittle N, Crockett N, Shields JG, MacDonald TT (1999) Regulation of T cell activation in vitro and in vivo by targeting the OX40-OX40 ligand interaction: amelioration of ongoing inflammatory bowel disease with an OX40-IgG fusion protein, but not with an OX40 ligand-IgG fusion protein. J Immunol 162(1):486–493
Shaikh RB, Santee S, Granger SW, Butrovich K, Cheung T, Kronenberg M, Cheroutre H, Ware CF (2001) Constitutive expression of LIGHT on T cells leads to lymphocyte activation, inflammation, and tissue destruction. J Immunol 167(11):6330–6337. doi:10.4049/jimmunol.167.11.6330
Robey RC, Mletzko S, Gotch FM (2010) The T-cell immune response against Kaposi’s sarcoma-associated herpesvirus. Adv Virol 2010(5):1–9. doi:10.1016/S1286-4579(99)80036-7
Castellano LR, Filho DC, Argiro L, Dessein H, Prata A, Dessein A, Rodrigues V (2009) Th1/Th2 immune responses are associated with active cutaneous leishmaniasis and clinical cure is associated with strong interferon-γ production. HIM J 70(6):383–390. doi:10.1016/j.humimm.2009.01.007
Cunninghame Graham DS, Graham RR, Manku H, Wong AK, Whittaker JC, Gaffney PM, Moser KL, Rioux JD, Altshuler D, Behrens TW, Vyse TJ (2008) Polymorphism at the TNF superfamily gene TNFSF4 confers susceptibility to systemic lupus erythematosus. Nat Genet 40(1):83–89. doi:10.1038/ng.2007.47
Gateva V, Sandling JK, Hom G, Taylor KE, Chung SA, Sun X, Ortmann W, Kosoy R, Ferreira RC, Nordmark G, Gunnarsson I, Svenungsson E, Padyukov L, Sturfelt G, Jönsen A, Bengtsson AA, Rantapää-Dahlqvist S, Baechler EC, Brown EE, Alarcón GS, Edberg JC, Ramsey-Goldman R, McGwin G, Reveille JD, Vilá LM, Kimberly RP, Manzi S, Petri MA, Lee A, Gregersen PK, Seldin MF, Rönnblom L, Criswell LA, Syvänen A-C, Behrens TW, Graham RR (2009) A large-scale replication study identifies TNIP1, PRDM1, JAZF1, UHRF1BP1 and IL10 as risk loci for systemic lupus erythematosus. Nat Genet 41(11):1228–1233. doi:10.1038/ng.468
Han J-W, Zheng H-F, Cui Y, Sun L-D, Ye D-Q, Hu Z, Xu J-H, Cai Z-M, Huang W, Zhao G-P, Xie H-F, Fang H, Lu Q-J, Xu J-H, Li X-P, Pan Y-F, Deng D-Q, Zeng F-Q, Ye Z-Z, Zhang X-Y, Wang Q-W, Hao F, Ma L, Zuo X-B, Zhou F-S, Du W-H, Cheng Y-L, Yang J-Q, Shen S-K, Li J, Sheng Y-J, Zuo X-X, Zhu W-F, Gao F, Zhang P-L, Guo Q, Li B, Gao M, Xiao F-L, Quan C, Zhang C, Zhang Z, Zhu K-J, Li Y, Hu D-Y, Lu W-S, Huang J-L, Liu S-X, Li H, Ren Y-Q, Wang Z-X, Yang C-J, Wang P-G, Zhou W-M, Lv Y-M, Zhang A-P, Zhang S-Q, Lin D, Li Y, Low HQ, Shen M, Zhai Z-F, Wang Y, Zhang F-Y, Yang S, Liu J-J, Zhang X-J (2009) Genome-wide association study in a Chinese Han population identifies nine new susceptibility loci for systemic lupus erythematosus. Nat Genet 41(11):1234–1237. doi:10.1038/ng.472
Sanchez E, Webb RD, Rasmussen A, Kelly JA, Riba L, Kaufman KM, Garcia-de la Torre I, Moctezuma JF, Maradiaga-Cecena MA, Cardiel-Rios MH, Acevedo E, Cucho-Venegas M, Garcia MA, Gamron S, Pons-Estel BA, Vasconcelos C, Martin J, Tusie-Luna T, Harley JB, Richardson B, Sawalha AH, Alarcon-Riquelme ME (2010) Genetically determined Amerindian ancestry correlates with increased frequency of risk alleles for systemic lupus erythematosus. Arthritis Rheum 62(12):3722–3729. doi:10.1002/art.27753
Zhou XJ, Cheng FJ, Qi YY, Zhao MH, Zhang H (2013) A replication study from Chinese supports association between lupus-risk allele in TNFSF4 and renal disorder. BioMed Res Int 2013:597921. doi:10.1155/2013/597921
