
Abstract
Diagnosis of breast cancer (BC) by using sensitive and specific biomarkers is necessary. Cell-free DNA is a candidate biomarker in various cancers. Contrasting, shorted uniformed DNA released from apoptotic non-diseased cells, DNA released from malignant cells varies in size. DNA integrity is a ratio between 247 and 115 bp. So, this study was designed to investigate the role of plasma ALU-247, ALU-115, and DNA integrity as possible diagnostic and prognostic markers in BC patients as compared to plasma CA15.3. The concentrations of selected parameters were determined for 40 patients with BC (2 stage I, 31 stage II, 2 stage III, and 5 stage IV) and 10 healthy volunteers by quantitative real-time PCR and ELISA. The sensitivities of ALU-247, ALU-115, and cfDI as biomarkers for BC were evaluated and compared with CA15.3. Also, disease-free survival and overall survival were estimated. For all parameters, the concentrations in patients were significantly higher than in the control group; association with tumor stage and high sensitivities was observed. The studied parameters failed to predict survival or relapse in BC patients before surgery. Plasma ALU-247, ALU-115, and DNA integrity may prove to have clinical utility in BC diagnosis. Elevated preoperative CA15.3 was shown to be directly related to tumor burden, which may improve its diagnostic capability. Those selected parameters could be effectively used together with plasma CA15.3 for BC screening at early stage. Furthermore, both ALU-247 and ALU-115 seem to be preoperative prognostic markers for BC.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Breast cancer (BC) represents 23% of all global cancers diagnosed worldwide among women and is the second cause of cancer death (14%) [1]. In Egypt, the incidence rate of BC is 29.9/100,000 population with the average age 30–40 years [2]. In Alexandria 2016, 36% of newly diagnosed cancer females were breast cancer [3]. Among BC patients, the failure of curative management and poor quality of life as well as the elevated morbidity and mortality rate are frequently attributed to metastasis, where the high percentage of cancer patients are diagnosed at advanced stages [4]. Accordingly, adopting and advancing measures (such as risk assessment, estimating prognosis, early diagnosis, observing therapy response and biomarkers from the tumor itself or blood) can result in an extra successful treatment, an approving outcome, and improving the quality of life for patients [5].
Currently, serum non-invasive biomarkers in BC patients are useful to provide a further effective management of the disease. CA15.3 is the most broadly used marker to follow up [6] and monitor the recurrence and metastasis in BC patients [7], but CA15.3 as a biomarker has low sensitivity and specificity [8]. Therefore, novel trustful biomarkers are urgently needed for BC diagnosis at an early stage.
In the recent years, cell-free DNA (cfDNA) can be detected in a variety of body samples such as serum, plasma, urine, and other fluids and provide a circulating picture of a specific disease [9]. Since cfDNA is proposed to be released from tumor tissue sites, so cfDNA may be used as a surrogate marker for tissue biopsies [10], a rapid, non-invasive, sensitive marker for cancer diagnosis, prognosis, and monitoring of response to therapy in different types of cancers [11]. Moreover, cfDNA integrity (cfDI), which measures the extent of cfDNA fragmentation, may be exploited as a possible diagnostic and prognostic biomarker [12].
The most of circulating cell-free DNA are belonging to DNA repeat sequences comprising short and long interspersed nucleotide elements. Arthrobacter luteus sequences (ALU) are short interspersed elements (SINEs, 300 nucleotides) [13] and the most plentiful sequences in the human genome (more than 10% of the genome), with 1.4 million copy numbers/genome [14]. In general, the cfDNA integrity was calculated as a ratio of longer DNA to shorter DNA for ALU repeats (247 and 115 bp).
Cell-free DNA is elevated in many tumor entities with different sensitivity and specificity and that allow distinguishing patients with non-malignant disease form healthy individual (e.g., patients with colorectal or periampullary cancer) [15].
Therefore, the aim of this study was to investigate the role of plasma cfDNA (ALU-247 and ALU-115) and DNA integrity as possible diagnostic and prognostic markers in breast cancer patients as compared to plasma CA15.3. In addition, the correlations of ALU-247, ALU-115, DNA integrity, and CA15.3 with clinicopathological characteristics of BC patients were analyzed.
