
Abstract
Background
Short-type double-balloon endoscope (DBE)-assisted endoscopic retrograde cholangiopancreatography (ERCP) has been developed as an alternative approach for cases with a surgically altered gastrointestinal anatomy. However, this technique is sometimes technically challenging and carries a risk of severe adverse events.
Aims
To evaluate the factors affecting the technical success rate and adverse events of DBE-ERCP.
Methods
A total of 319 patients (805 procedures) with a surgically altered gastrointestinal anatomy underwent short DBE-ERCP. The factors affecting the technical success rate and adverse events, and the learning curve of the trainees were retrospectively evaluated.
Results
The technical success rate of all procedures was 90.7%. Adverse events occurred in 44 (5.5%) procedures. A multivariate analysis indicated that Roux-en-Y reconstruction and first-time short DBE-ERCP were factors affecting the technical failure and adverse event rates, while the modified Child method after subtotal stomach-preserving pancreaticoduodenectomy reconstruction was a non-risk factor for adverse events. The trainee caseload did not affect the technical success or adverse event rates significantly; however, trainees tended to perform cases involving the modified Child method after subtotal stomach-preserving pancreaticoduodenectomy reconstruction. The success rate of scope insertion increased according to experience; however, the overall success rate did not differ to a statistically significant extent.
Conclusion
Short DBE-ERCP was useful and safe for managing cases with a surgically altered anatomy; however, trainees should concentrate on accumulating experience with easy cases, such as those with the modified Child method after subtotal stomach-preserving pancreaticoduodenectomy reconstruction or a history of DBE-ERCP.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Endoscopic retrograde cholangiopancreatography (ERCP) is a crucial technique for diagnosing or treating pancreaticobiliary diseases; however, it is sometimes difficult to perform, especially in patients with a surgically altered gastrointestinal anatomy [1]. Such patients can have a long intestinal distance to their papillae or anastomoses and may thus require a long endoscope. The double-balloon endoscope (DBE) was initially developed to evaluate small intestinal diseases and has since been applied to cases of ERCP for patients with an altered gastrointestinal anatomy [2,3,4,5,6].
Short-type DBE-assisted ERCP (DBE-ERCP) has been developed as an innovative technique for these patients [5, 7]. However, some cases are still difficult to manage and experience technical failure of DBE-ERCP, occasionally resulting in adverse events. Shimatani et al. [5] reported an adverse event rate of 10.6%, and Billroth II (B-II) reconstruction and cases with papillae were found to be significant risk factors. Severe adverse events include perforation requiring surgical treatment.
The interventional endoscopic ultrasound (IV-EUS) technique has recently been developed, and the efficacy of this approach for cases of altered gastrointestinal anatomy has been reported [8]. However, this technique is still being developed, and appropriate guidelines concerning the use of different techniques in different situations are needed. While DBE-ERCP may be positioned as the core technique for patients with an altered anatomy, further evaluations and the establishment of a training program are needed.
In this study, we retrospectively evaluated a large case series of DBE-ERCP and considered the factors associated with technical success and adverse events.
Methods
Patients
A total of 319 patients (805 procedures) with a surgically altered gastrointestinal anatomy who underwent DBE-ERCP from November 2011 to August 2018 at Okayama University Hospital were retrospectively evaluated. Sixty-two patients were included in the previous multicenter prospective study in Japan [5].
Instruments and DBE-ERCP Procedure
Short-type DBEs (EC-450BI5, EI-530B, and EI-580BT; Fujifilm, Tokyo, Japan) were used. Procedures were performed under conscious sedation with midazolam or propofol, in combination with pentazocine. DBE-ERCP was performed by endoscopists who had completed standard colonoscopy training and experienced at least 100 ERCP procedures. ERCP trainees were supervised by expert ERCP endoscopists who had experienced at least 500 ERCP procedures. Trainees gave way to their supervisors at the experts’ discretion. All procedures were performed with carbon dioxide (CO2) insufflation. Informed consent for DBE-ERCP was obtained from all patients.
