
Abstract
We aimed to evaluate the feasibility and reliability of brush cytology in the biomarker expression profiling of oral squamous cell carcinomas within the concept of theranostics, and to correlate this biomarker profile with patient measurable outcomes. Markers representative of prognostic gene expression changes in oral squamous cell carcinoma was selected. These markers were also selected to involve pathways for which commercially available or investigational agents exist for clinical application. A set of 7 markers were analysed by immunocytochemistry on the archival primary tumour material of 99 oral squamous cell carcinoma patients. We confirmed the feasibility of the technique for the expression profiling of oral squamous cell carcinomas. Furthermore, our results affirm the prognostic significance of the epidermal growth factor receptor (EGFR) family and the angiogenic pathway in oral squamous cell carcinoma, confirming their interest for targeted therapy. Brush cytology appears feasible and applicable for the expression profiling of oral squamous cell carcinoma within the concept of theranostics, according to sample availability.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
OSCC Epidemiology
Head and neck squamous cell carcinoma (HNSCC) is the 6th commonest cancer, with an estimated worldwide incidence of 0.65 million new cases and 350,000 deaths annually [1]. Within HNSCC, oral squamous cell carcinoma (OSCC) accounts for 90 % of oral cancer, and represents an anatomical region of moderate prognosis in the cartography of the head and neck tumors. The overall 5-year cancer-specific survival is 62 %, ranging from 82 % for the localised disease to 57 % for the node-positive tumors and 35 % for the metastatic disease [2].
Theranostics and Targeted Therapy
The concept of blocking key pathways of tumour survival and growth is supported by abundant evidence, has found celebrated applications in targeted therapy of solid tumours, and is currently undergoing daring expansion in all fields of oncology. The concept of theranostics is an emerging treatment strategy that combines the modalities of therapy and diagnostic imaging [3]. In this context, it aims to develop material or apply existing technologies with the capacity of monitoring the treated tissue and efficacy in the long-term period. It can also be used for identifying patients most likely to benefit from tailored cancer targeted therapy, therefore personalising treatment from the early diagnostic stages. In order to achieve this, the selection and validation of appropriate biomarkers is essential.
Prognostic Biomarkers in OSCC
The network-based meta-analysis of the HNSCC transcriptome data has identified enriched signaling pathways and hotspots of transcriptional profiles implicated in the regulation of early, advanced and metastatic HNSCC. Amongst these vascular endothelial growth factor (VEGF) and EGFR signaling, integrin signaling, p53 signaling, antigen presentation genes and epithelial-matrix interaction pathways are significantly overexpressed hubs [4]. Unsurprisingly, these pathways have also been identified as prognostic biomarkers, with a relationship between survival parameters of OSCC patients and their expression levels, mainly using immunohistochemistry [5].
Angiogenesis Biomarkers
The VEGF family and their receptors play a pivotal role in OSCC, and is most frequently used by a tumor to switch on its angiogenic phenotype. VEGF represents an independent negative prognostic factor for OSCC [6–9]. Anti-VEGF therapies are successfully integrated in the management of major solid tumors such as colorectal, lung and ovarian cancer, and are currently investigated in HNSCC, in combination with chemotherapy or other targeted therapy [10–13].
CD34 is a highly sensitive marker for endothelial cell differentiation and has also been studied as a marker for angiogenesis in vascular tumors. When overexpressed around tumor microvessels in cancer cell nests and marginal areas of cancer infiltration it is associated with early lymph node metastasis and poor survival in OSCCs [14, 15]. This pattern of stromal CD34 expression seems to be dynamic and specific: the border of invasive squamous cell carcinomas is characterized by a loss of CD34-positive fibroblasts paralleled by a gain of α-SMA-positive myofibroblasts [16]. Furthermore, the existence of CD34-positive penetrating vessels within tumor nests was significantly associated with risk of cervical node metastasis [17, 18].
Platelet-derived Endothelial Cell Growth Factor (PDGF) is overexpressed [15, 19] and is an independent prognostic factor for poor survival in OSCCs [15]. Furthermore, as PDGF is identical to thymidine phosphorylase, an essential enzyme for the activation of prodrugs of 5-fluorouracil (5FU), it is predictive of response to 5FU-based chemotherapy [15].
