
Abstract
Candesartan cilexetil is an angiotensin II receptor blocker and it is widely used to treat hypertension and heart failure. This drug is a prodrug that rapidly converts to candesartan after oral administration. Candesartan is metabolized by cytochrome P450 2C9 (CYP2C9) enzyme or uridine diphosphate glucurinosyltransferase 1A3, or excreted in an unchanged form through urine, biliary tract and feces. We investigated the effect of genetic polymorphism of CYP2C9 enzyme on drug pharmacokinetics using physiologically based pharmacokinetic (PBPK) modeling. In addition, by introducing the age and ethnicity into the model, we developed a model that can propose an appropriate dosage regimen taking into account the individual characteristics of each patient. To evaluate the suitability of the model, the results of a clinical trial on twenty-two healthy Korean subjects and their CYP2C9 genetic polymorphism data was applied. In this study, PK-Sim® was used to develop the PBPK model of candesartan.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Frequently, a drug administered to a patient through proper diagnosis and prescription does not provide the desired therapeutic effects (Noetzli and Eap 2013). In addition, serious adverse drug reactions may occur in patients who normally use the drug as prescribed. These adverse reactions can significantly influence the quality of life of the patient and, in severe cases, may impose risk to the patient’s life. In order to solve these problems, precision medicine, which treats patients considering the individual patient characteristics that may influence the drug effects, such as individual demographic data, enzyme genotype and life style, may be a solution (Jameson and Longo 2015; König et al. 2017). Right dose, one of the most important factors in precision medicine, considers the individual characteristics of these patients and maintains the plasma concentration of the drug properly within the therapeutic window, providing the most appropriate treatment effect to the patient and minimizing the risk of adverse reactions (Lesko and Schmidt 2012). Physiologically based pharmacokinetic (PBPK) modeling a method of predicting drug concentration in plasma or organs by applying individual physiological characteristics, drug characteristics, and biological responses to drugs. Individual differences such as gender, age, weight, genotype, disease severity, co-administered drugs, lifestyle and environmental factors that mainly affect drug responses can be introduced into the modeling (Chetty et al. 2014). In addition, dose regimens such as dose changes, routes of administration, and intervals of administration can be introduced into the modeling. Thus, the individual pharmacotherapy can be introduced by using PBPK modeling.
Candesartan cilexetil is an angiotensin II receptor blocker and it is widely used to treat hypertension and heart failure (AstraZeneca 2005). It is a prodrug that is completely converted to the active metabolite candesartan by the carboxylesterase 2 (CES2) enzyme (Laizure et al. 2013; Nishimuta et al. 2014) in the intestinal wall during absorption. Candesartan is highly selective of AT1 subtype of angiotensin II receptor (Gleiter and Mörike 2002), it undergoes hepatic metabolism through the cytochrome P450 2C9 (CYP2C9) enzyme or is excreted in an unchanged form though urine, biliary tract and feces (Gleiter and Mörike 2002; Zhou et al. 2009). Also, it undergoes glucuronidation through uridine diphosphate glucurinosyltransferase 1A3 (Zhou et al. 2009).
CYP2C9 enzyme is mainly expressed in the liver. It accounts for 15–20% of the total cytochrome P 450 enzymes (Shimada et al, 1994; Mizutani, 2003). About 16% of all drugs currently are metabolized by the CYP2C9 enzyme, such as antidiabetic agents (glipizide, glimepiride and tolbutamide), antihypertensive agents (losartan and candesartan) and some non-steroidal anti-inflammatory drugs (NASIDs). It also metabolizes warfarin and phenytoin, which have a narrow therapeutic index (Kumar et al. 2008). To date, 71 CYP2C9 allele have been confirmed (https://www.pharmvar.org/gene/CYP2C9). In Caucasians, CYP2C9*2 allele (rs1799853) has been identified with a frequency of 8–19.1% and CYP2C9*3 allele (rs1057910) has been identified with a frequency of 3.3–16.2% (García-Martín et al. 2006). However, in Asians, the CYP2C9*2 allele has rarely been identified (0–0.1%), but the CYP2C9*3 allele has been identified at a frequency of 0.07–6.0% (Bae et al. 2005, 2011; Nakai et al. 2005; García-Martín et al. 2006). In addition, CYP2C9*13 (rs72558187) has been identified at a very low rate with a frequency of only 0.2–1% in Asians (Bae et al. 2011). Since the pharmacokinetic changes by genetic polymorphism of the CYP2C9 enzyme have been reported in various drugs (Lee et al. 2015; Kim et al. 2017; Byeon et al. 2018), it may be necessary to take into account the pharmacokinetic changes of candesartan metabolized by the CYP2C9 enzyme.
In this study, we developed the PBPK modeling of candesartan for prediction of the pharmacokinetic differences of candesartan due to the genetic polymorphism of the CYP2C9 enzyme. In addition, parameters of age groups and ethnic groups were introduced in this modeling. The accuracy of the PBPK model and predicted pharmacokinetic data was evaluated using actually conducted pharmacokinetic data from various ethnic groups with appropriate equations. After evaluating the fit of the model, the model has been applied to pediatric patient groups of various ethnicity and genotypes. As a result, this PBPK model is expected to propose an appropriate drug regimen based on individual patient characteristics.
