
Abstracts
Anaplastic thyroid cancer (ATC) is a rare but aggressive malignancy of the thyroid. No effective treatment modalities are currently available. Targeted therapy against protein kinases showed promising results in preclinical studies. Our goal was to assess the mutational status of potential therapeutic targets, as well as the biomarker for immunotherapy in the clinical context. Using allele specific PCR, Sanger sequencing, fragment analysis and immunohistochemistry, we assessed BRAF, KRAS, EGFR mutations and protein overexpression of C-KIT and PDL1 in anaplastic thyroid cancer specimens. Results were compared to clinical information and patient outcome to assess the utility of these biomarkers. There were 13 patients in our study with a median overall survival of 19 weeks. Of the 13 ATC patients, 3 (23 %) had BRAF V600E mutation. C-KIT overexpression was found in 1 (8 %) patient who responded well to a tyrosine kinase inhibitor. PDL1 expression was seen in 3 (23 %) patients, none of them were surgical candidates due to unresectability and poor performance status. KRAS codon 12/13 and EGFR exon 18, 19, 20 and 21 were all wild type in our patients. Protein kinase inhibitors and immunotherapy may be useful adjuvant therapies for ATC.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Anaplastic thyroid carcinoma (ATC) is a rare thyroid malignancy, accounting for less than 2 % of all cases of thyroid carcinoma [1]. It is a highly aggressive neoplasm that is often widely invasive or metastatic at presentation. All patients are classified as stage IV regardless of the tumor size or the presence of metastasis because of the high risk of mortality [2]. The 6-month cause-specific survival rate has been reported between 36 and 68.4 % by different studies [3, 4]. So far, there are no effective treatment modalities available. Some studies showed a multimodal approach with surgery, radiation and chemotherapy is beneficial, while other studies showed no survival benefit [3, 5–9]. The extremely poor prognosis signifies the urgency in developing novel therapeutic strategies.
Inhibition of BRAF V600E and EGFR with small molecular inhibitors showed antitumor activity towards ATC in cell lines and xenograft models [10–12], suggesting the presence of BRAF V600E and EGFR mutations in ATC. Biologically, it has been postulated that ATC may develop from anaplastic transformation of preexisting well differentiated thyroid cancer, as evidenced from the existence of well differentiated areas in cases of ATC. The majority of well differentiated thyroid carcinomas are associated with a mutation in only one of the three genes involved in the MAPK pathway: Ras, BRAF mutations or RET/PTC rearrangement [13]. This may imply the presence of theses mutation in ATC. In fact, BRAF mutations have been observed in 10–35 % ATC [13]. These findings resulted in a surge in clinical trials to evaluate the efficacy of targeted therapy in ATC (reviewed in [14, 15]).
Programmed death-1 (PD-1) is an inhibitory receptor expressed on the surface of activated T cells. The binding of PD-1 to its ligand PDL1 and PDL2 inhibits T cell function. PDL1 and PDL2 are predominantly expressed within the tumor microenvironment, where they mediated the inhibition of T cells through a process known as adaptive resistance [16]. Recently, two clinical trials of monoclonal antibodies that target PD1and PDL1 showed promising results as new anticancer immunotherapy [17, 18]. In a cohort of patients that were largely comprised of melanoma and non-small cell lung cancers, those with tumors that had tested positive for PDL1 expression showed response rates of 36 % in the anti-PD1 study [18]. The expression of PDL1 in ATC has not been evaluated. However, a phase I trial with an inflammatory modulator, Bardoxolone methyl, showed partial response in 1 out 4 ATC patients, suggesting a role of immunotherapy in the management of ATC [19].
In this current study, we report the patient outcome in our single institution experience, and examine the correlation between the clinical behavior and the mutational status of EGFR, KRAS, as well as protein expression status of C-KIT and PDL-1.
Material and Methods
Patients and Tissue Samples
A retrospective clinical-pathological study in patients diagnosed with anaplastic thyroid carcinoma at Boston Medical Center from 2003 to 2012 was conducted. Clinical information was extracted from the electronic medical record. The histological diagnosis was reevaluated by 2 pathologists at the time of this study, aided by immunohistochemical studies for AE1/3, PAX8 and TTF-1.
