
Abstract
Background
In endoscopic retrograde cholangiopancreatography (ERCP) for patients who have undergone a pancreatoduodenectomy (PD) with a Braun anastomosis, two different approaches are available: the afferent-limb route and the efferent-limb route. This study was to clarify the usefulness of a short double-balloon enteroscope (DBE) in ERCP for prior-PD patients, and to reveal which route was optimal for ERCP.
Methods
Seventy-two consecutive patients with a prior PD underwent diagnostic or therapeutic ERCP using the DBE. This retrospective study evaluated the outcome of the ERCP and assessed the shape of the DBE by fluoroscopic imaging to compare the maneuverability of the two routes.
Results
In 71 patients (99 %) the bilioenteric anastomosis was reached and cholangiography was performed. Treatment was required in 59 patients (83 %) and was performed successfully in all. Complications occurred in two patients (3 %) with cholangitis. In three patients, the afferent-limb route had to be changed to the efferent-limb route in the procedure. A gentler arc-shaped angulation of the DBE was induced using the efferent-limb route compared to the afferent-limb route (128° (n = 42) vs. 113° (n = 15); p = 0.037), and that was also revealed in 11 patients (15 %) who underwent repeated ERCP by each route (123° vs. 96°; p = 0.003).
Conclusions
The short DBE facilitates ERCP in prior-PD patients. Particularly, ERCP using the efferent-limb route can achieve a maneuverable procedure without unnecessary stress, such as scope insertion to the sharp-angled afferent limb and the handling of various accessories through the narrow scope channel with a sense of resistance.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Pancreatoduodenectomy (PD) is a standard operation performed for patients with a pancreatobiliary disease such as pancreatic cancer, bile duct cancer, ampulla of vater carcinoma, or chronic pancreatitis with severe biliary stricture. Despite improvement in surgical techniques, biliary and pancreatic complications of PD are still frequent [1]. The use of diagnostic and therapeutic endoscopic retrograde cholangiopancreatography (ERCP) for patients with surgically altered anatomies has been facilitated by the development of balloon enteroscopy, including the use of a double-balloon enteroscope (DBE), a single-balloon enteroscope, and a short DBE [2–5], and ERCP has been commonly performed as the initial attempt to manage postoperative disorders prior to percutaneous drainage and reoperation.
One of the general reconstructions of PD is the modified Child method with Braun anastomosis, which is performed to divert bile from the gastric stump by creating an anastomosis between the afferent and efferent limbs [6]. When ERCP is performed for patients with this reconstruction, the enteroscope is conventionally advanced into the afferent limb at the gastrojejunal anastomosis (GJA) [7]. However, the Braun anastomosis makes the direction of scope insertion to a bilioenteric or pancreatoenteric anastomosis complicated. In addition, sharp angulations along the afferent limb sometimes occur [7, 8] and hinder the endoscopic manipulation.
In ERCP for patients undergoing PD with a Braun anastomosis, two different approaches for cholangiopancreatography are available anatomically; that is, the afferent-limb route and the efferent-limb route approaches as described below (Fig. 1). As yet, there have been no studies that explain technically how the approach is made in each route and that compare the suitability of the two routes for ERCP. Here we describe the outcome of ERCP for prior-PD patients in whom a short DBE was used, and we discuss how to approach by each route and which route is optimal for the performance of ERCP.

Two endoscopic approaches for cholangiopancreatography in patients undergoing pancreatoduodenectomy with a Braun anastomosis. A Afferent-limb route: the double-balloon enteroscope (DBE) is introduced through the opening linked to the lesser curvature of the stomach, which usually leads to the afferent limb at the gastrojejunal anastomosis (GJA); then it is advanced without passing the suture line (dotted line) at the Braun anastomosis, and reaches the bilioenteric and pancreaticoenteric anastomosis. B Efferent-limb route: the DBE is introduced through the opening linked to the greater curvature of the stomach, which usually leads to the efferent limb at the GJA; then it is advanced across the middle of the three-pronged lumens at the Braun anastomosis, and reaches the bilioenteric and pancreaticoenteric anastomosis
Methods
Patient population
From 2007 to 2013, 72 consecutive patients with prior PD including subtotal stomach-preserving pancreatoduodenectomy (SSPPD) and pylorus-preserving pancreatoduodenectomy (PPPD) underwent attempted diagnostic or therapeutic ERCP at Okayama University Hospital. All of the patients had clinical features of cholestasis or cholangitis. They were referred for abdominal ultrasonography, computed tomography, or magnetic resonance cholangiopancreatography for further evaluation. According to these imaging studies, when a dilation of bile duct was revealed, ERCP was immediately arranged. ERCP was also conducted for patients whose cases lacked a definitive explanation of liver damage despite the evaluation with additional imaging.
