
Abstract
Glioblastoma is the most common malignant brain tumor accounting for more than 54 % of all gliomas. Despite aggressive treatments, median survival remains less than 1 year. This might be due to the unavailability of effective molecular diagnostic markers and targeted therapy. Thus, it is essential to discover molecular mechanisms underlying disease by identifying dysregulated pathways involved in tumorigenesis. Notch signaling is one such pathway which plays an important role in determining cell fates. Since it is found to play a critical role in many cancers, we investigated the role of Notch genes in glioblastoma with an aim to identify biomarkers that can improve diagnosis. Using real-time PCR, we assessed the expression of Notch genes including receptors (Notch1, Notch2, Notch3, and Notch4), ligands (JAG1, JAG2, and DLL3), downstream targets (HES1 and HEY2), regulator Deltex1 (DTX1), inhibitor NUMB along with transcriptional co-activator MAML1, and a component of gamma-secretase complex APH1A in 15 formalin-fixed paraffin-embedded (FFPE) patient samples. Relative quantification was done by the 2−ΔΔCt method; the data are presented as fold change in gene expression normalized to an internal control gene and relative to the calibrator. The data revealed aberrant expression of Notch genes in glioblastoma compared to normal brain. More than 85 % of samples showed high Notch1 (P = 0.0397) gene expression and low HES1 (P = 0.011) and DTX1 (P = 0.0001) gene expression. Our results clearly show aberrant expression of Notch genes in glioblastoma which can be used as putative biomarkers together with histopathological observation to improve diagnosis, therapeutic strategies, and patient prognosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gliomas account for 28 % of all primary brain tumors and 80 % of all malignant tumors [1]. Gliomas are classified based on the extent of anaplasia as per WHO classification into pilocytic astrocytoma (grade I), diffuse astrocytoma (grade II), anaplastic astrocytoma (grade III), and glioblastoma multiforme (GBM) (grade IV) [2]. As per CBTRUS data, GBM accounts for 54.7 % of all primary brain and CNS gliomas, making it the most common form of brain malignancy [1]. Patients with GBM have a median survival of less than 1 year even with the use of the most aggressive treatments like surgery, radiation, and chemotherapy. This could be because of insufficient understanding of the expression pattern of various genes involved in GBM development. It is hoped that understanding the molecular pathways to identify specific molecular markers, together with histological observation, can improve diagnosis, therapeutic strategies, and patient prognosis. Like in other cancers, dysregulation of several signaling pathways has been reported in astrocytic tumors [3, 4]. A thorough understanding of the expression pattern of genes in these signaling pathways and their downstream targets is essential to improve diagnosis and find new therapeutic strategies.
The Notch pathway is a highly conserved cell signaling pathway that plays a pivotal role in a variety of cellular processes, including differentiation, proliferation, survival, and apoptosis. Depending on the cell type, the Notch pathway can positively or negatively influence the cellular and developmental processes. The four Notch receptors (Notch1–4) and five ligands (Jagged1, Jagged2, Delta-like-1, Delta-like-3, and Delta-like-4) have been identified in mammals. Notch receptors are transmembrane proteins which on binding with appropriate ligands on adjacent cells are sensitized to proteolytic cleavage mediated by ADAM and gamma-secretase families of proteases. These cleavage events release Notch intracellular domain (NICD) from the plasma membrane which translocates to the nucleus. In the nucleus, it forms a complex with the members of CSL transcription factors (C promoter binding protein-1) and with transcriptional co-activators of the MAML (Mastermind-like) family, which in turn mediates the transcription of target genes [5]. The most prominent Notch pathway target genes include two families of transcriptional factors Hes (HES1 and HES5) and Hey (HEY1 and HEY2).