Cell Growth and Proliferation Biomarkers
The EGFR family members including EGFR, ErbB2 (Neu, HER2), ErbB3, and ErbB4 play a critical role in cancer development. Aberrant expression of EGFR and its dimerisation partner HER2 are indicators of poor prognosis in OSCC [20, 21]. Frequent co-expression of ErbB receptors may enhance oncogenicity due to receptor heterodimerization and predict worse disease outcome in patients with OSCC [21]. EGFR, overexpressed in 80–90 % of HNSCC, is an early event associated with more aggressive disease, regional lymph node metastasis, resistance to chemotherapy and poorer survival [22, 23]. The frequency of HER2 overexpression varies between 6 % and over 80 % depending on tumor type and has been associated with shorter disease-free (DFS) and overall survival (OS) in OSCC in some studies [20, 21, 24–26], although not all studies [27, 28]. EGFR and Her2 have been shown to be more frequently overexpressed in oral cavity tumors compared to other HNSCC localizations [24–29]. Agents targeting EGFR are now approved for HNSCC treatment. Intriguingly, the activation status of HER2 but not EGFR predicts resistance to the EGFR inhibitor gefitinib in HNSCC [30], suggesting that interactions between family members are important.
c-KIT (CD117) is a transmembrane tyrosine kinase receptor, structurally related to PDGFR. Its natural ligand is stem cell factor (SCF). The SCF/c-KIT signaling pathway is closely related to the regulation of tumor cell proliferation, differentiation, adhesion, and apoptosis. c-kit was found to be overexpressed in 86 % of oral/oropharyngeal tumors, however not correlated with DFS [31]. Like CD34, c-kit seems to have a selective pattern of expression in tumor-associated myofibroblasts in OSCCs [16]. In another study, reactivity to c-kit was confined to stromal cells, many of which were arranged as a barrier near the front of invasion in OSCC tumors. Most of these CD117+ cells were of mesenchymal origin, enhancing the formation of tumor stroma [32].
Cyclooxygenase (COX) is the rate-limiting enzyme in the formation of prostaglandins. COX-2 is overexpressed in OSCC, and is a predictor of poor survival [33] and poor DFS [34], although not in all studies [35, 36]. Prostaglandins can enhance tumor growth and metastasis by stimulating angiogenesis [34] and invasiveness, in addition to inhibiting apoptosis and immune surveillance. Short-term administration of a COX-2 inhibitor restored anti-tumoral immunity and increased infiltration into the tumor of monocytes and Th1 and CD25+ activated lymphocytes [37]. Thus, in vivo inhibition of the COX-2 pathway may potentiate cancer immunotherapy. Selective inhibitors of COX-2, such as celecoxib, have chemopreventive action in advanced oral premalignant lesions [38]. Combined COX-2 and EGFR inhibition in the neoadjuvant setting decreased tumoral proliferation in HNSCC patients [39]. Studies in combination with EGFR inhibitors in the adjuvant (NCT01515137) or metastatic setting (NCT00392665), as well as for radiosensitisation (NCT00581971) are currently ongoing.
Cytology-Based Theranostics in OSCC
The immunohistochemical (IHC) expression of the above-mentioned markers has been investigated to a variable degree in OSCC. However, the feasibility and reliability of their immunocytochemistry detection (ICC) has not to date been investigated for the majority of the above markers.
The purpose of our study was to investigate the expression profile of selected markers in cytological brushes of OSCCs using ICC and to verify their prognostic significance. This does not only involve use of archived tissue to establish the medical utility of a marker, but also assesses the applicability and prognostic validity of a non-invasive, easily repetitive technique.
Materials and Methods
Patient Cohort
Patients with histology-proven OSCC for whom both clinocopathological data and archived cytological material were available were selected. All patients were treated at the Department of Oral & Maxillofacial Surgery of the “Theagenio” Cancer Hospital of Thessaloniki, Greece in the period 2003–2011. The study was approved by the Institutional Review Board of “Theagenio” Cancer Hospital.
Data Collection
Data were extracted from the patient notes and collected in a dedicated electronic database, and were subsequently coded for statistical analysis. Data were collected on patient demographics, disease characteristics (localization, staging, histology, treatment modalities), disease outcome (relapse-free survival [RFS], OS and last known status) and biomarker ICC scoring.
Marker Selection
A set of 7 markers (EGFR, c-erb-B2, COX-2, PDGF, VEGF, CD117/c-KIT, CD34) was selected from the spectrum of prognostic gene expression changes in OSCC. They were selected to represent pathways for which commercially available or investigational agents exist for clinical application in other types of tumors, including epithelial tumors. EGFR was selected to serve as an internal control for the sensitivity/specificity of the cytology-based diagnosis, since it extensively studied in HNSCC [Ang 2002, Kong 2006]. Finally, we aimed to have a molecular tumor profile readily available for future personalized medicine treatment planning.