Endoscopic protocol
Before the patients underwent ERCP with a DBE, the procedure was fully explained to them, and written informed consent was obtained from all of the patients. This procedure was performed with the patient in a prone position under conscious sedation with diazepam and pethidine hydrochloride.
Diagnostic and therapeutic ERCP was conducted with a short DBE (EC-450BI5 or EI-530B, Fujifilm, Tokyo) under direct vision and fluoroscopy in the initial attempt. This type of DBE has a 152-cm working length and a 2.8-mm working channel, allowing for the use of almost all conventional accessories. In addition, the attachment was normally equipped at the tip of the DBE to improve the intubation of the scope and the visibility for seeking the equivocal anastomosis. A standard push-and-pull technique was used throughout the procedure [3] with CO2 insufflation.
After the identification of the bilioenteric anastomosis was achieved, cholangiography was generally performed using a 4-Fr tapered catheter (PR-V234Q, Olympus Medical Systems, Tokyo) and a 0.025- to 0.035-inch guidewire. In cases with bilioenteric anastomotic stricture, dilation by a 6- to 8-mm dia. balloon dilation catheter (Quantum TTC, COOK, Tokyo; Maxpass, Olympus Medical Systems) was usually performed. In cases with hepaticolithiasis, a retrieval balloon catheter, basket catheter, or mechanical lithotripter (XEMEX Crusher Catheter, XEMEX, Tokyo) was used for the removal of stones. In some cases with comorbidity of difficult hepaticolithiasis or severe cholangitis, the placement of the 6- or 7-Fr plastic stents was also performed in the initial session. When the subsequent stone extraction was completed or severe cholangitis subsided, the stents were removed. If residual stones were suspected, a peroral direct cholangioscopy with an ultraslim enteroscope (EG-530NW; Fujifilm) using overtube guidance was sometimes performed. If it was not easy to pass the accessories through the scope channel (showing resistance), olive oil was used as a lubricant during the procedure.
Two approaches for ERCP and techniques of scope insertion
Regarding the route to the bilioenteric anastomosis, two endoscopic approaches (the afferent-limb route and efferent-limb route) were used in prior-PD patients with Braun anastomosis. In the afferent-limb route, the DBE was introduced through the opening linked to the lesser curvature of the stomach, which usually led to the afferent limb at the GJA [7, 8]; then it was advanced without passing the suture line at the Braun anastomosis, and reached the bilioenteric anastomosis (Fig. 1A). In the efferent-limb route, the DBE was introduced through the opening linked to the greater curvature of the stomach, which usually led to the efferent limb at the GJA; then it was advanced across the middle of the three-pronged lumens at the Braun anastomosis and reached the bilioenteric anastomosis (Fig. 1B). This technique was applicable in the patients with prior PD or SSPPD.
In the patients with prior PPPD, the DBE was introduced through the opening visualized to the left or upper left side in the endoscopic view, which usually led to the afferent limb at the duodenojejunal anastomosis (DJA), and the subsequent route to the bilioenteric anastomosis was the same as described above; i.e., the afferent-limb route. However, the DBE was introduced through the opening visualized to the right or lower right side, which usually led to the efferent limb at the DJA, and then the procedure was the same as described above (i.e., the efferent-limb route).
The selection of the approach route was left to the endoscopist’s discretion in each case. If the scope insertion to the bilioenteric anastomosis by one route was unsuccessful, the insertion was attempted again after changing the approach route to the other route.
On the other hand, the afferent-limb route was always selected in prior-PD patients without Braun anastomosis.
Evaluations
To determine the usefulness of the short DBE in ERCP for patients who had prior PD, we retrospectively analyzed the following parameters of the initial session: the technical success rate, the details of treatment, the procedural time, and complications. As the evaluation of the maneuverability in the treatment, we used fluoroscopic images to analyze the shape of the DBE when it reached the bilioenteric anastomosis. Specifically, we measured the angle of the DBE which was formed by the intersection of the two tangent lines at 5 cm from the bottom of the arc-shaped scope bilaterally (Fig. 2). If a patient had no fluoroscopic images that were filmed in the prone position and described the whole shape of the DBE, the patient was excluded from this analysis. For revealing which route was optimal for ERCP, the angles of the DBE were compared between the two routes. Additionally, in the patients who underwent ERCP by each route during the study period, the angles of the DBE were compared individually.

