
Abstract
Tacrolimus is an immunosuppressive drug widely used in kidney transplantation. Cytochrome P450 3A5 (CYP3A5) protein is involved in tacrolimus metabolism. Single nucleotide polymorphism in the CYP3A5 gene (6986A>G) results in alteration in metabolic activity of CYP3A5 protein which eventually affects the tacrolimus concentration. Patients with CYP3A5 expresser genotypes (A/A *1/*1 and A/G *1/*3) metabolize tacrolimus more rapidly than CYP3A5 nonexpressers (G/G *3/*3). We performed meta-analysis to estimate the effect of CYP3A5 polymorphism on the trough concentration–dose ratio (Co/D) and risk of renal allograft rejection with similar post-transplant periods and Asian vs. European populations. Our results showed that the tacrolimus Co/D ratio is significantly lower in CYP3A5 expresser group as compared with nonexpresser in Asian as well as in European populations at any post-transplant period (p < 0.00001). No significant association was found with renal allograft rejection episodes between expressers and nonexpressers in European populations (OR: 1.12; p = 0.47). Interestingly, Asian population (with expresser genotypes) and patients after 3 years post-transplantation (with expresser genotypes) have a higher risk of rejection (OR: 1.62; p < 0.05), (OR: 1.68; p < 0.05), respectively. This could be due to high prevalence of expresser genotypes in Asian population. Few tacrolimus-based studies are identified with long-term graft survival. There is a need to have more studies looking for long-term graft survival in expresser as well as no-expresser groups especially in Asian populations who have high frequency of CYP3A5 functional genotype.
Similar content being viewed by others

Introduction
Tacrolimus (Prograf, PK-506) is a potent immunosuppressive drug widely used in renal transplantation. It acts as calcineurin inhibitor and prevents T-cell activation by inhibiting phosphatase calcineurin [1]. Hence, it may lower the risk of renal allograft rejection mediated by T cells (TCMR). The optimum drug dose and plasma concentration level of tacrolimus are desired for stable graft functioning. Subtherapeutic tacrolimus drug concentration initiates allograft rejection while supratherapeutic levels of tacrolimus result in drug toxicity, infections, fibrosis, etc [2,3,4,5]. Thus, a very fine margin between sub- and supratherapeutic levels is maintained based on tacrolimus dosage and its metabolism in renal transplantation.
Cytochrome P450 (CYP) 3A5 isoenzymes are identified as the major enzyme responsible for tacrolimus metabolism. Single nucleotide polymorphism in the CYP3A5 gene (rs776746; 6986A>G) results in a change in metabolic activity of CYP3A5 protein which ultimately affects the tacrolimus concentration [6]. The CYP3A5-A reference allele (also known as *1) codes for a functional CYP3A5 protein. Individuals carrying homozygous AA (*1/*1) or heterozygous AG (*1/*3) CYP3A5 genotypes exhibit rapid enzymatic metabolizing rate for tacrolimus, hence categorized as rapid and intermediate drug metabolizers, respectively. Both these genotypes (AA and AG) of CYP3A5 are categorized as expressers. On the other hand, homozygous GG (*3/*3) genotype has a nonfunctional CYP3A5 protein that shows poor tacrolimus metabolism, hence known as nonexpresser.
The tacrolimus pharmacokinetics may vary with the presence of CYP3A5 gene polymorphism, ethnicity, and post-transplantation period [7]. Systematic reviews have evaluated the effect of CYP3A5 gene polymorphism on tacrolimus pharmacokinetics in adults and pediatric renal transplant population [7,8,9,10,11]. These studies have shown significantly higher tacrolimus trough concentration divided by daily dose per body weight (Co/D) in patient carrying CYP3A5 (GG or *3/*3) polymorphism i.e., nonexpresser, than expresser CYP3A5 (AA or *1/*1) at various post-transplant time (<1, 3–9, 12–24, 36–60 months). These analyses have certain limitations as they lack pooled studies with similar clinical covariates, ethnicity, and post-transplantation duration.
In this meta-analysis, we aim to analyze studies with similar clinical covariates (such as donor type, living/deceased donor), ethnicity (Caucasians/Asian), region (European/Asian/American), post-transplant time (weeks/months) with CYP3A5 gene polymorphism, and tacrolimus pharmacokinetics (Co/D). Further, to investigate the impact of CYP3A5 polymorphism on the tacrolimus and subsequently on rejection event(s) on the short/long-term renal graft survival.