Methods
In vivo clinical study of candesartan
Subjects
In the pharmacokinetic study of candesartan cilexetil, 22 healthy Korean male subjects with CYP2C9*1/*1 (n = 12, mean age 25.1 ± 1.3 years, weight 70.0 ± 5.0 kg, height 177.5 ± 4.3 cm and body max index (BMI) 22.2 ± 1.2 kg/m2), CYP2C9*1/*3 (n = 8, mean age 25.2 ± 1.3 years, weight 70.1 ± 5.2 kg, height 175.1 ± 3.6 cm and BMI 22.9 ± 2.0 kg/m2) and CYP2C9*1/*13 (n = 2, mean age 25.0 ± 1.4 years, weight 68.5 ± 7.8 kg, height 174.5 ± 0.7 cm and BMI 22.5 ± 2.7 kg/m2) genotypes were selected. Peripheral blood leukocytes were used to isolate genomic DNA using the Genomic DNA Kit (Wizard®, Promega, Madison, WI, USA). After isolation of genomic DNA, we used the polymerase chain reaction restriction fragment length polymorphisms method for CYP2C9*2, *3 and *13 allele analysis as described previously (Bae et al. 2005). All subjects were between 24 and 29 years old, and BMI were between 20 and 26 kg/m2. All subjects had no health problem, including the vital signs (such as body temperature, blood pressure, and pulse), physical examination, and medical history. For the study, all subjects were strictly forbidden to take any drugs, alcohol, or caffeine containing beverages for 10 days before and during the study.
Study protocol
This pharmacogenomic study was conducted according to the Helsinki Declaration on Biomedical Research and the protocol was approved by the Institutional Review Board of Metro Hospital (Anyang, Republic of Korea). Written informed consent was obtained from each participant prior to enrillment. Single oral dose of candesartan cilexetil (Atacand, AstraZeneca Korea, 8 mg, two tablets) with 240 mL of water was provided to all subjects. We collected blood samples before the drug administration and at 0.5, 1, 1.5, 2, 3, 4, 6, 8, 10, 12, 24 and 36 h after the administration of candesartan cilexetil. All blood samples were centrifuged at 3000 rpm for 10 min. After centrifuge, the plasma samples were collected and stored at −70°C until analysis.
Detection of candesartan concentration in human plasma
High performance liquid chromatography-fluorescence detector was used to detect candesartan concentration in human plasma. Briefly, 0.5 mL of plasma was spiked with 10 μL of an internal standard (valsartan, 20 μg/mL) into a glass tube, and the mixture was acidified with 100 μL of 1 M HCl. After vortex mixing with 6 mL of diethyl ether, the organic phase was moved into a clean glass tube and evaporated at 40°C under a constant flow of nitrogen gas. The residue was reconstituted with 500 μL of the mobile phase. Separation of candesartan and internal standard was performed using Luna C18 CN column (4.6 × 250 mm, 5 µm, Phenomenex, Inc., Torrance, CA, USA). The mobile phase consisted of a mixture of 20 mM phosphate buffer-acetonitrile (65:35, V/V, pH adjusted to 3.5). The flow rate was 1.0 mL/min, and the column oven temperature was 30°C. The effluents were detected with fluorescence detection at excitation and emission wavelengths of 250 nm and 375 nm, respectively. The lower limit of quantification for candesartan was 1 ng/mL. The linear range of the standard curves for candesartan was from 1 to 300 ng/mL in plasma ( r2 = 0.9998), in which the mean accuracy of candesartan was 89.38–106.43%. The coefficients of variation (within-day and between-day precision) of candesartan in plasma were 0.73–13.57%.
Enzyme kinetic assay
To measure the drug metabolism of candesartan by CYP2C9, an enzyme kinetics analysis using a recombinant enzyme was performed. Stock solutions of candesartan were prepared at a concentration of 20 mM using dimethyl sulfoxide. 170 µL of 100 mM potassium phosphate buffer (pH 7.4), 10 µL of the prepared candesartan (20–10,000 µM), and 10 μL of CYP2C9 recombinant protein (stored at a concentration of 100 pmol) were transferred into a 1.5 mL glass tube. After pre-incubation (37°C for 10 min), 10 μL of NADPH generation system (6.6 mM glucose-6-phosphate, 0.8 U/mL glucose-6-phosphate dehydrogenase, 2.6 mM NADP+, and 6.6 mM MgCl2) was added to initiate the reaction (final volume: 200 µL). The incubation proceeded for 30 min, and 200 µL of chilled acetonitrile containing an internal standard was added to terminate the reaction. The mixture was centrifuged for 10 min at 4°C at 13,000 rpm, and then the supernatant was collected and injected to LC–MS/MS to analyze for the formation of O-desethyl candesartan. The O-desethyl candesartan was measured using the method of Hanatani et al. (2001), and calculation of enzyme activity was performed using the Michaelis–Menten equation from GraphPad Prism 6 (San Diego, CA, USA).
Development of candesartan PBPK modeling
PBPK modeling of candesartan was developed using PK-Sim® 7.4 (Bayer AG, Wuppertal, Germany). Quantitative mechanistic framework on human, system-specific properties and drug properties were used to develop PBPK modeling of candesartan. For demographic data used for PBPK modeling, the data from subjects of each clinical studies, were used. Physicochemical and pharmacokinetic (absorption, distribution, metabolism and excretion) data of candesartan cilexetil and candesartan used to develop PBPK modeling are represented in Tables 1 and 2. The time for dissolution of 80% of candesartan cilexetil was measured through the peddle method and applied to modeling. Data on molecular weight, unbound fraction, solubility, pKa, and lipophilicity in plasma were obtained from the DrugBank database (https://go.drugbank.com/drugs/DB13919). The specific intestinal permeability was calculated using literature information (Thelen et al. 2011), and partition coefficients for candesartan cilexetil and candesartan were calculated using Rogers and Rowland method (Rodgers and Rowland 2006) for candesartan cilexetil and candesartan.