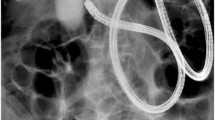
Fluoroscopic images in two cases. A Afferent-limb route (Case 1). B Efferent-limb route (Case 1). C Afferent-limb route (Case 2). D Efferent-limb route (Case 2)
Statistical analysis
Continuous data are presented as medians and ranges. Continuous variables were compared with the Mann–Whitney U test. Frequency distribution was compared with Fisher’s exact test or the χ 2 test. A paired analysis by Wilcoxon signed test was used for comparison of the angles of the DBE in the same individual. All statistical analyses were performed with JMP 8.0.1 software (SAS Institute, Cary, NC, USA). P values < 0.05 were considered significant.
Results
Overall outcome
The characteristics of the 72 patients are shown in Table 1. In 71 patients (98.6 %), the bilioenteric anastomosis was reached using the short DBE. In the unsuccessful case with a severe adhesion of the afferent limb, the anastomosis was unidentified, although the DBE nearly reached the anastomosis. Fortunately, this patient’s cholangitis improved conservatively without later percutaneous drainage.
The median length of time from scope insertion to the time when the bilioenteric anastomosis was reached in the 71 patients was 10 min (range 3–109 min). The median length of that in the patients with PD (n = 42), PPPD (n = 19), and SSPPD (n = 10) were 10.5 min (range 4–109 min), 9 min (range 3–85 min), and 9 min (range 3–40 min), respectively (p = 0.259).
Successful cannulation and cholangiography were achieved in all 71 patients (98.6 %) whose bilioenteric anastomosis was reached. Treatment for pancreatobiliary disorders was required in 59 of 71 patients (83 %). Fifty-two (73 %) and four (6 %) of the 71 patients had a bilioenteric anastomosis (benign, 48; malignant, four) and intrahepatic bile duct stricture (benign, two; malignant, two), respectively. In addition, 17 patients (24 %) had hepaticolithiasis, 14 of whom had comorbidity of bilioenteric anastomosis. The details of the treatments are given in Table 2. All endoscopic procedures for treatments were performed successfully.
The median procedural time from scope insertion to scope withdrawal in the 71 patients in whom successful ERCP was achieved was 50 min (range 9–167 min). The median procedural times in the patients with PD, PPPD, and SSPPD were 55 min (range 11–167 min), 40 min (range 30–106 min), and 51 min (range 9–120 min), respectively (p = 0.973).
Complications occurred in two patients (3 %) with cholangitis, which improved with conservative treatment. No complications including pancreatitis and perforation were observed.
Analysis of outcomes and the shape of the DBE by approach route
Among the 72 patients, the efferent-limb route was finally selected in 49 patients and the afferent-limb route in 18 patients (including the 2 patients without a Braun anastomosis), as the approach route to the bilioenteric anastomosis in the initial session. The remaining four patients with an unknown route and the single patient with Roux-en-Y reconstruction were excluded from the following analyses.
The DBE reaching rate for the bilioenteric anastomosis and the rate of successful treatment were both 98 % (48/49) with the use of the efferent-limb route, and they were both 100 % (18/18) with the use of the afferent-limb route. In an unsuccessful case in which the efferent-limb route was used, the bilioenteric anastomosis was unidentified as well by the afferent-limb route, because of a severe adhesion of the afferent limb. In addition, reaching the bilioenteric anastomosis was achieved in three patients by changing from the afferent-limb route to the efferent-limb route, because an inability to reach the Braun anastomosis in two patients and to pass the GJA in one patient occurred when using the afferent-limb route. However, no patients suffered procedural disadvantages when the efferent-limb route was used.
As shown in Table 3, the median lengths of time from scope insertion to the time that the bilioenteric anastomosis was reached were similar between the efferent-limb route (n = 48) and the afferent-limb route (n = 18) (9.5 min, range 3–109 min vs. 10 min, range 5–53 min, p = 0.282). According to the median procedural time from scope insertion to scope withdrawal, there was also no significant difference between the two routes (41 min, range 9–167 min vs. 63 min, range 12–50 min, p = 0.331). However, the median angle of the DBE was significantly larger when the efferent-limb route (n = 42) was used compared to when the afferent-limb route (n = 15) was used (128°, range 93°–151° vs. 113°, range 11°–158°, p = 0.037).