Lee YH, Song GG (2012) Associations between TNFSF4 and TRAF1-C5 gene polymorphisms and systemic lupus erythematosus: a meta-analysis. Hum Immunol 73(10):1050–1054. doi:10.1016/j.humimm.2012.07.044
Manku H, Langefeld CD, Guerra SG, Malik TH, Alarcon-Riquelme M, Anaya JM, Bae SC, Boackle SA, Brown EE, Criswell LA, Freedman BI, Gaffney PM, Gregersen PA, Guthridge JM, Han SH, Harley JB, Jacob CO, James JA, Kamen DL, Kaufman KM, Kelly JA, Martin J, Merrill JT, Moser KL, Niewold TB, Park SY, Pons-Estel BA, Sawalha AH, Scofield RH, Shen N, Stevens AM, Sun C, Gilkeson GS, Edberg JC, Kimberly RP, Nath SK, Tsao BP, Vyse TJ (2013) Trans-ancestral studies fine map the SLE-susceptibility locus TNFSF4. PLoS Genet 9(7), e1003554. doi:10.1371/journal.pgen.1003554
Bossini-Castillo L, Broen JC, Simeon CP, Beretta L, Vonk MC, Ortego-Centeno N, Espinosa G, Carreira P, Camps MT, Navarrete N, Gonzalez-Escribano MF, Vicente-Rabaneda E, Rodriguez L, Tolosa C, Roman-Ivorra JA, Gomez-Gracia I, Garcia-Hernandez FJ, Castellvi I, Gallego M, Fernandez-Nebro A, Garcia-Portales R, Egurbide MV, Fonollosa V, de la Pena PG, Pros A, Gonzalez-Gay MA, Hesselstrand R, Riemekasten G, Witte T, Coenen MJ, Koeleman BP, Houssiau F, Smith V, de Keyser F, Westhovens R, De Langhe E, Voskuyl AE, Schuerwegh AJ, Chee MM, Madhok R, Shiels P, Fonseca C, Denton C, Claes K, Padykov L, Nordin A, Palm O, Lie BA, Airo P, Scorza R, van Laar JM, Hunzelmann N, Kreuter A, Herrick A, Worthington J, Radstake TR, Martin J, Rueda B (2011) A replication study confirms the association of TNFSF4 (OX40L) polymorphisms with systemic sclerosis in a large european cohort. Ann Rheum Dis 70(4):638–641. doi:10.1136/ard.2010.141838
Gourh P, Arnett FC, Tan FK, Assassi S, Divecha D, Paz G, McNearney T, Draeger H, Reveille JD, Mayes MD, Agarwal SK (2010) Association of TNFSF4 (OX40L) polymorphisms with susceptibility to systemic sclerosis. Ann Rheum Dis 69(3):550–555. doi:10.1136/ard.2009.116434
Coustet B, Bouaziz M, Dieude P, Guedj M, Bossini-Castillo L, Agarwal S, Radstake T, Martin J, Gourh P, Elhai M, Koumakis E, Avouac J, Ruiz B, Mayes M, Arnett F, Hachulla E, Diot E, Cracowski JL, Tiev K, Sibilia J, Mouthon L, Frances C, Amoura Z, Carpentier P, Cosnes A, Meyer O, Kahan A, Boileau C, Chiocchia G, Allanore Y (2012) Independent replication and meta analysis of association studies establish TNFSF4 as a susceptibility gene preferentially associated with the subset of anticentromere-positive patients with systemic sclerosis. J Rheumat 39(5):997–1003. doi:10.3899/jrheum.111270
Faraco J, Lin L, Kornum BR, Kenny EE, Trynka G, Einen M, Rico TJ, Lichtner P, Dauvilliers Y, Arnulf I, Lecendreux M, Javidi S, Geisler P, Mayer G, Pizza F, Poli F, Plazzi G, Overeem S, Lammers GJ, Kemlink D, Sonka K, Nevsimalova S, Rouleau G, Desautels A, Montplaisir J, Frauscher B, Ehrmann L, Hogl B, Jennum P, Bourgin P, Peraita-Adrados R, Iranzo A, Bassetti C, Chen WM, Concannon P, Thompson SD, Damotte V, Fontaine B, Breban M, Gieger C, Klopp N, Deloukas P, Wijmenga C, Hallmayer J, Onengut-Gumuscu S, Rich SS, Winkelmann J, Mignot E (2013) ImmunoChip study implicates antigen presentation to T cells in narcolepsy. PLoS Genet 9(2), e1003270. doi:10.1371/journal.pgen.1003270
