
Abstract
Purpose
Children of parents with mental health problems (CPM) have an increased risk for impaired health-related quality of life (HRQoL). This study aims at investigating the age- and gender-specific course of HRQoL and at exploring predictors of HRQoL in CPM based on longitudinal data (baseline, 1-year and 2-year follow-up) of a German population-based sample.
Methods
Longitudinal data from the German BELLA study was analyzed (n = 1429; aged 11 to 17 years at baseline). The SCL-S-9 in combination with the cutoff for the General Severity Index (GSI) from the longer SCL-90-R served to identify CPM (n = 312). At first, we compared domain-specific HRQoL according to the KIDSCREEN-27 in CPM versus Non-CPM. Focusing on CPM, we used individual growth modeling to investigate the age and gender-specific course, and to explore effects of risk and (personal, familial and social) resource factors on self-reported HRQoL in CPM.
Results
Self-reported HRQoL was reduced in CPM compared to Non-CPM in all domains, but in social support & peers. However, a minimal important difference was only reached in girls for the domain autonomy & parent relation. Internalizing and externalizing mental health problems were associated with impaired HRQoL in CPM. Self-efficacy, social support and family climate were identified as significant resources, but parental mental health problems over time were not associated with any investigated domain of HRQoL in CPM.
Conclusions
Adolescent female CPM may be especially at risk for reduced HRQoL. When developing support programs for CPM, self-efficacy, social support and family climate should be considered, HRQoL and mental health problems in CPM should be addressed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Plain English Summary
Children whose parents suffer from mental health problems have an increased risk for developing mental health problems themselves. Whether they have also an increased risk for impaired well-being is in question and could be important for supporting them more effectively.
In this study, we explored the well-being of children aged from 11 to 17 years whose parents suffered from mental health problems. The children and their parents answered various questionnaires three times during a time span of 2 years.
This study indicates that adolescent girls of parents with mental health problems may have an increased risk for reduced well-being. Moreover, self-efficacy, social support and family climate were relevant for the well-being of the children. Unexpectedly, the mental health problems of their parents were not significantly associated with the children’s well-being in this study. Findings from this study are important for supporting children whose parents suffer from mental health problems.
Introduction
Children of parents with mental health problems (CPM) have an increased risk of psychological and developmental difficulties compared to children of parents without mental health problems. In a German population sample, 18.6% of the children had parents with mental health problems [1]. Recent reviews revealed that about 50% of the CPM develop mental health problems in childhood or adolescence. While mental health problems in CPM have comprehensively been studied [2, 3], research on health-related quality of life (HRQoL) in CPM is rare so far. However, the few existing results suggest that HRQoL in CPM may also be compromised compared to the reference population [4].
HRQoL has gained increasingly importance in the research of a multitude of health conditions over the last decades. As a multidimensional construct, HRQoL covers physical, emotional, social and behavioral components of the subjective well-being and functioning [5, 6]. Consensus prevails, that it is always preferable to obtain the child´s own report on HRQoL if possible; parent- and proxy-reports may be gathered in addition [7].
Findings of epidemiological studies on children and adolescents of the general population reported that HRQoL decreased with ongoing age, girls reported lower HRQoL than boys and girls had a greater decrease with age than boys. Significant predictors of HRQoL were mental health problems and physical problems of children and adolescents, as well as age, gender, and the socioeconomic status [8, 9]. Some epidemiological studies considered the association of children’s HRQoL with parental mental health problems. In a Greek nation-wide random sample of children and their parents [10] parental subjective mental health status was significantly correlated with children’s physical and psychological well-being, moods and emotions, parent–child relationship, school environment and financial resources. Parental subjective physical health in contrast was associated only with the children’s self-perception, and no other HRQoL dimension. Male gender, younger age, social support and the absence of chronic health care needs were positively associated with children’s HRQoL. In a longitudinal study [11], based on data of the BELLA study, significant predictors of HRQoL of the children were mental health problems and physical problems of the children, mental health problems of the parents, and age, gender, migration background and socioeconomic status. Otto and colleagues [12] found in their longitudinal study, also using data of the BELLA study, that mental health problems as well as parental mental health problems were negatively, whereas self-efficacy, family climate, and social support were positively associated with children’s initial HRQoL. In this study, changes in mental health problems were negatively, changes in self-efficacy and social support were positively associated with the change of HRQoL over time.
Two recent reviews incorporate 57 studies concerning HRQoL in children with mental disorders [13, 14]. They consistently state that HRQoL in children with various mental disorders was compromised across multiple domains and across several disorders compared to healthy controls. The largest effect sizes were found for psychosocial and family-related domains and for the total HRQoL score, whereas physical domains generally were less affected [13]. No clear HRQoL domain profiles distinguishing different diagnoses were discerned. Most of the studies included clinical samples and cross-sectional designs, thus limiting the interpretability and transferability of results.