Paraffin-embedded sections from cancers obtained by fine-needle aspiration or resection were collected for immunohistochemical studies or mutational analysis.
The following characteristics were collected: age, gender, race, pathological diagnosis, radiation therapy and type of chemotherapy. The cancers were categorized as spindle cell/ sarcomatoid (mainly spindle cells with rare giant cells), giant cell type (more than half of the cancer cells were tumor giant cells), squamoid (more than half of the cancer cells were squamous cell carcinoma) and mixed giant cell and spindle cell/sarcomatoid. The overall survival (OS) was defined as the time of initial diagnosis to the time of death. All samples were de-identified.
Mutational Analysis
The assays for BRAFV600E mutation, KRAS codon 12/13 mutation and EGFR exon 18–21 mutations were performed at Diagnostic Molecular Pathology lab in the anatomic pathology department of Boston Medical Center using standard diagnostic procedures. All sample assays were either duplicated or triplicated and repeated as needed.
DNA extraction:
Tissue was cut from corresponding tissue block and subjected to de-paraffin process to harvest as a dry tissue pellet. The tissue pellet was then digested with Tris-proteinase K buffer (250 ug/ml proteinase K). DNA was quantified with spectrophotometer. Working solution was diluted from stock to concentrations of 25–50 ng/microliter.
BRAFV600E mutation assay [20–22]
Allele-specific PCR was used for forward and reverse strand BRAF codon 600 mutation assay. The primer set and sequences are listed as follow:
For BRAF forward allele:
Forward-5′ ACAGTAAAAATAGGTGATTTTGGTCTAGCTACAGA 3′
Reverse-5′CTATGAAAATACTATAGTTGAGACCTTCAATGACTTTC 3′
For BRAF reverse allele:
Forward-5′ CTAAACTCTTCATAATGCTTGCTC 3′
Reverse-5′ GGACCCACTCCATCGAGATTTCT 3′
For DNA quality control GAPDH:
Forward- 5′ GAAATGTGCTTTGGGGAGGCA 3′
Reverse-5′ TTTGCAGGGCTGAGTCAGCTTC 3′
The forward and reverse allele PCR were run on a ABI PCR thermocycler and TaqGold DNA polymerase with 25 μl in total reaction, 50–100 ng template DNA per reaction for the following cycle profile: 5 min @ 95 °C to activate DNA polymerase followed by 20 s @ 94 °C, 30 s @ 62 °C, 25 s @ 72 °C for 45 cycles and one extension @ 72 °C for 5 min. The PCR products was then run on an 3 % agarose gel, analysis and documented on a Polaroid film. Mutation positive, negative and no DNA controls are included in each run for both forward and reverse allele PCR.
KRAS codon12/13 mutation assay by Sanger sequencing [20, 23, 24]:
The following primers was used to generated a 290 bp KRAS fragment spanning codon 12 and 13 region, forward primer-5′ GTACTGGTGGAGTATTTGAT 3′, reverse primer- 5′ACTCATGAAAATGGTCAG-3′. Once the PCR showed a band on agarose electrophoresis, the forward primer was used for sequencing reaction. ABI standard BigDye sequencing kit (ver3.0) was used for sequencing.
After sequencing reaction is completed, the products were purified by ethanol precipitation and centrifugation and dissolved in formamide and run on an ABI 3130XL genetic analyzer. Electrophorograms were printed, scanned and documented for codon 12/13 mutation.
EGFR exon 18–21 mutation assay by fragment analysis (exon 19 and 21) and Sanger sequencing (exon 18 and 20) [25–27].
Standard Sanger sequencing for exon 18 and 20 was performed same as the KRAS sequencing but the following primers and only forward strand was sequencing analyzed:
Exon 18 PCR primers: forward [26]:
PCR primers: EGFR18ext-F: 5′-CAAGTGCCGTGTCCTGGCACCCAAGC-3′, EGFR18ext-R: 5′-CCAAACACTCAGTGAAACAAAGAG-3′
sequencing primer:EGFR18Seq-F: 5′-GCCATGTCTGGCACTGCTTT-3′.