Nordmark G, Kristjansdottir G, Theander E, Appel S, Eriksson P, Vasaitis L, Kvarnstrom M, Delaleu N, Lundmark P, Lundmark A, Sjowall C, Brun JG, Jonsson MV, Harboe E, Goransson LG, Johnsen SJ, Soderkvist P, Eloranta ML, Alm G, Baecklund E, Wahren-Herlenius M, Omdal R, Ronnblom L, Jonsson R, Syvanen AC (2011) Association of EBF1, FAM167A(C8orf13)-BLK and TNFSF4 gene variants with primary Sjogren’s syndrome. Genes Immun 12(2):100–109. doi:10.1038/gene.2010.44
Wilde B, Dolff S, Cai X, Specker C, Becker J, Totsch M, Costabel U, Durig J, Kribben A, Tervaert JW, Schmid KW, Witzke O (2009) CD4 + CD25+ T-cell populations expressing CD134 and GITR are associated with disease activity in patients with Wegener’s granulomatosis. Nephrol Dial Transplant: Proc Eur Dial Assoc Eur Ren Assoc 24(1):161–171. doi:10.1093/ndt/gfn461
Aten J, Roos A, Claessen N, Schilder-Tol EJ, Ten Berge IJ, Weening JJ (2000) Strong and selective glomerular localization of CD134 ligand and TNF receptor-1 in proliferative lupus nephritis. J American Soc Nephrol: JASN 11(8):1426–1438
Abo-Elenein A, Shaaban D, Gheith O (2008) Flowcytometric study of expression of perforin and CD134 in patients with systemic lupus erythematosus. Egypt J Immunol / Egypt Assoc Immunol 15(2):135–143
Farres MN, Al-Zifzaf DS, Aly AA, Abd Raboh NM (2011) OX40/OX40L in systemic lupus erythematosus: association with disease activity and lupus nephritis. Ann Saudi med 31(1):29–34. doi:10.4103/0256-4947.75775
Kshirsagar S, Binder E, Riedl M, Wechselberger G, Steichen E, Edelbauer M (2013) Enhanced activity of Akt in Teff cells from children with lupus nephritis is associated with reduced induction of tumor necrosis factor receptor-associated factor 6 and increased OX40 expression. Arthritis Rheum 65(11):2996–3006. doi:10.1002/art.38089
Mesquita Junior D, Cruvinel WM, Araujo JA, Salmazi KC, Kallas EG, Andrade LE et al (2014) Imbalanced expression of functional surface molecules in regulatory and effector T cells in systemic lupus erythematosus. Braz J Med Biol Res = Revista brasileira de pesquisas medicas e biologicas / Sociedade Brasileira de Biofisica 47(8):662–669
Patschan S, Dolff S, Kribben A, Durig J, Patschan D, Wilde B, Specker C, Philipp T, Witzke O (2006) CD134 expression on CD4+ T cells is associated with nephritis and disease activity in patients with systemic lupus erythematosus. Clin Exp Immunol 145(2):235–242. doi:10.1111/j.1365-2249.2006.03141.x
Zhou YB, Ye RG, Li YJ, Xie CM (2009) Targeting the CD134-CD134L interaction using anti-CD134 and/or rhCD134 fusion protein as a possible strategy to prevent lupus nephritis. Rheumatol Int 29(4):417–425. doi:10.1007/s00296-008-0697-2
Bornsen L, Christensen JR, Ratzer R, Oturai AB, Sorensen PS, Sondergaard HB, Sellebjerg F (2012) Effect of natalizumab on circulating CD4+ T-cells in multiple sclerosis. PLoS One 7(11), e47578. doi:10.1371/journal.pone.0047578
Xiaoyan Z, Pirskanen R, Malmstrom V, Lefvert AK (2006) Expression of OX40 (CD134) on CD4+ T-cells from patients with myasthenia gravis. Clin Exp Immunol 143(1):110–116. doi:10.1111/j.1365-2249.2005.02955.x
Szypowska A, Stelmaszczyk-Emmel A, Demkow U, Luczynski W (2014) High expression of OX40 (CD134) and 4-1BB (CD137) molecules on CD4(+)CD25(high) cells in children with type 1 diabetes. Adv Med Sci 59(1):39–43. doi:10.1016/j.advms.2013.07.003
