
Abstract
Background
The use of myocardial perfusion imaging (MPI) in the management of coronary artery disease (CAD) is well established. Although prior studies have shown disparities in the use of invasive angiography in patients with acute MI, data on factors affecting referral to angiography post-MPI are lacking. We sought to evaluate the primary determinants of referral to invasive angiography post-MPI and specifically assess the role of non-traditional non-clinical factors such as race/ethnicity, socioeconomic factors, insurance status, and marital status.
Methods
All patients without known CAD who underwent stress SPECT MPI over 15 years were reviewed and the performance of coronary angiography within 90 days of their MPI was recorded. Multiple factors were analyzed for an association with referral to angiography, including exercise and MPI results, baseline demographics, traditional cardiac risk factors, and non-traditional factors such as ethnicity, insurance, marital and socioeconomic status. In a secondary analysis, these factors were assessed with regard to abnormal MPI results.
Results
Out of 27,895 total patients, 2,150 (7.7%) underwent invasive coronary angiography. On multivariate analysis, inpatient location, positive ECG response, and abnormal MPI results were the strongest predictors of angiography. Non-traditional factors such as race/ethnicity and insurance status had a significant association with referral to angiography with Caucasians (OR 1.42, 95% CI 1.18-1.71, P < .0001) and those with private insurance (OR 1.35, 95% CI 1.13-1.62, P = .001) or Medicare (OR 1.30, 95% CI 1.08-1.56, P = .006) having higher rates of angiography despite controlling for traditional risk factors and test results.
Conclusion
Our study results indicate that non-traditional factors such as race/ethnicity and insurance status influence patient management decisions and impact the performance of downstream cardiac invasive testing after stress MPI. Higher rates of angiography in Caucasians, privately insured and Medicare patients were seen despite controlling for traditional risk factors and abnormal test results. Further research is needed to better understand these disparities, especially in the current healthcare environment.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The value of myocardial perfusion imaging (MPI) for diagnosing coronary artery disease (CAD) and the prognostic utility of perfusion imaging is well established.1 Perhaps because of this, the number of stress tests with MPI has been increasing in the US, with the proportion of stress tests with imaging growing from 59% of all stress tests in 1993-1995 to 87% in 2008 to 2010.2 Previous studies have shown that MPI results are the biggest determinant of referral for coronary angiography with a strong correlation between increasing severity and extent of perfusion defects and the rates of angiography.3,4,5,6 Other strong predictors of referral for angiography include baseline clinical factors, characteristics of presenting symptoms, previous known CAD, and the ECG response to exercise stress.3,7
In the non- acute coronary syndrome (ACS) setting, the understanding of the reasons for referral for angiography immediately following MPI is limited. In particular, the impact of variables such as race/ethnicity, socioeconomic status, insurance, and marital status on the decision to refer for cardiac catheterization is not fully understood and the degree to which these factors may contribute to referral bias remains undetermined. Prior studies have documented lower rates of cardiac catheterization in ethnic minority patients hospitalized for acute myocardial infarction (MI).8,9,10 A large cross-sectional analysis of 669,002 patients hospitalized with acute MI demonstrated that African American patients are significantly less likely to undergo coronary angiography compared to Caucasian and Hispanic patients.10 Other studies have observed lower rates of referral for angiography in African American patients as well as less frequent stress testing and revascularization than Caucasian patients.11,12 Cardiac catheterization rates have also been shown to be lower in publicly insured patients hospitalized for chest pain as well as in elderly Medicaid patients with unstable angina.8,13
Although these disparities have been observed in patients with acute MI or suspected ACS, there is limited knowledge on whether such non-clinical factors affect referral for angiography following the performance of non-invasive cardiac stress testing. Previous studies have shown gender differences in referral patterns to angiography after MPI (with women being less likely than men to undergo angiography), while other investigations have failed to show significant differences in referral rates on the basis of gender.14,15,16,17 Thus, multiple studies have indicated disparities in overall angiography rates based on race/ethnicity and insurance coverage in patients presenting with ACS but less is known about referral bias following elective non-invasive testing. Accordingly, our study was conducted in order to investigate the principal determinants of referral for coronary angiography following SPECT MPI in patients with no prior CAD, and to assess whether non-traditional factors such as race, marital status, insurance, and socioeconomic status have an impact on downstream decision-making.