Notch signaling is found to play an important role in cell fate decisions throughout glial and neuronal differentiation from neural stem cells during normal brain development. Activation of the Notch pathway appears to have a critical role in gliogenesis directly promoting differentiation of many glial cell subtypes at the expense of neurons [6, 7]. In the developing brain, the Notch pathway is also essential for maintaining neural progenitor cells (NPCs) in a proliferating state. The absence of vital pathway components leads to neuronal differentiation and NPC depletion. Notch signaling modulator Numb protein negatively regulates Notch gene expression resulting in cell cycle arrest and differentiation of NPCs [8]. In adult rodent spinal cord and in cell culture, Notch3 promotes neuronal differentiation contrary to Notch1 [9]. In primary astrocyte and neurosphere co-cultures, astrocytes were found to negatively regulate neurogenesis through endocytosis of the Notch ligand Jagged1 [10]. Thus, depending on cellular context, individual Notch receptors and ligands can have differing functions. Apart from developmental functions, Notch pathway genes are also expressed in adult brain cells, suggesting its role in neurological plasticity throughout life [11]. In this manner, the Notch pathway controls self-renewal of NPC and cell fate decisions in developing and adult brain.
It has been reported that abnormal Notch signaling can contribute to the development of many cancers including T cell acute lymphoblastic leukemia; Hodgkin lymphoma; multiple myeloma; glioma; cervical, pancreatic, lung, and breast cancer; hepatocellular carcinoma; etc. [12, 13]. A dysregulated Notch pathway can be either oncogenic or tumor suppressive depending on the cellular context [14]. The molecular mechanisms underlying the oncogenic and tumor suppressor role of Notch are not fully understood. Notch3 acts as both an oncogene [15] and a tumor suppressor gene [16] depending on the type of malignancy. In a murine non-small cell lung cancer model, Notch1 and Notch2 were found to have opposing roles in tumorigenesis. Notch2 receptor deletion led to increased carcinogenesis, thus highlighting its tumor suppressor function, while Notch1 receptor deletion resulted in reduced tumor formation in vivo [17]. Notch1 and Delta-like-1 showed overexpression in glioma cell lines as well as primary human gliomas [18]. Pretreatment of glioma cells with Notch1 or Delta-like-1 small interfering RNA prolonged survival in a murine orthotopic brain tumor model, thus showing dependence of glioma cells on a single Notch ligand. However, the mechanisms underlying Notch activation and its importance in the regulation of brain tumors remain poorly defined. In another study, forced overexpression of Notch1 in glioma cells led to increased proliferation and formation of neurosphere-forming stem cells [19]. Interestingly, inhibition of Notch signaling through expression of DN-MAML1, a dominant negative form of mastermind-like 1, and treatment with a gamma-secretase inhibitor resulted in reduction of glioblastoma cell growth and proliferation in vitro and in vivo. Also, knockdown of Notch receptors revealed that Notch2 had a predominant role in GBM cell growth [20]. In a novel three-dimensional explant system of surgical GBM samples, Notch inhibition resulted in decreased proliferation and self-renewal of GBM cells. Combination therapy of Notch blockade and radiation resulted in a significant decrease in cell proliferation and self-renewal in tumor explants while only radiation therapy was less effective [21]. In addition, anti-Dll4 has been proposed as a potential therapeutic agent in Dll4-expressing tumors which reduces tumor burden and prolongs survival [22]. These data suggest that the Notch signaling pathway plays a critical role by contributing significantly to tumor growth and is thus a potential therapeutic target.
Notch downstream targets HES and HEY genes are expressed in specific patterns based on cell type in infantile hemangiomas. Hemangioma endothelial cells expressed HEY2 whereas hemangioma stem cells expressed HEY1, HEYL, and HES1 [23]. Hepatocellular carcinoma patients with higher expression of HES1 showed better survival, indicating the probable tumor suppressor role of the gene [24]. However, the role of other Notch family genes such as positive and negative regulators, co-activators, genes in gamma-secretase complex, etc. has not been studied thoroughly and their contribution in tumor development remains controversial. Along these lines, these data showcase ambiguous functions of Notch pathway genes in the pathogenesis of various cancers and insist the need to define clear-cut roles of each gene involved in the Notch signaling pathway.