For exon 20 direct sequencing [27]
PCR primers: EGFR20F1: 5′-ctccaggaagcctacgtgat-3′,
EGFR20R: 5′GTCTTTGTGTTCCCGGACAT-3′.
For exon 19 deletion/insertion assay by fragment analysis:
Standard PCR was performed by using the following set of primers: EGFR-19F1: 5′-GCACCATCTCACAATTGCCAGTTA-3′ and EGFR-19R1: 5′-FAM-AAAAGGTGGGCCTGAGGTTCA-3′ with reverse primer 6-FAM labeled. The primers generate a 207 bp wild-type product which included entire length of exon 19. The PCR products was agarose electrophoresed and properly loaded on ABI Genetic Analyzer 3130XL and capillary electrophoresed. The electrophoresed product was analyzed by GeneMapper v3.5 to detect shortened fragment (deletion) or lengthened fragment (insertion). Positive and negative controls were included in each batch of the assay.
Exon 21 L858R mutation assay by RE digestion and fragment analysis: the following primer set were used to perform PCR on exon 21 spanning codon 858 region (product size 222 base pair) . The reverse primer was 6-FAM labeled.
EGFR-21F1: 5′-CCTCACAGCAGGGTCTTCTCTGT-3′,
EGFR-21R1: 5′-FAM-TCAGGAAAATGCTGGCTGACCTA-3′.
Patients DNA were first PCR amplified and agarose electrophoresed and documented on film. The PCR products then were digested with restriction enzyme Sau96I (GGNCC, NE Bio lab) to generate PCR-RFLP pattern. Proper amount of digested PCR product were then mixed with formamide and denatured electrophoresed on ABI Genetic Analyzer and analyzed with GeneMapper v3.5 to identify L858R mutation: wild-type shows a 175 bp fragment while mutated fragment will be 87 bp in size on capillary electrophoresis. Positive and negative controls were included in each batch of the assay.
Immunohistochemistry
Selected cases of paraffin-embedded sections were subjected to immunohistochemical staining for AE1/3, CAM5.2, p53, MIB1 (Ki67), PAX8, TTF-1, p63, thyroglobin, S100, Mart-1 (all antibodies from Ventana) on Benchmark XT platform (Ventana) according to the manufacturer’s manual. The results were evaluated by a pathologist at the time of initial diagnosis. All cases were immunostained for CD117 (Ventana) and PDL-1 (mouse anti-human B7-H1 mAb, clone 5H1, kindly provided by Dr. Lieping Chen’s lab at Yale University) at the time of this study, and reviewed by two pathologists independently, and the evaluations were identical. A cancer was considered immunopositive for CD117 when there was membranous staining pattern.
Statistical Analysis
The analysis was descriptive in nature. Mean, median and frequency counts were reported for demographic, clinical variables. The Kaplan-Meier method was used to estimate overall survival.
Results
Patient Characteristics
Between January 1st, 2003 and December 31st, 2012, 13 patients were diagnosed with ATC at Boston Medical Center. Patient characteristics are listed in Table 1. There were seven females and six males, and the median age was 63 years (ranges 42–75). Nine patients were Caucasian, three African Americans and one was Latino. All but one patient (92 %) had metastasis at presentation, including 8 patients (62 %) presented with distant metastases, most commonly to the lungs. One patient had thyroidectomy 24 years before the presentation of ATC, so the size of the thyroid could not be evaluated. For the rest of the patients, the maximal dimension of thyroid ranged from 3.4 to 9.7 cm by ultrasound examination. Pathologically, there were 5 cases with well-differentiated component, including 4 cases of papillary thyroid cancer and 1 case of follicular carcinoma.