Methods
Patient Population
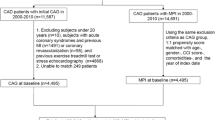
In a retrospective study approved by our Institutional Review Board, we reviewed all patients who underwent a clinically indicated stress SPECT MPI from 10/1/1997 to 8/1/2012 at Hartford Hospital, a 900-bed urban teaching hospital. Patients who underwent invasive coronary angiography within 90 days of SPECT MPI were identified. Patients with known coronary artery disease at the time of stress testing were excluded. Studies were performed for a variety of clinical indications as directed by the requesting provider and included both inpatient and outpatient studies. Data from stress testing and coronary angiography were available from prospectively collected electronic cardiology databases.
Patient demographic information, cardiac risk factors, past cardiac history, medications, hemodynamic data, and stress test results were prospectively collected at the time of the stress testing. CAD risk factors including hypertension, diabetes, and hypercholesterolemia were defined on the basis of patient history or medical record documentation. A family history of premature CAD was defined as a CAD diagnosis in a first degree relative ≤ 55 years of age. Smoking history was considered positive for either prior or current smoking. Patients were labeled as having known CAD at the time of testing if their medical history included any of the following: prior abnormal stress test, history of MI, percutaneous coronary intervention (PCI), coronary artery bypass grafting (CABG), or prior coronary angiography demonstrating evidence of atherosclerotic disease. Congestive heart failure (CHF) was defined based on patient report or documented history of systolic or diastolic heart failure.
Data about non-traditional factors were prospectively collected at the time of stress testing. Race and marital status were self-reported. Insurance status was defined as the patient’s primary insurance at the time of stress testing. Socioeconomic status was defined by the median household income by zip code using patients’ address of residence at the time of stress testing.18
Stress Protocols
Stress MPI was performed according to the American Society of Nuclear Cardiology (ASNC) protocols under the supervision of a board certified cardiologist.19 Patients were instructed to fast for at least 4 hours prior to the stress test and avoid consumption of any product containing methylxanthines for at least 12 hours prior to the stress test. Symptom limited exercise stress testing with standard Bruce or modified Bruce protocol was performed, according to American Heart Association guidelines.20 Pharmacological stress agents used included adenosine, dipyridamole, regadenoson, or dobutamine. Adenosine was administered as a 6-minute infusion at 140 mcg·kg−1·minute−1 which could be reduced to 110 mcg·kg−1·minute−1 if severe symptoms or hemodynamic effects were encountered. Dipyridamole was infused over 4 minutes at a dose of 0.56 mg·kg−1. Regadenoson was administered as a 0.4 mg/5 ml bolus followed by a 5-ml saline flush. Dobutamine was infused starting at 5-10 µcg·kg−1·minute−1, and incrementally increased every 3 minutes by 10 µcg·kg−1·minute−1 to a maximum of 40 µcg·kg−1·minute−1 until attainment of > 85% of maximal predicted heart rate. In patients unable to achieve target heart rate on dobutamine alone, atropine 0.2-0.5 mg in divided doses up to a maximum of 2 mg was administered. ECG tracings were continuously monitored during the stress tests, with recording of a 12 lead ECG and blood pressure at rest, every 2-3 minutes during stress, and during recovery. Development of any arrhythmia, ST segment changes, or symptoms was recorded. A positive ECG response to stress was defined as 1 mm or greater horizontal or downsloping ST segment, or 1.5 mm or greater upsloping ST depression, that persisted 80msec after the J point, for three consecutive beats in any lead. ECG changes that approached but did not meet these criteria were noted as borderline at the discretion of the interpreting physician. The ECG response was considered non-diagnostic in the presence of a left bundle branch block, wide right bundle branch block, paced ventricular rhythm, left ventricular hypertrophy with strain pattern, or extensive resting ST changes.
SPECT Imaging
SPECT perfusion images were obtained according to the ASNC guidelines.21 SPECT imaging was performed using a conventional dual head Na I camera (Cardio 60 or Cardio MD, Philips/ADAC Laboratories, Andover, MA USA). Attenuation correction with a Gd-153 line source (Vantage Pro, Philips/ADAC) was used when available. Radioisotope doses were weight-adjusted.
Interpretation of MPI was performed by board certified nuclear cardiologists. The extent and severity of perfusion defects were quantified at the time of the clinical read using the standard 17 myocardial segment model, with each segment scored using a 5 point scale (0 = normal tracer uptake, 1 = mildly reduced tracer uptake, 2 = moderately reduced tracer uptake, 3 = severely reduced tracer uptake and 4 = absent tracer uptake). Myocardial perfusion was assessed using Summed Stress Score (SSS), Summed Rest Score (SRS) and Summed Difference Score (SDS). Using the 5 point scale, SSS is the sum of all the 17 myocardial segments points at stress, SRS is the sum at rest, and SDS is the difference between SSS and SRS. An abnormal MPI result was defined as a summed stress score (SSS) ≥ 4. Results of MPI were further stratified by SSS, into normal perfusion (SSS ≤ 3), mildly abnormal (SSS = 4-8), moderately abnormal (SSS = 9-13), and severely abnormal (SSS ≥ 14). Semi-quantitative perfusion results were reported based on non-attenuation corrected images as attenuation correction was not universally available over the time period studied.