Marker analysis was subject to specimen availability, so not all markers could be investigated in each patient. Analysis was performed on primary tumor specimens exclusively.
Specimen Collection
All brush biopsy specimens were collected by two trained cytopathologists of the Department of Cytopathology, “Theagenio” Cancer Hospital of Thessaloniki, Greece. Specimens were collected, processed, and archived using departmental standard operational procedures.
Immunocytochemical Techinique
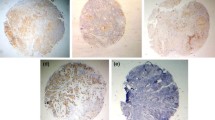
Profiling was performed using conventional cytology and Liquid Based Cytology (ThinPrep®, Cytyc Co, USA), subject to specimen availability. There was no specific intentional order for marker analysis, and patient samples were analyzed according to specimen availability. Assay-specific procedures were determined individually for each marker. Monoclonal antibodies against VEGF (clone EP1176Y, 1:50, Biocare Medical), PDGF (clone P-GF.44C, 1:50, Novocastra), c-Kit (CD117) (Clone T595, 1:25, Novocastra), and CD34 (clone QBEnd/10, 1:50, Biocare Medical) were used. Cytoplasmic and cell membrane staining for VEGF-A and CD34, nuclear and cytoplasmic for PDGF and membranous staining for c-Kit (CD117) was evaluated. A single examiner (RMV) evaluated the results to ensure consistency and eliminate inter-examiner variability bias. The staining positivity was scored as strong (3+ when >50 % of cells were stained), intermediate (2+ when 15–50 % of cells were stained, weak (1+ when 10–15 % of cells were stained) and 0 (when less than 10 % of the cells were stained).
Statistical Analysis
The correlation of immunopositivity to several factors like smoking history, histological grade, pathological and clinical staging, treatment modality, local control of the disease, RFS and OS was investigated.
The Wilcoxon rank sum and χ2 tests were used to compare variables between groups. OS was defined as the time from surgery to death from any cause. RFS was defined as the time from surgery to disease relapse (local, regional or distant). Censoring was at the date of last contact for surviving or non-relapsing patients respectively. The Kaplan-Meier method and Cox proportional hazards models were used to assess the association between predictor variables and time-to-event outcomes. All P values are two-sided. P < 0.05 was considered statistically significant. Analyses were conducted the SPSS software version 10.
Data mining was done with the use of the CHAID (Chi-squared Automatic Interaction Detection) tree-growing algorithm. Significance level for splitting and merging was set at 5 %, adjusted using the Bonferroni method. The feature selection node was also used for data mining, using the following set of criteria: maximum percentage of missing values: 70 %; maximum percentage of records in a single category: 90 %; maximum number of categories as a percentage of records: 95 %; minimum coefficient of variation: 0.1; minimum standard deviation: 0.0. Artificial neural network forecasting was done with use of the Multilayer Perceptions (MLP) method.
Results
Patient Cohort
The cohort included 99 patients (67 males [67.7 %], 32 females [32.3 %]) with OSCC. All tumors were localized in the oral cavity and lip. Baseline characteristics are presented in Table 1. Details on treatment modalities and outcome measurements are given in Table 2.
Marker Analysis
The immunocytochemical expression analysis of the different markers is outlined in Table 3.
Survival Analysis-RFS and OS
Four clinicopathological factors were identified in the univariate analysis as significant for OS: M stage (p = 0.016), surgery (p = 0.000), local control at the end of definite treatment (p = 0.000) and relapse (p = 0.007) (Table 4). Four markers were significant in the univariate analysis: EGFR (p = 0.003) (3+ expression associated with shorter OS and increased risk of death), PDGF (p = 0.002) (lack of expression associated with longer OS and decreased risk of death), VEGF (p = 0.035) (lack of expression associated with longer OS and decreased risk of death), and CD34 (p = 0.010) (3+ expression associated with shorter OS and increased risk of death) (Table 5, Fig. 1).

Overall survival according to the status of informative markers in univariate analysis. A: EGFR; B: PDGF; C: VEGF; D: CD34
In regard with RFS, two markers were significant in the univariate analysis: EGRF (p = 0.046) (3+ expression associated with shorter RFS and increased relapse risk), and PDGF (p = 0.005) (lack of expression associated with longer RFS and decreased relapse risk) (Table 5, Fig. 2). Six clinicopathological factors were also significant for RFS: localization (p = 0.016; lip primaries had longer RFS), N stage (p = 0.004), M stage (p = 0.032), surgery (p = 0.002), radiotherapy (p = 0.001), and local control at the end of definite treatment (p = 0.000) (Table 4).