We systematically collected and combined the published data on the effect of CYP3A5 gene polymorphism on tacrolimus pharmacokinetics and performed meta-analysis to evaluate the inconsistence in the result of various studies that might be due to the chance variation, sample size, ethnic/geographic difference, or low power studies.
Meta-analysis
Literature search strategy and sources
The review protocol used for this study was not preregistered. Literature was searched for the relevant studies from the electronic databases of the PubMed, Google Scholar, EMBASE, and Cochrane library published by March 2019. Keywords used for the search were related to the TAC (Tacrolimus, FK506, and Prograf), Cytochrome P450 gene polymorphisms (CYP3A5*3 and CYP3A5*1) in transplantation (renal or kidney). No language limitations were applied in search and only human species based studies were included. To expand the relevant articles search, the references cited in the retrieved articles were further explored. The databases search was conducted by two researchers independently.
Data extraction and eligibility criteria
The selected articles were screened for the relevance of data according to the eligibility criteria. The articles were scrutinized by three independent researchers and conflicting issues were resolved through discussions. The information extracted from each selected study includes first author name, year of publication, study design, total number of cases/controls, age group, ethnicity, and CYP3A5 genotyping (CYP3A5*1/*1, CYP3A5*1/*3, and CYP3A5*3/*3) among renal transplant patients. Data regarding tacrolimus drug administration such as initial drug dose/ strength, mode of administration (Oral), number of doses per day (BD), the measurement of tacrolimus trough levels in blood, and calculated tacrolimus trough level/dose (Co/D) levels at various post-transplant time were also included. Studies that reported incidence of rejection (acute) episodes and pharmacokinetic data on tacrolimus classified according to the CYP3A5 gene polymorphism of the renal transplant patients were separately analyzed.
Sufficient data for the evaluation of statistical significance
The eligible studies were selected to meet the following criteria: (1) original studies with appropriately presented data; (2) inclusion of only renal transplant-based studies provided either (a) tacrolimus (Co/D) levels between CYP3A5 expresser and nonexpresser or (b) tacrolimus (Co/D) levels in rejection and nonrejection as events between CYP3A5 expresser and nonexpresser.
The studies were excluded on the basis of insufficiency of data presented in the article, involving either transplant patients other than renal or combined transplantation (renal and pancreas etc). Review articles were also omitted. Only published studies were used for data extraction. Corresponding authors were contacted via email for any additional information.
Statistical analysis
Forest plots were generated for tacrolimus pharmacokinetic studies using Review Manager Software (RevMan, version 5.3). Continuous data were analyzed by the inverse variance method and association of tacrolimus Co/D with CYP3A5 gene polymorphism was determined by standard mean difference (SMD). On the other hand, dichotomous data (data regarding expressers and nonexpressers group) were analyzed by the Mantel–Haenszel (M–H) method and the strength of their association with rejection was determined by the odds ratio (OR).
Heterogeneity (I2) among the studies was calculated using Higgins I2 statistic and chi-squared (χ2) tests. The range of heterogeneity was 0–100%. Based on heterogeneity value, either fixed or random effect model was used to calculate the effect size of the study. For heterogeneity of >50% or P ≤ 0.05, the random-effect model was used. Furthermore, variance among the selected studies was calculated by Tau2 using random-effect model.
Articles’ (publication) biases were assessed by the Egger’s rank correlation test and Begg’s regression tests, respectively [12, 13]. Both tests were performed using Metaphor, a meta-analysis package for R [14, 15]. A P value ≤0.05 was considered as significant publication bias.
The cumulative effect of the studies was determined by the Z score. A Z score ≥1.96 or P value ≤0.05 indicates that the genotype is in significant association with (a) tacrolimus Co/D levels and (b) renal allograft rejection events.
Results
Meta-analysis
Study selection and characteristics
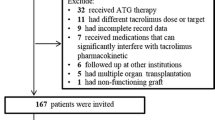
The course of study selection for the association of the CYP3A5 gene polymorphism with tacrolimus pharmacokinetics and rejection is given in Fig. 1. Electronic databases were searched using predefined search strategy. Initial databases search retrieved (n = 777) articles using various MeSH terms. All of the results were entered in the Endnote software for title and abstract screening.

Flow diagram depicting the selection procedure of eligible studies.