Subject and Methods
The present study was carried out on 50 females. Ten healthy participants with no family history of BC (age range 30–65 years; mean age 48) and 40 females with BC (age range 38–65 years; mean age 50) were selected from those admitted to Department of Cancer Management and Research, Medical Research Institute Hospital, Alexandria University, from 2014 to 2015.
Patients above 65 years that had organ failure (liver, kidney, or heart), suffering from diabetes mellitus type 2, hemophilia, Alzheimer, and neurofibromatosis were excluded from the study. Healthy controls comprised of individuals with no clinically diagnosed malignancies, autoimmune diseases, or inflammation at the time of blood collection.
All patients were subjected to full medical history taking; menopausal status was confirmed and routine laboratory investigations included complete blood picture, liver and kidney function tests. Radiological examinations were performed including mammography, chest x-ray, abdominal US, bone scanning, and CT when needed.
Preoperative evaluation was carried out to all patients by fine needle aspiration cytology (FNAC) biopsy to detect the presence of malignancy or excision biopsy and then modified radical mastectomy. Postoperative histopathology examinations including tumor size, lymph node metastases, hormonal receptors (estrogen and progesterone), epidermal growth factor receptor (HER-2) histological type, vascular invasion, and histological grade and stage were performed (n = 33 early clinical stage and n = 7 advanced clinical stage) [16].
This study was approved by the local ethical committee of the Medical Research Institute, Alexandria University. Also assigned informed consent was obtained from all the participants in the present study.
Blood Specimen Collection and Processing
EDTA blood was collected from all patients at the time of diagnosis before they underwent any therapy or surgery and from controls. Plasma was separated by centrifuging blood at 6000 rpm for 10 min at 4 °C, then carefully collected from each sample and frozen at – 80 °C until used for quantification of circulating cfDNA (ALU-247 and ALU-115) by real-time PCR and CA15.3 by ELISA.
Measurement of cfDNA Concentration and Integrity by Quantitative PCR of ALU Repeats: [17]
DNA Extraction
cfDNA was extracted from 200 μL of plasma using the QIAamp DNA Mini kit (Qiagen, Hilden, Germany) following the manufacturer’s instructions and the standard protocol. DNA was detected by electrophoresis using a 1.0% agarose gel containing ethidium bromide (0.5 μg/mL) for 40 min at 100 V and the gel was observed under UV light. The eluted DNA was collected immediately, placed in ice, or stored at − 20 °C for further processing.
Quantification ALU-247 and ALU-115 Repeats by Real-time PCR
cfDNA concentration and integrity in plasma samples were examined by measuring ALU repeats (ALU-115 bp, ALU-247 bp).
The primer for 115 bp amplicon (ALU-115) amplifies both shorter and longer DNA fragments, while the primer for the 247 bp amplicon (ALU-247) amplifies only longer DNA fragments.
ALU-115 primers (Invitrogen, Life technologies, Thermo Fisher, Scientific Inc. USA) were:
-
Forward: 5/-CCTGAGGTCAGGAGTTCGAG-3/
-
Reverse: 5/-CCCGAGTAGCTGGGATTACA-3/
ALU-247 primers were:
-
Forward: 5/-GTGGCTCACGCCTGTAATC-3/
-
Reverse: 5/-CAGGCTGGAGTGCAGTGG-3/
The PCR was achieved with FastStart Universal SYBR Green Master Mix (Life Technologies—Thermo Fisher, Scientific Inc., USA) in a final volume of 25 μL containing 12.5 μL of 1× SYBR Green, 0.5 μL of 0.2 μM PCR forward primer, 0.5 μL of 0.2 μM PCR reverse primer, 5 μL DNA template, and 6.5 μL of RNase-free water. The real-time PCR amplification was performed with pre-activation of DNA polymerase at 95 °C for 15 min, followed by 40 cycles of denaturation at 94 °C for 15 s, annealing at 64 °C for 30 s, extension at 72 °C for 30 s, and then final extension at 72 °C for 10 min using StepOne™ real-time PCR (Applied Biosystems one step, Foster City, CA, USA) (Fig. 1a, b).

Amplification and melting curves for a ALU-247 and b ALU-115
The ALU-247 and ALU-115 standard curves of gently prepared genomic DNA obtained from peripheral blood leukocytes of healthy volunteers with serial dilutions from 10 ng to 0.01 pg were used to determine the absolute corresponding concentration of the ALU-247 and ALU-115 in each sample (Fig. 2a, b). Finally, the cfDNA integrity was considered as ALU-247/ALU-115.