Luczynski W, Stasiak-Barmuta A, Juchniewicz A, Wawrusiewicz-Kurylonek N, Ilendo E, Kos J, Kretowski A, Gorska M, Chyczewski L, Bossowski A (2010) The mRNA expression of pro- and anti-inflammatory cytokines in T regulatory cells in children with type 1 diabetes. Folia Histochem Cytobiol / Pol AcadSci, Pol Histochem Cytochem Soc 48(1):93–100. doi:10.2478/v10042-008-0113-5
Rajabi P, Alaee M, Mousavizadeh K, Samadikuchaksaraei A et al (2012) Altered expression of TNFSF4 and TRAF2 mRNAs in peripheral blood mononuclear cells in patients with systemic lupus erythematosus: association with atherosclerotic symptoms and lupus nephritis. Inflamma Res: Off J EurHistamine Res Soc 61(12):1347–1354. doi:10.1007/s00011-012-0535-6
Komura K, Yoshizaki A, Kodera M, Iwata Y, Ogawa F, Shimizu K, Wayaku T, Yukami T, Murata M, Hasegawa M, Fujimoto M, Takehara K, Sato S (2008) Increased serum soluble OX40 in patients with systemic sclerosis. J Rheumat 35(12):2359–2362
Laustsen JK, Rasmussen TK, Stengaard-Pedersen K, Horslev-Petersen K, Hetland ML, Ostergaard M, Junker P, Hvid M, Deleuran B (2014) Soluble OX40L is associated with presence of autoantibodies in early rheumatoid arthritis. Arthritis Res Ther 16(5):474. doi:10.1186/s13075-014-0474-4
Li M, Yang Q, Zhang Y (2007) Effects of CD134 monoclonal antibody on hemolysis activities and expression of perforin in peripheral blood mononuclear cells of systemic lupus erythematosus patients. Hybridoma 26(4):191–200. doi:10.1089/hyb.2007.010
Wang Q, Zhang K, Ma Y, Zhang G (2013) Amplification of T cell autoreactivity by OX40/OX40L functional complex on peripheral CD4+ T cells in Graves’ disease. Front Immunol Conference Abstract: 15th International Congress of Immunology (ICI). doi: 10.3389/conf.fimmu.2013.02.01092
Kaleeba JA, Offner H, Vandenbark AA, Lublinski A, Weinberg AD (1998) The OX-40 receptor provides a potent co-stimulatory signal capable of inducing encephalitogenicity in myelin-specific CD4+ T cells. Int Immunol 10(4):453–461
Wang XD, Wu TY (2008) The role of OX40 in CD4+ T cells cytokines production in ulcerative colitis. Zhonghua nei ke za zhi 47(1):15–18
Zhang N, Li G, Xiao B, Liu Y, Cai Y, Sun X, Liang J (2010) Dynamic change OX40/OX40L mRNA in experimental allergic neuritis. Zhong nan da xue xue bao Yi xue ban = J Cent South UnivMedic Sci 35(9):964–968. doi:10.3969/j.issn.1672-7347.2010.09.011
Yu S, Medling B, Yagita H, Braley-Mullen H (2001) Characteristics of inflammatory cells in spontaneous autoimmune thyroiditis of NOD.H-2h4 mice. J Autoimmun 16(1):37–46. doi:10.1006/jaut.2000.0458
Saijo S, Asano M, Horai R, Yamamoto H, Iwakura Y (2002) Suppression of autoimmune arthritis in interleukin-1-deficient mice in which T cell activation is impaired due to low levels of CD40 ligand and OX40 expression on T cells. Arthritis Rheum 46(2):533–544
Nakae S, Saijo S, Horai R, Sudo K, Mori S, Iwakura Y (2003) IL-17 production from activated T cells is required for the spontaneous development of destructive arthritis in mice deficient in IL-1 receptor antagonist. Proc Natl Acad Sci U S A 100(10):5986–5990. doi:10.1073/pnas.1035999100
Pakala SV, Bansal-Pakala P, Halteman BS, Croft M (2004) Prevention of diabetes in NOD mice at a late stage by targeting OX40/OX40 ligand interactions. Eur J Immunol 34(11):3039–3046. doi:10.1002/eji.200425141
Elmann A, Sharabi A, Dayan M, Zinger H, Ophir R, Mozes E (2007) Altered gene expression in mice with lupus treated with edratide, a peptide that ameliorates the disease manifestations. Arthritis Rheum 56(7):2371–2381. doi:10.1002/art.22736
