
Abstract
Rhythm control in atrial fibrillation (AF) can be achieved using pharmacological therapy. Amiodarone is the most efficacious anti-arrhythmic agent; however, its use is limited due to an unfavourable safety profile, including pro-arrhythmia, thyroid, liver, skin and pulmonary complications. Dronedarone, which is structurally similar to amiodarone, was developed to try and achieve a favourable balance of efficacy and risk. Dronedarone has been evaluated in several large clinical trials, which have shown reduced mortality and hospitalization rates in patients with non-permanent AF. In patients with permanent AF and/or heart failure, dronedarone has been shown to cause increased mortality and morbidity and should not be used in these groups. Compared with amiodarone, dronedarone has fewer toxic effects (thyroid, skin, pulmonary) and, although less efficacious, may be used as first-line therapy for maintenance of sinus rhythm in patients with non-permanent AF. Clinicians must be vigilant in monitoring their patients to ensure they do not develop permanent AF or heart failure.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia, and gives rise to substantial mortality and morbidity due to thromboembolism and stroke [1–3]. Treatment involves stroke prevention with appropriate anticoagulation, and choosing a rate versus rhythm control strategy [4–6]. A rhythm control strategy can be achieved with pharmacological, electrical or more invasive intervention such as catheter ablation. The safety profile of anti-arrhythmic agents is a major concern to clinicians and, in particular, the risk of pro-arrhythmia. In this review we will discuss dronedarone, a relatively novel anti-arrhythmic agent, and evaluate its role in the treatment of AF. We aim to provide an overview of its benefits and risks, using all the available evidence and hope to put this drug into perspective to help guide clinicians in its appropriate use.
1.1 Literature Search Methodology
Although this is not a formal systematic review, information was obtained using the MEDLINE search engine (between January 1980 and December 2011), recent guidelines on the management of AF and recent review articles. The following search terms were used individually or in combination: ‘dronedarone’, ‘atrial fibrillation’, ‘AF’, ‘rate control’, ‘rhythm control’, ‘cardioversion’, ‘safety’, ‘risks’ and ‘adverse effects’. Only articles in English were used.
2 Types of Atrial Fibrillation (AF) and Natural Course
For the purpose of this review we refer to the different types of AF (paroxysmal, persistent and permanent) which are distinguished based on presentation and duration. Unless otherwise specified, the following definitions apply (obtained from the European Society of Cardiology guidelines for the management of AF) [5]. Paroxysmal AF refers to an episode of AF lasting up to 7 days. Persistent AF is an episode lasting more than 7 days or requiring termination by cardioversion. Permanent AF is when the presence of AF is accepted by the patient and physician, and rhythm control strategies are not pursued. Long-standing persistent AF refers to patients with AF of more than 1 year’s duration where a rhythm strategy is still to be pursued.
The distinction between long-standing persistent and permanent AF is based purely on the intention to cardiovert or remain in abnormal rhythm. The natural course of AF is such that patients usually begin with paroxysmal AF and eventually progress into permanent AF. At some point patients may become symptomatic and therefore require cardioversion, during which time they are labelled as persistent AF; therefore, it can be seen that the type of AF is not static and can change depending on the time course, symptoms and management intention.
3 Rhythm Control Strategy and Anti-Arrhythmic Agents
Large trials have determined no significant difference in mortality between rate or rhythm approach [7–11]. A significant proportion of patients will remain symptomatic despite adequate ventricular rate control and may require restoration of sinus rhythm to fully control symptoms [8–12]. Early cardioversion may also be necessary in patients when AF causes hypotension and worsening heart failure [4–6]. The main drugs available for cardioversion include amiodarone, dronedarone, flecainide, propafenone and sotalol. Other drugs such as quinidine, disopyramide, dofetilide or procainamide are available; however, their usefulness is not well established with the exception of disopyramide, which may be useful in vagally-mediated AF [4, 5].
Amiodarone is the most effective drug in maintaining sinus rhythm, and is recommended for use in patients with structural heart disease or severe heart failure [4–6]. Unfortunately, amiodarone has many adverse effects, including thyroid dysfunction, liver toxicity, photosensitivity, visual disturbances, gastrointestinal symptoms, pulmonary fibrosis and pro-arrhythmia, which have limited its use [13, 14]. It has been thought that many of the adverse effects are a result of the iodine content and prolonged half-life of the drug [13–15].
The ideal anti-arrhythmic agent for the treatment of AF would need to be effective at cardioversion and maintenance of sinus rhythm, with minimal adverse effects. Dronedarone, structurally similar to amiodarone but without iodine, was developed to try and achieve this balance. It was approved for the treatment of AF by the US FDA [16] in July 2009 and by the European Medicines Agency [17] (EMA) in December 2009. The FDA approved dronedarone to “reduce the risk of cardiovascular hospitalization in patients with paroxysmal or persistent AF/atrial flutter (AFl), with a recent episode of AF/AFl and associated cardiovascular risk factors (including age >70 years, hypertension, diabetes, prior cerebrovascular accident, left atrial diameter ≥50 mm or left ventricular ejection fraction [LVEF] <40 %), who are in sinus rhythm or who will be cardioverted” [18]. In December 2011 a warning was added to the product labelling and dronedarone was contraindicated in patients with heart failure (New York Health Association [NYHA] class IV or class II–III and recent decompensation requiring hospitalization or referral to a specialized heart failure clinic). This warning was added following evidence from a large clinical trial (which will be discussed later in this review) which showed that dronedarone doubled the mortality in this group of patients [19].
The EMA approved dronedarone in adult clinically stable patients with non-permanent AF to prevent the recurrence of AF or to lower the ventricular rate. In September 2011, further safety messages were added that [20]:
-
dronedarone should not be used in patients with NYHA class IV or unstable class III;
-
dronedarone is not recommended in patients with recent (1–3 months) stable NYHA class III or with LVEF <35 %;
-
liver function tests should be performed prior and during treatment.
4 Pharmacological Properties
The structural, electrophysiological and pharmacological properties of dronedarone are summarized in Tables 1 and 2. In Table 2, comparisons are made with amiodarone because of the following: (i) historically, dronedarone was developed from amiodarone to try and overcome its unfavourable safety profile; (ii) clinicians may view dronedarone as a direct alternative to amiodarone in the management of AF; and (iii) amiodarone is the only antiarrhythmic that has been compared with dronedarone in a robust clinical trial (see Sect. 4) [21].
4.1 Structure and Electrophysiological Effects
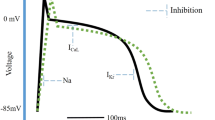
Dronedarone (N-[2-butyl-3[4-(3-dibutylaminopropoxy)benzoyl]-benzofurane-5-yl]methane-sulfonamide hydrochloride) is a non-iodinated benzofuran derivative of amiodarone, which was synthesized by removal of iodine and addition of a methane-sulfonyl group [20, 22] (see fig. 1). Unsurprisingly, dronedarone has similar electrophysiological properties to amiodarone [20, 23–27] (see Table 1) and fulfills all four classes of the Vaughan-Williams classification. Dronedarone is a multichannel inhibitor: potent fast Na+ channel current inhibitor [28] (class I); potent acetylcholine-activated K+ current inhibitor [29] (class III); other K+ current inhibition [delayed-rectifier, slowly activated delayed-rectifier and inward-rectifier K+ current] [30–33] (class III); and L-type Ca2+ current inhibitor [30–34] (class IV). It has α- and β-adrenoreceptor antagonist activity [35–37] (class II), and delays the cardiac action potentials and refractoriness [23, 38, 39]. Its effects result in sinus rate slowing [23, 29, 38], prolongation of the PR interval and mild QTc prolongation [37, 39]. Importantly, in animals, dronedarone has been shown to reduce ischaemia-induced ventricular arrhythmias [23, 40–42].