Treatment and Patient Outcomes
Five patients had debulking thyroidectomy for ATC, one patient (Patient #13) had thyroidectomy for papillary thyroid cancer 24 years ago, and the remaining 7 patients did not receive surgery due to unresectability and poor performance status (Table 1). In single variant analysis, those received surgical resection survived better than those without (median overall survival 32.8 weeks in patients with resection versus 9.1 weeks in patients without resection). Four out of 5 (80 %) patients who had surgery had well-differentiated components, while only 1 out 7 (14 %) patients who did not have surgery had well-differentiated components (Patient #5). Except for 2 patients who passed away soon after the diagnosis (Patient #1 and #13), all the remaining patients received external radiation therapy to the neck of different dosages (from 19 to 66 Gy). Chemotherapy regimen information was not available for Patient #11 and #12. For the remaining 11 patients, 3 did not receive any chemotherapy, 4 received cytotoxic chemotherapy (Taxol, Platin, and Adriamycin), and the remaining 4 received targeted therapy (Sunitinib, Cetuximab, Erlotinib, Vemurafenib, and Pazopanib) with or without cytotoxic chemotherapy.
The overall survival was available for 12 patients, it ranged from 2.3 weeks to more than 400 weeks, and the median overall survival was 15.9 weeks.
Of Patients #1 to #7 who did not have surgery, receiving targeted therapy appears to increase survival compared to those without targeted therapy. Patients #1 and #2 did not receive any chemotherapy, and the overall survival was 2.4 and 12.9 weeks, respectively. Patients #3 and #4 had cytotoxic chemotherapy, and the overall survival was 8.3 and 5.1 weeks. For the remaining 3 patients who received targeted therapy, the overall survival ranged from 9.1 to 21.3 weeks.
Of patients who had resection for the primary cancer, 2 patients are still alive at the time of this study (#9 and #10). Patient #8 survived 22.6 weeks without any chemotherapy. Patient #9 had squamous cell carcinoma with coexistent papillary thyroid cancer, and upper endoscopy and laryngeal biopsies had ruled out the possibility of a metastatic cancer. This patient had been treated with cisplatin, and has been cancer free for almost 10 years. Patient #10 had a similar histopathology as #9, with squamous cell carcinoma intimately mixed with a papillary thyroid cancer. She was treated with Pazopanib and has survived more than 43 weeks from the initial diagnosis with persistent disease.
Expression Profiles of Cancer Biomarker
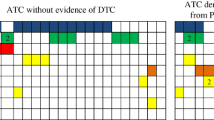
BRAF V600E mutation was present in 3 patients (#1, 5 and 13), 2 of which had conventional papillary thyroid cancer. KRAS codon 12/13 mutation were absent in all the patients, including Patient #12, who had follicular carcinoma as the well-differentiated component. EGFR exons 18, 19, 20 and 21 were all wild type in all the cases (Table 2).
C-KIT protein overexpression was observed in Patient #10 (Fig. 1), who responded well to Pazopanib. In addition, Patient #8 had C-KIT overexpression in the well differentiated follicular carcinoma component.

Patchy membranous stain for C-KIT in this case of squamous anaplastic thyroid carcinoma with focal mucinous cells
PDL1 expression was seen 3 patients (#1, 2 and 4) (Fig. 2), all of them presented with huge tumor mass, and none of them was surgical candidate.

Diffuse cytoplasmic staining for PDL1 in this case of sarcomatoid anaplastic thyroid carcinoma
Discussion
ATC is an aggressive malignancy with grave prognosis under current management strategies. Targeted therapy against protein tyrosine kinases showed promising results in preclinical studies. Our goal was to assess the mutational status of potential therapeutic targets, as well as the expression of biomarker for immunotherapy in the clinical context. Of the 13 patients included in our study, 3 (23 %) had BRAF V600E mutation. KRAS codon 12/13 and EGFR exon 18, 19, 20 and 21 were all wild type. C-KIT overexpression was found in 1 (8 %) patient who responded well to a tyrosine kinase inhibitor pazopanib, and PDL1 expression was seen in 3 (23 %) patients.
Overall, 4 patients received protein kinase inhibitors either as monotherapy or in conjunction with cytotoxic chemotherapy. Three of these patients were not surgical candidates (Patients #5, 6 and 7). Patient #5 received Vemurafenib targeting the BRAF V600E mutation identified in his cancer, in conjunction of Adriamycin. He survived relatively longer than other non-surgical candidates at 19 weeks as compared to a median of 9.1 weeks. Even though anti-BRAF (V600E) mutation appears promising in preclinical studies [10], 2 clinical trials failed in confirming this finding in 6 treated patients receiving Sorafenib, a multitargeted tyrosine kinase inhibitor that weakly inhibits the BRAF and more potently inhibits VEGFR [28, 29]. The most recent clinical trial on Sorafenib showed a modest 10 % partial response in ATC patients. The outcome of our patients suggests that targeting BRAF may be of benefit if the mutation is present.