Analysis of outcomes and the shape of the DBE in patients undergoing repeated ERCP by each route
Fourteen (19 %) of the 72 patients underwent repeated ERCP in each route. In all 11 patients (15 %) whose DBE angle could be measured, a gentler arc-shaped angulation of the DBE was induced using the efferent-limb route compared to the afferent-limb route (median, range 123°, 85°–163° vs. 96°, 40°–158°, p = 0.003) (Fig. 3). However, the median length of time from scope insertion to reaching the bilioenteric anastomosis were essentially the same (10 min, range 4–28 min vs. 10 min, range 4–24 min, p = 0.741).

Comparison of the shape of the DBE in patients undergoing repeated cholangiography using both the afferent-limb route and the efferent-limb route
Discussion
Endoscopic management for pancreatobiliary disorders in patients with surgically altered anatomies is difficult because of the unusual anatomical features of the small intestine and postoperative adhesion. To improve this technical success rate, a pediatric colonoscope [8], a duodenoscope [8, 9], and an anterior oblique-viewing endoscope [10, 11] have been used instead of the conventional front-viewing enteroscope [12]. Balloon enteroscopy has enabled endoscopists to access the papilla or biliopancreatoenteric anastomoses more definitively and safely [2–5], and has been commonly performed as the initial attempt to manage several postoperative disorders, in patients with not only Roux-en-Y reconstruction but also prior PD and Billroth II gastrectomy. The present study examined a large case series undergoing ERCP using the short DBE for prior-PD patients. This is a first description of the two different methods of approach for ERCP in prior-PD patients with a Braun anastomosis, and the results revealed that the efferent-limb route is suitable as the primary approach because of the higher maneuverability during the procedure.
In previous articles, the rate of successful ERCP for biliary indications in prior-PD patients was 69–86 % using a front-viewing enteroscope, a pediatric colonoscope, or a duodenoscope [8, 9, 12]. Owing to the development of the short DBE which has a shorter radius of curvature of the tip of the scope as well as easier and greater maneuverability [13], this rate was increased to 96.7 % (29 of total 30 sessions) in 18 prior-PD patients [2, 5, 14]. However, the details of the digestive reconstruction were not mentioned in most of these studies.
In the present study, successful ERCP was achieved in 98.6 % (138 of 140 sessions) of 72 patients, even though 69 patients (96 %) had a Braun anastomosis which increased the length of the limbs [15] and challenged the endoscopist’s skill. It seems that both the utility of the short DBE and our insertion technique (described in Methods section) contributed greatly to the achievement of this high success rate of ERCP. The causes of unsuccessful ERCP were the inability to reach the bilioenteric anastomosis due to a malignant intestinal obstruction in one patient and severe adhesion of the afferent limb in another. There was no unsuccessful ERCP by the short DBE due to excessive length of the afferent limb. In addition, there were no severe complications in the previous and present studies [2, 5, 14].
Conventionally, the afferent-limb route has been selected for ERCP in prior-PD patients with or without a Braun anastomosis, perhaps because that route was considered a shortcut to the bilioenteric or pancreatoenteric anastomosis. However, we experienced some cases in which it became easy to reach the anastomoses by altering the approach route from the afferent-limb route to the efferent-limb route. An earlier study reported that the causes of difficulty in reaching the bilioenteric or pancreatoenteric anastomosis in prior-PD patients were severe adhesions of the afferent limb and/or efferent limb, excessive looping of the enteroscope and/or excessive length of the afferent limb, and metastatic obstruction of the intestine [8]. In addition, scope insertion to the afferent limb at the GJA was sometimes difficult by the afferent-limb route, perhaps because sharp angulation was formed from the effects of surgery [16]. Failure to enter the afferent limb occurred in 2.2–10 % of patients with a Billroth II gastrectomy in several different series [17–19].