Chemical structure of dronedarone compared with amiodarone
4.2 Pharmacokinetics
Overall, 70–94 % of dronedarone is absorbed following oral administration. The bioavailability of dronedarone increases 2- to 3-fold when taken with food. It has low absolute bioavailability (15 %) as it undergoes hepatic first-pass metabolism via the cytochrome P450 (CYP) mechanism, and therefore twice-daily regimens are required to maintain steady-state concentrations [47]. Six percent is excreted through the kidney and does not pass the blood-brain barrier nor the placenta; however, it is excreted in breast milk [45, 46]. Dronedarone and its metabolites are heavily protein-bound and have a volume of distribution of 1.2–1.4 L [45, 47–49]. Steady-state concentrations are reached in 7 days, and the half-life is 13–31 hours, which is much reduced compared with amiodarone [45, 47–49] (half-life 10–40 days; see Table 2). Dronedarone can cause a 10–20 % rise in serum creatinine levels, but does not affect glomerular filtration rate [50]. The recommended dose is 400 mg twice-daily orally (initiation and maintenance); one tablet with the morning meal and one with the evening meal [17, 18]. There are no intravenous preparations of dronedarone, and there are no dose adjustments for age, kidney function, ethnicity or sex [51].
5 Efficacy
In this section we will evaluate the efficacy of dronedarone in the treatment of AF as determined from clinical trials (see Tables 3 and 4). Studies have demonstrated a number of benefits, which include conversion to sinus rhythm; prevention of AF recurrence after successful cardioversion; ventricular rate-slowing; blood pressure (BP) lowering; reductions in hospitalizations due to cardiovascular events; and reductions in mortality.
5.1 DAFNE 2003
The Dronedarone Atrial Fibrillation study after Electrical Cardioversion (DAFNE) was a double-blind, randomized, placebo-controlled trial designed to select the most appropriate dose of dronedarone for the prevention of recurrent AF after successful cardioversion [59]. Overall, 270 patients with persistent AF from 50 centres in 11 countries were randomized to receive placebo or dronedarone in doses of either 800 mg, 1200 mg or 1600 mg daily (400 mg, 600 mg or 800 mg twice daily), and all underwent electrical cardioversion. Of 270 patients, 199 were successfully restored to sinus rhythm and continued treatment for 6 months.
The average age of patients included was around 60 years, with the majority being male (57–79 %), around half with hypertension and just under one-fifth with heart failure. Patients in the four groups had similar characteristics.
5.1.1 Prevention of Recurrent AF After Successful Cardioversion
The primary endpoint was time to first AF recurrence, which was significantly greater in patients receiving 800-mg dronedarone than placebo. The median time to first AF recurrence was 5.3 days in the placebo group and 60 days in the dronedarone 800-mg group (relative risk reduction 55 %; 95 % CI 72–28 %; p = 0.001). In the 800-mg group, 35 % of patients remained in sinus rhythm at 6 months, compared with 10 % in the placebo group. There were similar outcomes in the intention-to-treat analysis, with time to AF recurrence of 56 days in the dronedarone 800-mg group compared with 5.3 days in the placebo group. There was no significant difference in time to AF recurrence in the other doses of dronedarone compared with placebo, which is interesting as it suggests there is no dose effect.
5.1.2 Conversion to Sinus Rhythm
Rates of spontaneous cardioversion were higher in patients receiving dronedarone compared with placebo. Furthermore, this relationship appeared to be dose-related with increasing effect at higher doses. Cardioversion rates were 5.8 %, 8.2 % and 14.8 % in patients receiving dronedarone 800 mg, 1200 mg and 1600 mg, respectively, compared with 3.1 % in the placebo group. In this study, dronedarone was not shown to significantly affect the rates of electrical cardioversion, which were 73 % in the placebo group compared with 77.3 %, 87.9 % and 76.6 % in patients receiving dronedarone 800 mg, 1200 mg and 1600 mg, respectively.
5.1.3 Slowing of Ventricular Rate
In patients receiving dronedarone, a significant ventricular rate-slowing effect was seen following AF recurrence, which increased with higher doses. The ventricular rate slowed by 13.2, 19.2 and 17.8 beats per minute (bpm) in the 800 mg, 1200 mg and 1600 mg groups, respectively, compared with placebo (p = 0.0001).
5.2 EURIDIS/ADONIS 2007
The European Trial in Atrial Fibrillation or Flutter Patients receiving Dronedarone for the maintenance of Sinus Rhythm (EURIDIS) and the American-Australian-African Trial with Dronedarone in Atrial Fibrillation or Flutter Patients for the Maintenance of Sinus Rhythm (ADONIS) were identical, placebo-controlled, multicentre, double-blind, parallel-group trials conducted in 17 countries worldwide [51]. The trials were designed to evaluate the efficacy of dronedarone in the management of patients with non-valvular AF. To qualify for the study patients had to have had at least one episode of AF within the preceding 3 months and were in sinus rhythm for at least 1 hour before randomization. Exclusion criteria included permanent AF, torsades de pointes, bradycardia, heart failure or taking class I or III antiarrhythmic agents.
Overall, 612 (EURIDIS) and 625 (ADONIS) patients were randomized to receive either dronedarone 400 mg twice daily or placebo. The mean age of patients was 63 years, approximately 70 % were male, 41 % had structural heart disease and 57 % had hypertension.
5.2.1 Prevention of Recurrent AF
In EURIDIS, the primary endpoint was time from randomization to the first documented recurrence of AF, which, in the modified intention-to-treat analysis, occurred after 96 days (median) in the dronedarone group compared with 41 days in the placebo group. Following 1 year, 67.1 % of patients in the dronedarone group and 77.5 % of patients in the placebo group had a recurrence of AF (hazard ratio [HR] 0.78; 95 % CI 0.64–0.96; p = 0.01). The on-treatment analysis had similar results (p = 0.01).
In ADONIS, in the modified intention-to-treat analysis, the median times from randomization to documented AF recurrence were 158 days in the dronedarone group compared with 59 days in the placebo group. After 12 months, 61.1 % of patients in the dronedarone group had a recurrence of AF compared with 72.8 % of patients in the placebo group (HR 0.73; 95 % CI 0.59–0.89; p = 0.002). Once again there were similar results in the on-treatment analysis (p = 0.002).
When data from both trials were combined, the median times to documented AF recurrence were 116 days in the dronedarone group compared with 53 days in the placebo group. After 12 months, rates of AF recurrence were 64.1 % in the dronedarone group compared with 75.2 % in the placebo group (HR 0.75; 95 % CI 0.65–0.87; p < 0.001). In these analyses, patients who discontinued dronedarone or who had an AF recurrence within 5 days were not included. Furthermore, rates of symptomatic AF recurrence were less in the dronedarone group (37.7 %) compared with placebo (46.0 %; HR 0.71; 95 % CI 0.60–0.86; p < 0.001).
5.2.2 Slowing of Ventricular Rate
In patients with AF recurrence, the mean ventricular rate ± standard deviation (SD) was found to be slower in patients taking dronedarone (103 ± 25.9 bpm) compared with placebo (117.1 ± 30.4 bpm; p < 0.001).