Coronary Angiography
The decision for referral for coronary angiography was clinically driven by the treating clinical cardiologist. Results of invasive coronary angiography performed within 90 days after the MPI study were obtained and recorded. Interpretation of coronary angiograms was done by board certified interventional cardiologists and quantified at the time of the clinical read. Obstructive CAD was defined as ≥ 70% stenosis in any of the three main epicardial coronary arteries or their major branches or ≥ 50% stenosis of the left main coronary artery. Atherosclerosis with luminal narrowing < 50% of the left main coronary artery and < 70% of a major epicardial vessel or branch was considered as nonobstructive CAD. No angiographic evidence of atherosclerosis was labeled as normal coronary arteries.
End Points
The primary endpoint was defined as referral for angiography following stress SPECT MPI. Traditional demographic and cardiac risk factors as well as non-traditional factors including gender, ethnicity, insurance type, marital, and socioeconomic status were included in the analysis as potential factors influencing referral to angiography. A secondary analysis assessed how the traditional and non-traditional factors were associated with abnormal MPI results.
Statistical Analysis
Continuous variables are reported as mean ± standard deviation and categorical data as percentages. Means of continuous variables were compared using a two-tailed t-test or one-way ANOVA. Chi-square test or Fisher’s exact test for small sample sizes were employed for categorical variables. Univariate and multivariate logistic regression analysis of variables associated with referral for angiography were performed. Variables with a P value ≤ .10 in the univariate analysis were included in the multivariate analysis. A P value ≤ .05 was considered significant. SPSS 25 (IBM, Armonk, NY USA) was used for statistical analysis.
Results
Demographic Comparison
A total of 27,895 patients without known CAD who underwent exercise or pharmacological stress MPI during the specified time period were analyzed (Table 1). The mean age of all patients was 60.7 ± 13.5 years, 54.9% were women, and inpatients accounted for a slight majority of the total (52.4%). Hypertension (61.4%) and hyperlipidemia (49.6%) were the most common traditional CAD risk factors. A greater proportion of the patients were Caucasian (69.7%), married (54.2%), and had private insurance (46.0%). African American and Hispanic minorities accounted for 10.2% and 15.7% of the population, respectively. Out of the total patient cohort 49.4% underwent exercise stress and positive ECG responses were seen in 15.2% of all patients. Abnormal MPI results were observed in 18.3%, 12.9% had mildly abnormal MPI (SSS 4-8), 3.0% demonstrated moderately abnormal MPI (SSS 8-13), and 2.0% had severely abnormal MPI (SSS ≥ 14) results.
Out of the entire study cohort, 2,150 patients (7.7%) underwent invasive coronary angiography (Table 1). Patients who underwent angiography were older had a greater proportion of men and had a greater burden of traditional cardiac risk factors except family history. Patients who underwent pharmacologic stress tests and inpatients were more likely to undergo angiography. Those undergoing angiography had larger and more severe perfusion defects and a greater degree of ischemia than patients who did not. The SSS (7.3 ± 6.3, vs 1.5 ± 2.9, P < .0001), SRS (2.6 ± 4.6 vs 1.0 ± 2.5, P < .0001), and SDS (4.3 ± 4.9 vs 0.6 ± 1.7), were all higher in the angiography cohort compared to those who did not undergo angiography. Interestingly, 454 normal MPI studies (1.6% of the total population) underwent coronary angiography and 3,404 abnormal MPI studies (12.2% of the total population) did not undergo coronary angiography. The mean left ventricular ejection fraction was lower, but still normal, among patients undergoing angiography, 56% ± 13% compared to 64% ± 9% in the no angiography group.
With regard to the non-traditional factors evaluated, the percentage of the Caucasian population in the angiography cohort was significantly higher compared to the non-angiography cohort (73.9% vs 69.3%, P < .0001), while there was no significant difference for African Americans and Hispanics. There were also significant differences in privately insured and Medicare patients between those who were referred for angiography compared to those who were not referred. A greater proportion of Medicare patients were found in the angiography cohort (40.8% vs 35.3%, P < .0001) and a smaller proportion of private patients were present (42.1% vs 46.3%, P = .0003). There was no significant difference in marital status or median household income with regard to angiography.