PBPK model validation
For evaluation of the candesartan PBPK model, acceptance criteria based on the observed human pharmacokinetic data were calculated using the appropriate equation (Eqs. 1–3) (Abduljalil et al. 2014).
CV%, the coefficient of variation, represents the observed mean of the area under curve (AUC), Cmax, and Tmax value from identified clinical trials data; \(\upsigma\) is the variability of PK parameter that is calculated using PK in the population; \(\overline{x}\) is the average of the observed PK data; and N is the average number of subjects participating in the PK study. Each A and B are maximum and minimum boundaries for acceptable fold error, respectively.
Population simulation in diverse ethnic groups were performed to evaluate the candesartan PBPK model. These simulations were based on previously published human clinical PK reports. Demographic data (such as age, height, weight, BMI, and portion of female) and ethnic groups were also based on published clinical PK reports (Table 3) (Hoogkamer et al. 1998; Malerczyk et al. 1998; Buter et al. 1999; Cabaleiro et al. 2013; Jeon et al. 2013; Tjandrawinata et al. 2013; Patel et al. 2017). Demographic data from the population group used for population simulation was randomly formed within the specified demographic data, resulting in different results when modeling. Therefore, to reduce this error, more than 100 repeated experiments on average were performed. The fit of the population model was assessed using a two-fold error method, comparing the results of clinical trials with those derived from the simulation model. When the PK data (such as AUC, Cmax, Tmax, and T1/2) obtained through simulation divided by the actual PK data, the model was judged to be suitable if the value was within the two-fold error boundary (Eq. 4).
Pediatric model development
For PBPK modeling of candesartan in pediatric groups, PK-Sim® random population generation was used within the defined demographic data. Two pediatric groups were used for modeling. The first Caucasian pediatric group consisted of a population of 1000 with a male to female ratio of 50:50, age of 0.1–12 years, and weight of 3–50 kg (Sy et al. 2014). The second Asian pediatric group was divided into two groups of all males and all females. The Asian male pediatric group consisted of a population of 1000, age of 0.1–12 years, weight of 3.41–40.3 kg, and height of 50.12–146.71 cm and the Asian female pediatric group consisted of a population of 1000, age of 0.1–12 years, weight of 3.29–39.24 kg, and height of 49.35–146.71 cm (Kim et al. 2018). In the modeling, a single oral dose of candesartan 12 mg or 16 mg, and CYP2C9*1, CYP2C9*3 and CYP2C9*13 genetic polymorphisms were applied.
Results
In this study, PBPK modeling of candesartan was developed in three phases. First, after developing the model, the generated model evaluated the fit of the model using appropriate equations and clinical data with a 99.998% confidence interval (Abduljalil et al. 2014). Second, after modeling the fitness for the diverse population, the model was evaluated by comparing the literature with PK data in the literature using the two-fold error equation. Finally, we derived the results by application to a model that assessed fitness to pediatric models of various ethnicities and genotypes.
The PBPK modeling of candesartan was developed based on a single oral dose of 16 mg of candesartan cilexetil. Candesartan cilexetil is rapidly and completely metabolized to the potent metabolite candesartan by CES2 enzyme (Laizure et al. 2013; Nishimuta et al. 2014) in the intestinal wall during absorption. In humans, two carboxylesterases, CES1 and CES2, are expressed in the liver, but only high levels of CES2 are expressed in the intestine (Laizure et al. 2013). CES2 is mainly present in the liver, kidney, and intestine, and the metabolic rate of candesartan cilexetil to each organ was used for modeling. Among candesartan metabolism, biliary clearance and renal clearance were applied with reference to the published literature (Gleiter and Mörike 2002). Also, metabolism of candesartan using a recombinant enzyme measured for PBPK modeling of the genetic polymorphism of the CYP2C9 enzyme was calculated through the Michaelis–Menten equation (Table 2). The results of the PBPK modeling of 16 mg single oral dose of candesartan in relation to the CYP2C9 genetic polymorphism are presented in Table 4. In addition, the time-concentration profile of each CYP2C9 genetic polymorphic group is shown in Fig. 1A. As a result, pharmacokinetic parameters such as AUC0–36, AUCinf, Cmax and Tmax were within the acceptance criteria based on clinically observed human PK data in vivo. In these modeling, the AUC0–36 of candesartan in CYP2C9*1/*3 and CYP2C9*1/*13 groups were 1.4-fold and 1.58-fold higher than CYP2C9*1/*1 group, respectively. The AUCinf of candesartan in CYP2C*1/*3 and CYP2C9*1/*13 groups were 1.43-fold and 1.63-fold higher than CYP2C9*1/*1 group, respectively. The Cmax of candesartan in CYP2C*1/*3 and CYP2C9*1/*13 groups were 1.21-fold and 1.33-fold higher than CYP2C9*1/*1 group, respectively. However, there was no significant difference in the Tmax of candesartan in each group. To evaluate the suitability of the developed candesartan PBPK model, pharmacokinetic parameters were observed by applying the model to various population groups. Modeling was conducted considering the demographic data, ethnic group and dose. The suitability of the model was evaluated through a two-fold ratio. As a result of modeling, the results of PK data such as AUC, Cmax, Tmax and T1/2 were within the acceptance criteria, and it was confirmed that this model is suitable for application in various conditions (Table 4).