This study was designed to reveal genes in the Notch signaling pathway underlying the pathogenesis of GBM. In this study, we examined the expression of 13 Notch pathway genes in 15 human GBM formalin-fixed paraffin-embedded (FFPE) tissue sections using real-time polymerase chain reaction (PCR). We report aberrant expression of few Notch signaling pathway genes in majority of the samples examined as compared to normal brain FFPE tissue sections. A novel finding from our study was high expression of Notch1 and low expression of DTX1 and HES1 in more than 85 % of GBM cases. We thus propose that aberrant expression of Notch pathway genes may be a frequent event and that these genes could be used as diagnostic markers and probable drug targets in GBM.
Materials and methods
Histopathology
Prior to the initiation of this study, institutional ethical review board approval was acquired (IERB/1/198/08). Informed consent was obtained from all individual participants included in the study. Biopsy was collected based on clinical evidence and confirmation for GBM at St. John’s Medical College, Bangalore, India, by a neurosurgeon. Tissues were processed and FFPE blocks were prepared. Tumor area was marked and re-blocked after histopathological confirmation by a pathologist from St. John’s Medical College, Bangalore, India, to ensure the absence of any normal brain tissue.
Samples
A total of 15 GBM FFPE samples from St. John’s Medical College, Bangalore, India, and two normal brain FFPE samples from the Brain Bank, NIMHANS, Bangalore, India, were collected. Tumor samples were obtained from 3 female and 12 male patients with age ranging between 13 and 63 years and mean age of 41.4 years. Normal brain autopsy (cerebral cortex, frontal lobe, gray and white matter) was obtained from a 50-year-old male and a 27-year-old female.
RNA isolation and reverse transcription
Total RNA was extracted from two 10-μm-thick FFPE tissue sections by TRIzol (Invitrogen, CA, USA) method after de-paraffinization and proteinase K digestion [25]. RNA samples retrieved were quantified by measuring the absorbance using NanoDrop and visualized on an agarose gel for quality assurance. One microgram of RNA was reverse transcribed to complementary DNA (cDNA) using a high-capacity cDNA reverse transcription kit (Applied Biosystems, CA, USA).
Quantitative real-time PCR
The relative quantitation of expression levels of 13 test genes was carried out in Applied Biosystems StepOnePlus™ Instrument. Amplification was performed using SYBR Green master mix (Fermentas, MA, USA), 100 nM forward and reverse primers (Sigma-Aldrich, MO, USA), and 10 ng of cDNA template. Amplification was carried out with an initial denaturation step at 95 °C for 10 min followed by 40 cycles at 95 °C for 15 s, 60 °C for 30 s, and 72 °C for 30 s in a total of 25-μl reaction volume. All reactions were run in triplicate, and the mean was used for further calculations. For each primer set, PCR efficiency was calculated from dilution curves generated using serially diluted cDNA used for the study. The TATA binding protein (TBP), a housekeeping gene, was chosen as an appropriate internal control after validating six conventionally used housekeeping genes in gene expression studies [26]. Normal brain samples were used as calibrator. Relative quantification was done by the 2−ΔΔCt method; the data are presented as fold change in gene expression normalized to an endogenous reference gene and relative to the calibrator and are given by:
where ΔΔCt = (CtTarget − CtTBP)Tumor − (CtTarget − CtTBP)Calibrator.
Reverse transcription PCR (RT-PCR) was carried out with a very high cDNA template concentration for detecting poorly expressed transcripts from samples that were not detected in quantitative real-time PCR (qPCR). Conditions used for RT-PCR will be provided on request. Statistical significance was assessed by calculating probability values through Student’s t test using GraphPad (CA, USA). P values less than 0.05 were considered as significant.
Results
Real-time PCR analysis of selected genes
All the 13 genes investigated were expressed in both GBM and normal brain tissues, with few exceptions. The mean expression levels of 8 out of 13 Notch pathway genes studied were lower in GBM compared to their normal counterparts. However, the expression level of each gene varied considerably from patient to patient.