HRQoL of CPM in clinical samples of parents have only rarely been studied. In a small sample of psychiatric inpatients and their children, the overall HRQoL in the children was associated with the severity of parental symptomatology, parental somatization and depression. Moreover, parental perceived impairment was associated with children’s HRQOL and children’s psychopathology was associated with their HRQoL [15, 16]. Dittrich [17] found in a sample of mothers with and without a history of depression and/or early life maltreatment and their children an association of maternal history of depression (but not of maternal history of early life maltreatment) and HRQoL of the children. In children, whose parents received treatment for severe physical illness, mental illness or substance abuse, children’s self-reported HRQoL was positively associated with their social skills [18]; boys and younger children reported better HRQoL in several domains compared to girls and older children and children in this sample reported significantly lower HRQoL than the reference population in one domain, namely physical well-being [4].
In a cross-sectional study of CPM [19] based on data of the BELLA study, significant resources for HRQoL of the children were self-efficacy, optimism, family climate, and school climate, suggesting that a combination of personal, familial and social resources and particularly resources outside of the family may be important for CPM.
Findings suggest [18, 19] that personal resources such as the cognitive and social capabilities of the youth, as well as positive family relationships and social support, act as resource factors for CPM. In order to develop specific support programs for this high-risk group, resource factors, especially those that can be influenced by therapeutic or preventive interventions, should be studied in greater detail.
To our knowledge, this is the first study, investigating the gender- and age-specific course as well as risk and resource factors of HRQoL in CPM. Existing literature suggests that CPM may have a reduced HRQoL compared to children of the general population. To date only very few studies have investigated this association. Especially results based on self-reported HRQoL and longitudinal data are missing. The current study aims at investigating the age- and gender-specific course of HRQoL in CPM and exploring risk factors and personal, familial and social resource factors for HRQoL in CPM based on longitudinal data of a CPM sample from the general population. Our hypotheses are:
-
1.
Increasing mental health problems of the parents are associated with decreasing HRQoL in CPM.
-
2.
HRQoL in CPM is reduced compared to children of parents without mental health problems (Non-CPM).
-
3.
Decrease of HRQoL with ongoing age is more pronounced in female CPM compared to female Non-CPM.
-
4.
Increasing internalizing and externalizing problems in CPM are each associated with decreasing HRQoL in CPM.
-
5.
Stronger personal, familial and social resources are each associated with better HRQoL in CPM.
The analyses were conducted in a sample of children and adolescents aged 11 to 17 years comparing CPM and Non-CPM. Further analyses focused on CPM investigating the age- and gender-specific course and exploring risk and resource factors of HRQoL controlling for sociodemographic variables.
Methods
Study design
We analyzed data from the longitudinal BELLA study, which is the mental health module of the German National Health Interview and Examination Survey for children and adolescents (KIGGS). The baseline assessment of the BELLA study (conducted 2003 to 2006) included 2863 children and adolescents aged 7 to 17 years. It was followed up by further assessments including a 1-year (2004 to 2007) and a 2-year follow-up (2005 to 2008). Self- and parent-reported data was collected by computer-assisted telephone interviews and paper–pencil questionnaires using psychometrically sound and established measures, if available; self-reports were gathered from 11 years on. Ethical approval was received from the ethics committee of the University Hospital Charité in Berlin and the Federal Commissioner for Data Protection in Germany. More information on design and methods of both studies are published [20, 21].
Sample
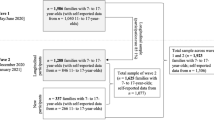
We investigated data from the baseline assessment, 1-year and 2-year follow-ups of the BELLA study. Cases were included in this study, if (i) aged 11 to 17 years at baseline (n = 1724), (ii) valid scores in the five KIDSCREEN scales were given for at least one measurement point each (n = 1589), and (iii) parent-reported data was reported by the same biological parent at each measurement point (n = 1472). Within this sample, n = 1334 had valid scores in at least one domain of HRQoL at baseline and were used for comparing CPM with Non-CPM.
Selection of the main study sample
Within the above described sample (n = 1472), we identified children and adolescents who had parents with considerable mental health problems at baseline (n = 312 CPM). To identify CPM, the Symptom-Check List Short-version (SCL-S-9) [22] was used, which represents an abbreviated 9-item version of the SCL-90-R [23]. The SCL-90-R is a multidimensional screening measure for mental symptoms and provides with its General Severity Index (GSI) a very established index for overall psychological stress [24]. The shorter SCL-S-9 includes one item of each SCL-R-90 scale and showed good reliability and good model fit for a one-factor model in a recent German study [24]; these authors reported a very high correlation (r = 0.93) between the GSI resulting from the SCL-S-9 and the GSI of the SCL-90-R [24]. Please note, that those authors used the term SCL-K-9, but we are using the term SCL-S-9 to describe the same measure (as already done in former articles from the BELLA study [1, 11, 12, 19, 21, 25,26,27,28]). In the present study (in line with former publications from the BELLA study on CPM [1, 26, 27]), we used parent-reported baseline data and calculated the SCL-S-9 sum score. We then adapted the SCL-S-9 to the SCL-90-R sum score (by simple multiplication). Subsequently, we followed the recommended procedure for the SCL-90-R by transferring the sum score into T-values and using the cutoff of the GSI (T-values ≥ 63 indicate mental health problems) to allow a gender-specific identification of parents with mental health problems [29]. This lead to a sample of n = 312 CPM aged 11 to 17 years at baseline in the present study.
Measures
The following constructs were measured at each measurement point, only SES and migration background were solely measured at baseline.