5.2.3 Reduced Hospitalization or Death
A post hoc analysis was performed. In EURIDIS, 21.2 % of patients in the dronedarone group had been hospitalized or died at 12 months, compared with 32.0 % of patients in the placebo group (HR 0.66; 95 % CI 0.47–0.93; p = 0.02). In ADONIS, rates of hospitalization or death in the dronedarone group were 24.5 % compared with 29.8 % in the placebo group (HR 0.80; 95 % CI 0.56–1.14; p = 0.22). In the combined analysis, rates of hospitalization or death in the dronedarone group were 22.8 % compared with 30.9 % in the placebo group (HR 0.73; 95 % CI 0.57–0.93; p = 0.01).
5.3 ERATO 2008
The Efficacy and Safety of Dronedarone for the Control of Ventricular Rate during Atrial Fibrillation (ERATO) study was a randomized, double-blind, placebo-controlled, parallel-group, multicentre study conducted in nine European countries [60]. ERATO was designed to assess the efficacy of dronedarone in the control of ventricular rate in patients with permanent AF (>6 months’ duration), when added to standard therapy. Patients included in this trial had symptomatic, permanent AF where cardioversion was not considered an option. Overall, 174 patients were randomized to receive 6 months’ treatment with dronedarone 400 mg twice daily or matching placebo, and assessed using 24-hour holters at days 0 and 14 and 4 months following treatment. Patients were also assessed using exercise tolerance tests at days 0 and 14. The mean age of patients was approximately 65 years, approximately 68 % were male, approximately 50 % had hypertension, approximately 40 % had structural heart disease and approximately 50 % had concomitant β-blockers (excluding sotalol).
5.3.1 Slowing of Ventricular Rate
In ERATO, dronedarone treatment resulted in a reduced ventricular rate compared with placebo. The mean ventricular rate after 2 weeks was reduced by 11.0 bpm in the dronedarone group compared with an increase of 0.7 bpm in the placebo group (p < 0.001). Patients receiving concomitant rate-lowering drugs were also found to have a reduced ventricular rate with dronedarone. In patients receiving dronedarone, mean ventricular rates were reduced by 14.9, 11.5 and 5.1 bpm in those receiving concomitant β-blockers, digoxin and calcium channel blockers, respectively, compared with placebo. In the 4-month analysis, a sustained reduction in mean ventricular rate was seen in patients receiving dronedarone (10.1 bpm) compared with placebo (1.3 bpm; p < 0.001). Similarly, there was a reduction in heart rate in patients receiving concomitant rate-lowering therapy.
In the per-protocol analysis, the mean ventricular rate was reduced by 12.3 bpm (95 % CI −14.6 to −10.0 bpm) after 14 days in the dronedarone group compared with an increase of 0.4 bpm in the placebo group (95 % CI −2.2 to 2.9; p < 0.001).
The rate-lowering effect was also observed during exercise testing with reductions of 25.6 (submaximal exercise) and 27.4 bpm (maximal exercise) in the dronedarone group compared with 2.2 (submaximal) and 2.9 bpm (maximal) in the placebo group (p < 0.001). Importantly, there was no reduction in exercise tolerance in the dronedarone group.
5.4 ATHENA 2009
ATHENA (A Placebo-Controlled, Double-Blind, Parallel Arm Trial to Assess the Efficacy of Dronedarone 400 mg bid for the Prevention of Cardiovascular Hospitalization or Death from Any Cause in Patients with Atrial Fibrillation/Atrial Flutter) was conducted in 37 countries between 2005 and 2007 [61]. A total of 4628 patients with paroxysmal AF or atrial flutter were included with at least one of the following requirements: age of at least 70 years; arterial hypertension (treated with at least two antihypertensive drugs); diabetes mellitus; previous stroke; transient ischaemic attack, or thromboembolism; left atrial diameter greater than or equal to 50 mm; and LVEF ≤40 %. The mean follow-up period was 21 months. Primary outcome measures included first hospitalization due to cardiovascular event or death from any cause. During the course of the study, the overall mortality figures were lower than expected and therefore the inclusion criteria was changed to include higher risk patients (minimum age of 70 years). The mean age was 71.6 years, approximately 53 % were male, approximately 86 % had hypertension and approximately 60 % had structural heart disease. Approximately 4 % and approximately 12 % had LVEF less than 35 % and 45 %, respectively, and around 70 % had concomitant β-blockers.
5.4.1 Reduced Hospitalization Due to Cardiovascular Event or Death
In the dronedarone group, 31.9 % of patients had a primary outcome event compared with 39.4 % in the placebo group (HR 0.76; 95 % CI 0.69–0.84; p < 0.001). In the dronedarone group, there were 116 deaths (5.0 %) compared with 139 (6.0 %) in the placebo group (HR 0.84; 95 % CI 0.66–1.08; p = 0.18).
In the dronedarone group, 29.3 % of patients had a first hospitalization due to cardiovascular event compared with 36.9 % of patients receiving placebo (HR 0.74; 95 % CI 0.67–0.82; p < 0.001).
With regard to all outcome events (hospitalization due to any cardiovascular event or death from any cause), there were fewer events in the dronedarone group (54.5 %) compared with placebo (71.7 %; HR 0.76; 95 % CI 0.68–0.84; p < 0.001).
In a post hoc analysis of ATHENA, EURIDIS and ADONIS, dronedarone was found to reduce the risk of cardiovascular hospitalization or death by 44 % in patients with lone AF (HR 0.56; 95 % CI 0.36–0.88; p = 0.004) [62].
5.4.2 Reduced Death from Cardiovascular Causes
Deaths due to a cardiovascular cause occurred in 2.7 % of patients taking dronedarone compared with 3.9 % of patients in the placebo group (HR 0.71; 95 % CI 0.51–0.98; p = 0.03). Deaths due to cardiac arrhythmia occurred in 1.1 % of patients receiving dronedarone compared with 2.1 % receiving placebo (HR 0.55; 95 % CI 0.34–0.88; p = 0.01).
5.4.3 Reduced Hospitalization Due to AF or Acute Coronary Syndrome
Further analysis showed that the reduction in hospitalization was mainly driven by a reduction in AF (14.6 vs 21.9 % dronedarone vs placebo; HR 0.63; 95 % CI 0.55–0.72; p < 0.01). There were also significantly less hospitalizations due to acute coronary syndrome with dronedarone compared with placebo (2.7 vs 3.8 %, respectively; HR 0.70; 95 % CI 0.51–0.97; p = 0.03). There were no significant differences in the number of hospitalizations for heart failure or ventricular arrhythmia or non-fatal cardiac arrests in both groups.
5.5 DIONYSOS 2010
The Randomized, Double-Blind Trial to evaluate the Efficacy and Safety of Dronedarone (400 mg bid) Versus Amiodarone (600 mg qd for 28 days, then 200 mg qd thereafter) for at least 6 months for the maintenance of sinus rhythm in patients with AF (DIONYSOS) was a short-term study comparing dronedarone and amiodarone [21]. The investigators aimed to provide a direct comparison of benefit-to-risk ratio of dronedarone and amiodarone, recruiting patients with documented AF (>72 hours’ duration) for whom cardioversion and anti-arrhythmic drugs were indicated. The trial was conducted in 112 centres in 23 countries with 504 patients randomized to receive either dronedarone or amiodarone. Patients underwent electrical cardioversion between 10 and 28 days following treatment, unless they had spontaneously reverted to sinus rhythm. The mean age was 64 years, approximately 70 % were male, 67 % had hypertension, 29 % had structural heart disease and approximately 22 % had chronic heart failure.