Standard curve for a ALU-247 and b ALU-115
Determination of CA15.3
CA15.3 was determined by enzyme-linked immunosorbent assay (ELISA) (Monobind Inc., USA) according to the manufacturer’s protocol. The concentration of each sample in units per milliliter was calculated from the standard curve (Fig. 3).

Standard curve of CA15.3
Statistical Analyses
Data were fed to the computer and analyzed using IBM SPSS software package version 20.0. p values < 0.05 were statistically significant.
The distribution of quantitative variables was tested for normality using the D’Agstino test, Kolmogorov-Smirnov test, and Shapiro-Wilk test. For abnormally distributed data, comparisons between two independent populations were done using the Mann-Whitney test whereas the Kruskal-Wallis test was used to compare between different groups. Correlations between two quantitative variables were assessed using the Spearman coefficient. Agreement of the different predictive with the outcome was used and was expressed in specificity, sensitivity, negative predictive value, positive predictive value, and accuracy. The receiver operating characteristic curve (ROC) was plotted to analyze a recommended cutoff, and the area under the ROC curve denotes the diagnostic performance of the test. An area more than 50% gives an acceptable performance and an area about 100% is the best performance for the test. The Kaplan-Meier survival curve was used.
Result
Clinicopathological Characteristics of BC Patients
From Table 1, only 1 patient had a family history of BC (2.5%). Premenopausal were 18 (45%) patients and postmenopausal 22 (55%). For tumor size, 7 patients (7.5%) had T2 tumor (2–5 cm) and 33 patients (82.5%) had T3 tumor (> 5 cm). With respect to pathological type, patients with invasive ductal carcinoma (IDC) were 39 (97.5%) and only 1 patient with invasive lobular carcinoma (ILC) (2.5%). According to histological grade, 33 (82.5%) of patients were grade II and 7 (17.5%) were grade III. Negative lymph nodes were observed in 11 (27.5%) of patients whereas 29 (72.5%) patients were positive. Vascular invasion was presented only in 34 (85%) patients. For ER, 5 (12.5%) patients were negative and 35 (87.5%) patients were positive. For PR, 8 (2 0%) patients were negative and 32 (80%) patients were positive. For HER-2, 20 (50%) patients were negative and 20 (50%) patients were positive. At the beginning of the study, metastasis was detected in 5 patients (12.5%), where one patient with bone, lung, and liver metastasis and 4 patients with bone metastasis only. During follow-up period, another 9 patients develop metastasis. Finally, 2 patients (5%) were classified as pathological stage I, 31 (77.5%) stage II, 2 (5%) stage III, and 5 (12.5%) stage IV.
Molecular and Biochemical Results
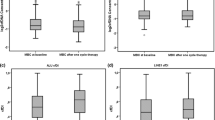
The mean values of ALU-247, ALU-115 repeats, and cfDNA integrity as well as CA15.3 concentration were significantly higher in BC patients as compared to the corresponding values in the control group (Table 2). Also, there was a significant increase in ALU-247, ALU-115 repeats, and cfDNA integrity concentration in patients with stages II, III, and IV as compared to the control group, while results from patients with stage I showed no statistical significance. The mean values of CA15.3 were significantly higher in patients with stages I, II, III, and IV than that of the control group (Fig. 4a–d). For all parameters, an association with tumor stage was established, as their relative median values upregulated with stage (p = 0.001, 0.002, 0.009, and < 0.001 respectively) (Table 3).

a ALU-247, b ALU-115, c DNA integrity, and d CA15.3 (U/mL) in control and BC patients with different stages
There was no correlation between plasma ALU-247, ALU-115 repeats, cfDNA integrity, CA15.3 concentration, and clinicopathological characteristics of BC patient group except there was a significant positive correlation between ALU-247, ALU-115, and metastasis at the beginning of the study (p < 0.001). DNA integrity was significantly positively correlated with HER2 (p = 0.03). Furthermore, CA15.3 was significantly positively correlated with tumor size and metastasis at the beginning of the study (p = 0.022 and < 0.001 respectively). Finally, there was a significant positive correlation between all parameters—ALU-247, ALU-115, cfDNA integrity, and CA15.3—(p < 0.001, 0.016, and 0.0117) except between cfDNA integrity and CA15.3 (p = 0.152) (Figs. 5a–d, 6a–c, and 7a–c).