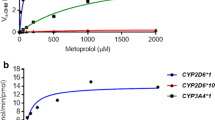
Simulated candesartan plasma concentration after 16 mg single oral dose of candesartan cilexetil by CYP2C9 genotypes in the first phase development of candesartan PBPK modeling (a). Plasma concentration of candesartan by CYP2C9 genotype of Asian male pediatrics (b). Plasma concentration of candesartan by CYP2C9 genotype of Asian female pediatrics (c). Plasma concentration of candesartan by CYP2C9 genotype of Caucasian pediatrics (d)
Modeling in pediatric group
In the Caucasian pediatric model, oral administration of 12 mg candesartan showed that AUCinf and Cmax increased rapidly compared to the adult group. Applying the CYP2C9 genotype, the pharmacokinetic differences between the adult and pediatric groups were more pronounced. In the CYP2C9*1/*1 pediatric group, AUCinf increased by 4.20-fold and Cmax increased by 3.71-fold compared to the Caucasian CYP2C9*1/*1 adult group. In addition, in the pediatric group of the CYP2C9*1/*3 and CYP2C9*1/*13 genotypes, AUCinf increased by 6.08-fold and 6.04-fold, respectively, and Cmax increased by 4.49-fold and 4.48-fold, respectively, compared to the Caucasian adult group (Fig. 1D). In the Asian pediatric group, modeling was conducted by dividing into male and female groups. The Asian pediatric group with 16 mg single oral dose of candesartan had increased AUCinf and Cmax compared to adult group, but the increase rate was not as sharp as the Caucasian pediatric group. In the CYP2C9*1/*1 male pediatric group, AUCinf increased by 2.50-fold and Cmax increased by 2.61-fold compared to the Asian adult patient group. In addition, in the male pediatric group of the CYP2C9*1/*3 and CYP2C9*1/*13 genotypes, AUCinf increased by 3.64-fold and 3.61-fold, respectively, and Cmax increased by 3.19-fold and 3.18-fold, respectively, compared to the Asian adult group (Fig. 1B). In the CYP2C9*1/*1 female pediatric group, AUCinf increased by 2.55-fold and Cmax increased by 2.61-fold compared to the Asian adult patient group. In addition, in the female pediatric group of the CYP2C9*1/*3 and CYP2C9*1/*13 genotypes, AUCinf increased by 3.70-fold and by 3.67-fold, respectively, and Cmax increased by 3.20-fold and by 3.19-fold, respectively, compared to the Asian adult group (Fig. 1C). In Asian pediatric groups, no pharmacokinetic differences due to gender differences were found. Among ethnic groups in the pediatric population, higher pharmacokinetic concentrations (AUCinf and Cmax) were observed in Caucasians than in Asians when applying the same dose (16 mg). When comparing the same CYP2C9 genotypes, AUCinf increased by 1.36-fold and Cmax increased by 1.15-fold (Table 5).
Discussion
Most drug metabolizing enzymes and transporters involved in drug absorption, distribution, metabolism, or excretion are genetically polymorphic, and these genetic polymorphisms affect drug dispositions and drug responses to varying degrees (Bae et al. 2011, 2020; Lee et al. 2015; Kim et al. 2017; Byeon et al. 2018, 2019; Jung et al. 2020a, b; Shin et al. 2020). Drug interactions also have significant effects on drug responses (Lee et al. 2019). PBPK modeling may enable an optimized drug administration strategy for each individual patient by reflecting all of the characteristics such as the patient's physical characteristics, genetic polymorphisms of drug metabolizing enzymes and transporters, drug interactions, diseases, etc. (Duan et al. 2017; Kim et al. 2018, 2021).
To date, there have been many pharmacokinetic studies of candesartan in various populations. However, these studies have not sufficiently considered the genetic polymorphism of the CYP2C9 enzyme. In addition, pharmacokinetic studies of candesartan in pediatric groups have been conducted (Trachtman et al. 2008; Schaefer et al. 2010; Hoy and Keating 2010), but studies on pediatric pharmacokinetics of various ethnic groups taking into account the genetic polymorphism of CYP2C9 enzyme are not sufficient. Even more than the adult patients, the dose regimen of a medication is crucial for pediatric patients. Because children are not little adults, age-dependent values such as tissue size, tissue composition, plasma-protein concentration and hematocrit that can influence the drug absorption, distribution, metabolism and excretion (ADME) must be considered (Kearns et al. 2003; Lukacova et al. 2016). This model was confirmed to be suitable for Asians, Europeans, White Americans, and Mexican American-whites through population simulation. The results of this study in adult groups showed higher AUCinf and Cmax in Asians when comparing the pharmacokinetics of Europeans, Caucasians, Mexicans, and American Caucasians. However, in the pediatric group, AUCinf and Cmax concentrations in Caucasian pediatric group were higher than those in Asian pediatric group (AUCinf: 1.36-fold increased, Cmax: 1.15-fold increased). To identify the rationale for these differences, we compared the demographic data between the Caucasian and Asian pediatric groups, which is thought to have a large impact on the PK of the drug. As a result of the demographic analysis, the weight and height of Caucasians were higher than that of Asians, which did not provide the explanation for the pharmacokinetic differences, making it difficult attribute the pharmacokinetic difference due to demographic data. Therefore, it is thought that there are other age-ethnic-dependent factors that are yet to be identified.