HRQoL in CPM was assessed using the self-report of the well-established KIDSCREEN-27 [30, 31] which includes 27 items and covers the domains physical well-being, psychological well-being, autonomy & parent relation, social support & peers, and school. T-values (M = 50; SD = 10) were calculated based on Rasch Person-parameters of a European norm sample [30]. Higher T-values indicate better domain-specific well-being.
Parental mental health problems were gathered from parents using the Symptom-Check List Short-version (SCL-S-9) [22] (for more information please see Sample, Selection of the main study sample). The SCL-S-9 was not only used to select the main study sample based on baseline data, we used the SCL-S-9 sum scores additionally as assessed at each measurement point in our analyses on predictors of HRQoL to control for parental mental health problems over time.
Internalizing and externalizing mental health problems of CPM were measured with the self-report of the Strengths and difficulties questionnaire (SDQ) [32]. The SDQ scale on internalizing problems gathers the subscales emotional symptoms and peer related problems (five items per subscale); the scale on externalizing problems includes the five-item subscales conduct problems and hyperactivity/inattention [33]. For each scale, higher scores reflect more severe problems.
Self-efficacy in CPM was measured using the self-reported version of the General Self-Efficacy Scale (GSE) [34]. Higher GSE sum scores (over its ten items) reflect higher self-efficacy.
Family climate was assessed using self-reports of CPM based on the German Family Climate Scale (FCS) [35]. In the BELLA study, eight items of the FCS were administered which refer to active recreational organization and cohesion. Higher sum scores over the FCS items indicate better family climate.
Social support was measured by self-reports based on the Social Support Survey (SSS) [36]. Eight items of the original SSS were administered, which were slightly modified for use in children and adolescents to assess how frequent specific types of support are available. Higher sum scores over all items indicate more frequent social support.
SES was assessed by means of the Winkler-index [37] that gathers information on education, profession and income of both parents. In our multivariate analyses we used the metric score of the Winkler-index (range: 3 to 21). Only for the purpose of sample description, participants were allocated to groups with low (scores from 3 to 8), medium (9 to 14) and high SES (15 to 21) [38].
Migration background was determined based on Schenk [39] gathering information on countries of birth and citizenship. Migration background was assumed, if (i) the child or adolescent immigrated to Germany and had at least one parent not born in Germany, or if (ii) at least one parent immigrated to Germany and did not hold German citizenship.
Data analysis
At first, we compared HRQoL in CPM versus Non-CPM using the described sample of children and adolescents aged 11 to 17 years (n = 1334), domain-specific T-values and baseline data. We conducted T-tests, and we considered Cohen’s d and half a standard deviation as threshold for a minimal important difference.
Subsequently, we focused on CPM (n = 312) and used individual growth modeling to investigate age- and gender-specific effects on HRQoL in CPM based on data from all three measurement points. For each KIDSCREEN-27 domain a model was calculated including age (at baseline), gender, the interaction age by gender, a time variable (with information about the intervals between measurement points in years) and a squared time variable (time × time) as fixed effects; only time was additionally used as random effect. We further examined, if a cohort effect was given (investigating the interaction between age and measurement point for each outcome). Graphs were created on the age-specific course of HRQoL in male and female CPM using Estimated Marginal Means from the corresponding models.
Moreover, we explored predictors of HRQoL in CPM over time using linear mixed models with repeated measurements (the intercept represents the individual score at baseline, the slope reflects the individual change per year). Again, domain-specific models were calculated. We followed a stepwise approach starting with the null-models (including the outcome, but no further predictors) [40]. Subsequently, we added (i) level 1-predictors (i.e., time variables and variables for all constructs measured longitudinally), (ii) level 2-predictors (sociodemographic variables measured only at baseline), and (iii) interaction terms (i.e., time × age, time × gender, age × gender, and age × gender × time) to each model. Please note that we kept only those interaction terms in our final models, which were significant for at least one domain. Predictors served as fixed effects, only time was additionally used as random effect. The squared time variable was only kept in a model, if this improved model fit according to the log likelihood difference-test and the Bayesian information criterion (BIC). We used McFadden’s R2 [41] to roughly estimate the strengths of effects based on log likelihood estimates of models with and without the predictor in question. Finally, we checked our results for effects according to the responding parent (mother vs. father). Prior to the analyses, we centered metric predictors by the grand mean. Analyses were conducted using IBM SPSS 26 and Maximum-Likelihood estimation.
Results
At first, we investigated the sample of children and adolescents aged 11 to 17 years at baseline (n = 1334; age: M = 13.92, SD = 1.977; 51% female; SES: 22% low, 51% medium, 27% high; 7% migration background, and 92% with mother-reported parental mental health problems). We found significantly lower means in each domain for CPM compared to Non-CPM (see Table 1). For social support & peers the difference was only negligible (Cohen’s d < 0.20), but for remaining domains effect sizes indicated small differences. However, for no domain the threshold for a minimal important difference was reached. Results of gender-specific comparisons (see Table 1) indicated a minimal important difference only among girls and only in autonomy & parent relation. Subsamples of CPM (n = 273) and Non-CPM (n = 1061) did not differ in gender or migration background (p > 0.05 each), only negligible differences in age (p = 0.037; Cohen’s d < 0.20) and responding parent were found (p = 0.044; ϕ < 0.10). For the significant difference in SES a small effect size was found (Cohen’s d = 0.31; Cramer’s V/Contingency Coefficient = 0.11); in line with the literature [1, 42] we found lower SES in CPM compared to Non-CPM.