The primary endpoints included a measure of efficacy (recurrence of AF, or premature discontinuation of drug due to lack of efficacy), and a measure of safety (premature discontinuation of drug due to intolerance). For the purpose of analysis, treatment failure included AF recurrence, unsuccessful electrical cardioversion plus no spontaneous cardioversion and no electrical cardioversion. The main safety endpoint included thyroid, hepatic, pulmonary, neurologic, skin, eye or gastrointestinal specific events, or premature discontinuation due to an adverse event.
The composite primary endpoint, which included time to first AF recurrence or premature drug discontinuation, occurred more frequently in the dronedarone group (75.1 %) compared with amiodarone (58.8 %; HR 1.59; 95 % CI 1.28–1.98; p < 0.001) following 12 months of treatment.
5.5.1 Prevention of Recurrent AF After Successful Cardioversion/Conversion to Sinus Rhythm
The rates of AF recurrence (including lack of cardioversion) occurred more frequently in the dronedarone group (63.5 %) compared with amiodarone (42.0 %). There were fewer spontaneous cardioversions in the dronedarone group (29) compared with the amiodarone group (83). Consequently, there were more electrical cardioversions performed in the dronedarone group. The number of unsuccessful cardioversions was higher in the dronedarone group (29 vs 16); however, this may be explained by the higher numbers of patients undergoing electrical cardioversion in the dronedarone group (200 vs 153) as the proportion of successful cardioversions was similar in both groups (83.0 vs 85.6 %).
5.5.2 Reducing Blood Pressure (BP)
Dronedarone was found to have a BP-lowering effect compared with amiodarone. The mean change from diastolic BP was −2.04 mmHg with dronedarone compared with −0.32 mmHg with amiodarone (p = 0.0068). The mean change from systolic BP was +1.55 mmHg with dronedarone compared with +6.58 mmHg with amiodarone (p < 0.0001).
5.6 PALLAS 2011
The Permanent Atrial Fibrillation Outcome Study Using Dronedarone on Top of Standard Therapy (PALLAS) was a randomized, double-blind, placebo-controlled trial conducted in 37 countries [19]. The primary outcome measures included a combination of stroke, myocardial infarction, systemic embolism or death from cardiovascular causes, and are discussed in Sect. 6. Other outcome measures included death from non-cardiovascular causes and rates of hospitalization. A total of 3236 patients with permanent AF were randomized to receive either dronedarone (400 mg twice daily) or placebo. The study was stopped early due to safety concerns. In both groups the mean age was 75 years, and approximately 69 % of patients had a >2 year history of permanent AF or atrial flutter. Two-thirds of patients had heart failure, 88 % were receiving rate-lowering therapy (one-third receiving digoxin) and 84 % were receiving a vitamin K antagonist (VKA).
5.6.1 Conversion to Sinus Rhythm
At 4 months, 3.7 % of patients in the dronedarone group were in sinus rhythm compared with 1.4 % in the placebo group (p = 0.01).
5.6.2 Slowing Ventricular Rate
At 1 month, the mean heart rate (±SD) was reduced by 7.6 ± 14.5 bpm in the dronedarone group, compared with an increase of 0.1 ± 14.0 in the placebo group (p < 0.001).
5.6.3 Reducing BP
At 1 month, the mean reduction in systolic BP was 3.5 ± 16.1 mmHg in the dronedarone group compared with 1.7 ± 16.1 mmHg in the placebo group (p = 0.003).
6 Risk Assessment
In this section, we have used data from the seven large clinical trials [19, 21, 51, 59–61, 63], of which only one was a direct comparison with amiodarone (DIONYSOS) [21].
6.1 Heart Failure
The Antiarrhythmic Trial with Dronedarone in Moderate to Severe Chronic Heart Failure Evaluating Morbidity Decrease (ANDROMEDA) was a double-blind, placebo-controlled, randomized, parallel-group trial conducted at 72 hospitals [63]. The study randomly assigned 627 patients with symptomatic heart failure and severe left ventricular (LV) systolic dysfunction to receive either dronedarone 400 mg twice daily or placebo. The median age of patients was approximately 71 years, and approximately three-quarters were male. Around one-third of patients had hypertension, approximately 30 % of patients had dilated cardiomyopathy and approximately 60 % were taking β-blockers. Almost 60 % of patients were classified as New York Heart Association (NYHA) class III and the mean duration of heart failure was approximately 20 months.
The primary endpoint was the composite of death from any cause or hospitalization for heart failure. The study was stopped prematurely after 7 months because of safety concerns. During the median 2 months’ follow–up, 25 patients in the dronedarone group (8.1 %) died compared with 12 patients in the placebo group (3.8 %; HR 2.13; 95 % CI 1.07–4.25; p = 0.03). The higher mortality in the dronedarone group was attributed to worsening heart failure, which occurred in ten patients in the dronedarone group compared with two patients in the placebo group.
In PALLAS there was a significantly higher risk of hospitalization due to heart failure in patients receiving dronedarone compared with placebo (HR 1.81; 95 % CI 1.10–2.99; p = 0.02) [19]. However, a sub-study analysis found similar risks of both primary outcomes (combination of stroke, myocardial infarction, systemic embolism or death from cardiovascular causes) and hospitalization for heart failure in patients with an LVEF lower than 40 % compared with those with an ejection fraction >40 %.
In prior studies, rates of heart failure were low with only 38 out of 3604 patients (approximately 1 %) reported to have heart failure as a consequence of dronedarone therapy [21, 51, 59–61]. In ATHENA, 92 patients with LV ejection fraction <35 %, and 464 patients with NYHA class II–III received dronedarone; however, death from cardiovascular causes occurred less frequently in the dronedarone group (2.7 %) compared with placebo (3.9 %; HR 0.71; 95 % CI 0.51–0.98; p = 0.03) [61]. There was no significant difference in rates of first hospitalization due to congestive cardiac failure in the dronedarone group (4.9 %) compared with placebo (5.7 %; HR 0.86; 95 % CI 0.67–1.10; p = 0.22).
Further discussion can be found in Sect. 8.
6.2 Permanent AF
In ERATO, the first study to include patients with permanent AF (≥6 months’ duration), dronedarone was found to be generally well tolerated with no major adverse effects. During the study, one sudden death was reported in the dronedarone group (a female patient with congenital heart disease and family history of sudden death) and two further deaths occurred following trial completion (one in the dronedarone group), although these were considered unrelated to trial participation. This study suggested dronedarone may be safe in patients with permanent AF, however it was far from conclusive: ERATO was a short study (duration of dronedarone was only 6 months) with relatively few patients (85 patients).
The role of dronedarone in permanent AF was further investigated in PALLAS, however the study was discontinued early due to safety concerns [19].
The first co-primary event (composite of stroke, myocardial infarction, systemic embolism or death from cardiovascular disease) occurred in 43 patients receiving dronedarone compared with 19 in the placebo group (HR 2.29; 95 % CI 1.34–3.94; p = 0.002). The second co-primary event (composite of unplanned hospitalization for cardiovascular causes or death) occurred in 127 patients receiving dronedarone compared with 67 patients receiving placebo (HR 1.95; 95 % CI 1.45–2.62; p < 0.001).
There were 25 deaths in the dronedarone group compared with 13 in the placebo group (HR 1.94; 95 % CI 0.99–3.79; p = 0.049). Of these deaths, 21 were due to cardiovascular causes in the dronedarone group compared with 10 in the placebo group (HR 2.11; 95 % CI 1.00–4.49; p = 0.046). In the dronedarone group there were 13 deaths due to arrhythmia compared with 4 in the placebo group (HR 3.26; 95 % CI 1.06–10.00; p = 0.03).