Relapse-free survival according to the status of informative markers in univariate analysis. A: EGFR; B: PDGF
No factor was identified as significant in the multivariate analysis for either RFS or OS.
MLP prediction did not identify any clinicopathological factor as significant for OS (the biomarkers were not included in the analysis). Analysis of the relative importance of the factors indicated the smoking history as the most important factors for OS prediction (importance: 0.1425, non-significant) and the relapse as the least significant (importance: 0.0251).
Survival Analysis-Last Known Status
Data mining using the classification model CHAID indicated that the last known status depended on relapse. For patients with no relapse, last known status depended on c-erbB2; e.g. all 4 patients with c-erbB2 0 or 1+ did not relapse and died of another cause.
For patients who relapsed, last known status depended on T stage; e.g. 15 patients with T stage >1 relapsed and died of their disease. For patients with T stage 1 who relapsed, last known status depends on local control at the end of definitive treatment. For patients with T stage > 1 who relapsed, last known status depends on VEGF (if VEGF was overexpressed they were more likely to relapse and die of their disease). Finally, for patients with VEGF = 0, T stage > 1, and relapse, last known status depends on whether surgery was used as treatment modality.
The above data was confirmed using feature selection node. The most important inputs relative to the last known status, in highest to lowest ranking, were the following: relapse (0.999999), local control with definite treatment (0.999997), c-erb-B2 (0.999643), localization (0.997135), T stage (0.983131) and surgery (0.9967229).
Discussion
Despite diagnostic and therapeutic improvements, OSCC prognosis especially for the advanced stages remains poor [2]. Therefore, the importance of markers prognostic of tumor aggressiveness and predictive of response to treatment is paramount [5, 18].
Brush cytology is a valuable and reliable diagnostic tool, used for early diagnosis and clinical follow-up of oral cancer. Cytological preparations are readily, painlessly and directly obtained without need of an endoscope, without significant damage of the tissues, so it can be repeatable in clinical follow-up [40].
Liquid-based cytology offers an automated or semi-automated processing and distribution of cells in a thin, evenly dispersed layer, to enhance specificity (95 %-100 %) and sensitivity (80 %) [41]. It increases sample quality and diagnostic accuracy, mainly because of better cytomorphologic picture and cleaner background. It is easier and less time-consuming to screen and interpret the slides, as the cells are limited to a smaller area. Its great advantage is that it allows creation of archival material and application of new techniques on the same sample [42]. The ability to stain for cellular proteins and more recently genes and gene products in cells, or obtain tumoral DNA or RNA [43] represents a major advancement.
Our results indicate that, in addition to the known significance of the EGFR overexpression, the angiogenetic pathway is of prognostic significance in OSCC. An angiogenic switch involving increased expression of PDGF, VEGF and CD34 in the tumor and its microenvironment seems to characterize a more aggressive phenotype with less favorable survival outcomes in our cohort, in concordance with previous reports [6, 44]. However, more insight on the potentially dynamic temporo-spatial role of these markers ought to be further investigated. Insight from other cancers reveals sometimes opposing roles; for example, CD34 was found to play a biphasic role in tumor progression in melanoma, maintaining early-stage vascular integrity but accelerating late-stage growth via altering immune cell infiltration [45].
It ought to be noted that the relatively small patient number and the limited quantity of available material compromised our analysis. As a result of the latter not all markers could be analyzed for every patient, and this may entail non-intentional bias. The reason for this was that the study did not involve a prospective collection of specimens, but rather consisted of archival material primarily intended for initial diagnostic purposes. Conversely, a prospective database construction would have been compromised by the lack of long survival/follow-up data, and therefore a “prospective-retrospective” design using archival material was used [46]. To our knowledge this is the only cytological biomarker expression and outcome analysis of this extent in OSCC. Nevertheless, the retrospective nature of our study entails weaknesses such as important number of missing data in terms of clinical characteristics, such as smoking history, alcohol consumption and metabolic disorders (insulin resistance).