In this study we developed a PBPK modeling of candesartan in relation to CYP2C9 genotypes that are frequently confirmed in Caucasian and Asian population with diverse age groups and ethnic groups. As a result of the modeling, AUC and Cmax were observed to be significantly increased in CYP2C9*1/*3 and CYP2C9*1/*13 groups compared to CYP2C9*1/*1 (wild type) group in adult groups. Through this result, it was confirmed that dose control is necessary in the CYP2C9*1/*3 and CYP2C9*1/*13 groups. In the case of CYP2C9*1/*3 and CYP2C9*1/*13 groups, it is necessary to reduce the dose to about 25% of the original dose to achieve the PK parameters similar to the wild type (CYP2C9*1/*1). When this developed model was applied to the pediatric groups and compared to the adult groups, AUCinf and Cmax were significantly increased in the Caucasian pediatric groups. Right dose, one of the most important factors in precision medicine, was calculated using the PBPK modeling. In order to obtain pharmacokinetic data similar to that of the adult group administered a 12 mg single oral dose of candesartan cilexetil in the Caucasian pediatric group, the CYP2C9*1/*1 genotype requires approximately 75% dose reduction and CYP2C9*1/*3 and CYP2C9*1/*13 genotypes require an approximately 84% dose reduction. In the case of the Asian pediatric group, to obtain pharmacokinetic data similar to that of the adult group administered a 16 mg single oral dose of candesartan cilexetil, the CYP2C9*1/*1 genotype requires approximately 60% dose reduction and CYP2C9*1/*3 and CYP2C9*1/*13 genotypes require an approximately 73% dose reduction. In this study, we developed a PBPK model of candesartan through a three-phase process. In the first phase, a model was developed using the clinical data from healthy Korean male subjects. However, the quantitative mechanism model used to model healthy Korean male subjects is a model that considers Asians in general, and it is difficult to accurately apply it to Koreans particularly. According to the previous studies, liver volume of Koreans was larger than that of other Asians, such as (Japanese and Chinese, and Caucasians (Yu et al. 2004; Johnson et al. 2005; Chan et al. 2006; Yuan et al. 2008; Fu-Gui et al. 2009; Shi et al. 2009; Kim et al. 2019). Also, the mean kidney volume in Koreans is measured to be 205.29 cm3 which was a little smaller than that used in the model (Shin et al. 2009). Such differences can possibly influence the liver plasma clearance, renal plasma clearance, and biliary plasma clearance. The volumes of these organs are very important factors in determining the blood flow rate and plasma clearance during the modeling process and it is likely to influence pharmacokinetics. Also, the hematocrit of Koreans was 45.5% for men and 42% for women (Kim et al. 2019), which is slightly lower than the 47% hematocrit set in the modeling. Hematocrit has a great effect on the volume of fraction (Vf) of neutral lipids, neutral phospholipids, extracellular water and intracellular water, and may affect liver plasma clearance and kidney plasma clearance in modeling. Changes in the Vf change the composition of the tissue, which affects the distribution coefficient, which significantly affects the passive distribution of the drug. This has a great influence on PK in the drug modeling process. Despite these problems, there is a lack of basic research to implement the quantitative mechanistic framework for Koreans, which limits the research. Sensitivity analysis showed that the lipophilicity (logP) of candesartan and candesartan cilexetil had the greatest influence on the PK parameters (AUC and Cmax). Subsequently, it was found that the reference concentration, ontogeny factor, Km and Vmax of CYP2C9 enzyme greatly influenced the PK parameters (Fig. 2). As a result of the sensitivity analysis, it was confirmed that kidney volume, liver volume, and hematocrit can affect the PK parameters, but the effect was not significant. In addition, as a result of the modeling, the relationship between kidney volume, liver volume, or hematocrit and PK parameters could not be confirmed. Because the individual characteristics of patients are so diverse, it is very difficult to deal with many variables in one study. This study covered genetic polymorphism, ethnicity, and age as factors and applied them into the model. However, in the case of patients receiving candesartan cilexetil, drugs to treat other diseases are frequently administered together, and in serious cases, the composition of organs in the body may be changed by surgery. These factors can also affect PK and may need to be considered when deciding on a dosage regimen. In a further study, we would like to suggest the appropriate dose regimen for these patients through PBPK modeling that considers these factors.