In the subsample of CPM (n = 312) mean age was about 14 years (M = 14.14; SD = 1.992), about half of the CPM were female (49%), half of the participants had a medium SES (low: 32%; medium: 50%; high: 18%), a tenth had a migration background (10%), and for the great majority mothers reported on parental mental health problems (88%; 12% with fathers’ reports). Means and standard deviations of scale scores for each measurement point are depicted in Table 2.
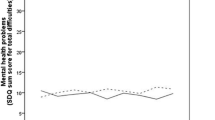
Age- and gender-specific effects on HRQoL in CPM (n = 312) were investigated over time. Better physical well-being was found in boys compared to girls (b = − 4.26, 95% Confidence Interval (95%; CI) = − 5.73, − 2.78; p < 0.001) and an interaction effect indicated decreasing physical well-being with ongoing age especially for girls (b = − 1.13, CI = − 1.87, − 0.39; p = 0.003). For psychological well-being results were similar with higher scores for boys (b = − 4.34, CI = − 6.01, − 2.67; p < 0.001) and decreasing well-being with ongoing age for girls (b = − 1.23, CI = − 2.07, − 0.38; p = 0.004). Concerning autonomy & parent relation, higher scores in boys were found (b = − 3.00, CI = − 4.62, − 1.39; p < 0.001). For social support & peers no age- or gender-specific effect was detected. For school, an interaction effect indicated higher scores for girls in younger and for boys in older participants (b = − 0.79, CI = − 1.53, − 0.06; p = 0.034). No evidence was found for a cohort effect for any outcome. Figure 1 presents graphs on the age- and gender-specific course of HRQoL in CPM.

Age- and gender-specific trajectories of health-related quality of life according to the domains of the KIDSCREEN-27 in children of parents with mental health problems (aged 11 to 19 years)
We further explored predictors of HRQoL in CPM over time (n = 312). Intra class-correlations (ICCs) from null-models indicated that between 31 and 50% of the total variance in the outcomes could be explained by differences between the subjects. Results of final models are presented in Table 3 (average scores for each outcome after controlling for covariates can be found in the line on the intercept, changes over time in the lines on Time and Time × time).
Better physical well-being was associated with less severe internalizing and externalizing child problems, higher self-efficacy, and better family climate over time. Better psychological well-being was associated with less pronounced internalizing and externalizing problems, higher self-efficacy and more social support over time. For both models, fit improved most by adding self-efficacy (McFadden’s R2 = 0.02). Better well-being according to autonomy and parent relation was related to less severe internalizing problems, better family climate and more social support. McFadden’s R2 indicated that most improvement was gained by adding family climate and social support (0.02 for each). Higher scores in social support & peers were related to less severe internalizing problems, higher self-efficacy and more social support over time. Self-efficacy and social support lead to the most improvement of model fit (McFadden’s R2 = 0.02 for each). Better well-being concerning school was related to less severe externalizing problems, higher self-efficacy and better family climate over time. Model fit improved most by including self-efficacy (McFadden’s R2 = 0.02).
Random effects (Table 3) underlined that a relatively high amount of variance in each outcome could be explained by inter-individual differences (less by changes over time). The residual variance estimates showed that considerable amounts of variance for each outcome were left unexplained.
Please note that, age- and gender-specific effects in our final predictor models were in line with domain-specific findings reported above (resulting from models on age- and gender-specific trajectories). Finally, we found no significant effect for the responding parent (mother vs. father) in any of our models.
Discussion
The present study compared HRQoL in CPM to Non-CPM, investigated the course of HRQoL in CPM over a period of two years and explored predictors for HRQoL in CPM over time. We found slightly reduced HRQoL in four out of five domains in CPM compared to Non-CPM. The age- and gender-specific course of HRQoL in CPM was roughly in line with results reported from the general population. Internalizing and externalizing problems constituted risk factors for HRQoL in CPM, whereas self-efficacy, family climate and social support were identified as resources for several HRQoL domains in CPM. Contrary to former findings in clinical samples we found no association of parental mental health problems with HRQoL in CPM over time.
Comparing HRQoL in CPM and Non-CPM, we only found a minimal important difference in females in the domain autonomy and parent relation. Similarly, HRQoL in children of parents with mental or somatic illness or substance abuse [4] was lower in only one HRQoL domain compared to the reference population, that is physical well-being. Boys in this study even reported significantly higher scores on peers & social support and school compared to the reference population. Male CPM may be able to activate resources of their peer and school environment to compensate for familial difficulties, female CPM may feel responsible for their ill parents and consequently their development of autonomy is impeded. Results suggest, that HRQoL in CPM is only slightly reduced compared to Non-CPM, but the development of autonomy in female CPM may be particularly at risk.
The gender and age-specific course we found in CPM corresponds largely to the course of HRQoL in German population samples [9, 11, 12] with predominantly better HRQoL in boys compared to girls and decreasing scores with ongoing age especially for girls. Nevertheless, female CPM, particularly with ongoing age, may be especially at risk for impeded HRQoL. Moreover, studies regarding mental health problems of CPM indicate that female CPM have a higher risk to develop mental health problems compared to male CPM [43]. Increasing internalizing and externalizing mental health problems were associated with decreasing HRQoL in CPM in the present study corresponding with former studies on children with mental health problems [13, 14, 44] and our hypotheses.