Stroke occurred in 23 patients receiving dronedarone compared with 10 in the placebo group (HR 2.32; 95 % CI 1.11–4.88; p = 0.02). Unplanned hospitalization for cardiovascular causes occurred in 113 patients receiving dronedarone compared with 59 patients in the placebo group (HR 1.97; 95 % CI 1.44–2.70; p < 0.001).
Hospitalization due to heart failure occurred in 43 patients in the dronedarone group compared with 24 in the placebo group (HR 1.81; 95 % CI 1.10–2.99; p = 0.02). Of note, there was no significant difference in the rates of myocardial infarction or systemic embolism in both groups, which occurred infrequently.
A sub-study analysis found consistent results across the sub-groups with regard to both co-primary outcomes. However, analysis of the secondary outcomes (hospitalization for cardiovascular causes or death) showed that patients with diabetes had a greater risk in the dronedarone group compared with patients without diabetes (p = 0.03 for interaction).
Patients with LVEF lower than or greater than 40 % had a similar risk of both primary outcomes and hospitalization for heart failure. The same was true for patients with NYHA symptoms classes II and III.
The results from PALLAS suggest that dronedarone causes increased mortality (mainly due to pro-arrhythmia and strokes) and hospitalization (mainly due to heart failure) in patients with permanent AF and increased risk of vascular events, and therefore should not be used in this group.
6.3 Adverse Effects
Dronedarone was found to be well tolerated, with only approximately 13 % of patients discontinuing the drug prematurely [19, 21, 51, 59–61] (see Table 5). The main complaint was gastrointestinal events, with diarrhoea being the most common. Dronedarone was found to be better tolerated than amiodarone with less premature discontinuations. The traditional adverse effects seen with amiodarone, including thyroid dysfunction, photosensitivity or pulmonary fibrosis, were rare in dronedarone [63].
6.3.1 Cardiovascular
There was one case of torsades de pointes tachycardia reported in a female patient receiving dronedarone, which occurred following resuscitation from out-of-hospital ventricular fibrillation [61]. An implantable defibrillator was inserted and she was discharged home.
Dronedarone was found to prolong QT/QTc interval significantly more than placebo and significantly less than amiodarone. Prolongation of the PR interval occurred more significantly with dronedarone compared with placebo, and the effect was greater with increasing doses. The incidence of peripheral oedema, dyspnoea, PR and QT/QTc prolongation and bradycardia was statistically significantly higher in patients receiving dronedarone compared with placebo; however, they did not occur frequently. In clinical trials of dronedarone, pro-arrhythmia (bradycardia, ventricular or supraventricular arrhythmia) was rarely seen with the exception of PALLAS where there were significantly more deaths due to arrhythmia in the dronedarone group compared with placebo [19, 21, 51, 59–61].
Heart failure is discussed earlier; however, excluding PALLAS and ANDROMEDA, occurred infrequently [51, 59–61]. In ANDROMEDA, when events resulting in death were excluded, around 22 % of patients in the dronedarone group reported cardiac events that were mainly driven by heart failure (10 %) [63]; However, these rates did not reach statistical significance when compared with placebo.
6.3.2 Gastrointestinal
In the DAFNE study, the main cause for cessation of dronedarone was due to gastrointestinal symptoms, which included diarrhoea, vomiting, nausea and gastroenteritis [59]. In the other trials, gastrointestinal effects were common. In DIONYSOS, there were more cases of gastrointestinal events in the dronedarone group (12.9 %) compared with the amiodarone group (5.1 %); however, none were serious [40]. In the dronedarone group, 9.2 % of patients had at least one episode of diarrhoea compared with 3.1 % in the amiodarone group, lasting a median of 7.0 and 4.0 days, respectively. Diarrhoea was reported four times more in the dronedarone group (8 %) compared with amiodarone (2 %).
6.3.3 Renal Events
In the large clinical trials, an increase in serum creatinine was seen in approximately 3 % of patients [19, 21, 51, 59–61]. There was a similar increase in serum creatinine levels in patients receiving amiodarone and dronedarone (mean increase of 10 μmol/L), which normalized 10–15 days following discontinuation in the dronedarone group and persisted in the amiodarone group [21].
6.3.4 Hepatic Events
Hepatic impairment was found to occur in approximately 3 % (0.5–12 %) of patients taking dronedarone; however, this was not statistically significant when compared with placebo or amiodarone [21, 51, 59, 63].
The FDA issued a safety communication following two cases of patients with dronedarone-induced acute liver failure requiring liver transplantation [64]. They advised clinicians to check liver function prior to initiating dronedarone and to continually monitor liver enzymes for at least 6 months after.
6.3.5 Other Events
Other reported events included central nervous system (dizziness, insomnia, paraesthesia), respiratory (dyspnoea, cough), dermatology (skin rash, discolouration) and thyroid dysfunction (hyper- and hypothyroidism). However, these were not significantly more frequent in patients taking dronedarone compared with placebo. There were fewer thyroid and neurological events in patients receiving dronedarone compared with amiodarone (thyroid 0.8 vs 5.9 %; neurological 1.2 vs 6.7 %) [21].
6.4 Drug Interactions
Dronedarone has several important drug interactions that clinicians will need to be aware of; for example, interactions with drugs using the CYP systems. Dronedarone is highly metabolized by CYP3A4 and is also a moderate inhibitor [20]. Potent CYP3A4 inhibitors such as antifungals, macrolide antibiotics and protease inhibitors will increase plasma levels of dronedarone causing toxicity and therefore should not be co-administered. Moderate inhibitors of CYP3A4 such as verapamil and diltiazem may be used cautiously with dronedarone. Simvastatin is metabolized with CYP3A and concomitant use with dronedarone will increase simvastatin levels. Dronedarone is a weak inhibitor of CYP2D6 [47]. β-blockers such as metoprolol are metabolized with CYP2D6 and result in increased β-blocker levels if used with dronedarone. Dronedarone is a p-glycoprotein inhibitor which, if used with digoxin or dabigatran (metabolized with p-glycoprotein), will result in increased digoxin or dabigatran levels. Therefore, reduced doses of calcium channel blockers, simvastatin, β-blockers, digoxin (half-dose) and dabigatran are advised [65].
In the large clinical trials, dronedarone was found to increase digoxin levels; however, this did not result in toxicity [19, 21, 60]. In PALLAS, patients receiving digoxin were found to have higher plasma concentrations 7 days following therapy in the dronedarone group compared with placebo (1.2 ± 0.8 vs 0.9 ± 0.6 ng/mL, respectively; p < 0.001) [19]. A similar change in digoxin levels was found with amiodarone [21].
Dronedarone does not appear to interact significantly with oral anticoagulants (OAC) as there was no effect seen on international normalized ratios (INR) of patients receiving OAC [60]. In contrast, amiodarone appeared to interact with OAC as there was a higher proportion of patients with elevated INR (>4.5) with amiodarone compared with dronedarone, and more frequent dose adjustments [21]. There were fewer haemorrhagic events in patients taking dronedarone and fewer patients with low haemoglobin levels (1.3 %) compared with amiodarone (4.7 %).
8 Place in Therapy
Before discussing the place of dronedarone in the management of AF we must first address some inconsistent findings between the studies. As previously stated, in earlier studies [51, 61] dronedarone was found to reduce the risk of cardiovascular hospitalization or death in patients with non-permanent AF. However, in more recent studies [19, 63] dronedarone was found to cause increased mortality, worsening heart failure, more strokes [19] and more cardiovascular hospitalizations.
