
Abstract
Background
The anastomosis of gastric remnant to esophagus after proximal gastrectomy is the traditional surgical treatment procedure for patients with types II and III adenocarcinoma of esophagogastric junction. However, the postoperative complications such as gastroesophageal reflux are frequent.
Aims
To assess the outcome of the intraperitoneal anastomosis of the reconstructed gastric tube to esophagus after proximal gastrectomy for types II and III adenocarcinoma of esophagogastric junction.
Methods
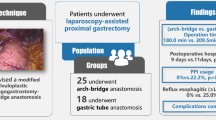
Seventy-six consecutive patients with preoperative diagnosis of type II or type III adenocarcinoma of esophagogastric junction were recruited. Forty-one patients had the traditional anastomosis of gastric remnant to esophagus and 35 patients underwent an anastomosis of esophagus to a gastric tube that was constructed from the gastric remnant after proximal gastrectomy.
Results
Twenty-three (56.1%) versus 12 (28.6%) patients (p = 0.016) complained various discomforts and/or were diagnosed with complications in the traditional group and gastric tube group, respectively, although there were no significant differences between the two groups in demographic data and pathological characteristics. Fourteen (34.1%) versus five (14.3%) patients (p = 0.046) complained of heartburn or acid regurgitation and nine (22.0%) versus two (5.7%) patients (p = 0.045) were confirmed reflux esophagitis in the traditional group and the gastric tube group, respectively.
Conclusions
The intraperitoneal anastomosis of the reconstructed gastric tube to esophagus demonstrates less complaints of gastroesophageal reflux and reflux esophagitis than the traditional anastomosis of gastric remnant to esophagus in the surgical treatment of types II and III adenocarcinoma of esophagogastric junction in 1-year follow-up.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The adenocarcinoma of esophagogastric junction (AEG) was systematically defined by Siewert et al. in 1996. Since then, the incidence of AEG has been increasing due partly to the worldwide diagnostic awareness [1, 2]. Currently, surgical treatment is still the preferred curative or palliative treatment [3].
According to Siewert’s classification, AEG is classified into three types. Type I AEG defines the distal esophageal adenocarcinoma located from 1 to 5 cm above the anatomic esophagogastric junction (EGJ). Type II AEG labels the adenocarcinoma positioned from 1 cm above to 2 cm below the EGJ. Type III AEG lies from 2–5 cm below the EGJ [4]. It is not uncommon that type II and type III AEG are accompanied by abdominal lymph node metastasis [5]. Abdominal surgery, both proximal gastrectomy and traditional esophagogastrostomy, with a D2 or D2+ lymphadenectomy are widely used to treat these two types of AEG [6]. High prevalence of postoperative complications such as reflux esophagitis were reported following surgical treatment [7, 8]. To reduce postoperative complications, we adopted the technique of reconstructing a gastric tube before anastomosis of the gastric remnant to the esophagus in this study that has been used in surgical treatment of esophageal cancer with fewer postoperative complications [9], and the technique of gastric tube reconstruction for the upper third gastric cancer by abdominal open surgery was first reported by Shiraishi et al. in 1998 [10]. The technique includes two steps; the gastric remnant is first reconstructed as a tube after proximal gastrectomy; then it is anastomosized with the proximal esophagus. A prospective cohort study was designed to assess the outcomes of the intraperitoneal anastomotic procedure of gastric tube in comparison to the traditional abdominal surgical approach.
Methods
Patient Selection
Seventy-six patients (59 males and 17 females, mean age 61 years) with AEG were admitted consecutively with curative intent in a single medical center, the Department of Gastrointestinal Surgery, West China Hospital, Sichuan University, China, between January 2009 and April 2010. The diagnosis and AEG classification were verified by a combination of endoscopy, CT scan, intraoperative observation, and histopathological examination. Twenty-seven patients were type II AEG and 49 patients were type III AEG according to Siewert’s classification. Patients who were with severe systemic disease, incapacitating general condition, distant metastasis, history of or comorbid with other cancer(s), history of gastric or esophageal surgery, or resection of the tumor that made it impossible to construct a gastric tube or complete esophagogastrostomy were excluded. No patient underwent preoperative neoadjuvant chemotherapy or radiotherapy. Of the 76 patients, the choice of surgical treatment was based on their own preference after signing an informed consent form. Forty-one patients (32 males, nine females) were performed direct anastomosis of the esophagus to the gastric remnant after proximal gastrectomy and were defined as the traditional group. The other 35 patients (27 males, eight females) who underwent anastomosis of tubular stomach to the esophagus were denoted as the gastric tube group. The protocol was approved by the institutional review board and committee of West China Hospital of Sichuan University. The patients were informed the purpose of the study, the nature of the surgery, possible postoperative complications, and the availability of other options in the patient recruitment process. However, no potential advantage of one procedure over the other was mentioned to the patients. All of the patients included in this study signed the informed consent forms.