We excluded n = 725 studies comprising duplicating articles (n = 424), reviews (n = 71), drug doses 1 vs. 2 (n = 21), non-renal transplant population (n = 60), drug predicting model (n = 18), drug interaction (n = 7), CYP detection methodology (n = 12), meta-analysis (n = 7), desired Tac Co/D unit not present (n = 16), and lack of Tac Co/D data (n = 89). Finally, a total of n = 52 articles were identified for data assessment for the meta-analysis.
The main characteristics of the studies included in this meta-analysis to investigate the CYP3A5 gene polymorphism with tacrolimus pharmacokinetics (Co/D; n = 27) and rejection episodes (n = 25) are provided in Supplementary Tables 1 and 2, respectively. The selected studies were published between 2003 and 2018.
Tacrolimus Co/D studies among renal transplant patients
Overall, a total of 15 studies were carried out in Europe including two studies from Belgium, four from Italy, three from Netherland and Spain, two from France, and one from Poland. These studies comprised Caucasian populations at large. However, seven studies involved mix populations i.e., Caucasian (76–98%) and African/Asian (2–29%).
There were twelve studies published from Asian region; five studies from China, four from Korea, two from Japan, and one from Jordan. A majority of these studies were cohort study designed based on either hospital or institute/university.
Tacrolimus Co/D ratio with time intervals among Asian transplant patients
The studies involving the tacrolimus Co/D ratio among Asian populations (n = 12) with CYP3A5 genotypes were classified according to post-transplant periods as 1 week, 2 week, 3–4 weeks, 3–6 months, and 12 months. The results showed no significant heterogeneity among the mean differences of Tac Co/D among Asian populations. A significantly low SMD (−1.35, −1.39, −1.15, −1.24, −1.02, and −1.10) in all time intervals revealed that there is highly decreased cumulative Co/D ratio in Asian expresser CYP3A5 genotypes (Fig. 2).

Tacrolimus Co/D levels in renal transplant patients among Asian population.
Tacrolimus Co/D ratio with time intervals among European transplant patients
The analysis of 15 studies of European population of CYP3A5 genotype also divided into six different time intervals following transplantation (1 week, 2 week, 3–4 weeks, 3 months, 6 months, and 1 year) showed that there was no significant heterogeneity among the mean differences. There was a significantly low SMD (−0.37, −1.01, −1.05, −0.95, −0.96, −0.77) in all time intervals, which means there is a decrease cumulative Co/D ratio in European expresser CYP3A5 genotypes (Fig. 3).

Tacrolimus Co/D levels in renal transplant patients among European population.
Tacrolimus based rejection episodes
The association of CYP3A5 genotypes with renal allograft rejection episode was determined in 25 studies. The selected studies contained 3181 patients. Results showed no significant heterogeneity for rejection events among renal transplant patients with specific CYP3A5 genotype (I2 = 9%, P = 0.34). The OR was 1.16 (95% CI = 0.96–1.41, P = 0.12), which showed no association of either expresser or nonexpresser genotypes with rejection episode (Fig. 4).

Association of CYP3A5 with renal allograft rejection.
The selected studies were further analyzed by stratifying on the time of rejection episode (a) 1–2 weeks, (b) 1–3 months, (c) 12 months, and (d) 36–60 months. The analysis included four studies with a follow-up period of 1–2 weeks, eight studies in 1- to 3-month duration, eight studies at 12 months and three studies with 36- to 60-month follow-up. Interestingly, we found a significant association of CYP3A5 expresser genotype with rejection episode within 36–60 months (OR = 1.68, P = 0.05). This indicated that patients carrying expresser genotype are at increased risk of rejection in long-term transplant. On the other hand, no association was found with rejection between expresser and nonexpresser in short term: (1–2 weeks, OR = 1.41, P = 0.34), (1–3 months, OR = 0.92, P = 0.57) and (12 months, OR = 1.19, P = 0.19: Fig. 5). No publication bias was found in any selected categories (Egger and Begg test, P > 0.05).

Association of CYP3A5 with renal allograft rejection stratifying on the time of rejection episode.
Association between CYP3A5 expresser and nonexpresser genotypes with renal allograft rejection in Asian populations
The analysis of ten studies of Asian population comprised 861 patients of CYP3A5 genotype showed that there was no significant heterogeneity among the studies. There was a significant OR 1.62 (95% CI = 1.16–2.24, P = 0.004*), which means there is a high chance of rejection events in Asian with expresser CYP3A5 genotype (Fig. 6a).