Expression of Notch receptors and ligands
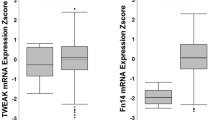
We first examined Notch receptor (Notch1, Notch2, Notch3, and Notch4) and ligand (JAG1, JAG2, and DLL3) expression in GBM samples. Our study showed that Notch1 was specifically overexpressed in 86.66 % (13/15) of GBM samples (P = 0.0397) (Table 1). Notch3 was moderately upregulated with messenger RNA (mRNA) levels elevated in 40 % of samples (6/15) (Table 1). Undetectable levels of Notch4 transcripts were confirmed with qualitative PCR which did not show any amplification product even at a template concentration of 200 ng (data not shown). Strikingly, no Notch2 gene expression was found in normal brain tissues even at a template concentration of 200 ng using basic PCR (data not shown). The levels of JAG1 and DLL3 were found to be underexpressed in 81.81 % (9/11) (P = 0.0433) and 85.71 % (6/7) (P = 0.0212) of samples, respectively (Fig. 1). JAG2 gene expression was not detected in any of the tumor tissues analyzed. On carrying out qualitative PCR, an amplification product showed up at template concentration of 150 ng which is 15 times more than the template concentration used for qPCR (data not shown).

Scatter plots of differentially expressed Notch pathway genes in terms of log2 ratio derived from qPCR analysis across GBM samples compared to normal brain samples. Each dot represents data obtained from one patient sample
Expression of Notch activators and inhibitors
Transcript levels of the Notch co-activator MAML1 were not detected in the GBM tissues analyzed. Confirmation with basic PCR did not show any amplification product even at 200 ng concentration (data not shown), while the mRNA levels of NUMB, an inhibitor of Notch, remained similar to or less than that of normal brain tissue in 73.33 % (11/15) of GBM samples (Table 1). There was a statistically significant association between low levels of NUMB and overexpression of Notch1 in this data set (P = 0.0001).
Expression of Notch downstream targets
We next measured the mRNA levels of Notch downstream targets HES1 and HEY2. HES1 showed low expression compared to the calibrator in 93.33 % (14/15) of samples studied (P = 0.011) (Table 1). However, statistical analysis revealed no significant correlation between the downregulation of HES1 and Notch ligands JAG1 (P = 0.9216) and DLL3 (P = 0.8645). On the other hand, we did not find any significant change in the expression of HEY2 when compared to normal brain in 50 % (7/14) of GBM samples (Table 1).
Expression of other Notch pathway genes
We additionally investigated the levels of APH1A, a member of the gamma-secretase complex. APH1A showed low expression in all 6 GBM samples studied compared to normal brain samples (P = 0.033) (Fig. 1). A statistically significant association between low expression of HES1 and APH1A was observed (P = 0.002). DTX1, a transcription factor that regulates the Notch pathway through ubiquitin ligase activity, showed extremely low expression in all 13 samples studied (P = 0.0001) (Fig. 1).
Discussion
The present study aimed to identify differentially expressed genes from the Notch signaling pathway in GBM. Many of the genes studied have known or suspected relevance to various cancer types. However, the significance of their regulation in GBM is not known. We identified aberrant expression of few Notch genes in GBM samples relative to normal brain samples by several folds.
Seventy-three percent (11/15) of GBM samples studied showed elevated Notch1 expression, low levels of HES1 and DTX1, and absence of Notch4, JAG2, and MAML1 mRNA. Notch1 overexpression has been documented previously in various cancers like myeloma, breast cancer, medulloblastoma, etc. promoting tumor growth [27–29]. Notch1 upregulation was found to have an association with poor prognosis in cervical cancer and hepatocellular carcinoma [30, 31]. Thus, the elevated Notch1 expression observed in our study might play a role in promoting GBM growth and could be an effective target for treatment. Also, Notch1 expression was found to have an inverse relationship with Notch ligand expression wherein all samples studied had low or undetected levels of Notch ligands JAG1, JAG2, and DLL3. This lack of correlation might be due to the existence of multiple Notch ligands and receptors, and some of which may not be regulated at the transcriptional level. The significance of the Notch4 gene in tumorigenesis is not clearly understood. However, the absence of Notch4 and JAG2 expression in the present study was in accordance with other studies which showed downregulation of Notch4 and JAG2 genes and their probable role as tumor suppressor genes in endometrial cancer [32]. Conversely, Notch1 gene silencing in gastric and prostate cancer cells inhibited tumor growth, which suggests its possible role as an oncogene [33, 34]. Therefore, Notch4 and JAG2 gene activation and Notch1 gene silencing could be potential therapeutic targets in GBM. These findings highlight differentially expressed Notch receptors and their distinct roles in GBM.