In brief, the afferent-limb route is not the best choice for ERCP. The volume of bile in the limb and peristalsis were reported to be helpful in distinguishing between the afferent limb and the efferent limb [20], but in fact, this was often not possible. In the present study, the direction of the afferent limb or efferent limb at the GJA and the Braun anastomosis was clarified using our insertion technique. In addition, we found that when using the efferent-limb route it was sometimes a far distance to the anastomoses, although there was no significant difference in the lengths of time from scope insertion to reaching the bilioenteric anastomosis between the two routes (Table 3). This might indicate that the disadvantage of the efferent-limb route was off-set using the DBE, which made the intestine pleated over the overtube. Making proper use of the two different routes allowed the achievement of reaching the bilioenteric or pancreatoenteric anastomosis definitely and rapidly in most cases.
We also observed that in the ERCP for prior-PD patients with a Braun anastomosis, an arc-shaped angulation of the enteroscope was usually formed as shown by fluoroscopic imaging when the enteroscope reached the bilioenteric or pancreatoenteric anastomosis. Our comparison of the two routes by fluoroscopic imaging revealed that a sharper angulation of the DBE occurred with the afferent-limb route compared to the efferent-limb route. Furthermore, in all 11 (15 %) individual patients who underwent repeated ERCP by each route during the study period, a gentler arc-shaped angulation of the DBE was induced using the efferent-limb route rather than the afferent-limb route, as described in Fig. 3. This phenomenon was easily speculated from the anatomical structure shown in Fig. 1. This sharp angulation of the DBE could sometimes cause reduced maneuverability in the ERCP, such as scope insertion to a tight and sharp-angled limb [8] and the handling of various accessories through the narrow scope channel with a sense of resistance. To overcome these difficulties, the injection of a lubricant such as olive oil into the scope channel was helpful, and the endoscopist’s expertise was necessary. The ERCP for some patients were barely completed using their ideas and experiences in our clinical practice, and then there was no significant difference in the technical success rate for treatment or the lengths of procedural time between the two routes, fortunately.
In fact, it is apparent that ERCP using the afferent-limb route had no advantage and was a challenging procedure. We propose that the efferent-limb route, which made the procedure maneuverable and stable without unnecessary stress, is suitable and acceptable as a first choice for ERCP. No other ideas for optimal ERCP in light of approach routes have been reported, to the best of our knowledge.
These analyses could be applied to ERCP for patients undergoing the Billroth II gastrectomy with intact papilla. The selection of the approach route might also affect the facilitation of the biliary cannulation for these patients. However, the present study was retrospective and we did not examine this issue. Additionally, our analysis of the optimal approach route was subject to a bias, namely the selection of the approach route depended on the endoscopists’ discretion. Randomized prospective studies with large patient numbers are necessary to establish the optimal strategy for ERCP in patients with a prior PD.
In conclusion, the short DBE facilitates diagnostic and therapeutic ERCP in patients with a prior PD. Particularly, ERCP using the efferent-limb route can achieve a maneuverable and stable procedure without unnecessary stress, such as scope insertion to the sharp-angled afferent limb, and the handling of various accessories through the narrow scope channel with a sense of resistance, despite the various lengths of limbs and degrees of adhesion. This efferent-limb route approach is optimal for ERCP in patients who have undergone a PD with a Braun anastomosis and may be considered the standard approach in that setting.
References
House MG, Cameron JL, Schulick RD, Campbell KA, Sauter PK, Coleman J, Lillemoe KD, Yeo CJ (2006) Incidence and outcome of biliary strictures after pancreaticoduodenectomy. Ann Surg 243:571–578
Shimatani M, Matsushita M, Takaoka M, Koyabu M, Ikeura T, Kato K, Fukui T, Uchida K, Okazaki K (2009) Effective “short” double-balloon enteroscope for diagnostic and therapeutic ERCP in patients with altered gastrointestinal anatomy: a large case series. Endoscopy 41:849–854