Correlation between ALU-247 and a metastasis at the beginning of the study, b ALU-115, c DNA integrity, and d CA15.3 in patients

Correlation between ALU-115 and a metastasis at the beginning of the study, b DNA integrity, and c CA15.3 in patients

Correlation between DNA integrity and (a) HER, b CA15.3 and tumor size, and c CA15.3 and metastasis at the beginning of the study in patients
The receiver operating characteristic analysis curve was used to compare the diagnostic values of ALU-247, ALU-115, cfDNA integrity, and CA15.3 depending on the area under the ROC curve (AUC). The greater AUC corresponded to the better diagnostic test. ALU-247 showed a significant AUC (79.5%, p = 0.004) with sensitivity (70%) and specificity (100%) at cutoff 6.35. ALU-115 showed a significant AUC (78.2%, p = 0.007) with sensitivity (67.5%) and specificity (100%) at cutoff 9.6. DNA integrity showed a significant AUC (82.5%, p = 0.002) with sensitivity (77.5%) and specificity (90%) at cutoff 0.67. CA15.3 showed a significant AUC (98%, p < 0.001) with sensitivity (70%) and specificity (100%) at cutoff 8.3 (Table 4 and Fig. 8). Furthermore, the performance of ALU-247, ALU-115, cfDNA integrity, and CA15.3 to identify metastatic from non-metastatic BC patients by the ROC curve was done. Both ALU-247 and ALU-115 showed a validity for the prediction of metastases in BC patients where they showed a significant AUC (71.7%, p = 0.025; and 71.0%, p = 0.030 respectively) with the same sensitivity (64.29%) and specificity (73.08 and 76.92% respectively). On the other hand, both DNA integrity and CA15.3 showed no validity for the prediction of metastases in BC patients where they did not show significant AUC (67.2%, p = 0.076; and 57.8%, p = 0.419 respectively) with sensitivity (71.43 and 42.86% respectively) and specificity (69.23 and 92.31% respectively) (Table 5 and Fig. 9).

ROC curve for ALU-247, ALU-115, DNA integrity, and CA15.3 in breast cancer patients

ROC curve for ALU-115, ALU-247, DNA integrity, and CA15.3 in breast cancer patients
The disease-free survival (DFS) and the overall survival (OS) were estimated by the Kaplan-Meier curve. Statistically significant differences in survival between two subgroups (patients with parameter levels ≤ cutoff value and those with parameter levels > cutoff value) were assessed by the log-rank test.
For plasma ALU-247, ALU-115 repeats, and cfDNA integrity, the number of metastases and death (at the end of the follow-up period of 36 months) was higher in patients over cutoff value (> 6.35, 9.6, and 0.67 respectively) than those less than cutoff value (≤ 6.35, 9.6, and 0.67 respectively). On the other hand, the number of metastases and death was lower in patients with plasma CA15.3 level over cutoff value (32.1 and 14.3% respectively) compared to those with plasma CA15.3 level less than cutoff value (41.7 and 16.7% respectively).
For all parameters, no statistical significant difference in DFS was found between patients with elevated parameter levels and those with lower parameter levels by means of log-rank test χ2 = 2.359, 3.035, 0.796, and 0.096 (p = 0.125, 0.081, 0.372, and 0.757 respectively). The same results were found for OS χ2 = 0.576, 0.777, 0.134, and 0.777 (p = 0.448, 0.378, 0.714, and 0. 378 respectively) (Tables 6 and 7; Figs. 10 and 11).

The Kaplan-Meier survival curve for DFS a ALU-247, b ALU-115, c DNA integrity, and d CA15.3 (U/mL)

The Kaplan-Meier survival curve for OS a ALU-247, b ALU-115, c DNA integrity, and d CA15.3 (U/mL)
Discussion
Diagnosis as well as prognosis of BC patients by using sensitive and specific biomarkers is critical. Although CA15.3 is the mainly predictable diagnostic marker for BC patients, its sensitivity and specificity are little [8]. Cell-free circulating DNA as a biomarker hold great promises since it is simply accessible and reproducible [18].
This study revealed that the mean values of plasma ALU-247 and ALU-115 as well as cfDNA integrity were significantly higher in BC patients as compared to control group. These results are in accordance with the study of Stötzer et al. [19].