Self-efficacy, family climate and social support were identified as resources for several HRQoL domains in CPM over time in line with findings for the general population from another longitudinal study based on data of the BELLA study [12]. Likewise, social support served as a resource factor for HRQoL in a Greek population sample [10]. The associations between self-efficacy and HRQoL domains we found in CPM are in line with findings in a sample of children and adolescents with psychiatric disorders [44]. The relationships we found between family climate and HRQoL domains correspond to findings in a sample of adolescents referred for psychiatric services over a 3-year period [45]. The associations between social support and HRQoL domains in our study are in line with existing results in children of parents with mental or physical illness or substance use [18] and in a sample of children and adolescents with psychiatric disorders [44]. In summary, our study confirms existing results regarding children of the general population and children with mental health problems for the investigated resources, in CPM largely. Existing results in CPM are likewise in line with our results [18, 19] and stress the importance of the investigated resources for prevention and intervention in CPM.
Whether mother or father reported on their own mental health problems, showed no impact on HRQoL in CPM in our study. Concordantly, existing results suggest that paternal psychiatric problems can be associated with an increased risk of adverse child outcomes, independent from maternal psychiatric problems. The impact of paternal mental health problems may differ from mothers´ but also plays an important role for children’s development [46, 47]. Future studies may wish to investigate these aspects in more detail.
Opposed to existing studies, our results showed no significant associations of children`s HRQoL with parental mental health problems over time [10,11,12]. We selected our sample from a German population sample comprising parents with mental health problems. If parental mental health problems persist over a longer period of time, children and parents may adjust their standards to their individual levels of impairment and may report no particular problems [48], thus obscuring the expected association. Moreover, change of parental mental health problems may not be associated with timely change of children’s HRQoL. Future studies may wish to investigate whether the assessment of mental health problems and HRQoL depend not only on respective symptomatology but also on the state and course of parental mental health problems. Moreover, self-reported HRQoL in children and adolescents of our sample differed from Non-CPM only for girls in one domain. Possibly, our subsample was not as impaired as other clinical samples investigated by former studies [11, 15, 17], thus obscuring the expected association.
Parental mental health problems in our sample were assessed by parent-reports of the SCL-S-9 asking for mental health problems during the last 7 days. If parental mental health problems persist over a longer period of time as common in chronic problems like, e.g., depression, the assessment of problems during the last seven days could be difficult in contrast to a “normal state” and could lead to underestimating as well as overestimating the current mental health problems. Moreover, we draw our subsample of CPM by identifying children and adolescents with parents who reported mental health problems at baseline and mental health problems in these parents did not necessarily sustain or re-appear at 1-year and/or 2-year follow-ups. We controlled for changes in parental mental health problems over time in our models on predictors, but still research in CPM whose parents have persistent long-term mental health problems would be very important. Further, information on parental mental health problems in the present study was assessed by only one parent, information about the second parent was not obtained. The risk for children to develop adversities is significantly higher, if both parents suffer from mental health problems compared to only one parent with mental health problems [43, 49]. Moreover, we explored effects for only a selection of predictors for HRQoL in CPM, for instance somatic problems or chronic health conditions were not included in our analyses. Future studies should investigate effects of further predictors in corresponding studies.
The present study is based on the same data set (baseline, follow-up 1 and follow-up 2) as our previous study on trajectories of mental health problems in CPM [26], where parental mental health problems were associated with internalizing mental health problems of the children over time; three other studies [1, 19, 27] regarding CPM based on data of the BELLA study used cross-sectional data. Further longitudinal analyses from the BELLA study investigated among others effects of parental mental health problems on the unselected sample of children and adolescents [11, 12, 21, 25, 28]. In those analyses parental mental health problems were identified as significant risk factor for child and adolescent mental health and HRQoL. We could not find corresponding associations focusing on HRQoL in a smaller sample of CPM. Our results suggest that change in parental mental health problems may not be associated with timely change in the children’s HRQoL. Future research should investigate further, in how far changes in parental mental health problems over time are associated with changes in HRQoL of their children.
Strengths and limitations
The present study has the following main limitations. Neither the investigated children, nor the parents received a clinical diagnose confirmed by clinical interviews. Future studies may further wish to assess mental health problems from both parents. Our analyses on risk and resource factors are only exploratory considering the size of the investigated sample; future studies may wish to confirm our findings. Future studies may further wish to investigate effects of additional predictors on HRQoL in CPM and associations with parental HRQoL (with measures that focus on similar aspects of HRQoL). Finally, the investigated time span only covered two years; future studies may wish to investigate CPM over a longer period.
The present study also has several strengths. We analyzed data of the general German population, whereas previous German studies on CPM have predominantly investigated clinical samples [15, 17]. The present data should thus fill an important gap in the existing literature. We further analyzed self-reported data on HRQoL in CPM to prevent a potential bias which may have occurred if parents with mental health problems report on HRQoL of their offspring. Future studies may wish to investigate predictors of parent-reported HRQoL and the agreement between self- and parent-reported data on HRQoL in CPM.