Association of CYP3A5 with renal allograft rejection among the Asian and European populations.
Association between CYP3A5 expresser and nonexpresser genotypes with renal allograft rejection in European populations
The analysis of 13 studies of European population comprised 1579 patients of CYP3A5 genotype showed that there was no significant heterogeneity among the studies. There was no significant OR 1.12 (95% CI = 0.83–1.52, P = 0.47: Fig. 6b).
Discussion
CYP3A5 is a member of cytochrome P450 monooxygenase enzymes mostly express in liver and metabolize tacrolimus via oxidation–reduction reactions. Genetic variations in the CYP3A5 gene can affect the enzyme activities, leading the enzyme to tacrolimus expresser genotypes (CYP3A5*1/*1 and *1/*3) or nonexpresser genotypes (CYP3A5*3/*3). According to several studies, CYP3A5*3 variant (rs776746, c.6986A>G) plays a significant role in tacrolimus metabolism. Variability in tacrolimus levels during early post-transplant period is generally anticipated. This variability in tacrolimus pharmacokinetics is contributed by different CYP3A5 genotypes. This in turn may contribute to graft rejection or early graft lost. Based on association of CYP3A5 polymorphism with tacrolimus metabolism, patients who carry CYP3A5-AA (*1/*1) or AG (*1/*3) genotypes require higher doses to maintain the target trough levels as compared with GG (*3/*3) genotype [7, 9, 16,17,18,19]. On the other hand, low dose is suggested for GG (*3/*3) genotype to avoid drug-related toxicities [18, 20, 21].
In the present study, we performed a meta-analysis to provide a reliable conclusion on the association between CYP3A5 polymorphism on concentration/dose of the tacrolimus (Co/D) ratio and rejection episode in renal transplant patients. Among the 52 included studies, the frequency of CYP3A5 expresser (A) allele was 43.2–48.6% among Asian populations and 14.4–23.7% among European populations. The key finding of current meta-analysis is the association of expresser genotype (CYP3A5*1/*1,*1/*3) with the risk of rejection in the long-term graft survival (from 36 to 60 months post transplantation) Fig. 5. However, no CYP3A5 association was found with the allograft rejection in short-term post-transplant studies (from 0 to 12 months post transplantation). Another significant finding was the association of expresser (CYP3A5*1/*1,*1/*3) with an increased risk of rejection in Asian populations due to high number of rejection episodes in expresser group than nonexpresser group. No CYP3A5 association was found in European population with rejection.
Another important observation was the cumulative decrease of the Co/D ratio in patient carrying CYP3A5 expresser genotype at all time intervals. Asian transplanted patients have shown a reduced Co/D ratio than European transplanted patients that may be due to the high prevalence of the CYP3A5 expresser allele in the Asian population. Asian populations have high heterogeneity because all the three studied Asian populations (Chinese, Japanese and Koreans) have varied expresser allele frequencies which led to cause the raised heterogeneity.
In our included European studies there are certain studies that contain African and Asian population. The allele frequency of functional CYP3A5*1 is more prevalent in both the populations when compared with Europeans. This may have some impact on tacrolimus pharmacokinetics. However, our results have shown no heterogeneity (0–13%) among European studies at different time interval. The results indicated little or no impact by including small portion of these mixed populations.
Currently, long-term graft survival (>10 years) remains the main goal in renal transplantation. Few studies have examined patients with tacrolimus based immunosuppressant levels monitoring in long-term (36–60 months) follow up [20, 22, 23]. Recently, Stegall et al. [24] reported 59% graft survival and 74% death-censored graft survival in tacrolimus based drug regimen at 10 years after transplantation. The major histological abnormalities (arterial hyalinosis (AH), global glomerulosclerosis, and mesangial sclerosis) were found in most (82.1%) of the graft. An AH is the most common histological lesion in functioning graft at 10 years [24].
During the initial phase of transplantation, maintenance of optimum trough level with adjustable tacrolimus doses by therapeutic drug monitoring has been a major challenge in transplantation. An initial tacrolimus dose is administrated based on body weight and subsequently adjusted according to the trough level. Several transplant-based studies have shown the involvement of tacrolimus pharmacokinetics with CYP3A5 polymorphism [21, 25]. Considering the CYP3A5 genotypes in adjusting tacrolimus dosage, instead of a uniform body weight, may help in achieving early target tacrolimus level [26,27,28,29,30,31,32,33,34,35,36]. This approach suggested to help in minimizing the risk of rejection episodes and drug-related complications and may have clinical benefits in short/long post-transplant duration.