In cases of choledochojejunal anastomosis (CJA), biliary or pancreatic stenosis requiring stent placement, periodic stent replacement is scheduled every 3 months until stenosis improves. If stones are combined with stenoses, stone removal is also performed.
In cases of failure to reach the papillae or anastomoses due to difficult scope insertion, procedures are attempted again after a few days.
Definitions and Outcome Measurement
The primary outcome was the factors associated with technical failure. The secondary outcomes were the factors associated with adverse events and the learning curve of the trainees. Technical success was defined as successful therapeutic interventions (plastic stent placement for stenosis, complete stone removal for bile duct stone, specimen sampling for diagnostic ERCP). Cases of stenoses combined with stones were categorized into the “stenoses” group. We collected data on the patient characteristics as well as the reconstruction methods, indication for DBE-ERCP, and physicians’ experience. Physicians’ experience was classified into three categories: novice (100–200 conventional ERCP procedures experienced), intermediate (201–500 conventional ERCP procedures experienced), and expert (> 500 conventional ERCP procedures and > 20 DBE-ERCP procedures experienced). Experience in other institutions was also included. Physicians who met the definitions of novice or intermediate were classified as trainees. The procedure results of trainees who were trained on a continuous basis over a 2-year period were evaluated over time.
This study was approved by the institutional review board of Okayama University Hospital and registered in the UMIN protocol registration system (identification number UMIN000036199).
Statistical Analyses
Statistical analyses were performed using the JMP Pro 14.0 software program (SAS institute, Japan). The categorical data were evaluated with the Chi-square test. P values < 0.05 were considered statistically significant. A multivariate logistic regression analysis was performed to analyze the associations between items that were associated with the prevalence according to a univariate analysis; P < 0.05) and the technical success and adverse events.
Results
The patients’ characteristics are shown in Table 1. A total of 319 patients (805 procedures) underwent DBE-ERCP during the study period. Surgical reconstruction was performed by the modified Child method after subtotal stomach-preserving pancreaticoduodenectomy (SSPPD) in 133 patients (312 procedures), modified Child method after pylorus-preserving pancreaticoduodenectomy (PpPD) in 29 patients (60 procedures), Roux-en-Y (R-Y) with CJA in 116 patients (361 procedures), R-Y without CJA in 19 patients (29 procedures), and Billroth II (B-II) gastrectomy in 22 patients (43 procedures). Indications for DBE-ERCP were as follows: CJA stenoses in 173 patients, bile duct stones in 58 patients, biliary stricture in 57 patients, pancreatic indications in 30 patients, and other (assessment of gallbladder tumor) in 1 patient.
The success rate of reaching the papillae or anastomoses among all procedures was 94.3% (759 procedures), and the overall technical success rate was 90.7% (730 procedures). The first-time DBE-ERCP rate was 39.6%. Seventy-five cases failed their procedures. There were 36 cases in which the papillae or anastomoses could not be reached, including 2 patients who required surgical treatment because of intestinal perforation. DBE-ERCP was reattempted in 16 cases, and retrials succeeded in 12. Thirty-two cases required percutaneous drainage because of stent placement failure. Six cases underwent EUS-guided drainage (four cases of biliary drainage and two cases of pancreatic drainage). Nineteen cases were managed conservatively, and all of them fortunately improved.
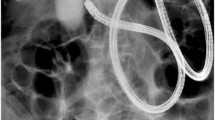
Adverse events occurred in 44 cases (5.5%), including mild cholangitis in 20, pancreatitis in 14, intestinal perforation in 6, and others (2 biliary leakage, 1 pancreatic leakage caused by guidewires, and 1 pneumothorax) in 4. These results are listed by surgical reconstruction procedure in Table 2. There were three adverse events that required further invasive intervention, including two cases with surgical treatment for intestinal perforation and one requiring percutaneous drainage for pancreatic leakage caused by a guidewire. Other adverse events improved with conservative treatment. One of the cases of surgical treatment for intestinal perforation is shown in Fig. 1, and one of the cases without surgical treatment for intestinal perforation is shown in Fig. 2.