Patient #6 did not have any mutations in the mutational hotspots of EGFR, but she was given EGFR targeted therapy (both cetuximab and erlotinib), and she had the longest survival among all the non-surgical candidates at 21.3 weeks. Preclinical studies showed prolonged survival in ATC with EGFR inhibitors [11]. However, a phase II clinical trial included 5 ATC patients showed no response to gefitinib, an EGFR inhibitor [30], even though one patient had stable disease for 12 months. The number of cases is very small to draw a meaningful conclusion. So far, there were only 3 publications examining the mutational status of EGFR in ATC [31–33]. All of these studies showed an absence of EGFR mutation in part of the hot spots examined. Consistent with these findings, we did not observe any hot-spot (all 4 exons) EGFR mutations in our patients. These results together suggest that small molecule EGFR inhibitors targeting specific hot-spot mutations may not be very effective in treating ATC. On the other hand, a monoclonal EGFR inhibitor may be of help in case of EGFR amplification or polysomy. One of these articles [32] also studied EGFR amplification and polysomy and found correlation between EGFR polysomy and overexpression detectable by IHC; however, they did not find any EGFR amplification. There was no information regarding to patients’ management and outcome to understand the significance of these polysomy.
Patient #7 received multi-kinase inhibitor Sunitinib as a monotherapy and she succumbed to the disease 9.1 weeks after the initial diagnosis. Sunitinib has not been extensively studied in ATC at the clinical level, however, there is a recent case report about a complete response in a patient with gross residual disease, who remained disease free more than 18 months after diagnosis after administering Sunitinib [34].
Patient #10 received Pazopanib as a monotherapy, and she is still alive at the time of this study (more than 43 weeks from the initial diagnosis), and the only targetable abnormality was c-KIT overexpression. Pazopanib is a multi-targeted tyrosine kinase inhibitor of VEGFR, PDGFR and c-KIT. A phase II clinical trial of Pazopanib showed a 49 % partial response rate in 39 patients with progressive metastatic well-differentiated thyroid cancer [35]. However, a multi-institutional phase II trial of Pazopanib monotherapy showed minimal single-agent clinical activity in a cohort of 15 advanced ATC patients [36].
Our patient did have a relatively small cancer (4.5 cm), and had resection of the primary lesion, both of which can contribute to the prolonged overall survival. However, the fact that this patient received Pazopanib as a single agent still suggests a benefit of Pazopanib in ATC patients with tyrosine kinase overexpression. In addition, in a trial of tyrosine kinase inhibitor imatinib, which primary targets include c-KIT and BCR-ABL, showed partial response in 2 out of 8 ATC patients [37]. Based on our observation, as well as the published data from both preclinical and clinical trials, it is perceivable that a clinical trial for protein kinase inhibitors in ATC may be better carried out based on the underlying molecular targets, similar to the success achieved in non-small cell lung cancer [38]. Admittedly, this approach may be difficult considering the rarity of ATC. Lastly, since Pazopanib is a multi-kinase inhibitor, a future study to examine the expression profile of its known targets like VEGFR and PDGFR in this patient is warranted. Moreover, the underlying causes for c-KIT overexpression in this case still need further studies.
Lastly, with the success of anti-PDL1 antibody in treating a variety of advanced cancers [17]; we tested the expression of PDL1 in ATC. PDL1 expression was seen in 3 (23 %) patients, and none of them had well-differentiated components. These patients were not surgical candidates due to large tumor size (>7 cm), unresectability and poor performance status. Detecting the expression of PDL1 in this group of patients indicates that immunotherapy may provide powerful alternatives or as adjuvant to current therapies in ATC patients, especially those who present with large unresectable tumor and poor performance status.