Sensitivity analysis results of the PBPK modeling of candesartan (a) AUC and (b) Cmax
References
Abduljalil KCT, Humphries H, Rostami-Hodjegan A (2014) Deciding on success criteria for predictability of pharmacokinetic parameters from in vitro studies: an analysis based on in vivo observations. Drug Metab Dispos 42:1478–1484. https://doi.org/10.1124/dmd.114.058099
AstraZeneca (2005) Atacan® (candesartan cilexetil) prescribing information. [Online] Available from https://www.accessdata.fda.gov/drugsatfda_docs/label/2005/020838s022lbl.pdf. Accessed 1 Oct 2021
Bae JW, Kim HK, Kim JH, Yang SI, Kim MJ, Jang CG, Park YS, Lee SY (2005) Allele and genotype frequencies of CYP2C9 in a Korean population. Br J Clin Pharmacol 60(4):418–422. https://doi.org/10.1111/j.1365-2125.2005.02448.x
Bae JW, Choi CI, Kim MJ, Oh DH, Keum SK, Park JI, Kim BH, Bang HK, Oh SG, Kang BS, Park HJ, Kim HD, Ha JH, Shin HJ, Kim YH, Na HS, Chung MW, Jang CG, Lee SY (2011) Frequency of CYP2C9 alleles in Koreans and their effects on losartan pharmacokinetics. Acta Pharmacol Sin 32(10):1303–1308. https://doi.org/10.1038/aps.2011.100
Bae JW, Oh KY, Yoon SJ, Shin HB, Jung EH, Cho CK, Lim CW, Kang P, Choi CI, Jang CG, Lee SY, Lee YJ (2020) Effects of CYP2D6 genetic polymorphism on the pharmacokinetics of metoclopramide. Arch Pharm Res 43(11):1207–1213. https://doi.org/10.1007/s12272-020-01293-4
Buter H, Navis GY, Woittiez AJ, de Zeeuw D, de Jong PE (1999) Pharmacokinetics and pharmacodynamics of candesartan cilexetil in patients with normal to severely impaired renal function. Eur J Clin Pharmacol 54(12):953–958. https://doi.org/10.1007/s002280050581
Byeon JY, Kim YH, Kim SH, Lee CM, Jung EH, Chae WK, Jang CG, Lee SY, Lee YJ (2018) The influences of CYP2C9*1/*3 genotype on the pharmacokinetics of zolpidem. Arch Pharm Res 41(9):931–936. https://doi.org/10.1007/s12272-018-1070-y
Byeon JY, Lee CM, Lee YJ, Kim YH, Kim SH, Jung EH, Chae WK, Lee YJ, Jang CG, Lee SY (2019) Influence of CYP2D6 genetic polymorphism on pharmacokinetics of active moiety of tolterodine. Arch Pharm Res 42(2):182–190. https://doi.org/10.1007/s12272-018-1099-y
Cabaleiro T, Román M, Ochoa D, Talegón M, Prieto-Pérez R, Wojnicz A, López-Rodríguez R, Novalbos J, Abad-Santos F (2013) Evaluation of the relationship between sex, polymorphisms in CYP2C8 and CYP2C9, and pharmacokinetics of angiotensin receptor blockers. Drug Metab Dispos 41(1):224–229. https://doi.org/10.1124/dmd.112.046292
Chan SC, Liu CL, Lo CM, Lam BK, Lee EW, Wong Y, Fan ST (2006) Estimating liver weight of adults by body weight and gender. World J Gastroenterol 12(14):2217–2222. https://doi.org/10.3748/wjg.v12.i4.2217
Chetty M, Rose RH, Abduljalil K, Patel N, Lu G, Cain T, Jamei M, Rostami-Hodjegan A (2014) Applications of linking PBPK and PD models to predict the impact of genotypic variability, formulation differences, differences in target binding capacity and target site drug concentrations on drug responses and variability. Front Pharmacol 26(5):258. https://doi.org/10.3389/fphar.2014.00258
Fu-Gui L, Lu-Nan Y, Bo L, Yong Z, Tian-Fu W, Ming-Qing X, Wen-Tao W, Zhe-Yu C (2009) Estimation of standard liver volume in Chinese adult living donors. Transplant Proc 41(10):4052–4056. https://doi.org/10.1016/j.transproceed.2009.08.079
García-Martín E, Martínez C, Ladero JM, Agúndez JA (2006) Interethnic and intraethnic variability of CYP2C8 and CYP2C9 polymorphisms in healthy individuals. Mol Diagn Ther 10(1):29–40. https://doi.org/10.1007/BF03256440
Gleiter CH, Mörike KE (2002) Clinical pharmacokinetics of candesartan. Clin Pharmacokinet 41(1):7–17. https://doi.org/10.2165/00003088-200241010-00002
Hanatani T, Fukuda T, Ikeda M, Imaoka S, Hiroi T, Funae Y, Azuma J (2001) CYP2C9*3 influences the metabolism and the drug-interaction of candesartan in vitro. Pharmacogenomics J 1(4):288–292. https://doi.org/10.1038/sj.tpj.6500063
Hoogkamer JF, Kleinbloesem CH, Ouwerkerk M, Högemann A, Nokhodian A, Kirch W, Weidekamm E (1998) Pharmacokinetics and safety of candesartan cilexetil in subjects with normal and impaired liver function. Eur J Clin Pharmacol 54(4):341–345. https://doi.org/10.1007/s002280050471
Hoy SM, Keating GM (2010) Candesartan cilexetil: in children and adolescents aged 1 to <17 years with hypertension. Am J Cardiovasc Drugs 10(5):335–342. https://doi.org/10.2165/11206300-000000000-00000
Jameson JL, Longo DL (2015) Precision medicine–personalized, problematic, and promising. N Engl J Med 372(23):2229–2234. https://doi.org/10.1056/NEJMsb1503104
Jeon JY, Im YJ, Kim Y, Han SM, Jo MJ, Shin DH, Yoo JS, Moon BK, Kim BK, Lee BH, Choi YH, Cho BS, Jang HY, Chae SW, Kim MG (2013) Pharmacokinetic properties and bioequivalence of candesartan cilexetil in Korean healthy volunteers. Drug Dev Ind Pharm. https://doi.org/10.3109/03639045.2012.725732