Further to the established role of cetuximab, there could possibly be a place for therapeutic targeting for tumors overexpressing these markers (15 %-30 % of tumours in our cohort), utilizing drugs such as bevacizumab (anti-VEGF monoclonal antibody), cediranib (oral selective inhibitor of VEGFR-1, −2 and −3) [47], afatinib (oral inhibitor of the broader erb-B family) [48] or even combined pathway targeting, e.g. cetuximab & bevacizumab [10, 11], erlotinib & bevacizumab [12], bevacizumab & pemetrexed [13]. It ought to be noted, however, that data on the use of anti-angiogenic agents in HNSCC is still immature, and that an enhanced risk of bleeding is reported in trials with VEGF inhibitors [13]. Moreover, there have been disappointing results on targeted therapies either as monotherapy or as combination therapies [49, 50].
Cytology can be used for repeated tumor profiling throughout the disease course, to evaluate the influence of treatment (chemotherapy, radiotherapy) on the tumoral molecular profile, and direct treatment according to the marker expression profile at diagnosis, between treatment lines, upon progression and/or relapse. However, further validation and standardization is required for the ICC scoring of these markers, especially in the aim of optimizing their use towards targeted therapy. The most celebrated example of targeted treatment in head and neck is EGFR targeting. If we borrow the knowledge obtained from EGFR targeting in lung cancer, an optimized IHC EGFR scoring may serve as a predictive factor for the efficacy of cetuximab and help select patients more appropriately for cetuximab treatment [51, 52].
Examples of theranostics application are the combination of molecular-targeted cancer imaging and therapy to improve cancer diagnosis and minimize the side effects of conventional treatments, such as ErbB2 targeting for bioluminescence imaging and therapy [53], or nanotheranostics applications [54]. To our knowledge, there is no published theranostics application in OSCC. Our results aim to serve as an introduction towards such a proof-of-concept, utilizing a well-established and broadly used existing technology, such as brush cytology.
This project was introduced as a forward step for oral cancer management in our Unit, within the wider concept of applied tumor targeted therapy in HNSCC. The identification of driver genetic alterations, the elucidation of cross-talk between oncogenic pathways and the detection of susceptibility to synthetic lethality facilitate the move towards biomarker-directed therapy and precision medicine. Our research is ongoing with the analysis of further markers (integrins, cadherins, NFκB etc) and a larger future analysis is planned.
References
Jemal A, Bray F, Center MM, Ferlay J, Ward E (2011) Global cancer statistics, 2008. CA Cancer J Clin 61:69–90
Siegel R, Naishadham N, Jemal A (2012) Cancer statistics, 2012. CA Cancer J Clin 62:10–29
Funkhouser J (2002) Reinventing pharma: the theranostic revolution. Current Drugs Discov 2:17–19
Yu YH, Kuo HK, Chang KW (2008) The evolving transcriptome of head and neck squamous cell carcinoma: a systematic review. PLoS One 3:e3215
Oliveira LR, Ribeiro-Silva A (2011) Prognostic significance of immunohistochemical biomarkers in oral squamous cell carcinoma. Int J Oral Maxillofac Surg 40:298–307
Smith BD, Smith GL, Carter D, Sasaki CT, Haffty BG (2000) Prognostic significance of vascular endothelial growth factor protein levels in oral and oropharyngeal squamous cell carcinoma. J Clin Oncol 18:2046–2052
Uehara M, Sano K, Ikeda H, Sekine J, Irie A, Yokota T, Tobita T, Ohba S, Inokuchi T (2004) Expression of vascular endothelial growth factor and prognosis of oral squamous cell carcinoma. Oral Oncol 40:321–325