We have identified three meta-analysis studies based on the effect of CYP3A5 polymorphisms on tacrolimus pharmacokinetics [9,10,11]. These meta-analyses have some limitations that prompted us to perform a comprehensive analysis with a number of recent studies that are not included in these previous studies. These studies reported TAC Co/D levels and its impact on rejection/drug toxicity including pooled populations of Asians, Africans, and Europeans. However, we stratified our data based on Asian and European population as to investigate the impact of CYP3A5 genotypes on both the populations. The first meta-analysis has some ambiguities regarding the ethnic backgrounds of populations included and sample size [9]. Another recent meta-analysis included only pediatric studies however, we analyzed both pediatric and adult studies [11].
Ethnicity is considered as one of the major contributing factors affecting the long-term graft survival. The frequencies of CYP3A5 functional (A) genotype has been reported in renal transplant patients among various ethnic groups/regions. According to our pooled meta-analysis data the highest prevalence of functional expression of CYP3A5 was reported in African (47%), followed by Asian (22–28%), and European (8–11%) [37, 38]. Pakistan is the homeland of approximately 208 million populations of various ethnic backgrounds (Census 2017). The frequency of CYP3A5 expresser and nonexpresser of our ethnic groups is not available. The awareness in clinician about the prevalence of CYP in various ethnic cast/tribe among renal transplant patients may better guide to achieve targeted tacrolimus dosage. This in turn may reduce drug-related issues such as infections, rejection, malignancies, and cyto-toxicity in short/long-term basis.
To the best of our knowledge, this is the most comprehensive meta-analysis evaluating the relationship between the CYP3A5 expresser genotype with the risk of rejection and the decreased Co/D ratio. In conclusion, our study suggests that a long-term follow-up (>3 years) could be performed in order to find out the increased number of rejection episodes in CYP3A5 expresser genotype and need of close monitoring of Co/D levels in patients carrying CYP3A5 expresser genotype.
References
Hamawy MM. Molecular actions of calcineurin inhibitors. Drug News Perspect. 2003;16:277–82.
Egeland EJ, Robertsen I, Hermann M, Midtvedt K, Storset E, Gustavsen MT, et al. High tacrolimus clearance is a risk factor for acute rejection in the early phase after renal transplantation. Transplantation. 2017;101:e273–e9.
Huang CT, Shu KH, Ho HC, Wu MJ. Higher variability of tacrolimus trough level increases risk of acute rejection in kidney transplant recipients. Transplant Proc. 2016;48:1978–80.
Miura M, Niioka T, Kagaya H, Saito M, Hayakari M, Habuchi T, et al. Pharmacogenetic determinants for interindividual difference of tacrolimus pharmacokinetics 1 year after renal transplantation. J Clin Pharm Ther. 2011;36:208–16.
Stratta P, Quaglia M, Cena T, Antoniotti R, Fenoglio R, Menegotto A, et al. The interactions of age, sex, body mass index, genetics, and steroid weight-based doses on tacrolimus dosing requirement after adult kidney transplantation. Eur J Clin Pharmacol. 2012;68:671–80.
Kuehl P, Zhang J, Lin Y, Lamba J, Assem M, Schuetz J, et al. Sequence diversity in CYP3A promoters and characterization of the genetic basis of polymorphic CYP3A5 expression. Nat Genet. 2001;27:383–91.
Tang HL, Xie HG, Yao Y, Hu YF. Lower tacrolimus daily dose requirements and acute rejection rates in the CYP3A5 nonexpressers than expressers review. Pharmacogenetics Genom. 2011;21:713–20.
Hendijani F, Azarpira N, Kaviani M. Effect of CYP3A5*1 expression on tacrolimus required dose for transplant pediatrics: a systematic review and meta-analysis. Pediatr Transplant. 2018;22:e13248.
Rojas L, Neumann I, Herrero MJ, Boso V, Reig J, Poveda JL, et al. Effect of CYP3A5*3 on kidney transplant recipients treated with tacrolimus: a systematic review and meta-analysis of observational studies. Pharmacogenomics J. 2015;15:38–48.