Johnson TN, Tucker GT, Tanner MS, Rostami-Hodjegan A (2005) Changes in liver volume from birth to adulthood: a meta-analysis. Liver Transplant 11(12):1481–1493. https://doi.org/10.1002/lt.20519
Jung EH, Lee CM, Byeon JY, Shin HB, Oh KY, Cho CK, Lim CW, Jang CG, Lee SY, Lee YJ (2020a) Relationship between plasma exposure of zolpidem and CYP2D6 genotype in healthy Korean subjects. Arch Pharm Res 43(9):976–981. https://doi.org/10.1007/s12272-020-01250-1
Jung EH, Lee YJ, Kim DH, Kang P, Lim CW, Cho CK, Jang CG, Lee SY, Bae JW (2020b) Effects of paroxetine on the pharmacokinetics of atomoxetine and its metabolites in different CYP2D6 genotypes. Arch Pharm Res 43(12):1356–1363. https://doi.org/10.1007/s12272-020-01300-8
Kearns GL, Abdel-Rahman SM, Alander SW, Blowey DL, Leeder JS, Kauffman RE (2003) Developmental pharmacology–drug disposition, action, and therapy in infants and children. N Engl J Med 349(12):1157–1167. https://doi.org/10.1056/NEJMra035092
Kim SW, Jung SS, Lee AR, Son JW (2012) Pharmaceutical formulation for treating cardiovascular disease. Republic of Korea patent KR-10-1205633. 2012 Nov 21
Kim SH, Kim DH, Byeon JY, Kim YH, Kim DH, Lim HJ, Lee CM, Whang SS, Choi CI, Bae JW, Lee YJ, Jang CG, Lee SY (2017) Effects of CYP2C9 genetic polymorphisms on the pharmacokinetics of celecoxib and its carboxylic acid metabolite. Arch Pharm Res 40(3):382–390. https://doi.org/10.1007/s12272-016-0861-2
Kim JH, Yun S, Hwang SS, Shim JO, Chae HW, Lee YJ, Lee JH, Kim SC, Lim D, Yang SW, Oh K, Moon JS, Committee for the Development of Growth Standards for Korean Children and Adolescents, Committee for School Health and Public Health Statistics, the Korean Pediatric Society, Division of Health and Nutrition Survey, Korea Centers for Disease Control and Prevention (2018) The 2017 Korean National Growth Charts for children and adolescents: development, improvement, and prospects. Korean J Pediatr 61(5):135–149. https://doi.org/10.3345/kjp.2018.61.5.135
Kim Y, Hatley O, Rhee SJ, Yi S, Lee HA, Yoon S, Chung JY, Yu KS, Lee H (2019) Development of a Korean-specific virtual population for physiologically based pharmacokinetic modelling and simulation. Biopharm Drug Dispos 40(3–4):135–150. https://doi.org/10.1002/bdd.2178
Kim YH, Kang P, Cho CK, Jung EH, Park HJ, Lee YJ, Bae JW, Jang CG, Lee SY (2021) Physiologically based pharmacokinetic (PBPK) modeling for prediction of celecoxib pharmacokinetics according to CYP2C9 genetic polymorphism. Arch Pharm Res 44(7):713–724. https://doi.org/10.1007/s12272-021-01346-2
König IR, Fuchs O, Hansen G, von Mutius E, Kopp MV (2017) What is precision medicine? Eur Respir J 50(4):1700391. https://doi.org/10.1183/13993003.00391-2017
Kumar V, Brundage RC, Oetting WS, Leppik IE, Tracy TS (2008) Differential genotype dependent inhibition of CYP2C9 in humans. Drug Metab Dispos 36(7):1242–1248. https://doi.org/10.1124/dmd.108.020396
Lee YJ, Byeon JY, Kim YH, Kim SH, Choi CI, Bae JW, Sohn UD, Jang CG, Lee J, Lee SY (2015) Effects of CYP2C9*1/*3 genotype on the pharmacokinetics of flurbiprofen in Korean subjects. Arch Pharm Res 38(6):1232–1237. https://doi.org/10.1007/s12272-015-0580-0
Lee CM, Jung EH, Byeon JY, Kim SH, Jang CG, Lee YJ, Lee SY (2019) Effects of steady-state clarithromycin on the pharmacokinetics of zolpidem in healthy subjects. Arch Pharm Res 42(12):1101–1106. https://doi.org/10.1007/s12272-019-01201-5
Lesko LJ, Schmidt S (2012) Individualization of drug therapy: history, present state, and opportunities for the future. Clin Pharmacol Ther 92(4):458–466. https://doi.org/10.1038/clpt.2012.113
Lukacova V, Goelzer P, Reddy M, Greig G, Reigner B, Parrott N (2016) A physiologically based pharmacokinetic model for ganciclovir and its prodrug valganciclovir in adults and children. AAPS J 18(6):1453–1463. https://doi.org/10.1208/s12248-016-9956-4
Malerczyk C, Fuchs B, Belz GG, Roll S, Butzer R, Breithaupt-Grögler K, Herrmann V, Magin SG, Högemann A, Voith B, Mutschler E (1998) Angiotensin II antagonism and plasma radioreceptor-kinetics of candesartan in man. Br J Clin Pharmacol 45(6):567–573. https://doi.org/10.1046/j.1365-2125.1998.00722.x
Mizutani T (2003) PM frequencies of major CYPs in Asians and Caucasians. Drug Metab Rev 35(2–3):99–106. https://doi.org/10.1081/dmr-120023681
Nakai K, Habano W, Nakai K, Fukushima N, Suwabe A, Moriya S, Osano K, Gurwitz D (2005) Ethnic differences in CYP2C9*2 (Arg144Cys) and CYP2C9*3 (Ile359Leu) genotypes in Japanese and Israeli populations. Life Sci 78(1):107–111. https://doi.org/10.1016/j.lfs.2005.04.049
Nishimuta H, Houston JB, Galetin A (2014) Hepatic, intestinal, renal, and plasma hydrolysis of prodrugs in human, cynomolgus monkey, dog, and rat: implications for in vitro-in vivo extrapolation of clearance of prodrugs. Drug Metab Dispos 42(9):1522–1531. https://doi.org/10.1124/dmd.114.057372
Noetzli M, Eap CB (2013) Pharmacodynamic, pharmacokinetic and pharmacogenetic aspects of drugs used in the treatment of Alzheimer’s disease. Clin Pharmacokinet 52(4):225–241. https://doi.org/10.1007/s40262-013-0038-9