8.1 Role in Heart Failure
In ATHENA the primary outcome was any cardiovascular hospitalization or death from any cause, which was found to be significantly less in patients receiving dronedarone [61]. However, further inspection suggests that dronedarone may not have such beneficial effects in heart failure as would first appear. The first point to note is that there was no significant reduction in all-cause mortality. Secondly, although there was a reduction in cardiovascular mortality, this was driven by a reduction in deaths due to cardiac arrhythmia (HR 0.55; 95 % CI 0.34–0.88; p = 0.01). Thirdly, although there was a reduction in first hospitalization due to cardiovascular causes, this was driven by reductions in AF and acute coronary syndrome-related hospitalizations, with no significant reduction in first hospitalization due to heart failure. The sub-group analysis of patients with heart failure (approximately 20 %) showed similar results. This study supports the finding that dronedarone has good anti-arrhythmic effects (maintenance of sinus rhythm and prevention of cardiac arrhythmias).
The results of ANDROMEDA were opposite to those of prior studies that had shown that dronedarone could have effects potentially beneficial to patients with heart failure: rate-lowering effect, mild BP-lowering effect, anti-adrenergic effect and a ventricular arrhythmia-suppressing effect. A reduction in mortality was expected, however the opposite occurred: dronedarone was found to double the risk of all-cause mortality. Almost all deaths were due to cardiovascular causes and were predominantly due to worsening heart failure and arrhythmias. To try and place these findings into context we must understand the group of patients studied and scrutinize the results further.
The main differences between ATHENA and ANDROMEDA are as follows. ATHENA was a study of 4628 patients with non-permanent AF (defined as an ECG showing AF or atrial flutter, and a second ECG showing sinus rhythm within 6 months prior to randomization), of whom around 20 % (approximately 900) had stable heart failure (with no recent decompensation within 4 weeks prior to randomization, and NYHA class I–III). ANDROMEDA was a study of 627 patients with unstable heart failure (recent hospitalization with new or worsening heart failure with NYHA class II–IV), of whom one-quarter (approximately 150) had AF (type unspecified) at randomization. In comparing these studies we are comparing approximately 900 patients with non-permanent AF and stable heart failure (ATHENA) with approximately 150 patients with unspecified AF and unstable heart failure (ANDROMEDA). At the time of randomization it appears that patients in ANDROMEDA were not optimally treated for heart failure, with 88 % receiving an ACE inhibitor or angiotensin-receptor blocker (ARB), 62 % receiving a β-blocker and 42 % receiving spironolactone. Given the majority of patients were in NYHA class II–III, there was scope for further optimization of heart failure therapy.
It is believed that the main cause for the increased mortality found in ANDROMEDA was the instability of patients recruited (recent onset or worsening of heart failure). It has also been suggested that the study was discontinued too prematurely and therefore was not statistically powered to draw major conclusions. The number of deaths was small (25 in the dronedarone group vs 12 in placebo), which has led to some believing that if the study had continued the mortality rates may have evened out. To further support this, when events resulting in death were excluded, similar rates of cardiac events (including heart failure) were seen in both groups (any cardiac event dronedarone vs placebo, 21.9 vs 16.4 %; heart failure event 10.0 vs 8.2 %).
Following ANDROMEDA, the FDA added a warning label to the product labelling for dronedarone contraindicating its use in heart failure NYHA class III–IV, or unstable NYHA class II [16].
8.2 Role in Permanent AF
PALLAS showed that dronedarone had deleterious effects in high-risk patients with permanent AF (almost double the death rate, double cardiovascular deaths, 3-fold increase in arrhythmia-associated deaths, double stroke rate and almost double hospitalizations due to heart failure) [19]. In PALLAS, permanent AF was defined as an ECG showing AF 14 days prior to randomization, and a second ECG showing AF 6 months or more prior to randomization. The conventional timescale for the definition of permanent AF is 1 year; therefore, it is possible that some of the patients recruited may not have had permanent AF in the strictest sense. However, this is unlikely to be the explanation as the majority of patients (70 %) had AF for a duration of more than 2 years. The increased stroke rate could not be attributed to a lack of oral anticoagulation (84 % of patients were receiving VKA). The increased hospitalizations due to heart failure also cannot be explained. In PALLAS, around 15 % of patients had symptomatic heart failure at randomization, with around 20 % reported to have an LVEF ≤40 %. Although this study was stopped early a large number of patients had already been enrolled, unlike ANDROMEDA. Therefore, it is unlikely that these findings were due to chance. Digoxin toxicity may have had a role in the increased mortality and arrhythmia risk. As mentioned previously, digoxin can interact with dronedarone, resulting in increased levels of digoxin. In PALLAS, a 33 % increase in digoxin serum levels (0.9–1.2 ng/mL) was reported, and a previous study showed that digoxin levels >1.2 ng/mL was associated with increased cardiovascular deaths [66].
It is unclear why dronedarone would cause such negative effects in permanent AF whilst having favourable outcomes in non-permanent AF. Our current understanding of AF is that permanent and non-permanent is the same disease pathology but that permanent AF is at a more advanced stage. However, the results of PALLAS may suggest that perhaps they are not the same but rather two distinct disease processes. Further work is required to fully understand permanent AF.
In light of the findings from PALLAS, the FDA updated the warning label contraindicating dronedarone for use in patients with atrial fibrillation who will not or cannot be cardioverted into sinus rhythm, i.e. patients with permanent AF [67].
8.3 Role in Non-Permanent AF
Dronedarone is licensed for use in patients with non-permanent AF [18, 20]. American and European guidelines recommend dronedarone to reduce cardiovascular hospitalizations in patients with paroxysmal AF or following cardioversion of persistent AF [4, 5]. Dronedarone is not as efficacious as amiodarone [21, 68] but because it lacks the toxicity of amiodarone it is recommended as first-line therapy (alongside other agents) in these patients with no (or minimal) heart disease, hypertension (without substantial LV hypertrophy) and coronary artery disease (see fig. 2).

Suggested use of dronedarone in the maintenance of sinus rhythm in patients with non-permanent atrial fibrillation, according to disease pathology. Drugs are listed in alphabetical order and do not represent the order of recommended use. Adapted from Wann et al., with permission [4]. LVH = left ventricular hypertrophy
Dronedarone can be used concomitantly with ACE inhibitors/ARBs/statins and β-blockers. It should not be used in patients with heart failure (specifically NYHA class IV heart failure, or patients with an episode of heart failure decompensation in the past 4 weeks, especially if they have an LVEF ≤35 %) or substantial LV hypertrophy, in which case amiodarone is preferred.
Dronedarone can be safely initiated in an outpatient setting; however, clinicians must be careful to monitor patients with an ECG every 3 months. If the patient is found to be in AF then a decision must be made to either adopt a rate or rhythm control strategy. If a rate control strategy is to be pursued (i.e. AF is accepted) then dronedarone should be stopped and alternative therapy may be initiated (e.g. β-blockers, calcium channel blockers, amiodarone). However, if a rhythm control strategy is to be pursued (i.e. to maintain sinus rhythm) then a cardioversion should be performed – with dronedarone or an alternative anti-arrhythmic agent (e.g. flecainide, sotalol, propafenone, dofetilide or amiodarone). If cardioversion is successful then dronedarone may be continued and the patient followed up with 3-monthly ECGs. If cardioversion is unsuccessful it may be reasonable to stop dronedarone and try another agent. It is advisable that dronedarone should be discontinued in patients who remain in AF for 6 months or more.
9 Future Trials
Several clinical trials are under way to evaluate dronedarone further. These are summarized in Table 7.
10 Conclusion
Dronedarone is an effective anti-arrhythmic agent in patients with non-permanent AF, reducing mortality and hospitalization rates. It should not be used in patients with permanent AF or those with heart failure because in these groups of patients it can cause increased mortality and morbidity.