Surgical Procedures and Management
All patients of two groups were operated on through the abdominal approach. The procedure started with a midline upper abdominal incision. Every patient underwent a radical proximal gastrectomy, vagectomy, and D2 lymphadenectomy or greater D2 lymphadenectomy in accordance with the guidelines of the Japanese Gastric Cancer Association (JGCA). The esophagus was dissected under direct vision through widened hiatus of the diaphragm. The incisional margin was assured free of tumor cells by the intraoperative histological examination of frozen sections. The stomach was sheared approximately 40–70% of its original size. Right gastric vessels and right gastroepiploic vessels were preserved after proximal gastrectomy. If the volume of gastric remnant was less than 30% of the original volume, where it was impossible to construct a gastric tube, a total gastrectomy was performed, and the case was excluded from this study.
For the traditional group, gastric remnant was directly anastomosed with the proximal esophageal end to reconstruct the archenteric continuity. In the gastric tube group, the lesser curvature of the gastric remnant approximately 3 cm proximal to the pylorus was removed first by a linear-stapling device. An approximately 5-cm-wide tubular stomach was then constructed with preserved right gastric vessels. The length of the tube was consistent with the greater curvature of the residual stomach. The reconstructed tubular stomach or gastric tube was lastly anastomosed with the proximal esophageal end.
Both operation procedures were performed by the same surgery team. All patients had the same postoperative program of treatment such as nil per os, gastric decompression, and nutritional support when staying in hospital. All patients with diabetes were insulinized in the perioperative period, and their blood glucose was control in 5.0–8.0 mmol/l range. Patients started convalescent diet after the recovery of gastrointestinal function. Patients were discharged from the hospital after the surgical wound healed and were able to ambulate.
Data Collection and Assessment
Patient information and hospital data were obtained from the patients’ medical records. All patients were followed-up in the outpatient clinic at the first, sixth, and twelfth month, respectively, after discharge. At the first follow-up clinic visit, patients with advanced stage higher than T2 or lymph node metastasis were started on adjuvant chemotherapy. At the sixth and twelfth-month visits, the patients underwent endoscopic examination in addition to the conventional outpatient follow-up procedures. With complaint of heartburn, acid regurgitation, or dysphagia, patients would undergo an endoscopy. An antacid would be given if the patient was diagnosed with reflux esophagitis. Patients with reflux esophagitis were followed more frequently by telephone or clinic visit for better management of the postoperative complications. The clinico-pathological TNM stages were made according to the criteria in the Seventh Edition of the American Joint Committee on Cancer (AJCC) Staging Manual [11]. The severity of reflux esophagitis was assessed in accordance with the Los Angeles Classification of Esophagitis [12]. Delayed gastric emptying (DGE) was based on the time of chyme presence in the gastric remnant or gastric tube.
Statistical Analysis
The means of the two groups were assessed with an independent sample t test. Enumeration data were analyzed with the Chi-square test. Ranked data were tested by Wilcoxon test method. Statistical analysis was run on SPSS 17.0 software for Windows. p < 0.05 was considered statistically significant.
Results
Demographic Data and Postoperative Complications
All 76 patients with type II AEG or type III AEG underwent radical surgical resection through the abdominal approach. Both groups had a majority of males. In the traditional group, there were 32 (78.0%) males and nine (22.0%) females; the average age was 59.49 ± 8.71 years. Accordingly, there were 27 (77.1%) males and eight (22.9%) females with an average age of 63.06 ± 7.94 years in the gastric tube group. There were no significant differences between the two groups with respect to their gender, age, and the length of postoperative hospital stay.
There were no significant differences between the two groups with respect to preoperative risk factors for postoperative complications, such as obesity (BMI) (p = 0.792), history of reflux/heartburn (p = 1.000), diabetes (p = 0.800). Twenty-three (56.1%) patients versus ten (28.6%) patients (p = 0.016) complained of various discomforts and/or were diagnosed with complications after surgery in the traditional group and the gastric tube group, respectively. There were no severe postoperative complications such as pneumonia, abdominal wound infection, intestinal obstruction, anastomotic leakage, or diarrhea of the 76 patients. One patient, who also had hypertension, in each group, experienced postoperative anastomotic bleeding. They were successfully managed by conservative medical treatment. Nevertheless, some mild to moderate postoperative complications or discomfort were reported from the 1-year follow-up visits.