Univariate and Multivariate Association to Referral for Angiography
Logistic regression univariate analysis found advancing age, male gender, obesity, all traditional cardiac risk factors except family history of CAD, inpatient status, and pharmacologic stress all had a significant association with increased referrals for angiography (Table 2). Univariate analysis demonstrated that a positive ECG response to stress (OR 3.2, 95% CI 2.9-3.5, P < .0001) and a non-diagnostic response (OR 1.2, 95% CI 1.1-1.3, P < .0001) resulted in increased referral to cardiac catheterization. Abnormal MPI findings resulted in increased referral to cardiac catheterization, with an odds ratio of 24.5 (95% CI 22.0-27.4, P < .0001). The likelihood of angiography increased with increasing severity of MPI abnormalities, with odds ratios of 9.0, 28.8, and 37.4 for mild, moderate, and severely abnormal MPI, respectively (P < .0001). The extent of stress perfusion abnormalities as measured by SSS (OR 1.29, 95% CI 1.28-1.31) and ischemic burden as assessed by SDS (OR 1.47, 95% CI 1.44-1.49) both had a significant association with increased rates of angiography (P < .0001). Lower left ventricular ejection fraction was also found to be associated with referral to angiography (P < .0001).
With respect to the non-traditional risk factors, univariate analysis revealed that Caucasian patients were more likely to undergo angiography (OR 1.16, 95% CI 1.06-1.28, P = .002) and Hispanic patients less likely (OR 0.83, 95% CI 0.73-0.95, P = .005). African American race was not statistically significantly associated with the referral to coronary angiography. Medicare patients were referred for angiography more often (OR 1.32, 95% CI 1.21-1.45, P < .0001) and private insurance less often (OR 0.91, 95% CI 0.83-0.99, P = .03). Marital status and socioeconomic status were not significantly associated with angiography referral rates.
After multivariate adjustment including all univariate predictors with a P value < .1, traditional risk factors of diabetes mellitus and hyperlipidemia remained significantly associated with referral to angiography while gender and weight lost significance (Figure 1). Age, interestingly, lost strength of association with a decrease in Chi-square and the OR point estimate dropped below 1 making advanced age protective in the multivariate model. Inpatient status remained predictive of angiography while pharmacologic stress lost statistical significance. Positive ECG responses and abnormal MPI results continued to have strong associations with angiography, with odds ratios of 2.6 (95% CI 1.94-3.55, P < .001) and 26.7 (95% CI 22.9-31.1, P < .0001), respectively. After multivariate adjustment, race/ethnicity and insurance status retained a significant association with the likelihood of angiography. Caucasian patients were more likely to undergo angiography (OR 1.42, 95% CI 1.18-1.71, P < .0001) and Hispanic race/ethnicity lost any statistically significant association. Both Medicare and private insurance patients were more likely to undergo angiograms (OR 1.30, 95% CI 1.08-1.56, P = .006 and OR 1.35, 95% CI 1.13-1,62, P = .001).

Odds Ratios for the association of traditional and non-traditional factors to referral for invasive coronary angiography
Interaction of ECG and MPI Results
Analysis of patients based on MPI results finds similarities between patients with abnormal MPI and those undergoing angiography, but not complete agreement (Table 3). Traditional cardiac risk factors, inpatient location, pharmacologic stress, and abnormal study results were all more prevalent in patients with abnormal MPI results as expected. There was no difference in the proportion of Caucasians based on MPI results while African Americans were more prevalent and Hispanics less prevalent in the abnormal MPI group. Marital status, including married and widowed status, showed differences based on perfusion results as did private insurance and Medicare.
The univariate and multivariate logistic regression analysis of variables predicting an abnormal MPI result can be seen in Supplemental Table 1. In the multivariate analysis, traditional factors such as age, gender, and diabetes along with inpatient status, pharmacologic stress, and abnormal ECG results were statistically significantly associated with abnormal MPI results similar to the angiography analysis. Differences were seen with race/ethnicity with no association found with Caucasians but Hispanics being less likely to have an abnormal MPI study (OR 0.71, 95% CI 0.62-0.82, P < .0001). Only Medicare patients were associated with MPI results (OR 1.42, 95% CI 1.19-1.69, P < .0001), similar to angiographic referral without an association with private insurance. Marital status showed no association to MPI results after multivariate correction which corresponded to its angiography findings.