Terrazzino S, Quaglia M, Stratta P, Canonico PL, Genazzani AA. The effect of CYP3A5 6986A>G and ABCB1 3435C>T on tacrolimus dose-adjusted trough levels and acute rejection rates in renal transplant patients: a systematic review and meta-analysis. Pharmacogenetics Genom. 2012;22:642–5.
Zong YP, Wang ZJ, Zhou WL, Zhou WM, Ma TL, Huang ZK, et al. Effects of CYP3A5 polymorphisms on tacrolimus pharmacokinetics in pediatric kidney transplantation: a systematic review and meta-analysis of observational studies. World J Pediatr. 2017;13:421–6.
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34.
Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50:1088–101.
Viechtbauer W. Conducting meta-analyses in R with the metafor package. J Stat Softw. 2010;36:1–48.
R Core Team. R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. 2014. http://www.R-project.org/.
Flahault AD, Anglicheau, Loriot Marie-Anne, Thervet Eric, Pallet Nicolas. Clinical impact of the CYP3A5 6986A>G allelic variant on kidney transplantation outcomes. Pharmacogenomics. 2017;18:165–73.
Maldonado AQ, Asempa T, Hudson S, Rebellato LM. Prevalence of CYP3A5 genomic variances and their impact on tacrolimus dosing requirements among kidney transplant recipients in Eastern North Carolina. Pharmacotherapy. 2017;37:1081–8.
Nair SS, Sarasamma S, Gracious N, George J, Anish TS, Radhakrishnan R. Polymorphism of the CYP3A5 gene and its effect on tacrolimus blood level. Exp Clin Transplant. 2015;13(Suppl 1):197–200.
Ro H, Min SI, Yang J, Moon KC, Kim YS, Kim SJ, et al. Impact of tacrolimus intraindividual variability and CYP3A5 genetic polymorphism on acute rejection in kidney transplantation. Ther Drug Monit. 2012;34:680–5.
Singh R, Srivastava A, Kapoor R, R KS, R DM. Impact of CYP3A5 and CYP3A4 gene polymorphisms on dose requirement of calcineurin inhibitors, cyclosporine and tacrolimus, in renalallograft recipients of North India. Naunyn-Schmiedebergs Arch Pharmacol. 2009;380:169–77.
Chen JS, Li LS, Cheng DR, Ji SM, Sun QQ, Cheng Z, et al. Effect of CYP3A5 genotype on renal allograft recipients treated with tacrolimus. Transplant Proc. 2009;41:1557–61.
Kuypers DR, Naesens M, de Jonge H, Lerut E, Verbeke K, Vanrenterghem Y. Tacrolimus dose requirements and CYP3A5 genotype and the development of calcineurin inhibitor-associated nephrotoxicity in renal allograft recipients. Ther Drug Monit. 2010;32:394–404.
Quteineh L, Verstuyft C, Furlan V, Durrbach A, Letierce A, Ferlicot S, et al. Influence of CYP3A5 genetic polymorphism on tacrolimus daily dose requirements and acute rejection in renal graft recipients. Basic Clin Pharmacol Toxicol. 2008;103:546–52.
Stegall MD, Cornell LD, Park WD, Smith BH, Cosio FG. Renal allograft histology at 10 years after transplantation in the tacrolimus era: evidence of pervasive chronic injury. Am J Transplant. 2018;18:180–8.
Min SI, Kim SY, Ahn SH, Min SK, Kim SH, Kim YS, et al. CYP3A5 *1 allele: impacts on early acute rejection and graft function in tacrolimus-based renal transplant recipients. Transplantation. 2010;90:1394–400.
Billing H, Hocker B, Fichtner A, van Damme-Lombaerts R, Friman S, Jaray J, et al. Single-nucleotide polymorphism of cyp3a5 impacts the exposure to tacrolimus in pediatric renal transplant recipients: a pharmacogenetic substudy of the TWIST Trial. Therapeutic Drug Monit. 2017;39:21–28.
Almeida-Paulo GN, Dapia Garcia I, Lubomirov R, Borobia AM, Alonso-Sanchez NL, Espinosa L, et al. Weight of ABCB1 and POR genes on oral tacrolimus exposure in CYP3A5 nonexpressor pediatric patients with stable kidney transplant. Pharmacogenomics J. 2018;18:180–6.