Conclusions
CPM in the general population may exhibit reduced HRQoL compared to Non-CPM. Especially female CPM show an increased risk of impaired HRQoL in the domain autonomy & parent relation. Early assessment with regard to reduced HRQoL, especially in risk groups, is needed in order to help these children and adolescents as soon as possible. Consequently, tailored support and prevention programs not only for CPM in clinical populations but moreover in the general population are needed that focus not only on mental health problems but also on HRQoL especially of female CPM; corresponding programs are currently developed and progressively implemented in mental care services [50, 51]. Our findings that self-efficacy, social support and family climate may serve as significant resources for HRQoL in CPM, can facilitate the development of adapted support and prevention programs for this risk group.
References
Plass-Christl, A., Haller, A. C., Otto, C., Barkmann, C., Wiegand-Grefe, S., Holling, H., et al. (2017). Parents with mental health problems and their children in a German population based sample: Results of the BELLA study. PLoS ONE. https://doi.org/10.1371/journal.pone.0180410.
Goodman, S. H., Rouse, M. H., Connell, A. M., Broth, M. R., Hall, C. M., & Heyward, D. (2011). Maternal depression and child psychopathology: A meta-analytic review. Clinical Child and Family Psychology Review, 14(1), 1–27. https://doi.org/10.1007/s10567-010-0080-1.
van Santvoort, F., Hosman, C. M. H., Janssens, J., van Doesum, K. T. M., Reupert, A., & van Loon, L. M. A. (2015). The impact of various parental mental disorders on children’s diagnoses: A systematic review. Clinical Child and Family Psychology Review, 18(4), 281–299. https://doi.org/10.1007/s10567-015-0191-9.
Hagen, K. A., Hilsen, M., Kallander, E. K., & Ruud, T. (2019). Health-related quality of life (HRQoL) in children of ill or substance abusing parents: Examining factor structure and sub-group differences. Quality of Life Research, 28(4), 1063–1073. https://doi.org/10.1007/s11136-018-2067-1.
Oltean, I. I., & Ferro, M. A. (2019). Agreement of child and parent-proxy reported health-related quality of life in children with mental disorder. Quality of Life Research, 28(3), 703–712. https://doi.org/10.1007/s11136-018-2026-x.
Ravens-Sieberer, U., Erhart, M., Wille, N., Wetzel, R., Nickel, J., & Bullinger, M. (2006). Generic health-related quality-of-life assessment in children and adolescents: Methodological considerations. Pharmacoeconomics, 24(12), 1199–1220.
Ellert, U., Ravens-Sieberer, U., Erhart, M., & Kurth, B. M. (2011). Determinants of agreement between self-reported and parent-assessed quality of life for children in Germany-results of the German Health Interview and Examination Survey for Children and Adolescents (KiGGS). Health and Quality of Life Outcomes, 9, 102. https://doi.org/10.1186/1477-7525-9-102.
Ellert, U., Brettschneider, A. K., & Ravens-Sieberer, U. (2014). Health-related quality of life in children and adolescents in Germany. Results of the KiGGS study: first follow-up (KiGGS Wave 1). Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz, 57(7), 798–806. https://doi.org/10.1007/s00103-014-1978-4.
Baumgarten, F., Cohrdes, C., Schienkiewitz, A., Thamm, R., Meyrose, A. K., & Ravens-Sieberer, U. (2019). Health-related quality of life and its relation to chronic diseases and mental health problems among children and adolescents. Results from KiGGS Wave 2. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz, 62(10), 1205–1214. https://doi.org/10.1007/s00103-019-03006-9.
Giannakopoulos, G., Dimitrakaki, C., Pedeli, X., Kolaitis, G., Rotsika, V., Ravens-Sieberer, U., et al. (2009). Adolescents’ wellbeing and functioning: Relationships with parents’ subjective general physical and mental health. Health and Quality of Life Outcomes, 7, 100. https://doi.org/10.1186/1477-7525-7-100.
Barkmann, C., Petermann, F., Schlack, R., Bullinger, M., Schulte-Markwort, M., Klasen, F., et al. (2016). Course of health-related quality of life: Results of the BELLA Cohort Study. Kindheit und Entwicklung, 25(1), 50–59. https://doi.org/10.1026/0942-5403/a000188.
Otto, C., Haller, A. C., Klasen, F., Holing, H., Bullinger, M., Ravens-Sieberer, U., et al. (2017). Risk and protective factors of health-related quality of life in children and adolescents: Results of the longitudinal BELLA study. PLoS ONE. https://doi.org/10.1371/journal.pone.0190363.
Dey, M., Landolt, M. A., & Mohler-Kuo, M. (2012). Health-related quality of life among children with mental disorders: a systematic review. Quality Life Research. https://doi.org/10.1007/s11136-012-0109-7.
Jonsson, U., Alaie, I., Wilteus, A. L., Zander, E., Marschik, P. B., Coghill, D., et al. (2017). Annual research review: Quality of life and childhood mental and behavioural disorders—A critical review of the research. Journal of Child Psychology and Psychiatry, 58(4), 439–469. https://doi.org/10.1111/jcpp.12645.