In conclusion, we analyzed the profiles of molecular targets in 13 cases of ATC with clinical follow-up. Our results suggest that kinase inhibitors and immunotherapy may be useful adjuvant therapeutics for ATC.
References
Carling T, Udelsma R (2008) Thyroid tumors. In: DeVita VT, Lawrence TS, Rosenberg SA (eds) Devita, Hellman & Rosenberg’s cancer [electronic resource]: principles and practice of oncology. Wolters Kluwer/Lippincott Williams & Wilkins, Philadelphia, pp 1663–1682
Edge SB, Byrd DR, Compton CC et al. (eds) (2010) AJCC cancer staging handbook. 7th ed. New York, NY: Springer New York
Sugitani I, Miyauchi A, Sugino K et al (2012) Prognostic factors and treatment outcomes for anaplastic thyroid carcinoma: ATC research consortium of Japan cohort Study of 677 patients. World J Surg 36:1247–1254
Kebebew E, Greenspan FS, Clark OH et al (2005) Anaplastic thyroid carcinoma. Treatment outcome and prognostic factors. Cancer 103:1330–1335
Busnardo B, Daniele O, Pelizzo MR et al (2000) A multimodality therapeutic approach in anaplastic thyroid carcinoma: study on 39 patients. J Endocrinol Investig 23:755–761
Pierie J-PEN, Muzikansky A, Gaz RD et al (2002) The effect of surgery and radiotherapy on outcome of anaplastic thyroid carcinoma. Ann Surg Oncol 9:57–64
Haigh PI, Ituarte PH, Wu HS et al (2001) Completely resected anaplastic thyroid carcinoma combined with adjuvant chemotherapy and irradiation is associated with prolonged survival. Cancer 91:2335–2342
Smallridge RC (2012) Approach to the patient with anaplastic thyroid carcinoma. J Clin Endocrinol Metab 97:2566–2572
Akaishi J, Sugino K, Kitagawa W et al (2011) Prognostic factors and treatment outcomes of 100 cases of anaplastic thyroid carcinoma. Thyroid : Off J Am Thyroid Assoc 21:1183–1189
Nehs MA, Nagarkatti S, Nucera C et al (2010) Thyroidectomy with neoadjuvant PLX4720 extends survival and decreases tumor burden in an orthotopic mouse model of anaplastic thyroid cancer. Surgery 148:1154–1162, discussion 1162
Gule MK, Chen Y, Sano D et al (2011) Targeted therapy of VEGFR2 and EGFR significantly inhibits growth of anaplastic thyroid cancer in an orthotopic murine model. Clin Cancer Res 17:2281–2291
Nobuhara Y, Onoda N, Yamashita Y et al (2005) Efficacy of epidermal growth factor receptor-targeted molecular therapy in anaplastic thyroid cancer cell lines. Br J Cancer 92:1110–1116
Kondo T, Ezzat S, Asa SL (2006) Pathogenetic mechanisms in thyroid follicular-cell neoplasia. Nat Rev Cancer 6:292–306
Sipos JA, Shah MH (2010) Thyroid cancer: emerging role for targeted therapies. Ther Adv Med Oncol 2:3–16
Antonelli A, Fallahi P, Ferrari SM et al (2012) RET TKI: potential role in thyroid cancers. Curr Oncol Rep 14:97–104
Keir ME, Butte MJ, Freeman GJ et al (2008) PD-1 and its ligands in tolerance and immunity. Annu Rev Immunol 26:677–704
Brahmer JR, Tykodi SS, Chow LQM et al (2012) Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N Engl J Med 366:2455–2465
Topalian SL, Hodi FS, Brahmer JR et al (2012) Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med 366:1–12
Hong DS, Kurzrock R, Supko JG et al (2012) A phase I first-in-human trial of bardoxolone methyl in patients with advanced solid tumors and lymphomas. Clin Cancer Res 18:3396–3406
Yang S, Farraye FA, Mack C et al (2004) BRAF and KRAS Mutations in hyperplastic polyps and serrated adenomas of the colorectum: relationship to histology and CpG island methylation status. Am J Surg Pathol 28:1452–1459
Davies H, Bignell GR, Cox C et al (2002) Mutations of the BRAF gene in human cancer. Nature 417:949–954