Aouam K, Kolsi A, Kerkeni E, Ben Fredj N, Chaabane A, Monastiri K, et al. Influence of combined CYP3A4 and CYP3A5 single-nucleotide polymorphisms on tacrolimus exposure in kidney transplant recipients: a study according to the post-transplant phase. Pharmacogenomics. 2015;16:2045–54.
Niioka T, Kagaya H, Saito M, Inoue T, Numakura K, Habuchi T, et al. Capability of utilizing CYP3A5 polymorphisms to predict therapeutic dosage of tacrolimus at early stage post-renal transplantation. Int J Mol Sci. 2015;16:1840–54.
Han N, Ha S, Yun HY, Kim MG, Min SI, Ha J, et al. Population pharmacokinetic-pharmacogenetic model of tacrolimus in the early period after kidney transplantation. Basic Clin Pharm Toxicol. 2014;114:400–6.
Coto E, Tavira B, Suarez-Alvarez B, Lopez-Larrea C, Diaz-Corte C, Ortega F, et al. Pharmacogenetics of tacrolimus: ready for clinical translation? Kidney Int Suppl. 2011;1:58–62.
Zhang J, Zhang X, Liu L, Tong W. Value of CYP3A5 genotyping on determining initial dosages of tacrolimus for Chinese renal transplant recipients. Transplant Proc. 2010;42:3459–64.
Press RR, Ploeger BA, den Hartigh J, van der Straaten T, van Pelt J, Danhof M, et al. Explaining variability in tacrolimus pharmacokinetics to optimize early exposure in adult kidney transplant recipients. Ther Drug Monit. 2009;31:187–97.
Satoh S, Saito M, Inoue T, Kagaya H, Miura M, Inoue K, et al. CYP3A5 *1 allele associated with tacrolimus trough concentrations but not subclinical acute rejection or chronic allograft nephropathy in Japanese renal transplant recipients. Eur J Clin Pharmacol. 2009;65:473–81.
MacPhee IA, Fredericks S, Tai T, Syrris P, Carter ND, Johnston A, et al. The influence of pharmacogenetics on the time to achieve target tacrolimus concentrations after kidney transplantation-DL. Am J Transplant. 2004;4:914–9.
Thervet E, Anglicheau D, King B, Schlageter MH, Cassinat B, Beaune P, et al. Impact of cytochrome p450 3A5 genetic polymorphism on tacrolimus doses and concentration-to-dose ratio in renal transplant recipients. Transplantation. 2003;76:1233–5.
Turolo S, Tirelli AS, Ferraresso M, Ghio L, Belingheri M, Groppali E, et al. Frequencies and roles of CYP3A5, CYP3A4 and ABCB1 single nucleotide polymorphisms in Italian teenagers after kidney transplantation. Pharmacol Rep. 2010;62:1159–69.
Kurzawski M, Dąbrowska J, Dziewanowski K, Domański L, Perużyńska M, Droździk M. CYP3A5 and CYP3A4, but not ABCB1 polymorphisms affect tacrolimus dose-adjusted trough concentrations in kidney transplant recipients. Pharmacogenomics. 2014;15:179–88.
Acknowledgements
This work was supported by a core grant to SIUT.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Khan, A.R., Raza, A., Firasat, S. et al. CYP3A5 gene polymorphisms and their impact on dosage and trough concentration of tacrolimus among kidney transplant patients: a systematic review and meta-analysis. Pharmacogenomics J 20, 553–562 (2020). https://doi.org/10.1038/s41397-019-0144-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41397-019-0144-7
- Springer Nature Limited
This article is cited by
-
Effects of CYP3A4*22 and POR*28 variations on the pharmacokinetics of tacrolimus in renal transplant recipients: a meta-analysis of 18 observational studies
BMC Nephrology (2024)
-
The pharmacogenetics of tacrolimus in renal transplant patients: association with tremors, new-onset diabetes and other clinical events
The Pharmacogenomics Journal (2024)
-
Pharmacogenetic analysis of interleukin-10 variants and tacrolimus metabolism in kidney transplant patients from Pakistani population
Molecular Biology Reports (2024)
-
The impact of cytochrome P450 3A5 genotype on early tacrolimus metabolism and clinical outcomes in lung transplant recipients
International Journal of Clinical Pharmacy (2022)
-
The impact of IL-10 and CYP3A5 gene polymorphisms on dose-adjusted trough blood tacrolimus concentrations in early post-renal transplant recipients
Pharmacological Reports (2021)