Significant differences of the postoperative reflux symptoms (p = 0.046) and reflux esophagitis (p = 0.045) between the traditional group and the gastric tube group were found. Accumulatively, 14 (34.1%) patients in the traditional group reported reflux symptoms (heartburn or acid regurgitation) in the 12-month follow-up. Nine (22.0%) patients were confirmed to have reflux esophagitis by endoscopy. Of the nine patients, six were in grade A; two patients were in grade B; and one patient was in grade C based on the Los Angeles Classification of Esophagitis. In contrast, only five (14.3%) patients complained of reflux symptoms in the gastric tube group and two (5.7%) cases were verified as reflux esophagitis in grade A by endoscopic examination (Table 2). Furthermore, nine (22.0%) patients and four (11.4%) patients (p = 0.225) were diagnosed by endoscopy as anastomotic stenosis in the traditional group and the gastric tube group, respectively. No significant differences were found between the traditional group and the gastric tube group in the infrequent postoperative complications of anastomotic bleeding (p = 0.910), intractable hiccup (p = 1.000), delayed gastric emptying (p = 1.000), dysphagia (p = 1.000), and diarrhea (p = 0.889). The demographic data and postoperative complications are summarized in Table 1.
Operative Information
There were no significant differences between the two groups with respect to operation time (p = 0.057), intraoperative bleeding (p = 0.877), and perioperative blood transfusion (p = 1.000). There was no incidence of death or reoperation in the two groups. Table 3 summarized the postoperative complications in the two groups.
Tumorous and Pathological Characteristics
All patients had radical surgery. The incisional margins of all patients were assured free of residual tumor tissues by the intraoperative histological examination of frozen sections. The surgical specimens underwent postoperative histopathological examination and were graded according to the criteria in the Seventh Edition of the American Joint Committee on Cancer (AJCC) Staging Manual. There were no significant differences between the two groups in terms of the Siewert classification (p = 0.835), Bormann type (p = 0.791), histopathological characteristics (p = 0.553), tumor size (p = 0.166), and TNM stages (p = 0.660). Siewert type III and Bormann type II were the majority in both groups. Twenty-six (63.4%) patients versus 23 (65.7%) patients were in the Siewert type III and Bormann type II, respectively, in the traditional group. Thirty (73.2%) patients versus 29 (82.9%) patients were in the Siewert type III and Bormann type II, respectively, in the gastric tube group. Histopathologically, moderately and poorly differentiated types were of the typical. The average tumor size was 4.42 ± 1.59 and 3.93 ± 1.42 cm in the traditional and the gastric tube group (p = 0.166), respectively. The majority was stage pT4 and had stage III in the TNM stage evaluation. No lymphatic metastases were found in 11 patients of each group in postoperative pathologic examination. No patient had distant metastasis per intraoperative exploration and postoperative histopathological examination. Two patients with advanced III stage tumor in each group were found to have local tumor recurrence in the follow-up visits (p = 1.000). The pathological characteristics of the two groups are detailed in Table 3.