Aabakken L, Bretthauer M, Line PD (2007) Double-balloon enteroscopy for endoscopic retrograde cholangiography in patients with a Roux-en-Y anastomosis. Endoscopy 39:1068–1071
Itoi T, Ishii K, Sofuni A, Itokawa F, Tsuchiya T, Kurihara T, Tsuji S, Ikeuchi N, Umeda J, Moriyasu F (2010) Single-balloon enteroscopy-assisted ERCP in patients with Billroth II gastrectomy or Roux-en-Y anastomosis (with video). Am J Gastroenterol 105:93–99
Osoegawa T, Motomura Y, Akahoshi K, Higuchi N, Tanaka Y, Hisano T, Itaba S, Gibo J, Yamada M, Kubokawa M, Sumida Y, Akiho H, Ihara E, Nakamura K (2012) Improved techniques for double-balloon-enteroscopy-assisted endoscopic retrograde cholangiopancreatography. World J Gastroenterol 18:6843–6849
Kimura W (2008) Strategies for the treatment of invasive ductal carcinoma of the pancreas and how to achieve zero mortality for pancreaticoduodenectomy. J Hepatobiliary Pancreat Surg 15:270–277
Feitoza AB, Baron TH (2002) Endoscopy and ERCP in the setting of previous upper GI tract surgery. Part II: postsurgical anatomy with alteration of the pancreaticobiliary tree. Gastrointest Endosc 55:75–79
Chahal P, Baron TH, Topazian MD, Petersen BT, Levy MJ, Gostout CJ (2006) Endoscopic retrograde cholangiopancreatography in post-Whipple patients. Endoscopy 38:1241–1245
Farrell J, Carr-Locke D, Garrido T, Ruymann F, Shields S, Saltzman J (2006) Endoscopic retrograde cholangiopancreatography after pancreaticoduodenectomy for benign and malignant disease: indications and technical outcomes. Endoscopy 38:1246–1249
Kikuyama M, Sasada Y, Matsuhashi T, Ota Y, Nakahodo J (2009) ERCP after Roux-en-Y reconstruction can be carried out using an oblique-viewing endoscope with an overtube. Dig Endosc 21:180–184
Nakahara K, Horaguchi J, Fujita N, Noda Y, Kobayashi G, Ito K, Obana T, Takasawa O (2009) Therapeutic endoscopic retrograde cholangiopancreatography using an anterior oblique-viewing endoscope for bile duct stones in patients with prior Billroth II gastrectomy. J Gastroenterol 44:212–217
Matsushita M, Takakuwa H, Uchida K, Nishio A, Okazaki K (2009) Techniques to facilitate ERCP with a conventional endoscope in patients with previous pancreatoduodenectomy. Endoscopy 41:902–906
Haber GB (2008) Double-balloon enteroscopy in patients with altered biliary and/or pancreatic anatomy. Gastroenterol Hepatol (N Y) 4:397–399
Cho S, Kamalaporn P, Kandel G, Kortan P, Marcon N, May G (2011) ‘Short’ double-balloon enteroscope endoscopic retrograde cholangiopancreatography in patients with a surgically altered upper gastrointestinal tract. Can J Gastroenterol 25:615–619
Trede M (1997) Technique of Whipple pancreatoduodenectomy. In: Trede M, Carter DC, Longmire WP (eds) Surgery of the Pancreas. Churchill Livingstone, New York, pp 487–498
Lin LF, Siauw CP, Ho KS, Tung JC (1999) ERCP in post-Billroth II gastrectomy patients: emphasis on technique. Am J Gastroenterol 94:144–148
Kim MH, Lee SK, Lee MH, Myung SJ, Yoo BM, Seo DW, Min YI (1997) Endoscopic retrograde cholangiopancreatography and needle-knife sphincterotomy in patients with Billroth II gastrectomy: a comparative study of the forward-viewing endoscope and the side-viewing duodenoscope. Endoscopy 29:82–85
Faylona JM, Qadir A, Chan AC, Lau JY, Chung SC (1999) Small-bowel perforations related to endoscopic retrograde cholangiopancreatography (ERCP) in patients with Billroth II gastrectomy. Endoscopy 31:546–549
Ciçek B, Parlak E, Dişibeyaz S, Koksal AS, Sahin B (2007) Endoscopic retrograde cholangiopancreatography in patients with Billroth II gastroenterostomy. J Gastroenterol Hepatol 22:1210–1213
Feitoza AB, Baron TH (2001) Endoscopy and ERCP in the setting of previous upper GI tract surgery. Part I: reconstruction without alteration of pancreaticobiliary anatomy. Gastrointest Endosc 54:743–749
Disclosures
Koichiro Tsutsumi, Hironari Katio, Shinichiro Muro, Naoki Yamamoto, Yasuhiro Noma, Shigeru Horiguchi, Ryo Harada, Hiroyuki Okada, and Kazuhide Yamamoto have no conflicts of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Tsutsumi, K., Kato, H., Muro, S. et al. ERCP using a short double-balloon enteroscope in patients with prior pancreatoduodenectomy: higher maneuverability supplied by the efferent-limb route. Surg Endosc 29, 1944–1951 (2015). https://doi.org/10.1007/s00464-014-3889-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-014-3889-8