Hong GU, Kim NG, Jeoung D, Ro JY (2013) Anti-CD40 Ab- or 8-oxo-dG-enhanced Treg cells reduce development of experimental autoimmune encephalomyelitis via down-regulating migration and activation of mast cells. J Neuroimmunol 260(1–2):60–73. doi:10.1016/j.jneuroim.2013.04.002
Malmstrom V, Shipton D, Singh B, Al-Shamkhani A, Puklavec MJ, Barclay AN, Powrie F (2001) CD134L expression on dendritic cells in the mesenteric lymph nodes drives colitis in T cell-restored SCID mice. J Immunol 166(11):6972–6981
Yoshioka T, Nakajima A, Akiba H, Ishiwata T, Asano G, Yoshino S, Yagita H, Okumura K (2000) Contribution of OX40/OX40 ligand interaction to the pathogenesis of rheumatoid arthritis. Eur J Immunol 30(10):2815–2823. doi:10.1002/1521-4141(200010)30:10<2815::aid-immu2815>3.0.co;2-#
Saito K, Mori S, Date F, Ono M (2013) Sjogren’s syndrome-like autoimmune sialadenitis in MRL-Faslpr mice is associated with expression of glucocorticoid-induced TNF receptor-related protein (GITR) ligand and 4-1BB ligand. Autoimmunity 46(4):231–237. doi:10.3109/08916934.2012.757307
Boot EP, Koning GA, Storm G, Wagenaar-Hilbers JP, van Eden W, Everse LA, Wauben MH (2005) CD134 as target for specific drug delivery to auto-aggressive CD4+ T cells in adjuvant arthritis. Arthritis research & therapy 7(3):R604–R615. doi:10.1186/ar1722
Pohl M, Kawakami N, Kitic M, Bauer J, Martins R, Fischer MT, Machado-Santos J, Mader S, Ellwart JW, Misu T, Fujihara K, Wekerle H, Reindl M, Lassmann H, Bradl M (2013) T cell-activation in neuromyelitis optica lesions plays a role in their formation. Acta Neuropathol Commun 1(1):85. doi:10.1186/2051-5960-1-85
de Vos AF, Dick AD, Klooster J, Broersma L, McMenamin PG, Kijlstra A (2000) Analysis of the cellular infiltrate in the iris during experimental autoimmune encephalomyelitis. Invest Ophthalmol Vis Sci 41(10):3001–3010
Weinberg AD, Lemon M, Jones AJ, Vainiene M, Celnik B, Buenafe AC, Culbertson N, Bakke A, Vandenbark AA, Offner H (1996) OX-40 antibody enhances for autoantigen specific V beta 8.2+ T cells within the spinal cord of Lewis rats with autoimmune encephalomyelitis. J Neurosci Res 43(1):42–49. doi:10.1002/jnr.490430105
Odobasic D, Kitching AR, Tipping PG, Holdsworth SR (2005) CD80 and CD86 costimulatory molecules regulate crescentic glomerulonephritis by different mechanisms. Kidney Int 68(2):584–594. doi:10.1111/j.1523-1755.2005.00436.x
Usui Y, Akiba H, Takeuchi M, Okunuki Y, Kezuka T, Hattori T, Takeuchi A, Okumura K, Usui M (2005) The role of OX40/OX40L pathway in murine experimental autoimmune uveoretinitis (EAU). Invest Ophthalmol Vis Sci 46(5):995
Ndhlovu LC, Ishii N, Murata K, Sato T, Sugamura K (2001) Critical involvement of OX40 ligand signals in the T cell priming events during experimental autoimmune encephalomyelitis. J Immunol 167(5):2991–2999
Nohara C, Akiba H, Nakajima A, Inoue A, Koh CS, Ohshima H, Yagita H, Mizuno Y, Okumura K (2001) Amelioration of experimental autoimmune encephalomyelitis with anti-OX40 ligand monoclonal antibody: a critical role for OX40 ligand in migration, but not development, of pathogenic T cells. J Immunol 166(3):2108–2115
Elyaman W, Kivisakk P, Reddy J, Chitnis T, Raddassi K, Imitola J, Bradshaw E, Kuchroo VK, Yagita H, Sayegh MH, Khoury SJ (2008) Distinct functions of autoreactive memory and effector CD4+ T cells in experimental autoimmune encephalomyelitis. AM J Pathol 173(2):411–422. doi:10.2353/ajpath.2008.080142