Discussion
There is no shortage of literature in the field of the AEG in recent years. The prognosis of the AEG is still poor in general [13]. The purpose of treatment is mostly palliative with expectation to prolong the life and improve the quality of life. Surgical treatment is the current treatment of choice for AEG patients [14]. Proximal gastrectomy and total gastrectomy through the abdominal approach have been widely used and proved to be a reliable surgical method for patients with types II and III AEG [3, 14]. Although there were reports [15] that noted high morbidity of the proximal gastrectomy with esophagogastric anastomosis, Harrison et al. [16] reported that the long-term outcomes were not influenced by surgical procedures for proximal gastric cancer. Total gastrectomy and proximal gastrectomy had comparable overall survival time and recurrent rate. Shiraishi et al. [17] reported that total gastrectomy significantly increased operation time, blood loss, postoperative hospital stay, and hospital cost as compared to proximal gastrectomy although the quality of life was not statistically different. Furthermore, proximal gastrectomy has the advantage of retaining part of the stomach to meet the physiological requirements and benefit gastrointestinal reconstruction [18]. This surgical procedure, however, destroys the anatomic anti-reflux barriers, which includes the lower esophageal sphincter, diaphragmatic angle, diaphragmatic esophageal ligament, His horn, etc. [19]. The removal of anti-reflux barriers makes the backward flow of gastric contents easier and subsequently leads to regurgitation or reflux esophagitis. It is inevitable that most patients would complain of symptoms of reflux after the surgical treatment [20]. The gastroesophageal reflux may also increase the incidence of anastomotic stenosis [21]. In our traditional group, there was a high morbidity of gastroesophageal reflux complications. Fourteen (34.1%) patients complained of heartburn or acid regurgitation, and nine(22.0%) patients were diagnosed with reflux esophagitis. The results of nine (22.0%) patients found having anastomotic stenosis and two (4.9%) of them complaining of dysphagia support this speculation. Moreover, in surgical treatment, neither the option of a small gastric remnant, which increases the tension of the anastomotic stoma, nor the option of a large gastric remnant, which raises the incidence of anastomotic leakage due to poor blood supply, is favored [22]. No patient had anastomotic leakage in this study. In addition, the vagus nerve, which plays an important role in regulating gastrointestinal motility and secretion, is severed in the proximal gastrectomy procedure [23]. Denervation of the gastrointestinal system by vagotomy may cause gastroparesis, gastrointestinal obstruction, and functional impairment of the digestion and absorption [24]. There were two (4.9%) patients that had DGE and one (2.4%) complained of diarrhea.
Although the postoperative complications are contingent upon preoperative medical conditions, characteristics of tumors and the quality of perioperative care, it is a general consensus that the surgical procedure is the critical determinant in directing the extent and severity of postoperative complications [25]. The surgical procedure, intraperitoneal anastomosis of gastric tube, did show an improvement of the postoperative complication profiles, especially the complications with high incidence. In this study, there were no significant differences between the two groups with respect to the characteristics of tumors and preoperative risk factors such as obesity (BMI), history of reflux/heartburn, diabetes, and other medical conditions for postoperative complications. Compared with the traditional group, only five (14.3%) patients reported symptoms of gastroesophageal reflux in the gastric tube group (p = 0.046). Two (5.7%) patients were verified as having reflux esophagitis (p = 0.045). In addition, the grade of reflux esophagitis in the gastric tube group was also lower than that in the traditional group. The latency of the onset of reflux symptoms and reflux esophagitis after operation in the traditional group was shorter than that in the gastric tube group (Fig. 1).

Cumulative incidences of postoperative complications in the traditional group and the gastric tube group following proximal gastrectomy. a Symptoms of gastroesophageal reflux (p = 0.046). b Reflux esophagitis (p = 0.045)
The following mechanisms may be attributed to the improved postoperative complication profiles of the gastric tube reconstruction. Firstly, part of the gastric antrum was removed that would decrease the secretion of gastrin and acid and therefore reduce the severity of the esophageal reflux. Secondly, the gastric tube preserves the anatomic structure of the stomach [26]. Although it is smaller, it functions for food storage and digestion. Thirdly, the gap length between the esophagus and gastric remnant is directly related to anastomotic tension. Anastomotic tension can lead to complications like gastroesophageal reflux, stenosis, and anastomotic leakage [27]. The longer length of gastric tube would reduce the anastomotic tension, which can reduce the incidence of anastomotic leakage. Fourthly, reservation of the right blood vessels while reducing the gastric volume favors blood supply to the anastomic stoma.
Although the incidences of anastomotic stenosis were not statistically different in the two groups (p = 0.225), the latency between the two groups are prominent. We understand that the risk of reflux esophagitis might increase with time [28] and the development of anastomotic stenosis is positively related to gastroesophageal reflux or reflux esophagitis [18]. With data from 1 year of postoperative follow-up of this sample size, it is safe to speculate that the trend of fewer postoperative complications in the gastric tube group would occur with the increase of sample size and duration of postoperative follow-up. Moreover, the original low incidence of anastomotic leakage [4, 29], the improvement of the anastomotic instrument, and technology might contribute to the zero incidence of anastomotic leakage in this study. There is no evidence to state that the gastric tube group has the advantage of decreasing anastomotic leakage, although it should have, theoretically, considering the decreased anastomotic tension.