Kyzas PA, Cunha IW, Ioannidis JP (2005) Prognostic significance of vascular endothelial growth factor immunohistochemical expression in head and neck squamous cell carcinoma: a meta-analysis. Clin Cancer Res 11:1434–1440
Shao Z, Zhang WF, Chen XM, Shang ZJ (2008) Expression of EphA2 and VEGF in squamous cell carcinoma of the tongue: correlation with the angiogenesis and clinical outcome. Oral Oncol 44:1110–1117
Argiris A, Kotsakis AP, Hoang T, Worden FP, Savvides P, Gibson MK, Gyanchandani R, Blumenschein Jr GR, Chen HX, Grandis JR, Harari PM, Kies MS, Kim S (2013) Cetuximab and bevacizumab: preclinical data and phase II trial in recurrent or metastatic squamous cell carcinoma of the head and neck. Ann Oncol 24:220–225
Redman MW, Crowley JJ, Herbst RS, Hirsch FR, Gandara DR (2012) Design of a phase III clinical trial with prospective biomarker validation: SWOG S0819. Clin Cancer Res 18:4004–4012
Cohen EE, Davis DW, Karrison TG, Seiwert TY, Wong SJ, Nattam S, Kozloff MF, Clark JI, Yan DH, Liu W, Pierce C, Dancey JE, Stenson K, Blair E, Dekker A, Vokes EE (2009) Erlotinib and bevacizumab in patients with recurrent or metastatic squamous-cell carcinoma of the head and neck: a phase I/II study. Lancet Oncol 10:204–205
Argiris A, Karamouzis MV, Gooding WE, Branstetter BF, Zhong S, Raez LE, Savvides P, Romkes M (2011) Phase II trial of pemetrexed and bevacizumab in patients with recurrent or metastatic head and neck cancer. J Clin Oncol 29:1140–1145
Nagatsuka H, Hibi K, Gunduz M, Tsujigiwa H, Tamamura R, Sugahara T, Sasaki A, Nagai N (2005) Various immunostaining patterns of CD31, CD34 and endoglin and their relationship with lymph node metastasis in oral squamous cell carcinomas. J Oral Pathol Med 34:70–76
Fujieda S, Sunaga H, Tsuzuki H, Sugimoto C, Tanaka N, Saito H (1998) Expression of platelet-derived endothelial cell growth factor in oral and oropharyngeal carcinoma. Clin Cancer Res 4:1583–1590
Barth PJ, Schweinsberg TS, Ramaswamy A, Moll R (2004) CD34+ fibrocytes, α-smooth muscle antigen-positive myofibroblasts, and CD117 expression in the stroma of invasive squamous cell carcinomas of the oral cavity, pharynx, and larynx. Virchows Arch 444:231–234
Kademani D, Lewis JT, Lamb DH, Rallis DJ, Harrington JR (2009) Angiogenesis and CD34 expression as a predictor of recurrence in oral squamous cell carcinoma. J Oral Maxillofac Surg 67:1800–1805
Ascani G, Balercia P, Messi M, Lupi L, Goteri G, Filosa A, Stramazzotti D, Pieramici T, Rubini C (2005) Angiogenesis in oral squamous cell carcinoma. Acta Otorhinolaryngol Ital 25:13–17
Alcalde RE, Terakado N, Otsuki K, Matsumura T (1997) Angiogenesis and expression of platelet-derived endothelial cell growth factor in oral squamous cell carcinoma. Oncology 54:324–328
Xia W, Lau YK, Zhang HZ, Liu AR, Li L, Kiyokawa N, Clayman GL, Katz RL, Hung MC (1997) Strong correlation between c-erb-2 overexpression and overall patients with oral squamous cell carcinoma. Clin Cancer Res 3:3–9
Xia W, Lau YK, Zhang HZ, Xiao FY, Johnston DA, Liu AR, Li L, Katz RL, Hung MC (1999) Combination of EGFR, HER- 2/neu and HER-3 is a stronger predictor for the outcome of oral squamous cell carcinoma than any individual family members. Clin Cancer Res 5:4164–4174
Ang KK, Berkey BA, Tu X, Zhang HZ, Katz R, Hammond EH, Fu KK, Milas L (2002) Impact of epidermal growth factor receptor expression on survival and pattern of relapse in patients with advanced head and neck carcinoma. Cancer Res 62:7350–7356
Kong A, Leboucher P, Leek R, Calleja V, Winter S, Harris A, Parker PJ, Larijani B (2006) Prognostic value of an activation state marker for epidermal growth factor receptor in tissue microarrays of head and neck cancer. Cancer Res 66:2834–2843
Albuquerque Jr RL, Miguel MC, Costa AL, Souza LB (2003) Correlation of c-erbB-2 and S-100 expression with the malignancy grading and anatomical site in oral squamous cell carcinoma. Int J Exp Pathol 84:259–265