As referral to invasive angiography was most strongly related to stress test results, the interaction of MPI, stress ECG results, and non-traditional variables were explored (Figures 2A-D). Among patients with normal MPI results (SSS < 4) only 2.6% underwent angiography, compared to 19.5%, 43.7% and 50.2% with mildly abnormal (SSS 4-8), moderately abnormal (SSS 9-13), and severely abnormal (SSS ≥ 14) MPI results, respectively (P < .0001). Results in Figure 2A demonstrate that a positive ECG response during stress resulted in more frequent referrals to angiography with any degree of MPI findings (normal or mild, moderate, and severely abnormal MPI results), compared to negative, borderline, or non-diagnostic ECG responses to stress (P < 0.0001). Figure 2B indicates that in patients with moderately abnormal or severely abnormal MPI results, those with private insurance or no insurance were referred more frequently for coronary angiography compared to patients receiving Medicaid and Medicare. The Chi-square for independence for all moderate and severely abnormal perfusion was P = .001 and P < .0001. As demonstrated in Figure 2C, there was a trend for Caucasian patients to undergo angiography more frequently with any degree of abnormal MPI results. This finding only reached statistical significance in the mildly abnormal MPI group (P < .0001). Married patients with mild, moderate, or severely abnormal MPI findings had higher rates of coronary angiography compared to single or widowed patients (Figure 1D). This difference reached statistical significance in the mild group (P = .04) and severe group (P = .0003).

(A) The effect of the interaction of stress ECG results and MPI results on referral to coronary angiography. (B) The effect of the interaction of insurance status and MPI results on referral to coronary angiography. (C) The effect of the interaction of race/ethnicity and MPI results on referral to coronary angiography. (D) The effect of the interaction of marital status and MPI results on referral to coronary angiography
The results of the stress test, a surrogate for the prevalence of CAD, did not vary greatly based on race/ethnicity, marital status, or insurance type (Supplemental Table 2A-C). A positive ECG was seen in 10-17% of patients in these subgroups and in 15.2% of the total population, while an abnormal MPI result was seen in 12-24% and in 18% of the total population. Thus, it would seem that much of the variation in referral patterns within the non-traditional populations studied stems from factors not related to CAD or test results. Medicare and private insurance were the only insurance types with a significant association with angiography in the multivariate analysis and they both had a greater proportion of Caucasian patients who were also more likely to undergo angiography in the multivariate analysis. While there were more widowed patients in the Medicare cohort and more married patients in the private insurance cohort, marital status was not significantly associated with referral to coronary angiography. In African American and Hispanic patients who were less likely to undergo angiography in the multivariate model, there were more Medicaid patients (who tended not to go for angiography) and fewer private insurance and Medicare patients, a trend which was particularly true in the Hispanic population. These cohorts again had more single patients and fewer married patients.
Interaction of Time Period
The study duration was divided into three time periods of approximately 5 years each and the changes in traditional and non-traditional factors analyzed (Table 4). Clinically significant increases in the burden of traditional cardiac risk factors were seen over time without meaningful changes in age or gender proportions. Although statistically significant, the proportions of race/ethnic groups and marital status did not meaningfully change over time. Fluctuations were seen in the proportions of insurance over time with a trend toward more Medicare and less Medicaid over time. In addition, the referral rates to coronary angiography were assessed on a yearly basis showing an average referral rate of 7.7% (Figure 3). There was an initial trend toward decreasing rates of referral in the first decade and then a slight increase in the last 5 years.