Although not as efficacious as amiodarone, dronedarone is recommended as first-line therapy (as are other antiarrhythmic agents) to maintain sinus rhythm because it has less toxic effects (thyroid, skin, pulmonary). The main adverse effects include gastrointestinal (mainly diarrhoea), hepatic (rare but important) and QTc prolongation. Clinicians must monitor their patients every 3 months to ensure they do not develop permanent AF or heart failure, and every 6 months with liver function tests. Clinical trials are in place to further evaluate the safety of dronedarone (in particular the effect on LV function) and to determine its optimal timing. Dronedarone appears to be a useful addition to the armory for rhythm control strategies in the management of AF.
References
Lip GY. Stroke in atrial fibrillation: epidemiology and thromboprophylaxis. J Thromb Haemost. 2011;9(1):344–51.
Lip GY, Lim HS. Atrial fibrillation and stroke prevention. Lancet Neurol. 2007;6:981–93.
Ruder KM, Benjamin EJ. Epidemiology and significance of atrial fibrillation. Am J Cardiol. 1999;84(9A):131–8R.
Wann LS, Curtis AB, January CT, et al. 2011 ACCF/AHA/HRS focused update on the management of patients with atrial fibrillation (updating the 2006 guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2011;57(2):223–42.
Camm J, Kirchhof P, Lip GYH, et al. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Eur Heart J. 2010;31(19):2369–429.
National Institute for Health and Clinical Excellence. CG36, atrial fibrillation (CG36). The management of atrial fibrillation. 2006. http://www.nice.org.uk/CG036. Accessed 20 Dec 2011.
Olshansky B, Rosenfeld LE, Warner AL, et al. The Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) study: approaches to control rate in atrial fibrillation. J Am Coll Cardiol. 2004;43(7):1201–8.
Van Gelder IC, Hagens VE, Bosker HA, et al. A comparison of rate control and rhythm control in patients with recurrent persistent atrial fibrillation. N Engl J Med. 2002;347(23):1834–40.
Carlsson J, Miketic S, Windeler J, et al. Randomized trial of rate-control versus rhythm-control in persistent atrial fibrillation: the Strategies of Treatment of Atrial Fibrillation (STAF) study. J Am Coll Cardiol. 2003;41(10):1690–6.
Opolski G, Torbicki A, Kosior D, et al. Rate control v rhythm control in patients with nonvalvular persistent atrial fibrillation: the results of the Polish How to Treat Chronic Atrial Fibrillation (HOT CAFÉ) study. Chest. 2004;126(2):476–86.
Roy D, Talajic M, Nattel S, et al. Rhythm control versus rate control for atrial fibrillation and heart failure. N Engl J Med. 2008;358(25):2667–77.
Hohnloser SH, Kuck KH, Lilienthal J. Rhythm or rate control in atrial fibrillation—Pharmacological Intervention in Atrial Fibrillation (PIAF): a randomized trial. Lancet. 2000;356(9244):1789–94.
Mazzini MJ, Monahan KM. Pharmacotherapy for atrial arrhythmias: present and future. Heart Rhythm. 2008;5(6 Suppl):S26–31.
Hilleman D, Miller MA, Parker R, et al. Optimal management of amiodarone therapy: efficacy and side effects. Pharmacotherapy. 2011;18(6):138–45S.
Han TS, Williams GR, Vanderpump MPJ. Benzfuran derivatives and the thyroid. Clin Endocrinol (Oxf). 2009;70(1):2–13.
US FDA. FDA news release. FDA approves Multaq to treat heart rhythm disorder. 2 Jul 2009. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm170276.htm. Accessed 21 Dec 2011.
European Medicines Agency. European Public Assessment Report for Multaq. http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Summary_for_the_public/human/001043/WC500044536.pdf. Accessed 21 Dec 2011.
US FDA. Multaq prescribing information 2012. http://www.accessdata.fda.gov/drugsatfda_docs/label/2012/022425s002lbl.pdf. Accessed 20 Apr 2012.
Connolly SJ, Camm AJ, Halperin JL, et al. Dronedarone in high-risk permanent atrial fibrillation. N Engl J Med. 2011;365(24):2268–76.
European Medicines Agency. Multaq summary of product characteristics. http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/001043/WC500044534.pdf. Accessed 20 Apr 2012.
Le Heuzey J-Y, De Ferrari GM, Radzik D, et al. A short-term, randomized, double-blind, parallel-group study to evaluate the efficacy and safety of dronedarone versus amiodarone in patients with persistent atrial fibrillation: the DIONYSOS study. J Cardiovasc Electrophysiol. 2010;21(6):597–605.
Kathofer S, Thomas D, Karle CA. The novel antiarrhythmic drug dronedarone: comparison with amiodarone. Cardiovasc Drug Rev. 2005;23(3):217–30.
Agelaki MG, Pantos C, Korantzopoulos P, et al. Comparative antiarrhythmic efficacy of amiodarone and dronedarone during acute myocardial infarction in rats. Eur J Pharmacol. 2007;564(1–3):150–7.
Van Herendael H, Dorian P. Amiodarone for the treatment and prevention of ventricular tachycardia. Vasc Health Risk Manag. 2010;6:465–72.
Oyetayo OO, Rogers CE, Hofman PO. Dronedarone: a new antiarrhythmic agent. Pharmacotherapy. 2010;30(9):904–15.
Wolbretter D, Gonzalez M, Samii S, et al. Dronedarone for the treatment of atrial fibrillation and atrial flutter: approval and efficacy. Vasc Health Risk Manag. 2010;6:517–23.
Baroletti S, Catella J, Ehle M, et al. Dronedarone: a review of characteristics and clinical data. Crit Pathw Cardiol. 2010;9(2):94–101.
Lalevee N, Nargeot J, Barrere-Lemaire S, et al. Effects of amiodarone and dronedarone on voltage-dependent sodium current in human cardiomyocytes. J Cardiovasc Electrophysiol. 2003;14:885–90.
Guillemare E, Marion A, Nisato D, et al. Inhibitory effects of dronedarone on muscarinic K+ current in guinea pig atrial cells. J Cardiovasc Pharmacol. 2000;36:802–5.
Gautier P, Guillemare E, Marion A, et al. Electrophysiologic characterization of dronedarone in guinea pig ventricular cells. J Cardiovasc Pharmacol. 2003;41:191–202.
Gautier P, Marion A, Bertrand JP, et al. Electrophysiological characterization of dronedarone (SR33589), a new amiodarone-like agent, in cardiac ventricular myocytes. Eur Heart J. 1997;18(Suppl):269.
Rochetti M, Bertrand JP, Nisato D, et al. Cellular electrophysiological study of dronedarone, a new amiodarone-like agent, in guinea pig sinoatrial node. Nauyn Schmiedebergs Arch Pharmacol. 1998;358(1 Suppl 2):R617.
Aimond F, Beck L, Gautier P, et al. Cellular and in vivo electrophysiological effects of dronedarone in normal and postmyocardial infarcted rats. J Pharmacol Exp Ther. 2000;292:415–24.
Chatelain P, Meysmans L, Matteazzi JR, et al. Interaction of the antiarrhythmic agents SR 33589 and amiodarone with the beta-adrenoceptor and adenylate cyclase in rat heart. Br J Pharmacol. 1995;116:1949–56.
Djandjighian L, Planchenault J, Finance O, et al. Hemodynamic and antiadrenergic effects of dronedarone and amiodarone in animals with a healed myocardial infarction. J Cardiovasc Pharmacol. 2000;36:376–83.