ALU-247 and ALU-115 are used to distinguish between necrotic cell death as well as apoptotic cells. During apoptosis, DNA fragmentation leads to DNA pieces just about 185–200 bp; the longer ALU-247 is considered a necrotic product, whereas the shorter ALU-115 corresponded to the total amount of DNA [20]. Since necrotic cell death is mainly related to tumor progressive process [21], so the longer DNA is planned to be a promising marker for cancer [20].
The increased expression of ALU-247, ALU-115, and cfDNA integrity concentration in plasma may be due to rupture of tumor tissues, necrosis, apoptosis, mitotic catastrophe, autophagia, libration by the tumor itself, normal cells, and circulation of micrometastases [22]. Since the high cellular proliferation during cancer progression is firstly counter balanced by elevating rates of apoptotic cell death and subsequently by increasing rates of necrotic cell death as the tumor becomes invasive [21], therefore, cfDNA integrity is supposed as an appropriate biomarker for detection of cancers [20].
The data obtained from this study indicated that ALU-247, ALU-115 expression, and cfDNA integrity concentration showed a trend to increase with breast cancer stage, where the mean values of these parameters were significantly higher in BC patients with stages II, III, and IV than healthy subjects. These results may be due to the released DNA from tumor cells into the circulation is elevated by lymph vascular invasion (LVI) for the reason that blood or direct lymphatic flow through the tumor cells allows spreading of viable tumor cells and increases diffusion of DNA released from dead tumor cells into the circulation. Consequently, the circulating cfDNA may be directly associated with the turnover rate of tumor cell and tumor development, representing biologic tumor aggressiveness. Thus, the circulating cfDNA integrity may be suitable for monitoring of BC progression [17].
As compared to the control group, plasma CA15.3 concentration in BC patients as well as in each stage of breast cancer was significantly high. CA15.3 is the product of the MUC-1 gene, and mucin expression is upregulated in numerous adenocarcinomas and then shed into the blood stream [23]. For that reason, the high level of CA15.3 may be due to the overexpression of MUC1 gene which encodes CA15.3 [24] and may be related to tumor burden or implied the presence of malignant disease [25]. This observation is in accordance with Park et al. who found that the elevated level of CA15.3 preoperatively may be related to a larger burden of occult disease [26].
The results demonstrated that there was no statistical correlation between circulating cfDNA (ALU-247 and ALU-115) and age, family history, menstruation, and some clinicopathological characteristics (tumor size, pathological type, histological grade, lymph node, vascular invasion, ER, PR, HER2, and metastasis during the follow-up) except with metastasis at the beginning of the study. The result is in accordance with the previous study of Zhong et al., who found a pronounced raise of cfDNA with distant metastasis [27]. Also, Tokuhisa et al. stated that the elevated concentrations of cfDNA were linked with the high metastatic potential, but not to the appearance of de novo tumor [28]. A tumor-derived DNA can be moved from cell to cell via phagocytosis of apoptotic bodies moreover is steady over time, suggesting that a tumor-derived DNA has a promising role in metastasis progression [27]. Additionally, ALU-247 and ALU-115 were correlated with each other, cfDNA integrity, and CA15.3 concentration.
When comparing the enhanced level of cfDNA integrity with other traditional staging parameters (lymph node, tumor size, and metastasis) and predictive marker (receptors status, histological grade, and HER-2), the only finding is a pronounced increase of cfDNA integrity in BC patients with HER-2.
HER-2 is a transmembrane tyrosine kinase receptor and its dimerization results in the autophosphorylation of tyrosine residues and initiates various signaling pathways leading to cell proliferation, survival, differentiation, angiogenesis, and invasion. The enlargement of HER-2 occurs in about 15–30% of BC patients [29].
From the obtained results, the plasma CA15.3 was associated with tumor size and metastasis at the beginning of the study but was not associated with other clinicopathological characteristics and cfDNA integrity. The relationship between CA15.3 and tumor size as well as metastasis appears to be reasonable, as it is considered that the tumor markers reveal the number of malignant cells as well as their access to the blood stream [30]. The lack of correlation between CA15.3 and other clinicopathological characteristics is in line with some previous studies by Hussein et al. [31] and Zheng et al. [32]. These results may be due to that these cytokines are dependent on neoplasm activity and not on the histological type of tumor [33].