The percentage of patients who had coronary angiography within 90 days after MPI study displayed over the study period
Discussion
This study population confirms many previous findings such as the overall rates of angiography among patients undergoing non-invasive testing (19.5%, 43.7% and 50.2% for mild, moderate, and severely abnormal studies), as well as the ECG response to stress and MPI findings as the strongest predictors of referral for angiography.1,3,4,5,6 Previously seen gender disparities were not replicated - while male gender was associated with increased angiography referral in the univariate analysis, statistical significance was lost in the multivariate model.22 This study adds to this basic foundation by demonstrating differential rates of angiography based on race/ethnicity and insurance status following stress MPI. These factors were independently associated with referral for angiography, even after adjustment for other demographics, clinical risk factors and exercise stress test results. Furthermore, these disparities persisted regardless of the severity of the MPI findings and were observed even in those patients with moderately and severely abnormal MPI results. The management of patients with significant ischemia is of course in flux with the results of the recently released ISCHEMIA trial and the impacts of non-traditional risk factors are yet to be seen.23
Of particular interest in our study was the investigation of whether non-traditional, non-clinical factors influenced coronary angiography referral rates above and beyond traditional cardiac risk factors, ECG results, and MPI findings. After multivariate adjustment, race/ethnicity remained significantly associated with referral for angiography, with Caucasians being 42% more likely to undergo angiography (OR 1.42) while African American and Hispanic race/ethnicity not being significantly associated with angiography. This was also seen regardless of the degree of perfusion abnormalities on MPI, with African Americans and Hispanics being less likely to undergo angiography with any degree of abnormal MPI results. These findings are similar to prior studies which have shown racial differences in angiography rates in ethnic minority patients hospitalized for acute MI.8,9,10 We found different distributions of insurance coverage and marital status among ethnic groups while other possible contributing patient factors were not investigated including educational status, patient preferences, and negative attitudes toward invasive testing. Most studies suggest patient preference or patient refusal seem to account for only a small part of racial and gender differences in angiography rates.24,25,26 A previous study of 7,927 patients in three different community hospitals showed that after controlling for multiple factors, race was a significant negative determinant of referral for angiography, with African American patients less likely to be referred.12 However, once referral for angiography was made, there were no racial differences in undergoing the procedure, with African American patients being as likely to have angiography as Caucasian patients. An earlier review of ethnic differences in myocardial perfusion imaging found that while there were disparities in absolute cardiac event rates between ethnic groups despite similar imaging results, the prognostic ability of perfusion imaging appeared to be consistent and of similar magnitude across ethnic groups.27
Insurance status proved to be a significant predictor as private insurance patients were referred for angiography 35% more often (OR 1.35) and Medicare patients 30% more (OR 1.30). After stratifying based on severity of abnormal perfusion, patients with private insurance with abnormal MPI results had higher rates of angiography compared to other insurance categories. While our data do not provide the capacity to explain these differences, the financial incentives inherent in performing procedures have been noted in other similar settings. Previous literature has demonstrated lower cardiac catheterization rates in publicly insured patients hospitalized for chest pain and in elderly Medicaid patients with unstable angina.8,13 In a retrospective review of 3,122 patients over 65 years of age hospitalized for unstable angina in 22 hospitals, these patients underwent angiography less frequently after adjustment for demographics, comorbidities, and prior revascularization, but this finding was not present after adjusting for hospital characteristics.13 This particular study does come from data obtained a decade earlier than the current study which may limit the possible comparisons. Other studies have demonstrated that angiography was underutilized in Medicaid patients with otherwise appropriate criteria to undergo the test.8 Differential rates of angiography utilization/referral based on geographic variations in ethnic compositions and socioeconomic status were also observed in a large study evaluating rates of downstream testing after stress MPI in 80,676 patients with referral rates ranging from 3.8% in Los Angeles to 14.8% in St. Louis.28 Our findings would extend these results to suggest patients with private insurance and Medicare have higher rates of angiography, even after risk stratification with SPECT MPI.
Marital status was not found to have a significant association with subsequent angiography. This was demonstrated by the distribution of marital status among patients with and without subsequent angiography and based on multivariate analysis. In patients with abnormal MPI studies there was a trend toward married patients being referred more frequently for angiography than single, divorced or widowed patients. Possible reasons for this difference could involve greater understanding and shared decision-making on obtaining angiography with spouses, who might serve as sources of emotional and psychological support. Other potential reasons could be that marriage or the presence of spouses compels a more thorough workup of these patients, driving downstream testing and referrals to angiography.29 Other socioeconomic factors such as income did not have an independent association with referral for angiography in this cohort.
Limitations
This was a retrospective study that contains many of the inherent limitations of such investigations. Although the sample size was large and spanned a long period of time, this was a single-center study, so it is unclear if these results can be generalized to other populations. We could not evaluate or account for coronary angiography performed at other hospitals although our medical center is the largest in the area and one might anticipate that follow-up testing would be done in the same medical center as stress testing. The study design did not allow for assessment of patient preferences, educational status, physician perceptions about patient’s attitudes toward angiography, patient compliance, and physician preferences. Patient refusal of angiography was also not assessed or accounted for in this study. While presenting symptoms for stress testing have been shown to be related to subsequent angiography, these data were not reliably available for our cohort, nor were data on preceding acute coronary syndromes. Acute chest pain versus more chronic symptoms, pre-operative assessments, and post-MI risk stratification might all have different thresholds for referral for angiography. The comparison to previous studies on the topic may not be directly applicable given the differences in study populations and ours as well as the different time periods assessed. As long-term cardiovascular outcomes were not assessed, the clinical impact of varying rates of referral to angiography seen in the different subgroups could not be ascertained. The socioeconomic status data likely provided uninterpretable data given paucity in diversity of the household incomes seen in the study. The median household incomes were derived from zip codes using patients’ address of residence at the time of stress testing and were based on 2010 US Census data which might not have been applicable to patients throughout the study’s time period.