Hodeige D, Heyndrickx JP, Chatelain P, et al. SR 33589, a new amiodarone-like antiarrhythmic agent: anti-adrenoceptor activity in anaesthetized and conscious dogs. Eur J Pharmacol. 1995;279:25–32.
Sun W, Sharma JS, Singh BN. Electrophysiological effects of dronedarone (SR33589), a noniodinated benzofuran derivative, in the rabbit heart comparison with amiodarone. Circulation. 1999;100:2276–81.
Sun W, Sharma JS, Singh BN. Chronic and acute effects of dronedarone on the action potential of rabbit atrial muscle preparations: comparison with amiodarone. J Cardiovasc Pharmacol. 2002;39(5):677–84.
van Opstal JM, Schoenmakers M, Verduyn SC, et al. Chronic amiodarone evokes no torsade de pointes arrhythmias despite QT lengthening in an animal model of acquired long-QT syndrome. Circulation. 2001;104:2722–7.
Manning AS, Bruyninckx C, Ramboux J, et al. SR 33589, a new amiodarone-like agent: effect on ischemia- and reperfusion-induced arrhythmias in anesthetized rats. J Cardiovasc Pharmacol. 1995;26(3):453–61.
Rochetaing A, Barbe C, Kreher P. Beneficial effects of amiodarone and dronedarone (SR 33589b), when applied during low-flow ischemia, on arrhythmia and functional parameters assessed during reperfusion in isolated rat hearts. J Cardiovasc Pharmacol. 2001;38(4):500–11.
Finance O, Manning A, Chatelain P. Effects of a new amiodarone-like agent, SR 33589, in comparison to amiodarone, d,l-sotalol, and lignocaine, on ischemia-induced ventricular arrhythmias in anesthetized pigs. J Cardiovasc Pharmacol. 1995;26(4):570–6.
Verduyn SC, Vos MA, Leunissen HD, et al. Evaluation of the acute electrophysiologic effects of intravenous dronedarone, an amiodarone-like agent, with special emphasis on ventricular repolarization and acquired torsades de pointes arrhythmias. J Cardiovasc Pharmacol. 1999;33:212–22.
Mitchell LB, Wyse DG, Gillis AM, et al. Electropharmacology of amiodarone therapy initiation: time course of onset of electrophysiologic and antiarrhythmic effects. Circulation. 1989;80:34–42.
Sanofi-aventis Canda Inc. Product monograph: Multaq®. Date of revision September 12, 2012. http://products.sanofi.ca/en/multaq.pdf. Accessed 20 Apr 2012.
Dorian P. Clinical pharmacology of dronedarone: implications for the therapy of atrial fibrillation. J Cardiovasc Pharmacol Ther. 2010;15(4):15–8S.
Patel C, Yan G-X, Kowey PR. Dronedarone. Circulation. 2009;120(7):636–44.
Anastasiou-Nana M, Levis GM, Moulopoulos S. Pharmacokinetics of amiodarone after intravenous and oral administration. Int J Clin Pharmacol Ther Toxicol. 1982;20(11):524–9.
Andreasen F, Agerbaek H, Bjerregaard P, et al. Pharmacokinetics of amiodarone after intravenous and oral administration. Eur J Clin Pharmacol. 1981;19(4):293–9.
Tschuppert Y, Buclin T, Rothuizen LE, et al. Effect of dronedarone on renal function in healthy subjects. Br J Clin Pharmacol. 2007;64(6):785–91.
Singh BN, Connolly SJ, Crijns HJ, et al. Dronedarone for maintenance of sinus rhythm in atrial fibrillation or flutter. N Engl J Med. 2007;357(10):987–99.
Singh BN, Vaughan Williams EM. The effect of amiodarone, a new anti-anginal drug, on cardiac muscle. Br J Pharmacol. 1970;39(4):657–67.
Counihan PJ, McKenna WJ. Risk-benefit assessment of amiodarone in the treatment of cardiac arrhythmias. Drug Saf. 1990;5(4):286–304.
Holt DW, Tucker GT, Jackson PR, et al. Amiodarone pharmacokinetics. Am Heart J. 1983;106(4):840–7.
Pourbaix S, Berger Y, Desager JP, et al. Absolute bioavailability of amiodarone in normal subjects. Clin Pharmacol Ther. 1985;37(2):118–23.
Plomp TA, van Rossum JM, Robles de Medina EO, et al. Pharmacokinetics and body distribution of amiodarone in man. Arzneimittelforschung. 1984;34(4):513–20.
Adams PC, Holt DW, Storey GC, et al. Amiodarone and its desethyl metabolite: tissue distribution and morphologic during long-term therapy. Circulation. 1985;72(5):1064–75.
Meng Z, Mojaverian P, Doedee M, et al. Bioavailability of amiodarone tablets administered with and without food in healthy subjects. Am J Cardiol. 2001;87(4):432–5.
Touboul P, Brugada J, Capucci A, et al. Dronedarone for prevention of atrial fibrillation: a dose-ranging study. Eur Heart J. 2003;24(16):1481–7.
Davy JM, Herold M, Hoglund C, et al. Dronedarone for the control of ventricular rate in permanent atrial fibrillation: the efficacy and safety of dronedarone for control of ventricular rate during atrial fibrillation (ERATO) study. Am Heart J. 2008;156(3):527e1–9.
Hohnloser SH, Crijns HJGM, van Eickels M, et al. Effect of dronedarone on cardiovascular events in atrial fibrillation. N Engl J Med. 2009;360(7):668–78.
Duray GZ, Torp-Pedersen C, Connolly SJ, et al. Effects of dronedarone on clinical outcomes in patients with lone atrial fibrillation: pooled post hoc analysis from the ATHENA/EURIDIS/ADONIS studies. J Cardiovasc Electrophysiol. 2011;22(7):770–6.
Kober L, Torp-Pedersen C, McMurray JJV, et al. Increased mortality after dronedarone therapy for severe heart failure. N Engl J Med. 2008;358(25):2678–87.
US FDA. Drug safety communication: severe liver injury associated with the use of dronedarone (marketed as Multaq). http://www.fda.gov/drugs/drugsafety/ucm240011.htm. Accessed 21 Dec 2011.
Vallakati A, Chandra PA, Pednekar M, et al. Dronedarone-induced digoxin toxicity: new drug, new interactions. Epub: Am J Ther; 2011.
Rathore SS, Curtis JP, Wang Y, et al. Association of serum digoxin concentration and outcomes in patients with heart failure. JAMA. 2003;289:871–8.
US FDA. Drug safety communication: review update of Multaq (dronedarone) and increased risk of death and serious cardiovascular adverse events. http://www.fda.gov/Drugs/DrugSafety/ucm283933. Accessed 21 Dec 2011.
Piccini JP, Hasselblad V, Peterson ED, et al. Comparative efficacy of dronedarone and amiodarone for the maintenance of sinus rhythm in patients with atrial fibrillation. J Am Coll Cardiol. 2009;54:1089–95.
Acknowledgements
No funding was provided for this work. Gregory Lip has served as a consultant for Bayer, Astellas, Merck, Sanofi, BMS/Pfizer, Daiichi-Sanyko, Biotronik, Portola and Boehringer Ingelheim, and has been on the speakers bureau for Bayer, BMS/Pfizer, Boehringer Ingelheim and Sanofi-aventis. Ahmed Adlan has no conflict of interests to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Adlan, A.M.A., Lip, G.Y.H. Benefit-Risk Assessment of Dronedarone in the Treatment of Atrial Fibrillation. Drug Saf 36, 93–110 (2013). https://doi.org/10.1007/s40264-012-0012-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40264-012-0012-8