Aph-1 is found to play a dominant role in interacting with gamma-secretase substrates [35]. Thus, in its absence, proteolytic cleavage of Notch receptors releasing NICD might be hindered, in turn affecting the expression of Notch downstream targets. In the present study, 33 % (5/15) of GBM samples showed low expression of both APH1A and HES1 genes. Thus, HES1 downregulation despite having high Notch1 expression might be due to the downregulation or absence of the APH1A gene as discussed earlier or due to other inhibitory mechanisms involving various genes. Studies have shown that HES6, another member of the HES family of genes, inhibits HES1 [36, 37]. However, expression analysis of HES6 was not carried out to support the above data. Additionally, it could be due to the absence of Notch ligands which bind and simultaneously activate Notch receptors which in turn move to the nucleus to activate the transcription of Hes/Hey family genes [38]. Fifty-three percent (8/15) of GBM samples studied showed low expression of JAG1 and HES1 regardless of high Notch1 gene expression. Thus, significant decrease of ligands DLL3, JAG1, and JAG2 mRNA expression might play a role in the downregulation of Notch-mediated signaling, as observed by reduced levels of the Notch target gene HES1.
The transcriptional co-activator MAML1 interacts with Notch and CSL in the nucleus to activate transcription of Notch downstream targets. MAML genes are critical components regulating cellular events involving both normal development and oncogenesis [39]. Absence of MAML1 expression may thus contribute to the lack of Notch target gene expression in the GBM samples studied. DTX1, a regulator of Notch signaling, acts as both positive and negative regulator depending on the developmental and cellular context. The inhibition of Notch signaling is mediated by binding with the Notch intracellular domain and degradation of Notch receptors through ubiquitination [40]. In another study, induced expression of DTX1 was found to antagonize Notch1 signaling in hematopoietic progenitors by inhibiting co-activator recruitment resulting in B cell development in fetal thymic organ culture at the expense of T cell development [41]. Hence, it can be hypothesized that inducing DTX1 expression in GBM can lead to ubiquitination of overexpressed Notch1 receptors subsequently reducing tumor growth. Since, much of work is not carried out on MAML1 and DTX1, their role in oncogenesis is not clearly understood. Extensive research must be done to identify their functions in GBM pathogenesis in the future. In the present study, due to tissue limitations, genes that showed undetectable levels of expression in real-time PCR could not be confirmed by analyzing the expression level with an increased template concentration. A small sample size was another limitation of our study. These limitations will be addressed in the future with a larger sample size and sufficient amount of tissue which would confirm the results.
From our study, it is evident that a large percentage of GBM we examined exhibited dysregulated Notch genes, suggesting the possibility of their role in the development of GBM. Except for the receptors Notch1 and Notch3, all other pathway genes studied showed expression similar to or lower than that of normal brain samples. Specifically, the Notch1 gene showed high expression and the HES1 and DTX1 genes showed low expression in more than 85 % of samples. It can be therefore hypothesized that the Notch1, HES1, and DTX1 genes can be considered as potential biomarkers for GBM diagnosis. Additionally, these dysregulated Notch genes can be targeted for GBM therapy either by gene activation or silencing depending on their expression patterns. Although the results of the present study show dysregulated Notch genes, the exact means by which the Notch signaling pathway contributes to gliomagenesis remains unclear. Thus, a better understanding of how the Notch pathway mediates differentiation, growth, and transformation of glial cells is crucial. Information from the current study along with future works targeting individual Notch genes might be useful to understand tumor pathobiology and also to develop new therapeutic strategies.
References
Ostrom QT, Gittleman H, Liao P, et al. CBTRUS statistical report: primary brain and central nervous system tumors diagnosed in the United States in 2007-2011. Neuro Oncol. 2014;16 Suppl 4:iv1–63.
Mischel PS, Vinters HV. Neuropathology and molecular pathogenesis of primary brain tumors. Brain Tumor Immunother. 2001;3–45.