Conclusion
Our study results indicate that factors such as race/ethnicity and insurance influence patient management decisions after stress testing with perfusion imaging and impact the performance of downstream cardiac invasive testing. Although traditional risk factors and abnormal test results are the strongest predictors of referral to invasive angiography, non-traditional factors such as race/ethnicity and insurance status also have an impact on the clinical decision for referral to angiography, resulting in higher rates of angiography/stronger association with angiography in Caucasians, privately insured and Medicare patients despite controlling for traditional risk factors and abnormal test results. Further research is needed to better understand these disparities, especially in the current healthcare environment.
New Knowledge Gained
This is one of the first studies to specifically evaluate the influence of non-traditional factors such as race/ethnicity, insurance status, and marital status on post-MPI referral rates to angiography. While previously described factors such as age, traditional cardiac risk factors, stress ECG findings, and MPI results were again associated with angiography, this study revealed significant disparities in angiography referral rates based on race/ethnic and insurance type regardless of the severity of abnormal MPI findings. After adjustment for clinical risk factors and results of exercise stress and MPI testing, higher rates of angiography were seen in Caucasians, privately insured and Medicare patients.
Abbreviations
- ACS:
-
Acute coronary syndrome
- CAD:
-
Coronary artery disease
- CABG:
-
Coronary artery bypass grafting
- PCI:
-
Percutaneous coronary intervention
- SPECT:
-
Single photon emission computed tomography
- MPI:
-
Myocardial perfusion imaging
- MI:
-
Myocardial infarction
- CHF:
-
Congestive heart failure
- SSS:
-
Summed Stress Score
- SRS:
-
Summed Rest Score
- SDS:
-
Summed Difference Score
References
Dowsley T, Al-Mallah M, Ananthasubramaniam K, Dwivedi G, McArdle B, Chow BJ. The role of noninvasive imaging in coronary artery disease detection, prognosis, and clinical decision making. Can J Cardiol 2013;29:285-96.
Ladapo JA, Blecker S, Douglas PS. Physician decision making and trends in the use of cardiac stress testing in the United States: An analysis of repeated cross-sectional data. Ann Intern Med 2014;161:482-90.
Hannoush H, Shaar K, Alam S, Nasrallah A, Sawaya J, Dakik HA. Analysis of referral patterns, predictive accuracy, and impact on patient management of myocardial perfusion imaging in a new nuclear cardiology laboratory. J Nucl Cardiol 2003;10:148–53.
Hachamovitch R, Nutter B, Hlatky MA, Shaw LJ, Ridner ML, Dorbala S, et al. Patient management after noninvasive cardiac imaging results from SPARC (Study of myocardial perfusion and coronary anatomy imaging roles in coronary artery disease). J Am Coll Cardiol 2012;59:462-74.
Ladenheim ML, Pollock BH, Rozanski A, Berman DS, Staniloff HM, Forrester JS, et al. Extent and severity of myocardial hypoperfusion as predictors of prognosis in patients with suspected coronary artery disease. J Am Coll Cardiol 1986;7:464-71.
Amanullah AM, Kiat H, Hachamovitch R, Cabico JA, Cohen I, Friedman JD, et al. Impact of myocardial perfusion single-photon emission computed tomography on referral to catheterization of the very elderly. Is there evidence of gender-related referral bias? J Am Coll Cardiol 1996;28:680-6.
Koh AS, Gao F, Chin CT, Keng FY, Tan RS, Chua TS, et al. Differential risk reclassification improvement by exercise testing and myocardial perfusion imaging in patients with suspected and known coronary artery disease. J Nucl Cardiol 2015. https://doi.org/10.1007/s12350-015-0253-x.
Barnhart J, Bernstein SJ. Is coronary angiography underused in an inner-city population? Ethn Dis 2006;16:659-65.
Barnhart JM, Wassertheil-Smoller S, Monrad ES. Clinical and nonclinical correlates of racial and ethnic differences in recommendation patterns for coronary revascularization. Clin Cardiol 2000;23:580-6.
Bertoni AG, Goonan KL, Bonds DE, Whitt MC, Goff DC Jr, Brancati FL. Racial and ethnic disparities in cardiac catheterization for acute myocardial infarction in the United States, 1995–2001. J Natl Med Assoc 2005;97:317-23.