Croft M (2009) The role of TNF superfamily members in T-cell function and diseases. Nat Rev Immunol 9(4):271–285. doi:10.1038/nri2526
Gwyer Findlay E, Danks L, Madden J, Cavanagh MM, McNamee K, McCann F, Snelgrove RJ, Shaw S, Feldmann M, Taylor PC, Horwood NJ, Hussell T (2014) OX40L blockade is therapeutic in arthritis, despite promoting osteoclastogenesis. Proc Natl Acad Sci U S A 111(6):2289–2294. doi:10.1073/pnas.1321071111
Gaspal F, Withers D, Saini M, Bekiaris V, McConnell FM, White A, Khan M, Yagita H, Walker LS, Anderson G, Lane PJ (2011) Abrogation of CD30 and OX40 signals prevents autoimmune disease in FoxP3-deficient mice. J Exp Med 208(8):1579–1584. doi:10.1084/jem.20101484
Mayer CT, Tian L, Hesse C, Kuhl AA, Swallow M, Kruse F, Thiele M, Gershwin ME, Liston A, Sparwasser T (2014) Anti-CD4 treatment inhibits autoimmunity in scurfy mice through the attenuation of co-stimulatory signals. J Autoimmun 50:23–32. doi:10.1016/j.jaut.2013.08.010
Bresson D, Fousteri G, Manenkova Y, Croft M, von Herrath M (2011) Antigen-specific prevention of type 1 diabetes in NOD mice is ameliorated by OX40 agonist treatment. J Autoimmun 37(4):342–351. doi:10.1016/j.jaut.2011.10.001
Wu X, Rosenbaum JT, Adamus G, Zhang GL, Duan J, Weinberg A, Zhang Z (2011) Activation of OX40 prolongs and exacerbates autoimmune experimental uveitis. Invest Ophthalmol Vis Sci 52(11):8520–8526. doi:10.1167/iovs.11-7664
Chitnis T, Najafian N, Abdallah KA, Dong V, Yagita H, Sayegh MH, Khoury SJ (2001) CD28-independent induction of experimental autoimmune encephalomyelitis. J Clin Invest 107(5):575–583. doi:10.1172/jci11220
Weinberg AD, Wegmann KW, Funatake C, Whitham RH (1999) Blocking OX-40/OX-40 ligand interaction in vitro and in vivo leads to decreased T cell function and amelioration of experimental allergic encephalomyelitis. J Immunol 162(3):1818–1826
Gauvreau GM, Boulet LP, Cockcroft DW, FitzGerald JM, Mayers I, Carlsten C, Laviolette M, Killian KJ, Davis BE, Larche M, Kipling C, Dua B, Mosesova S, Putnam W, Zheng Y, Scheerens H, McClintock D, Matthews JG, O’Byrne PM (2014) OX40L blockade and allergen-induced airway responses in subjects with mild asthma. Clin Exp Allergy : J Brit Soc Allergy and Clin Immunol 44(1):29–37. doi:10.1111/cea.12235
Chen M, Xiao X, Demirci G, Li XC (2008) OX40 controls islet allograft tolerance in CD154 deficient mice by regulating FOXP3+ Tregs. Transplantation 85(11):1659–1662. doi:10.1097/TP.0b013e3181726987
Imura A, Hori T, Imada K, Kawamata S, Tanaka Y, Imamura S, Uchiyama T (1997) OX40 expressed on fresh leukemic cells from adult T-cell leukemia patients mediates cell adhesion to vascular endothelial cells: implication for the possible involvement of OX40 in leukemic cell infiltration. Blood 89(8):2951–2958
Morris NP, Peters C, Montler R, Hu HM, Curti BD, Urba WJ, Weinberg AD (2007) Development and characterization of recombinant human Fc:OX40L fusion protein linked via a coiled-coil trimerization domain. Mol Immunol 44(12):3112–3121. doi:10.1016/j.molimm.2007.02.004
Song Y, Margolles-Clark E, Bayer A, Buchwald P (2014) Small-molecule modulators of the OX40-OX40 ligand co-stimulatory protein-protein interaction. Br J Pharmacol 171(21):4955–4969. doi:10.1111/bph.12819