This is a case of intestinal perforation during scope insertion. The patient was a 71-year-old man whose intestinal tract had been reconstructed with B-II reconstruction. He was scheduled to undergo DBE-ERCP for the assessment of a pancreatic head tumor by an expert physician. However, scope insertion was difficult because of adhesion, and perforation occurred during stretching of the scope (a–c). Retroperitoneal emphysema was detected under radiographic guidance (b and d, red arrows), and intraperitoneal emphysema was also detected on CT (d, yellow arrow). He underwent emergent pancreaticoduodenectomy for pancreatic head tumor and intestinal perforation

This is a case of micro-intestinal perforation during biliary cannulation. The patient was an 83-year-old woman whose intestinal tract had been reconstructed with R-Y reconstruction without CJA. She underwent DBE-ERCP for the treatment of a CBD stone by a novice physician; however, approaching the bile duct through the papilla was difficult (a). During the cannulation approach, retroperitoneal emphysema was detected under radiographic guidance (b, red arrows). While the location of the perforation could not be detected, pernasal drainage tubes were deployed for decompression of the intestinal tract (c). On CT, retroperitoneal emphysema was detected around the right kidney (d, yellow arrows). Fortunately, she improved without surgical treatment
The factors affecting the technical failure rate were evaluated, and the results of the univariate analysis are shown in Table 3. Choledochojejunal anastomotic stenosis indication and SSPPD reconstruction were significant factors influencing a “successful” procedure. In contrast, pancreatic indication, R-Y reconstruction, first-time DBE-ERCP, and naïve papillae were significant risk factors for technical failure. In the multivariate analysis, pancreatic indication, R-Y reconstruction, and first-time DBE-ERCP remained significant risk factors for technical failure (Table 4).
The risk factors for adverse events according to the univariate analysis are shown in Table 5. Reconstruction with papillae (PpPD, R-Y without CJA, and B-II), first-time DBE-ERCP, naïve papillae, and pancreatic indication were risk factors for pancreatitis. Novice experience, first-time DBE-ERCP, and naïve papillae were risk factors for intestinal perforation. B-II reconstruction and naïve papillae were risk factors for other adverse events. In total, bile duct stone indication, B-II reconstruction, first-time DBE-ERCP, and naïve papillae were risk factors for adverse events. The multivariate analysis indicated first-time DBE-ERCP to be the only significant factor influencing adverse events. In addition, SSPPD reconstruction was the only significant factor affecting the procedure safety (Table 6).
The results of procedures performed by trainees (novice and intermediate) are shown in Table 7. The success rate of reaching the papillae or anastomoses was lower in cases of R-Y reconstructions, and 22.7% of procedures required expert assistance. There were seven cases of adverse events, including three cholangitis, two pancreatitis, and two perforations. Most cases improved with conservative treatment, but one patient with perforation required surgical reintervention. In addition, the comparison of trainees and experts (Table 8) showed that while the technical success rate, procedure time, and adverse event rate did not differ markedly between the two, there was a significant difference in the success rate without switching to a senior physician and the breakdown of the reconstruction methods. The rate of switching to a senior physician was significantly higher among trainees. Additionally, patients with SSPPD reconstruction tended to undergo DBE-ERCP by trainees, whereas those with R-Y reconstruction tended to undergo DBE-ERCP by experts.
There were twelve novices, eleven intermediates, and 12 experts (there were some redundant physicians). Nine trainees were trained on a continuous basis over a 2-year period. All of them were promoted to “experts” during the study period. Their DBE-ERCP procedures were evaluated over time (Table 9). The rate of reaching the papillae or anastomoses, and the overall success rate did not differ between the first and second periods. However, the rate of switching to a senior physician during scope insertion decreased significantly (P = 0.0121), and the overall technical success rates of procedures performed without the help from a senior physician increased significantly (P = 0.04). The success rates of scope insertions and overall procedures, according to the physicians’ DBE-ERCP experience, are shown in Fig. 3. The success rate of scope insertion increased according to DBE-ERCP experience; however, the overall success rate did not differ to a statistically significant extent.