Ulanovski D, Stern Y, Roizman P, Shpitzer T, Popovtzer A, Feinmesser R (2004) Expression of EGFR and cerb-B2 as prognostic factors in cancer of the tongue. Oral Oncol 40:532–537
Ekberg T, Nestor M, Engstrom M, Nordgren H, Wester K, Carlsson J, Anniko M (2005) Expression of EGFR, HER2, HER3, and HER4 in metastatic squamous cell carcinomas of the oral cavity and base of tongue. Int J Oncol 26:1177–1185
Kuropkat C, Venkatesan TK, Caldarelli DD, Panje WR, Hutchinson J, Preisler HD, Coon JS, Werner JA (2002) Abnormalities of molecular regulators of proliferation and apoptosis in carcinoma of the oral cavity and oropharynx. Auris Nasus Larynx 29:165–174
Angiero F, Sordo RD, Dessy E, Rossi E, Berenzi A, Stefani M, Sidoni A (2008) Comparative analysis of c-erbB-2 (HER-2/neu) in squamous cell carcinoma of the tongue: does over-expression exist? And what is its correlation with traditional diagnostic parameters? J Oral Pathol Med 37:145–150
Freier K, Bosch FX, Flechtenmacher C, Devens F, Benner A, Lichter P, Joos S, Hofele C (2003) Distinct site-specific oncoprotein overexpression in head and neck squamous cell carcinoma: a tissue microarray analysis. Anticancer Res 23:3971–3977
Erjala K, Sundvall M, Junttila TT, Zhang N, Savisalo M, Mali P, Kulmala J, Pulkkinen J, Grenman R, Elenius K (2006) Signaling via ErbB2 and ErbB3 associates with resistance and epidermal growth factor receptor (EGFR) amplification with sensitivity to EGFR inhibitor gefitinib in head and neck squamous cell carcinoma cells. Clin Cancer Res 12:4103–4111
Ongkeko WM, Altuna X, Weisman RA, Wang-Rodriguez J (2005) Expression of protein tyrosine kinases in head and neck squamous cell carcinomas. Am J Clin Pathol 124:71–76
Mărgăritescu C, Pirici D, Simionescu C, Stepan A (2011) The utility of CD44, CD117 and CD133 in identification of cancer stem cells (CSC) in oral squamous cell carcinomas (OSCC). Romanian J Morphol Embryol 52(3 Suppl):985–993
Chang BW, Kim DH, Kowalski DP, Burleson JA, Son YH, Wilson LD, Haffty BG (2004) Prognostic significance of cyclooxygenase-2 in oropharyngeal squamous cell carcinoma. Clin Cancer Res 10:1678–1684
Pannone G, Sanguedolce F, De Maria S, Farina E, Lo Muzio L, Serpico R, Emanuelli M, Rubini C, De Rosa G, Staibano S, Macchia L, Bufo P (2007) Cyclooxygenase isozymes in oral squamous cell carcinoma: a real-time RT-PCR study with clinic pathological correlations. Int J Immunopathol Pharmacol 20:317–324
Atula T, Hedström J, Ristimäki A, Finne P, Leivo I, Markkanen-Leppänen M, Haglund C (2006) Cyclooxygenase-2 expression in squamous cell carcinoma of the oral cavity and pharynx: association to p53 and clinical outcome. Oncol Rep 16:485–490
Ryott M, Marklund L, Wangsa D, Elmberger G, Munck-Wikland E (2011) Cyclooxygenase-2 expression in oral tongue squamous cell carcinoma. J Oral Pathol Med 40:385–389
Lang S, Tiwari S, Andratschke M, Loehr I, Lauffer L, Bergmann C, Mack B, Lebeau A, Moosmann A, Whiteside TL, Zeidler R (2007) Immune restoration in head and neck cancer patients after in vivo COX-2 inhibition. Cancer Immunol Immunother 56:1645–1652
Saba NF, Hurwitz SJ, Kono SA, Yang CS, Zhao Y, Chen Z, Sica G, Muller S, Moreno-Williams R, et al. (2014) Chemoprevention of head and neck cancer with celecoxib and erlotinib: results of a phase Ib and pharmacokinetic study. Cancer Prev Res 7:283–291
Gross NB, Bauman JE, Godding WE, Denq W, Thomas SM, Wang L, Chiosea S, Hood BL, Flint MS, Sun M, et al. (2014) Erlotinib-erlotinib-sulindac vs placebo: a randomised, double-blind, placebo-controlled window trial in operable head and neck cancer. Clin Cancer Res 20:3289–3298
De May RM (1996) The Art and Science of Cytopathology. ASCP Press 1st edition, USA, pp 329–330.