Tuladhar R, Oghumu S, Dong R, Peterson A, Sharpe AH, Satoskar AR (2015) Ox40L–Ox40 pathway plays distinct roles in regulating Th2 responses but does not determine outcome of cutaneous leishmaniasis caused by Leishmania mexicana and Leishmania major. Exp Parasitol 148(C):49–55. doi:10.1016/j.exppara.2014.11.002
Weinberg AD, Morris NP, Kovacsovics-Bankowski M, Urba WJ, Curti BD (2011) Science gone translational: the OX40 agonist story. Immunol Rev 244(1):218–231. doi:10.1111/j.1600-065X.2011.01069.x
Sharpe AH, Abbas AK (2006) T-cell costimulation--biology, therapeutic potential, and challenges. N Engl J Med 355(10):973–975. doi:10.1056/NEJMp068087
Smeets E, Meiler S, Lutgens E (2013) Lymphocytic tumor necrosis factor receptor superfamily co-stimulatory molecules in the pathogenesis of atherosclerosis. Curr Opin Lipidol 24(6):518–524. doi:10.1097/mol.0000000000000025
Souza HS, Elia CC, Spencer J, MacDonald TT (1999) Expression of lymphocyte-endothelial receptor-ligand pairs, alpha4beta7/MAdCAM-1 and OX40/OX40 ligand in the colon and jejunum of patients with inflammatory bowel disease. Gut 45(6):856–863
Periolo N, Guillén L, Arruvito ML, Alegre NS, Niveloni SI, Hwang JH, Bai JC, Cherñavsky AC (2014) IL-15 controls T cell functions through its influence on CD30 and OX40 antigens in celiac disease. Cytokine 67(1):44–51. doi:10.1016/j.cyto.2014.01.004
Brugnoni D, Bettinardi A, Malacarne F, Airo P, Cattaneo R (1998) CD134/OX40 expression by synovial fluid CD4+ T lymphocytes in chronic synovitis. Br J Rheumatol 37(5):584–585
Passacantando A, Parzanese I, Rascente M, Petrucci C, Minisola G, Tonietti G (2006) Synovial fluid OX40T lymphocytes of patients with rheumatoid arthritis display a Th2/Th0 polarization. Int J Immunopathol Pharmacol 19(3):499–505
Koo J, Kim S, Jung WJ, Lee YE, Song GG, Kim KS, Kim MY (2013) Increased lymphocyte infiltration in rheumatoid arthritis is correlated with an increase in LTi-like cells in synovial fluid. Immune Netw 13(6):240–248. doi:10.4110/in.2013.13.6.240
Papadopoulos C, Terzis G, Papadimas GK, Manta P (2013) OX40-OX40L expression in idiopathic inflammatory myopathies. Anal Quant Cytopathol Histopath 35(1):17–26
Tateyama M, Fujihara K, Ishii N, Sugamura K, Onodera Y, Itoyama Y (2002) Expression of OX40 in muscles of polymyositis and granulomatous myopathy. J Neurol Sci 194(1):29–34
Bossowski A, Stasiak-Barmuta A, Urban M, Bossowska A (2005) Analysis of costimulatory molecules OX40/4-1BB (CD134/CD137) detection on chosen mononuclear cells in children and adolescents with Graves’ disease during methimazole therapy. J Pediatr Endocrinol Metab 18(12):1365–1372
Bossowski A, Stasiak-Barmuta A, Urban M, Rinderle C (2005) Relationship between OX40/4-1 BB (CD134/CD137) costimulatory molecules expression on T lymphocytes and stimulating and blocking autoantibodies to the TSH-receptor in children with Graves’ disease. Endokrynol Diabetol Chor Przemiany Materii Wieku Rozw: organ Polskiego Towarzystwa Endokrynologow Dzieciecych 11(3):133–140
Zhu R, Jiang J, Wang T, Xu T, Wu M, Liu C, Zhang X (2013) Expressions and clinical significance of OX40 and OX40L in peripheral blood of patients with primary Sjogren’s syndrome. Xi bao yu fen zi mian yi xue za zhi = Chin J Cell Mol immunol 29(8):862–865
Onodera J, Nagata T, Fujihara K, Ohuchi M, Ishii N, Sugamura K, Itoyama Y (2000) Expression of OX40 and OX40 ligand (gp34) in the normal and myasthenic thymus. Acta Neurol Scand 102(4):236–243