This graph shows the success rate of trainees who performed DBE-ERCP procedures over a 2-year period “without a senior’s help”
Discussion
The endoscopic diagnosis and treatment of pancreaticobiliary diseases for patients with surgically altered anatomy are difficult because of the variety of intestinal features [9, 10]. The DBE was initially developed for the diagnosis and treatment of small bowel diseases [6], but it has since been applied to ERCP for patients with an altered gastrointestinal anatomy, showing widely recognized utility [3, 11].
A short-type DBE dedicated to ERCP that is compatible with many ERCP devices has recently been developed. This new endoscope has yielded a breakthrough in performing the ERCP procedures for patients with an altered gastrointestinal anatomy [4, 5, 12]. However, this approach is still being developed, and some issues remain to be addressed, such as the establishment of an educational system for trainees.
ERCP is an essential procedure for pancreaticobiliary diseases, but it is difficult to achieve a safe and successful procedure, and severe adverse events may occur. As such, a training program must be carefully and considerately developed. The QUASIE cohort found that the trainee caseload affected the technical success of ERCP but not the complication rate under observation by experts [13]. Frost et al. [14] also reported that the presence of a trainee did not impair the success rate of biliary cannulation.
However, the DBE-ERCP procedure differs somewhat from the standard ERCP procedure. DBE-ERCP requires not only an ERCP technique but also an endoscope insertion technique, such as that for colonoscopy. Kashani et al. [15] reported that the success rate and adverse event rate of DBE-ERCP performed by novices were not markedly different from those performed by experts. However, that study was relatively small, and a further evaluation is needed. Yane et al. [16] reported the factors influencing procedural failure of short-type single-balloon enteroscope (SBE)-assisted ERCP. That study found that pancreatic indication, first ERCP attempt, and no transparent hood were potential factors affecting the procedural failure of SBE-ERCP.
We assessed 805 DBE-ERCP procedures performed in 319 patients at our hospital and considered a number of potentially influential factors, including physicians’ experience, that might affect the technical success and adverse event rate.
Technical success is associated with various factors. Reaching the papillae or anastomoses is the first difficulty of DBE-ERCP. In the present study, the success rate of reaching the papillae or anastomoses was 94.3%, and the success rate of R-Y reconstruction was lower than with other procedures (Table 2). This was an expected result given the anatomy of R-Y reconstruction, in which the distance to the anastomosis or papillae is quite long [17]. Furthermore, R-Y without CJA reconstruction makes the procedure particularly difficult because it requires approaching through the papillae. This difficulty also affected the overall technical success rate of DBE-ERCP. R-Y reconstruction was found to be a significant factor affecting technical failure in both univariate and multivariate analyses (Tables 3, 4). There were no significant differences in the technical success rate according to physicians’ experience, as all procedures were performed under the supervision of experts. Regarding the prevalence of assistance requirement, 22.7% of procedures by trainees (novices and intermediates) required experts’ assistance, and 75% of these (24 cases) were during DBE insertion (Table 7). Scope insertion is the first hurdle facing a successful procedure, and we employ various techniques for facilitating insertion, such as scope insertion to the sharp-angled afferent limb in cases with SSPPD reconstruction and selecting the lumen in which the distal end of the scope progresses toward the patient’s liver or head in R-Y anastomosis sites [18, 19].