Wiegand-Grefe, S., Halverscheid, S., Petermann, F., & Plass, A. (2011). Psychopathology and quality of life in children of mentally ill parents. In L. L’Abate (Ed.), Mental illness. Evaluation, treatments and implications (pp. 21–34). Rijeka: Intech.
Wiegand-Grefe, S., Jeske, J., Bullinger, M., Plass, A., & Petermann, F. (2010). Lebensqualität von Kindern psychisch kranker Eltern Zusammenhänge zwischen Merkmalen elterlicher Erkrankung und gesundheitsbezogener Lebensqualität der Kinder aus Elternsicht. Zeitschrift für Psychiatrie, Psychologie, und Psychotherapie, 58(4), 315–322.
Dittrich, K., Fuchs, A., Bermpohl, F., Meyer, J., Fuhrer, D., Reichl, C., et al. (2018). Effects of maternal history of depression and early life maltreatment on children’s health-related quality of life. Journal of Affective Disorders, 225, 280–288. https://doi.org/10.1016/j.jad.2017.08.053.
Kallander, E. K., Weimand, B. M., Hanssen-Bauer, K., Van Roy, B., & Ruud, T. (2020). Factors associated with quality of life for children affected by parental illness or substance abuse. Scandinavian Journal of Caring Sciences. https://doi.org/10.1111/scs.12868.
Plass, A., Haller, A. C., Habermann, K., Barkmann, C., Petermann, F., Schipper, M., et al. (2016). Factors promoting mental health in children of parents with mental health problems: Results of the BELLA Cohort study. Kindheit und Entwicklung, 25(1), 41–49. https://doi.org/10.1026/0942-5403/a000187.
Kurth, B. M., Kamtsiuris, P., Holling, H., Schlaud, M., Dolle, R., Ellert, U., et al. (2008). The challenge of comprehensively mapping children’s health in a nation-wide health survey: Design of the German KiGGS-Study. BMC Public Health, 8(1), 196.
Ravens-Sieberer, U., Otto, C., Kriston, L., Rothenberger, A., Dopfner, M., Herpertz-Dahlmann, B., et al. (2015). The longitudinal BELLA study: Design, methods and first results on the course of mental health problems. European Child & Adolescent Psychiatry, 24(6), 651–663. https://doi.org/10.1007/s00787-014-0638-4.
Klaghofer, R., & Brahler, E. (2001). Construction and statistical testing of a short version of the SCL-90-R. Zeitschrift für Klinische Psychologie Psychiatrie und Psychotherapie, 49(2), 115–124.
Derogatis, L. R., Lipman, E. L., Rickels, K., Uhlenhut, E., & Covi, L. (1974). The Hopkins Symptom Checklist (HSCL): A self-report symptom inventory. Behavioral Science, 19, 1–15.
Petrowski, K., Schmalbach, B., Kliem, S., Hinz, A., & Brahler, E. (2019). Symptom-Checklist-K-9: Norm values and factorial structure in a representative German sample. PLoS ONE. https://doi.org/10.1371/journal.pone.0213490.
Wustner, A., Otto, C., Schlack, R., Holling, H., Klasen, F., & Ravens-Sieberer, U. (2019). Risk and protective factors for the development of ADHD symptoms in children and adolescents: Results of the longitudinal BELLA study. PLoS ONE. https://doi.org/10.1371/journal.pone.0214412.
Plass-Christl, A., Otto, C., Klasen, F., Wiegand-Grefe, S., Barkmann, C., Holling, H., et al. (2018). Trajectories of mental health problems in children of parents with mental health problems: Results of the BELLA study. European Child & Adolescent Psychiatry, 27(7), 867–876. https://doi.org/10.1007/s00787-017-1084-x.
Plass-Christl, A., Klasen, F., Otto, C., Barkmann, C., Hölling, H., Klein, T., et al. (2017). Mental health care use in children of parents with mental health problems. Journal of Child Psychiatry and Human Development. https://doi.org/10.1007/s10578-017-0721-4.
Klasen, F., Otto, C., Kriston, L., Patalay, P., Schlack, R., Ravens-Sieberer, U., et al. (2015). Risk and protective factors for the development of depressive symptoms in children and adolescents: Results of the longitudinal BELLA study. European Child & Adolescent Psychiatry, 24(6), 695–703. https://doi.org/10.1007/s00787-014-0637-5.
Franke, G. H. (2002). SCL-90-R: Symptom-Checkliste von L.R. Derogatis—deutsche Version. Göttingen: Beltz Test GmbH.
Ravens-Sieberer, U., & the European KIDSCREEN Group. (2006). The KIDSCREEN Questionnaires—Quality of life questionnaires for children and adolescents—Handbook. Lengerich: Pabst Science Publishers.
Ravens-Sieberer, U., Auquier, P., Erhart, M., Gosch, A., Rajmil, L., Bruil, J., et al. (2007). The KIDSCREEN-27 quality of life measure for children and adolescents: Psychometric results from a cross-cultural survey in 13 European countries. Quality of Life Research, 16(8), 1347–1356. https://doi.org/10.1007/s11136-007-9240-2.
Goodman, R. (1997). The strengths and difficulties questionnaire: A research note. Journal of Child Psychology and Psychiatry, 38(5), 581–586.