Godard S, Getz G, Delorenzi M, et al. Classification of human astrocytic gliomas on the basis of gene expression: a correlated group of genes with angiogenic activity emerges as a strong predictor of subtypes. Cancer Res. 2003;63:6613–25.
Nutt CL, Mani DR, Betensky RA, et al. Gene expression-based classification of malignant gliomas correlates better with survival than histological classification. Cancer Res. 2003;63:1602–7.
Kopan R, Ilagan MX. The canonical Notch signaling pathway: unfolding the activation mechanism. Cell. 2009;137:216–33.
Furukawa T, Mukherjee S, Bao ZZ, et al. rax, Hes1, and Notch1 promote the formation of Müller glia by postnatal retinal progenitor cells. Neuron. 2000;26:383–94.
Gaiano N, Fishell G. The role of Notch in promoting glial and neural stem cell fates. Annu Rev Neurosci. 2002;25:471–90.
Li HS, Wang D, Shen Q, et al. Inactivation of Numb and Numblike in embryonic dorsal forebrain impairs neurogenesis and disrupts cortical morphogenesis. Neuron. 2003;40:1105–18.
Rusanescu G, Mao J. Notch3 is necessary for neuronal differentiation and maturation in the adult spinal cord. J Cell Mol Med. 2014;18:2103–16.
Wilhelmsson U, Faiz M, de Pablo Y, et al. Astrocytes negatively regulate neurogenesis through the Jagged1-mediated Notch pathway. Stem Cells. 2012;30:2320–9.
Presente A, Andres A, Nye JS. Requirement of Notch in adulthood for neurological function and longevity. Neuroreport. 2001;12:3321–5.
Axelson H. Notch signaling and cancer: emerging complexity. Semin Cancer Biol. 2004;14:317–9.
Hansson EM, Lendahl U, Chapman G. Notch signaling in development and disease. Semin Cancer Biol. 2004;14:320–8.
Lobry C, Oh P, Aifantis I. Oncogenic and tumor suppressor functions of Notch in cancer: it’s NOTCH what you think. J Exp Med. 2011;208:1931–5.
Rahman MT, Nakayama K, Rahman M, et al. Notch3 overexpression as potential therapeutic target in advanced stage chemoresistant ovarian cancer. Am J Clin Pathol. 2012;138:535–44.
Cui H, Kong Y, Xu M, et al. Notch3 functions as a tumor suppressor by controlling cellular senescence. Cancer Res. 2013;73:3451–9.
Baumgart A, Mazur PK, Anton M, et al. Opposing role of Notch1 and Notch2 in a KrasG12D-driven murine non-small cell lung cancer model. Oncogene. 2015;34:578–88.
Purow BW, Haque RM, Noel MW, et al. Expression of Notch-1 and its ligands, Delta-like-1 and Jagged-1, is critical for glioma cell survival and proliferation. Cancer Res. 2005;65:2353–63.
Zhang XP, Zheng G, Zou L, et al. Notch activation promotes cell proliferation and the formation of neural stem cell-like colonies in human glioma cells. Mol Cell Biochem. 2008;307:101–8.
Chen J, Kesari S, Rooney C, et al. Inhibition of notch signaling blocks growth of glioblastoma cell lines and tumor neurospheres. Genes Cancer. 2010;1:822–35.
Hovinga KE, Shimizu F, Wang R, et al. Inhibition of notch signaling in glioblastoma targets cancer stem cells via an endothelial cell intermediate. Stem Cells. 2010;28:1019–29.
Ridgway J, Zhang G, Wu Y, et al. Inhibition of Dll4 signalling inhibits tumour growth by deregulating angiogenesis. Nature. 2006;444:1083–7.
Adepoju O, Wong A, Kitajewski A, et al. Expression of HES and HEY genes in infantile hemangiomas. Vasc Cell. 2011;3:19.
Viatour P, Ehmer U, Saddic LA, et al. Notch signaling inhibits hepatocellular carcinoma following inactivation of the RB pathway. J Exp Med. 2011;208:1963–76.