Moreover, the lack of correlation between the studied parameters may be due to the heterogeneity within the groups and/or to the small sample size.
The receiver operating characteristic curve has been widely used in assessment diagnostic and prognostic power of diverse markers [34].
The values of plasma ALU-247, ALU-115, cfDNA integrity, and CA15.3 in diagnosis of breast cancer before surgery were evaluated by the ROC curve analysis. The use of the area under the ROC curve was useful in the elucidation of the validity of a specific marker in the early detection of breast cancer. For plasma ALU-247, AUC = 79.5%, p = 0.004; for ALU-115, AUC = 78.2%, p = 0.007; for DNA integrity, AUC = 82.5%, p = 0.002, while for plasma CA15.3, AUC = 98%, p < 0.001. These results indicate the validity of using plasma ALU-247, ALU-115, DNA integrity, and plasma CA15.3 as diagnostic markers for breast cancer. In addition, plasma CA15.3 was superior to cfDNA integrity followed by ALU-247 and ALU-115 for prediction of BC patients.
The prognostic performance of plasma ALU-247, ALU-115, cfDNA integrity, and plasma CA15.3 before surgery to predict metastasis was evaluated by ROC curve analysis. The results revealed that both plasma ALU-247 and ALU-115 are good in identifying patients who developed metastasis from those who did not have metastasis in breast cancer (AUC = 71.7%, p = 0.025; and AUC = 71.0%, p = 0.03, respectively) while both cfDNA integrity and plasma CA15.3 are poor in identifying patients who developed metastasis from those who did not have metastasis in breast cancer (AUC = 67.2%, p = 0.076; and AUC = 57.8%, p = 0.419, respectively).
Survival Estimates by the Kaplan-Meier Curves
Disease-free survival (DFS) is defined as from the day of surgery until first evidence of disease progression. Overall survival (OS) is defined as the time between primary surgery and the patient’s death. Deaths from another cause than cancer or survival until the end of the observation period are considered as censored observations [34]. By comparing patients presenting plasma ALU-247, ALU-115, cfDNA integrity, and CA15.3 higher than cutoff values (6.35 ng/ml, 9.6 ng/ml, 0.67, and 8.3 U/ml respectively) to those with a concentration less than cutoff values did not show any significant difference for DFS or OS.
Plasma ALU-247, ALU-115, cfDNA integrity, and CA15.3 failed to predict survival or relapse in BC patients before surgery. These results are in line with the previous study, which indicated that CA15.3 was not significantly correlated with DFS of the breast cancer patients. Other studies also reported variable results on the prognostic value of CA15.3, and the variable cutoff values and short follow-up duration might contribute to this contradiction [26].
In conclusion, since circulating plasma ALU-247, ALU-115, and cfDNA integrity are significantly high in BC patients, so their measurement may prove to have clinical utility in diagnosis of BC. Elevated preoperative CA15.3 level was shown to be directly related to the tumor burden, which may improve its diagnostic capability for BC. The selected parameters (plasma ALU-247, ALU-115, and cfDNA integrity) are ideal early biomarkers for BC diagnosis, so they could be effectively used with plasma CA15.3 for BC screening at early tumor stage. Furthermore, both ALU-247 and ALU-115 seem to be preoperative prognostic markers for breast cancer. However, large-scale prospective studies are recommended by using large number of samples and long follow-up duration to establish the clinical utility of those parameters.
References
Jemal, A., Bray, F., Center, M. M., Ferlay, J., Ward, E., & Forman, D. (2011). Global cancer statistics. CA: a Cancer Journal for Clinicians, 61(2), 69–90.
Ibrahim, A. S., Khaled, H. M., Mikhail, N. N., Baraka, H., & Kamel, H. (2014). Cancer incidence in Egypt: results of the national population –based cancer registry program. Journal of Cancer Epidemiology, 2014, 1–18.
Alexandria Cancer Registry. Medical Research Institute. Annual Report 2016.
Kaczor-Urbanowicz, K. E., Martın Carreras-Presas, C., Kaczor, T., Tu, M., Wei, F., Garcia-Godoy, F., et al. (2017). Emerging technologies for salivaomics in cancer detection. Journal of Cellular and Molecular Medicine, 21, 640–647.
Cardoso, F., Castiglione, M., & Group EGW. (2009). Locally recurrent or metastatic breast cancer: ESMO clinical recommendations for diagnosis, treatment and follow-up. Annals of Oncology, 20, 15–18.