Giscombe R, Wang XB, Kakoulidou M, Lefvert AK (2006) Characterization of the expanded T-cell populations in patients with Wegener’s granulomatosis. J Intern Med 260(3):224–230. doi:10.1111/j.1365-2796.2006.01688.x
Qin W, Hongya W, Yongjing C, Fang X, Yue M, Xuekun Z, Xiaozhong L, Xueguang Z (2011) Increased OX40 and soluble OX40 ligands in children with Henoch-Schonlein purpura: association with renal involvement. Pediatr Allergy Immunol : Off Pub Eur Soc Pediatr Allergy Immunol 22(1 Pt 1):54–59. doi:10.1111/j.1399-3038.2010.01111.x
Zhou YB, Ye RG, Li YJ, Xie CM, Wu YH (2008) Effect of anti-CD134L mAb and CTLA4Ig on ConA-induced proliferation, Th cytokine secretion, and anti-dsDNA antibody production in spleen cells from lupus-prone BXSB mice. Autoimmunity 41(5):395–404. doi:10.1080/08916930802002240
Totsuka T, Kanai T, Uraushihara K, Iiyama R, Yamazaki M, Akiba H, Yagita H, Okumura K, Watanabe M (2003) Therapeutic effect of anti-OX40L and anti-TNF-alpha MAbs in a murine model of chronic colitis. Am J Physiol Gastrointest Liver Physiol 284(4):G595–G603. doi:10.1152/ajpgi.00450.2002
Martin-Orozco N, Chen Z, Poirot L, Hyatt E, Chen A, Kanagawa O, Sharpe A, Mathis D, Benoist C (2003) Paradoxical dampening of anti-islet self-reactivity but promotion of diabetes by OX40 ligand. J Immunol 171(12):6954–6960
So T, Croft M (2013) Regulation of PI-3-kinase and Akt signaling in T lymphocytes and other cells by TNFR family molecules. Front Immunol 4:139. doi:10.3389/fimmu.2013.00139
Kawamata S, Hori T, Imura A, Takaori-Kondo A, Uchiyama T (1998) Activation of OX40 signal transduction pathways leads to tumor necrosis factor receptor-associated factor (TRAF) 2- and TRAF5-mediated NF-kappaB activation. J Biol Chem 273(10):5808–5814
Boettler T, Choi YS, Salek-Ardakani S, Cheng Y, Moeckel F, Croft M, Crotty S, von Herrath M (2013) Exogenous OX40 stimulation during lymphocytic choriomeningitis virus infection impairs follicular Th cell differentiation and diverts CD4 T cells into the effector lineage by upregulating Blimp-1. J Immunol 191(10):5026–5035. doi:10.4049/jimmunol.1300013
Ohshima Y, Tanaka Y, Tozawa H, Takahashi Y, Maliszewski C, Delespesse G (1997) Expression and function of OX40 ligand on human dendritic cells. J Immunol 159(8):3838–3848
Stuber E, Strober W (1996) The T cell-B cell interaction via OX40-OX40L is necessary for the T cell-dependent humoral immune response. J Exp Med 183(3):979–989
Stuber E, Neurath M, Calderhead D, Fell HP, Strober W (1995) Cross-linking of OX40 ligand, a member of the TNF/NGF cytokine family, induces proliferation and differentiation in murine splenic B cells. Immunity 2(5):507–521
Piconese S, Gri G, Tripodo C, Musio S, Gorzanelli A, Frossi B, Pedotti R, Pucillo CE, Colombo MP (2009) Mast cells counteract regulatory T-cell suppression through interleukin-6 and OX40/OX40L axis toward Th17-cell differentiation. Blood 114(13):2639–2648. doi:10.1182/blood-2009-05-220004
Conflict of Interest
The authors declare no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Webb, G.J., Hirschfield, G.M. & Lane, P.J.L. OX40, OX40L and Autoimmunity: a Comprehensive Review. Clinic Rev Allerg Immunol 50, 312–332 (2016). https://doi.org/10.1007/s12016-015-8498-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12016-015-8498-3