Navone R, Pentenero M, Gandolfo S (2011) Liquid-based cytology in oral cavity squamous cell cancer. Curr Opin Otolaryngol Head Neck Surg 19:77–81
Malle D, Valeri RM, Photiou C, Kaplanis K, Andreadis C, Tsavdaridis D, Destouni C (2005) Significance of immunocytochemical expression of E-cadherin, N-cadherin and CD44 in serous effusions using liquid-based cytology. Acta Cytol 49:11–16
Schwartz JL, Panda S, Beam C, Bach LE, Adami GR (2008) RNA from brush oral cytology to measure squamous cell carcinoma gene expression. J Oral Pathol Med 37:70–77
Lothaire P, de Azambuja E, Dequanter D, Lalami Y, Sotiriou C, Andry G, Castro Jr G, Awada A (2006) Molecular markers of head and neck squamous cell carcinoma Promising signs in need of prospective evaluation. Head Neck 28:256–269
Simon RM, Paik S, Hayes DF (2009) Use of archived specimens in evaluation of prognostic and predictive biomarkers. J Natl Cancer Inst 101:1446–1452
Maltby S, Freeman S, Gold MJ, Baker JHE, Minchinton AI, Gold MR, Roskelley CD, McNagny KM (2011) Opposing roles for CD34 in B16 melanoma tumor growth alter early stage vasculature and late stage immune cell infiltration. PLoS One 6(4):e18160
Saura C, Baselga J, Herbst R, del Campo J, Marotti M, Tessier J, Collins B, Heymach J (2009) Antitumor activity of cediranib in patients with metastatic or recurrent head and neck cancer (HNC) or recurrent non-small cell lung cancer (NSCLC). an open-label exploratory study. J Clin Oncol 27(15S):6023
Machiels J, Haddad RI, Fayette J, Licitra L, Tahara M, Vermorken JB, Clement PM, Gauler T, Cupissol D, Grau JJ, Guigay J, Caponigro F, De Castro Jr G, De Souza VL, Keilholz U, Del Campo J, Cong X, Ehmrooth E, Cohen EE (2015) Afatinib versus methotrexate as second-line treatment for patients with recurrent or metastatic squamous-cell carcinoma of the head and neck progressing on or after platinum-based therapy (LUX-Head & Neck 1): an open-label, randomised phase 3 trial. Lancet Oncol 16:583–594
de Souza JA, Davis DW, Zhang Y, Khattri A, Seiwert TY, Aktolga S, Wong SJ, Kozloff MF, Nattam S, Lingen MW, Kunnavakkam R, Stenson KM, Blair EA, Bozeman J, Dancey JE, Vokes EE, Cohen EE (2012) A phase II study of lapatinib in recurrent/metastatic squamous cell carcinoma of the head and neck. Clin Cancer Res 18:2336–2243
Vermorken JB, Peyrade F, Krauss J, Mesía R, Remenar E, Gauler TC, Keilholz U, Delord JP, Schafhausen P, Erfán J, Brümmendorf TH, Iglesias L, Bethe U, Hicking C, Clement PM (2014) Cisplatin, 5-fluorouracil, and cetuximab (PFE) with or without cilengitide in recurrent/metastatic squamous cell carcinoma of the head and neck: results of the randomized phase I/II ADVANTAGE trial (phase II part). Ann Oncol 25:682–688
Fruh M, Pless M (2012) EGFR IHC score for selection of cetuximab treatment: ready for clinical practice? Transl Lung Cancer Res 1:145–146
Lynch T, Bhagavatheeswaran P, Mukhopadyay P (2011) A retrospective subgroup analysis of EGFR immunohistochemistry expression by histo-score correlated to outcomes from the BMS099 1st line phase III NSCLC trial of cetuximab plus carboplatin/taxane. Eur J Cancer 47:S591–S592
Han XJ, Sun LF, Nishiyama Y, Feng B, Michiue H, Seno M, Matsui H, Tomizawa K (2013) Theranostic protein targeting ErbB2 for bioluminescence imaging and therapy for cancer. PLoS One 8:e75288
Muthu MS, Tai Leong D, Mei L, Feng SS (2014) Nanotheranostics ˗ application and further development of nanomedicine strategies for advanced theranostics. Theranostics 4:660–677
Acknowledgments
The authors thank Dr. Petros Zikos for his help in data collection.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors have no conflicts of interest to declare.
Funding Information
No specific funding was available for this project.
Rights and permissions
About this article

Cite this article
Patrikidou, A., Valeri, R.M., Kitikidou, K. et al. Introducing Cytology-Based Theranostics in Oral Squamous Cell Carcinoma: A Pilot Program. Pathol. Oncol. Res. 22, 401–411 (2016). https://doi.org/10.1007/s12253-015-0017-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12253-015-0017-6