Daniele, A., Divella, R., Trerotoli, P., Abbate, I., Paradiso, A., & Casamassima, P. (2013). Clinical usefulness of cancer antigen 15.3 in breast cancer patients before and after surgery. Open Breast Cancer J, 5(1), 1–6.
Tarhan, M. O., Gonel, A., Kucukzeybec, Y., Somali, I., Erten, C., Dirican, A., et al. (2013). Prognostic significance of circulating tumor cells and serum CA15.3 levels in metastatic breast cancer, single center experience, preliminary results. Asian Pacific Journal of Cancer Prevention, 14(3), 1725–1729.
Hanash, S. M., Baik, C. S., & Kallioniemi, O. (2011). Emerging molecular biomarkers—blood-based strategies to detect and monitor cancer. Nature Reviews. Clinical Oncology, 8(3), 142–150.
De Mattos-Arruda, L., & Caldas, C. (2016). Cell-free circulating tumour DNA as a liquid biopsy in breast cancer. Molecular Oncology, 10(3), 464–474.
De Mattos-Arruda, L., Cortes, J., Santarpia, L., Vivancos, A., Tabernero, J., Reis-Filho, J. S., et al. (2013). Circulating tumour cells and cell-free DNA as tools for managing breast cancer. Nature Reviews. Clinical Oncology, 10(7), 377–389.
Volik, S., Alcaide, M., Morin, R. D., & Collins, C. (2016). Cell-free DNA (cfDNA): clinical significance and utility in cancer shaped by emerging technologies. Molecular Cancer Research, 14(10), 898–908.
Madhavan, D., Wallwiener, M., Bents, K., Zucknick, M., Nees, J., Schott, S., Cuk, K., Riethdorf, S., Trumpp, A., Pantel, K., Sohn, C., Schneeweiss, A., Surowy, H., & Burwinkel, B. (2014). Plasma DNA integrity as a biomarker for primary and metastatic breast cancer and potential marker for early diagnosis. Breast Cancer Research and Treatment, 146(1), 163–174.
Lei, K. I., Chan, W. Y., Johnson, P. J., & Lo, Y. M. D. (2002). Diagnostic and prognostic implication of circulating cell-free Epstein-Barr virus DNA in natural killer/T cell lymphoma. Clinical Cancer Research, 8(1), 29–34.
Wang, B. G., Huang, H. Y., Chen, Y. C., Bristow, R. E., Kassauei, K., Cheng, C. C., et al. (2003). Increased plasma DNA integrity in cancer patients. Cancer Research, 63(14), 3966–3968.
Umetani, N., Kim, J., Hiramatsu, S., Reber, H. A., Hines, O. J., Bilchik, A. J., & Hoon, D. S. (2006). Increased integrity of free circulating DNA in sera of patients with colorectal or periampullary cancer: direct quantitative PCR for ALU repeats. Clinical Chemistry, 52(6), 1062–1069.
Edge, S. B. (2010). Breast. In S. B. Edge, D. R. Byrd, & C. C. Compton (Eds.), AJCC Cancer Staging Manual (7th ed., pp. 347–376). New York: Springer.
Umetani, N., Giuliano, A. E., Hiramatsu, S. H., Amersi, F., Nakagawa, T., Martino, S., & Hoon, D. S. B. (2006). Prediction of breast tumor progression by integrity of free circulating DNA in serum. Journal of Clinical Oncology, 24(26), 4270–4276.
Schwarzenbach, H., Hoon, D. S. B., & Pantel, K. (2011). Cell-free nucleic acids as biomarkers in cancer patients. Nature Reviews Cancer, 11(6), 426–437.
Stötzer, O. J., Lehner, J., Fersching-Gierlich, D., & Nagel, D. (2014). Diagnostic relevance of plasma DNA and DNA integrity for breast cancer. Tumor Biology, 35(2), 1183–1191.
Jahr, S., Hentze, H., Englisch, S., Hardt, D., Fackelmayer, F. O., Hesch, R. D., & Knippers, R. (2001). DNA fragments in the blood plasma of cancer patients: quantitation and evidence for their origin from apoptotic and necrotic cells. Cancer Research, 61(4), 1659–1665.
Jin, Z., & El-deiry, W. S. (2005). Overview of cell death signaling pathways. Cancer Biology & Therapy, 4(2), 139–163.