Pollock PM, Harper UL, Hansen KS et al (2003) High frequency of BRAF mutations in nevi. Nat Genet 33:19–20
Amado RG, Wolf M, Peeters M et al. (2008) Wild-type KRAS is required for panitumumab efficacy in patients with metastatic colorectal cancer
Khambata-Ford S, Garrett CR, Meropol NJ et al (2007) Expression of epiregulin and amphiregulin and K-ras mutation status predict disease control in metastatic colorectal cancer patients treated with cetuximab. J Clin Oncol 25:3230–3237
Pan Q, Pao W, Ladanyi M (2005) Rapid polymerase chain reaction-based detection of epidermal growth factor receptor gene mutations in lung adenocarcinomas. J Mol Diagn JMD 7:396–403
Pinter F, Papay J, Almasi A et al (2008) Epidermal growth factor receptor (EGFR) high gene copy number and activating mutations in lung adenocarcinomas are not consistently accompanied by positivity for EGFR protein by standard immunohistochemistry. J Mol Diagn JMD 10:160–168
Oh Y-H, Kim Y, Kim Y-P et al (2010) Rapid detection of the epidermal growth factor receptor mutation in non-small-cell lung cancer for analysis of acquired resistance using molecular beacons. J Mol Diagn JMD 12:644–652
Gupta-Abramson V, Troxel AB, Nellore A et al (2008) Phase II trial of sorafenib in advanced thyroid cancer. J Clin Oncol 26:4714–4719
Kloos RT, Ringel MD, Knopp MV et al (2009) Phase II trial of Sorafenib in metastatic thyroid cancer. J Clin Oncol 27:1675–1684
Pennell NA, Daniels GH, Haddad RI et al. (2008) A phase II study of gefitinib in patients with advanced thyroid cancer
Elliott DD, Sherman SI, Busaidy NL et al (2008) Growth factor receptors expression in anaplastic thyroid carcinoma: potential markers for therapeutic stratification. Hum Pathol 39:15–20
Lee DH, Lee GK, Kong S et al (2007) Epidermal growth factor receptor status in anaplastic thyroid carcinoma. J Clin Pathol 60:881–884
Fisher KE, Jani JC, Fisher SB et al (2013) Epidermal growth factor receptor overexpression is a marker for adverse pathologic features in papillary thyroid carcinoma. J Surg Res. doi:10.1016/j.jss.2013.05.003
Schoenfeld JD, Odejide OO, Wirth LJ et al (2012) Survival of a patient with anaplastic thyroid cancer following intensity-modulated radiotherapy and sunitinib — a case report. Anticancer Res 32:1743–1746
Bible KC, Suman VJ, Molina JR et al. (2010) Efficacy of pazopanib in progressive, radioiodine-refractory, metastatic differentiated thyroid cancers: results of a phase 2 consortium study
Bible KC, Suman VJ, Menefee ME et al (2012) A multiinstitutional phase 2 trial of pazopanib monotherapy in advanced anaplastic thyroid cancer. J Clin Endocrinol Metab 97:3179–3184
Ha HT, Lee JS, Urba S et al (2010) A phase II study of imatinib in patients with advanced anaplastic thyroid cancer. Thyroid Off J Am Thyroid Assoc 20:975–980
Kimura H, Nakajima T, Takeuchi K et al (2012) ALK fusion gene positive lung cancer and 3 cases treated with an inhibitor for ALK kinase activity. Lung Cancer 75:66–72
Acknowledgments
We thank Ms. Teresa Lima, Alyssa Brown and Cathy Tilton for their technical assistance. Dr. Lieping Chen’s lab at Yale University provided mouse anti-human B7-H1 mAb, clone 5H1. This work was supported by Mallory Research Grant to HW and YS from the Mallory Institute of Pathology, Boston University.
Disclosure
The authors have nothing to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Wu, H., Sun, Y., Ye, H. et al. Anaplastic Thyroid Cancer: Outcome and the Mutation/Expression Profiles of Potential Targets. Pathol. Oncol. Res. 21, 695–701 (2015). https://doi.org/10.1007/s12253-014-9876-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12253-014-9876-5