Goodman, A., Lamping, D. L., & Ploubidis, G. B. (2010). When to use broader internalising and externalising subscales instead of the hypothesised five subscales on the Strengths and Difficulties Questionnaire (SDQ): Data from British parents, teachers and children. Journal of Abnormal Child Psychology, 38(8), 1179–1191.
Schwarzer, R., & Jerusalem, M. (1995). Generalized Self-Efficacy scale. In J. Weinman, S. Wright, & M. Johnston (Eds.), Measures in health psychology: A user’s portfolio. Causal and control beliefs (pp. 35–37). Windsor: NFER-NELSON.
Schneewind, K., Beckmann, M., & Hecht-Jackl, A. (1985). Familienklima-Skalen. Bericht 8.1 und 8.2. München: Ludwig Maximilians Universität, Institut für Psychologie- Persönlichkeitspsychologie und Psychodiagnostik.
Donald, C. A., & Ware, J. E. (1984). The measurement of social support. Research in Community & Mental Health, 4, 325–370.
Winkler, J., & Stolzenberg, H. (1999). Der Sozialschichtindex im Bundes-Gesundheitssurvey. Gesundheitswesen, 61, S178–S183.
Lange, M., Kamtsiuris, P., Lange, C., Schaffrath Rosario, A., Stolzenberg, H., & Lampert, T. (2007). Messung soziodemographischer Merkmale im Kinder- und Jugendgesundheitssurvey (KiGGS) und ihre Bedeutung am Beispiel der Einschätzung des allgemeinen Gesundheitszustands. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz, 50(5–6), 578–589.
Schenk, L., Bau, A. M., Borde, T., Butler, J., Lampert, T., Neuhauser, H., et al. (2006). Mindestindikatorensatz zur Erfassung des Migrationsstatus. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz, 49(9), 853–860.
Heck, R., Thomas, S., & Tabata, L. (2014). Multilevel and longitudinal modeling with IBM SPSS. New York: Routledge.
McFadden, D. (1974). Conditional logit analysis of qualitative choice behaviour. In P. Zarembka (Ed.), Frontiers in econometrics (pp. 105–142). New York: Academic Press.
Clemens, V., Berthold, O., Witt, A., Sachser, C., Brahler, E., Plener, P. L., et al. (2020). Lifespan risks of growing up in a family with mental illness or substance abuse. Scientific Reports. https://doi.org/10.1038/s41598-020-72064-w.
Ranoyen, I., Klockner, C., Wallander, J., & Jozefiak, T. (2015). Associations between internalizing problems in adolescent daughters versus sons and mental health problems in mothers versus fathers (the HUNT study). Journal of Child and Family Studies, 24(7), 2008–2020. https://doi.org/10.1007/s10826-014-0001-x.
Bastiaansen, D., Ferdinand, R. F., & Koot, H. M. (2020). Predictors of quality of life in children and adolescents with psychiatric disorders. Child Psychiatry & Human Development, 51(1), 104–113. https://doi.org/10.1007/s10578-019-00914-4.
Jozefiak, T., Greger, H. K., Koot, H. M., Klockner, C. A., & Wallander, J. L. (2019). The role of family functioning and self-esteem in the quality of life of adolescents referred for psychiatric services: A 3-year follow-up. Quality of Life Research, 28(9), 2443–2452. https://doi.org/10.1007/s11136-019-02197-7.
Ramchandani, P. G., Psychogiou, L., Vlachos, H., Iles, J., Sethna, V., Netsi, E., et al. (2011). Paternal depression: An examination of its links with father, child and family functioning in the postnatal period. Depression and Anxiety, 28(6), 471–477. https://doi.org/10.1002/da.20814.
Ramchandani, P., & Psychogiou, L. (2009). Paternal psychiatric disorders and children’s psychosocial development. Lancet, 374(9690), 646–653. https://doi.org/10.1016/s0140-6736(09)60238-5.
Katschnig, H. (2006). Quality of life in mental disorders: Challenges for research and clinical practice. World Psychiatry, 5(3), 139–145.
McLaughlin, K. A., Gadermann, A. M., Hwang, I., Sampson, N. A., Al-Hamzawi, A., Andrade, L. H., et al. (2012). Parent psychopathology and offspring mental disorders: Results from the WHO World Mental Health Surveys. British Journal of Psychiatry, 200(4), 290–299. https://doi.org/10.1192/bjp.bp.111.101253.
Brent, D., Brunwasser, S. M., Hollon, S. D., Weersing, V. R., Clarke, G. N., Dickerson, J. F., et al. (2015). Effect of a cognitive-behavioral prevention program on depression 6 years after implementation among at-risk adolescents: A randomized clinical trial. JAMA Psychiatry. https://doi.org/10.1001/jamapsychiatry.2015.1559.
Wiegand-Grefe, S., Alberts, J., Petermann, F., & Plass, A. (2016). Differential perspectives on family functioning and interfamilial relationships: The effect of a manualized intervention program on children of mentally ill parents. Kindheit und Entwicklung, 25(2), 77–88. https://doi.org/10.1026/0942-5403/a000192.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Plass-Christl, A., Ravens-Sieberer, U., Hölling, H. et al. Trajectories of health-related quality of life in children of parents with mental health problems: results of the BELLA study. Qual Life Res 30, 1841–1852 (2021). https://doi.org/10.1007/s11136-021-02783-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-021-02783-8