The adverse event rate among novices was also similar to that in intermediate trainees and experts; however, the intestinal perforation rate tended to be higher in procedures performed by novices than by those with more experience (Table 5). Perforation is a severe—sometimes fatal—adverse event. Indeed, two of six patients with intestinal perforation in this study required surgical reintervention. One of them was a patient in whom DBE-ERCP with B-II reconstruction was performed by an expert physician to assess a pancreatic tumor, and the other was a patient in whom DBE-ERCP with SSPPD reconstruction was performed by an intermediate-experience physician to treat choledochojejunal anastomotic stenosis (Fig. 1). Both incidents occurred during DBE insertion. In addition, physicians’ experience related to the rate of perforation (Table 5). The patient who developed perforation after being managed by a novice had common bile duct stones. Her intestinal tract was reconstructed with R-Y without CJA, and she had a naïve papilla. During a cannulation attempt, retroperitoneal free air was detected under radiographic guidance. Fortunately, she improved with fasting and antibiotic treatment (Fig. 2). Naïve papilla was found to be a strong risk factor for adverse events, such as pancreatitis and perforation. It is associated with a first-time DBE-ERCP attempt, which was also a significant factor affecting the technical success and adverse event rates. In contrast, SSPPD reconstruction was found to be safer than other reconstruction methods (Table 6). Several techniques facilitating DBE-ERCP for SSPPD reconstruction have been developed, such as scope insertion to the sharp-angled afferent limb and handling of various accessories [19]. These procedures can be performed more safely by mastering these techniques.
We evaluated whether or not physicians’ experience affected the results in detail. As shown in Tables 7 and 8, there were no significant differences in the technical success or adverse event rate between trainees and experts. However, this result might have been influenced by trainees being supervised by experts appropriately. Furthermore, patients with SSPPD reconstruction tended to be managed by trainees, whereas those with R-Y reconstruction tended to be managed by experts. This trend is a matter of course, as R-Y reconstruction is more difficult than SSPPD reconstruction; cases with SSPPD reconstruction are considered suitable for trainees to gain experience, given the associated high success rate and low risk of adverse events. Additionally, we evaluated the learning curve of trainees according to their experience in performing conventional ERCP and DBE-ERCP (Tables 8, 9 and Fig. 3). In fact, the success rate of scope insertion increased according to experience, while the overall success rate did not differ between the first and the second periods. This result might have been due to a selection bias—in fact, experts tended to work on difficult cases, as previously indicated. The success rates without switching to a senior physician were significantly higher in experts who had experienced > 20 DBE-ERCP procedures. This result indicates that the experience of > 20 DBE-ERCP can be a measure of the learning level. However, it is difficult to evaluate appropriately, because DBE-ERCP procedures have a wide range of difficulties. Thus, the present study is still associated with limitations in relation to its retrospective design and the relatively small number of procedures that were assessed. Further prospective studies should be conducted to construct a training system for DBE-ERCP.
In summary, R-Y reconstruction and first-time DBE-ERCP were factors associated with an increased procedure difficulty and first-time DBE-ERCP was also the risk factor for adverse events. While physician experience was not a significant factor influencing the technical success or adverse event rate under supervision by experts, trainees should concentrate on accumulating experience with safe cases, such as those with SSPPD reconstruction or a history of DBE-ERCP.
References
Wright BE, Cass OW, Freeman ML. ERCP in patients with long-limb Roux-en-Y gastrojejunostomy and intact papilla. Gastrointest Endosc. 2002;56:225–232.
Yamamoto H, Sekine Y, Sato Y, et al. Total enteroscopy with a nonsurgical steerable double-balloon method. Gastrointest Endosc. 2001;53:216–220.
Monkemuller K, Bellutti M, Neumann H, et al. Therapeutic ERCP with the double-balloon enteroscope in patients with Roux-en-Y anastomosis. Gastrointest Endosc. 2008;67:992–996.
Shimatani M, Matsushita M, Takaoka M, et al. “Short” double balloon enteroscope for endoscopic retrograde cholangiopancreatography with conventional sphincterotomy and metallic stent placement after Billroth II gastrectomy. Endoscopy. 2009;41:E19–E20.