Gormally, E., Caboux, E., Vineis, P., & Hainaut, P. (2007). Circulating free DNA in plasma or serum as biomarker of carcinogenesis: practical aspects and biological significance. Mutation Research/Reviews in Mutation Research, 635(2-3), 105–117.
Perey, L., Hayes, D. F., Maimonis, P., Abe, M., O'Hara, C., & Kufe, D. W. (1992). Tumor selective reactivity of a monoclonal antibody prepared against a recombinant peptide derived from the DF3 human breast carcinoma-associated antigen. Cancer Research, 52(9), 2563–2568.
Jamall, S., Ishaq, M., Alam, J. M., & Khadim, M. (2010). CA 15-3 and lipid profile in preoperative breast cancer patients. Pakistan Journal of Biochemistry and Molecular Biology, 43, 114–118.
Hewala TI, Abd EL-Moneim NA, Ebied SA, Sheta MI, Soliman K, Abu-EL-Enean A. Diagnostic and prognostic value of serum nitric oxide, tumor necrosis factor-a, basic fibroblast growth factor and copper as angiogenic markers in premenopausal breast cancer patients: a case-control study. British Journal of Biomedical Science 2010; 67:167–176, 4.
Park, B. W., Oh, J. W., Kim, J. H., Park, S. H., Kim, K. S., Kim, J. H., & Lee, K. S. (2008). Preoperative CA 15-3 and CEA serum levels as predictor for breast cancer outcomes. Annals of Oncology, 19(4), 675–681.
Zhong, X. Y., Ladewig, A., Schmid, S., Wight, E., Hahn, S., & Holzgreve, W. (2007). Elevated level of cell-free plasma DNA is associated with breast cancer. Archives of Gynecology and Obstetrics, 276(4), 327–331.
Tokuhisa, Y., Iizuka, N., Sakaida, I., Moribe, T., Fujita, N., Miura, T., Tamatsukuri, S., Ishitsuka, H., Uchida, K., Terai, S., Sakamoto, K., Tamesa, T., & Oka, M. (2007). Circulating cell-free DNA as a predictive marker for distant metastasis of hepatitis C virus-related hepatocellular carcinoma. British Journal of Cancer, 97(10), 1399–1403.
Iqbal, N., & Iqbal, N. (2014). Human epidermal growth factor receptor 2 (HER2) in cancers: overexpression and therapeutic implications. Molecular Biology International, 2014, 1–9.
Molina, R., Auge, J. M., Farrus, B., Zanón, G., Pahisa, J., Muñoz, M., et al. (2010). Prospective evaluation of carcinoembryonic antigen (CEA) and carbohydrate antigen 15.3 (CA 15.3) in patients with primary locoregional breast cancer. Clinical Chemistry, 56(7), 1148–1157.
Hussein, N. A., Anwer, M. M., EL-kerm, Y., Abozaid, N. A., & Rashad, M. M. (2013). Evaluation of serum big endothelial-1 for the diagnosis and prediction of disease recurrence in breast cancer patients. Journal of Cancer Research and Therapeutics, 7, 178–185.
Zheng, Y., Chen, Y., Hu, M., Lin, Y., & Chen, Y. (2012). Correlation of preoperative serum tumor markers and clinic0pathological features in breast cancer. Cancer Clinical Oncology, 1, 124–132.
Quaranta, M., Daniele, A., Coviello, M., Venneri, M. T., Abbate, I., & Caringella, M. E. (2007). MMP-2, MMP-9, VEGF and CA 15.3 in breast cancer. Anticancer Research, 27(5B), 3593–3600.
Ma, S., & Song, X. (2010). Ranking prognosis markers in cancer genomic studies. Briefings in Bioinformatics, 12, 33–40.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in the study involving human participants were in accordance with the Local Ethical Committee of the Medical Research Institute, Alexandria University.
Informed Consent
Written informed consent was obtained from all patients included in the study.
Rights and permissions
About this article

Cite this article
Hussein, N.A., Mohamed, S.N. & Ahmed, M.A. Plasma ALU-247, ALU-115, and cfDNA Integrity as Diagnostic and Prognostic Biomarkers for Breast Cancer. Appl Biochem Biotechnol 187, 1028–1045 (2019). https://doi.org/10.1007/s12010-018-2858-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12010-018-2858-4