Lucas FL, DeLorenzo MA, Siewers AE, Wennberg DE. Temporal trends in the utilization of diagnostic testing and treatments for cardiovascular disease in the United States, 1993-2001. Circulation 2006;113:374-9.
LaVeist TA, Morgan A, Arthur M, Plantholt S, Rubinstein M. Physician referral patterns and race differences in receipt of coronary angiography. Health Serv Res 2002;37:949-62.
Pamboukian SV, Funkhouser E, Child IG, Allison JJ, Weissman NW, Kiefe CI. Disparities by insurance status in quality of care for elderly patients with unstable angina. Ethn Dis 2006;16:799-807.
Hachamovitch R, Berman DS, Kiat H, Bairey-Merz N, Cohen I, Cabico JA, et al. Gender-related differences in clinical management after exercise nuclear testing. J Am Coll Cardiol 1995;26:1457-64.
Miller TD, Roger VL, Hodge DO, Hopfenspirger MR, Bailey KR, Gibbons RJ. Gender differences and temporal trends in clinical characteristics, stress test results and use of invasive procedures in patients undergoing evaluation for coronary artery disease. J Am Coll Cardiol 2001;38:690-7.
Zeltser R, Tortez LM, Druz RS, Kozikowski A, Makaryus AN, Lesser M, et al. Downstream resource utilization following SPECT: Impact of age and gender. J Nucl Cardiol 2016;24:1657-61.
Tobin JN, Wassertheil-Smoller S, Wexler JP, Steingart RM, Budner N, Lense L, et al. Sex bias in considering coronary bypass surgery. Ann Intern Med 1987;107:19-25.
United States Census Bureau. http://www.census.gov/quickfacts/table/HSG030210/09; 2010-2014.
Henzlova MJCM, Hansen CL, Taillefer R, Yao SS. ASNC imaging guidelines for nuclear cardiology procedures: Stress protocols and tracers. J Nucl Cardiol 2009;16:331.
Fletcher GF, Ades PA, Kligfield P, Arena R, Balady GJ, Bittner VA, et al. Exercise standards for testing and training: A scientific statement from the American Heart Association. Circulation 2013;128:873-934.
Holly TA, Abbott BG, Al-Mallah M, Calnon DA, Cohen MC, DiFilippo FP, et al. Single photon-emission computed tomography. J Nucl Cardiol 2010;17:941-73.
Hill E, Hachamovitch R. Has anyone been listening? Post-SPECT MPI referral rates to catheterization. J Nucl Cardiol 2016;24:1662-5.
Maron DJ, Hochman JS, Reynolds HR, Bangalore S, O’Brien SM, Boden WE, et al. Initial invasive or conservative strategy for stable coronary disease. N Engl J Med 2020;382:1395-407.
Gordon HS, Paterniti DA, Wray NP. Race and patient refusal of invasive cardiac procedures. J Gen Intern Med 2004;19:962-6.
Rathore SS, Ordin DL, Krumholz HM. Race and sex differences in the refusal of cardiac catheterization among elderly patients hospitalized with acute myocardial infarction. Am Heart J 2002;144:1052-6.
Heidenreich PA, Shlipak MG, Geppert J, McClellan M. Racial and sex differences in refusal of coronary angiography. Am J Med 2002;113:200-7.
Noble G, Heller GV. Ethnic differences in myocardial perfusion imaging—Identifying patients at higher risk. US Cardiol 2004;1:72-5.
Mudrick DW, Cowper PA, Shah BR, Patel MR, Jensen NC, Peterson ED, et al. Downstream procedures and outcomes after stress testing for chest pain without known coronary artery disease in the United States. Am Heart J 2012;163:454-61.
Barbash IM, Gaglia MA Jr, Torguson R, Minha S, Satler LF, Pichard AD, et al. Effect of marital status on the outcome of patients undergoing elective or urgent coronary revascularization. Am Heart J 2013;166:729-36.
Disclosures
All funding and support for this work came from within the Division of Cardiology at Hartford Hospital. There was no outside funding, grant, or industry support.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The authors of this article have provided a PowerPoint file, available for download at SpringerLink, which summarizes the contents of the paper and is free for re-use at meetings and presentations. Search for the article DOI on SpringerLink.com.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Gowdar, S., Hussain, N., Ahlberg, A.W. et al. Non-traditional factors affecting referral for coronary angiography following SPECT myocardial perfusion imaging. J. Nucl. Cardiol. 29, 1141–1155 (2022). https://doi.org/10.1007/s12350-020-02419-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-020-02419-3