Patel R, Palmer JL, Joshi S, Di Ció GA, Esquivel F (2017) Pharmacokinetic and bioequivalence studies of a newly developed branded generic of candesartan cilexetil tablets in healthy volunteers. Clin Pharmacol Drug Dev 6(5):492–498. https://doi.org/10.1002/cpdd.321
Rodgers T, Rowland M (2006) Physiologically based pharmacokinetic modelling 2: predicting the tissue distribution of acids, very weak bases, neutrals and zwitterions. J Pharm Sci 95(6):1238–1257. https://doi.org/10.1002/jps.20502
Rodgers T, Leahy D, Rowland M (2005) Physiologically based pharmacokinetic modeling 1: predicting the tissue distribution of moderate-to-strong bases. J Pharm Sci 94(6):1259–1276. https://doi.org/10.1002/jps.20322
Schaefer F, van de Walle J, Zurowska A, Gimpel C, van Hoeck K, Drozdz D, Montini G, Bagdasorova IV, Sorof J, Sugg J, Teng R, Hainer JW, Candesartan in Children with Hypertension Investigators (2010) Efficacy, safety and pharmacokinetics of candesartan cilexetil in hypertensive children from 1 to less than 6 years of age. J Hypertens 28(5):1083–1090. https://doi.org/10.1097/HJH.0b013e328336b86b
Shi ZR, Yan LN, Li B, Wen TF (2009) Evaluation of standard liver volume formulae for Chinese adults. World J Gastroenterol 15(32):4062–4066. https://doi.org/10.3748/wjg.15.4062
Shimada T, Yamazaki H, Mimura M, Inui Y, Guengerich FP (1994) Interindividual variations in human liver cytochrome P-450 enzymes involved in the oxidation of drugs, carcinogens and toxic chemicals: studies with liver microsomes of 30 Japanese and 30 Caucasians. J Pharmacol Exp Ther 270(1):414–423
Shin HS, Chung BH, Lee SE, Kim WJ, Ha HI, Yang CW (2009) Measurement of kidney volume with multi-detector computed tomography scanning in young Korean. Yonsei Med J 50(2):262–265. https://doi.org/10.3349/ymj.2009.50.2.262
Shin HB, Jung EH, Kang P, Lim CW, Oh KY, Cho CK, Lee YJ, Choi CI, Jang CG, Lee SY, Bae JW (2020) ABCB1 c.2677G>T/c.3435C>T diplotype increases the early-phase oral absorption of losartan. Arch Pharm Res 43(11):1187–1196. https://doi.org/10.1007/s12272-020-01294-3
Sy SK, Asin-Prieto E, Derendorf H, Samara E (2014) Predicting pediatric age-matched weight and body mass index. AAPS J 16(6):1372–1379. https://doi.org/10.1208/s12248-014-9657-9
Thelen K, Coboeken K, Willmann S, Burghaus R, Dressman JB, Lippert J (2011) Evolution of a detailed physiological model to simulate the gastrointestinal transit and absorption process in humans, part 1: oral solutions. J Pharm Sci 100(12):5324–5345. https://doi.org/10.1002/jps.22726
Tjandrawinata RR, Setiawati E, Yunaidi DA, Simanjuntak R, Santoso ID, Susanto LW (2013) Bioequivalence study of two formulations of candesartan cilexetil tablet in healthy subjects under fasting conditions. Drug Des Dev Ther 7:841–847. https://doi.org/10.2147/DDDT.S47272
Trachtman H, Hainer JW, Sugg J, Teng R, Sorof JM, Radcliffe J, Candesartan in Children with Hypertension (CINCH) Investigators (2008) Efficacy, safety, and pharmacokinetics of candesartan cilexetil in hypertensive children aged 6 to 17 years. J Clin Hypertens (Greenwich) 10(10):743–750. https://doi.org/10.1111/j.1751-7176.2008.00022.x
Yu HC, You H, Lee H, Jin ZW, Moon JI, Cho BH (2004) Estimation of standard liver volume for liver transplantation in the Korean population. Liver Transplant 10(6):779–783. https://doi.org/10.1002/lt.20188
Yuan D, Lu T, Wei YG, Li B, Yan LN, Zeng Y, Wen TF, Zhao JC (2008) Estimation of standard liver volume for liver transplantation in the Chinese population. Transplant Proc 40(10):3536–3540. https://doi.org/10.1016/j.transproceed.2008.07.135
Zhou SF, Zhou ZW, Yang LP, Cai JP (2009) Substrates, inducers, inhibitors and structure-activity relationships of human Cytochrome P450 2C9 and implications in drug development. Curr Med Chem 16(27):3480–3675. https://doi.org/10.2174/092986709789057635
Duan P, Zhao P, Zhang L (2017) Physiologically Based Pharmacokinetic (PBPK) modeling of pitavastatin and atorvastatin to predict Drug-Drug Interactions (DDIs). Eur J Drug Metab Pharmacokinet 42(4):689–705. https://doi. org/10. 1007/s13318-016-0383-9
Laizure SC, Herring V, Hu Z, Witbrodt K, Parker RB (2013) The role of human carboxylesterases in drug metabolism: have we overlooked their importance? Pharmacotherapy 33(2):210-22. doi: 10.1002/phar.1194.
Acknowledgements
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT, and Future Planning (NRF-2019R1A2C1004582).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Jung, E.H., Cho, CK., Kang, P. et al. Physiologically based pharmacokinetic modeling of candesartan related to CYP2C9 genetic polymorphism in adult and pediatric patients. Arch. Pharm. Res. 44, 1109–1119 (2021). https://doi.org/10.1007/s12272-021-01363-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12272-021-01363-1