Shimatani M, Hatanaka H, Kogure H, et al. Diagnostic and therapeutic endoscopic retrograde cholangiography using a short-type double-balloon endoscope in patients with altered gastrointestinal anatomy: a multicenter prospective study in Japan. Am J Gastroenterol. 2016;111:1750–1758.
May A, Nachbar L, Ell C. Double-balloon enteroscopy (push-and-pull enteroscopy) of the small bowel: feasibility and diagnostic and therapeutic yield in patients with suspected small bowel disease. Gastrointest Endosc. 2005;62:62–70.
Shimatani M, Matsushita M, Takaoka M, et al. Effective “short” double-balloon enteroscope for diagnostic and therapeutic ERCP in patients with altered gastrointestinal anatomy: a large case series. Endoscopy. 2009;41:849–854.
Khashab MA, El Zein MH, Sharzehi K, et al. EUS-guided biliary drainage or enteroscopy-assisted ERCP in patients with surgical anatomy and biliary obstruction: an international comparative study. Endosc Int Open. 2016;4:E1322–E1327.
Elton E, Hanson BL, Qaseem T, et al. Diagnostic and therapeutic ERCP using an enteroscope and a pediatric colonoscope in long-limb surgical bypass patients. Gastrointest Endosc. 1998;47:62–67.
Hintze RE, Adler A, Veltzke W, et al. Endoscopic access to the papilla of Vater for endoscopic retrograde cholangiopancreatography in patients with billroth II or Roux-en-Y gastrojejunostomy. Endoscopy. 1997;29:69–73.
Aabakken L, Bretthauer M, Line PD. Double-balloon enteroscopy for endoscopic retrograde cholangiography in patients with a Roux-en-Y anastomosis. Endoscopy. 2007;39:1068–1071.
Itoi T, Ishii K, Sofuni A, et al. Long- and short-type double-balloon enteroscopy-assisted therapeutic ERCP for intact papilla in patients with a Roux-en-Y anastomosis. Surg Endosc. 2011;25:713–721.
Voiosu T, Bengus A, Voiosu A, et al. Trainee caseload correlates with ERCP success rates but not with procedure-related complications: results from a prospective study (the QUASIE cohort). Endosc Int Open. 2016;4:E409–E414.
Frost JW, Kurup A, Shetty S, et al. Does the presence of a trainee compromise success of biliary cannulation at ERCP? Endosc Int Open. 2017;5:E559–E562.
Kashani A, Abboud G, Lo SK, et al. Double balloon enteroscopy-assisted endoscopic retrograde cholangiopancreatography in Roux-en-Y gastric bypass anatomy: expert vs. novice experience. Endosc Int Open. 2018;6:E885–E891.
Yane K, Katanuma A, Maguchi H, et al. Short-type single-balloon enteroscope-assisted ERCP in postsurgical altered anatomy: potential factors affecting procedural failure. Endoscopy. 2017;49:69–74.
Tomoda T, Tsutsumi K, Okada H. Comparison between Roux-en-Y patients with and without gastrectomy during endoscopic retrograde cholangiopancreatography using a short double-balloon enteroscope. Dig Endosc. 2015;27:775.
Tsutsumi K, Kato H, Hirao K, et al. Comparison of two fluoroscopic images to ensure efficient scope insertion for biliary intervention in patients with Roux-en-Y hepaticojejunostomy. Endoscopy. 2017;49:1256–1261.
Tsutsumi K, Kato H, Muro S, et al. ERCP using a short double-balloon enteroscope in patients with prior pancreatoduodenectomy: higher maneuverability supplied by the efferent-limb route. Surg Endosc. 2015;29:1944–1951.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interests for this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Uchida, D., Tsutsumi, K., Kato, H. et al. Potential Factors Affecting Results of Short-Type Double-Balloon Endoscope-Assisted Endoscopic Retrograde Cholangiopancreatography. Dig Dis Sci 65, 1460–1470 (2020). https://doi.org/10.1007/s10620-019-05857-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-019-05857-3