Kizys MM, Cardoso MG, Lindsey SC, et al. Optimizing nucleic acid extraction from thyroid fine-needle aspiration cells in stained slides, formalin-fixed/paraffin-embedded tissues, and long-term stored blood samples. Arq Bras Endocrinol Metabol. 2012;56:618–26.
Aithal MGS, Rajeswari N. Validation of housekeeping genes for gene expression analysis in glioblastoma using quantitative real-time polymerase chain reaction. Brain Tumor Res Treat. 2015;3:24–9.
Bolós V, Mira E, Martínez-Poveda B, et al. Notch activation stimulates migration of breast cancer cells and promotes tumor growth. Breast Cancer Res. 2013;15:R54.
Guo D, Li C, Teng Q, et al. Notch1 overexpression promotes cell growth and tumor angiogenesis in myeloma. Neoplasma. 2013;60:33–40.
Natarajan S, Li Y, Miller EE, et al. Notch1-induced brain tumor models the sonic hedgehog subgroup of human medulloblastoma. Cancer Res. 2013;73:5381–90.
Ahn S, Hyeon J, Park CK. Notch1 and Notch4 are markers for poor prognosis of hepatocellular carcinoma. Hepatobiliary Pancreat Dis Int. 2013;12:286–94.
Yousif NG, Sadiq AM, Yousif MG, et al. Notch1 ligand signaling pathway activated in cervical cancer: poor prognosis with high-level JAG1/Notch1. Arch Gynecol Obstet. 2015. doi:10.1007/s00404-015-3694-1.
Sasnauskienė A, Jonušienė V, Krikštaponienė A, et al. NOTCH1, NOTCH3, NOTCH4, and JAG2 protein levels in human endometrial cancer. Medicina (Kaunas). 2014;50:14–8.
Ye QF, Zhang YC, Peng XQ, et al. Silencing Notch-1 induces apoptosis and increases the chemosensitivity of prostate cancer cells to docetaxel through Bcl-2 and Bax. Oncol Lett. 2012;3:879–84.
Wei G, Chang Y, Zheng J, et al. Notch1 silencing inhibits proliferation and invasion in SGC-7901 gastric cancer cells. Mol Med Rep. 2014;9:1153–8.
Chen AC, Guo LY, Ostaszewski BL, et al. Aph-1 associates directly with full-length and C-terminal fragments of gamma-secretase substrates. J Biol Chem. 2010;285:11378–91.
Bae SK, Bessho Y, Hojo M, et al. The bHLH gene Hes6, an inhibitor of Hes1, promotes neuronal differentiation. Development. 2000;127:2933–43.
Gibert JM, Simpson P. Evolution of cis-regulation of the proneural genes. Int J Dev Biol. 2003;47:643–51.
Luo B, Aster JC, Hasserjian RP, et al. Isolation and functional analysis of a cDNA for human Jagged2, a gene encoding a ligand for the Notch1 receptor. Mol Cell Biol. 1997;17:6057–67.
Wu L, Griffin JD. Modulation of Notch signaling by mastermind-like (MAML) transcriptional co-activators and their involvement in tumorigenesis. Semin Cancer Biol. 2004;14:348–56.
Zhang P, Yang Y, Nolo R, et al. Regulation of NOTCH signaling by reciprocal inhibition of HES1 and Deltex 1 and its role in osteosarcoma invasiveness. Oncogene. 2010;29:2916–26.
Izon DJ, Aster JC, He Y, et al. Deltex1 redirects lymphoid progenitors to the B cell lineage by antagonizing Notch1. Immunity. 2002;16:231–43.
Acknowledgments
This study was funded by the Department of Science and Technology, New Delhi, India (grant number SR/FT/LS-170/2008). We thank the Brain Bank, NIMHANS, Bangalore, India, for providing the clinical samples.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None
Ethical approval
For this type of study, formal consent is not required.
Rights and permissions
About this article

Cite this article
Narayanappa, R., Rout, P., Aithal, M.G.S. et al. Aberrant expression of Notch1, HES1, and DTX1 genes in glioblastoma formalin-fixed paraffin-embedded tissues. Tumor Biol. 37, 6935–6942 (2016). https://doi.org/10.1007/s13277-015-4592-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-015-4592-7