For surgery per se, several factors are thought to be relevant to the safety of surgery, postoperative recovery, and prognosis of patients. It has been recognized that excessive intraoperative bleeding is associated with significant morbidity, mortality, and complications [30–32]. Prolonged operation time is also an independent predictor for the development of postoperative complications [33, 34]. The effect of perioperative transfusions to the recurrence of cancer is, however, still inconclusive. Blumberg et al. [35] reported that blood transfusion is significantly associated with the recurrence of cancer. McAlister et al. [36] considered that allogeneic blood transfusion and increases in the risk of adverse sequelae in patients with cancer undergoing surgery are not necessarily correlated. To create a gastric tube might need longer time than direct esophagogastrostomy. The operation time was 268.41 ± 28.18 and 280.00 ± 25.48 min in the traditional and the gastric tube group, respectively. It is not statistically different. There were also no significant differences in these basic surgical parameters such as intraoperative bleeding and blood transfusion between the two groups. In addition, the favorable postoperative outcome also supports the hypothesis that the surgical procedure approaching through abdomen may have little effect on cardio-pulmonary function and other systems [37, 38]. No patient suffered from pneumonia or other systemic complication in the two groups. Due to the almost similar effect on other systems, the postoperative hospitalization time was 10.54 ± 1.95 and 10.49 ± 1.93 days in the traditional group and the gastric tube group, respectively.
Pathologic features are the most important factor affecting the prognosis and survival of cancer patients. The incisional margin status is a risk factor of local recurrence [39]. Our data confirmed most of the pathologic features of the AEG noted by other authors such as dominance of Bormann type II, mainly moderately and/or poorly differentiated histopathological type and significant proportions with deep infiltration and lymphatic metastasis [40, 41]. The incisional margin was assured no residual tumor tissues by the intraoperative histological examination of frozen sections. The pathological features and tumor recurrence rate were not significantly different in the two groups (p > 0.05). However, there were two patients from each group who had local tumor recurrence. All of the four patients had the same pathological stage of advanced tumor before surgery. None of the patients died in the 12 months of follow-up. This should be credited not only to the postoperative chemotherapy but also to the standard operation procedures. There was no difference in the tumor resection procedure between the traditional and the gastric tube groups. Considering only one step more was added in the gastric tube group, it is understandable that barely any difference exists in the safety aspect of the surgery. As an effective surgical treatment to AEG, the gastric tube procedure is as good as, if not better than, the traditional surgical procedure in safety and feasibility of surgery.
The caveat of the present study is the duration of postoperative follow-up and sample size. Extended follow-up time and larger sample size may reveal more postoperative complications or recurrence of the tumor that may help in assessing the long-term advantage of the new surgical procedure [28]. Multicenter, randomized trials of a large sample in the future will generate more convincing data concerning the advantage of the gastric tube procedure.
In conclusion, the anastomosis of a constructed gastric tube to the esophagus demonstrates the advantage of less and milder postoperative complications, especially fewer symptoms of gastroesophageal reflux and incidence of reflux esophagitis, while not compromising the safety of the traditional surgical treatment of types II and III AEG.
References
Devesa SS, Blot WJ, Fraumeni JF Jr. Changing patterns in the incidence of esophageal and gastric carcinoma in the United States. Cancer. 1998;83:2049–2053.
Fan YJ, Song X, Li JL, et al. Esophageal and gastric cardia cancers on 4,238 Chinese patients residing in municipal and rural regions: a histopathological comparison during 24-year period. World J Surg. 2008;32:1980–1988.
Hasegawa S, Yoshikawa T. Adenocarcinoma of the esophagogastric junction: incidence, characteristics, and treatment strategies. Gastric Cancer. 2010;13:63–73.
Johansson J, Djerf P, Oberg S, et al. Two different surgical approaches in the treatment of adenocarcinoma at the gastroesophageal junction. World J Surg. 2008;32:1013–1020.
Barbour AP, Rizk NP, Gonen M, et al. Lymphadenectomy for adenocarcinoma of the gastroesophageal junction (GEJ): impact of adequate staging on outcome. Ann Surg Oncol. 2007;14:306–316.
Lehmann K, Schneider PM. Differences in the molecular biology of adenocarcinoma of the esophagus, gastric cardia, and upper gastric third. Recent Results Cancer Res. 2010;182:65–72.
An JY, Youn HG, Choi MG, Noh JH, Sohn TS, Kim S. The difficult choice between total and proximal gastrectomy in proximal early gastric cancer. Am J Surg. 2008;196:587–591.
Katai H, Sano T, Fukagawa T, Shinohara H, Sasako M. Prospective study of proximal gastrectomy for early gastric cancer in the upper third of the stomach. Brit J Surg. 2003;90:850–853.
Shibuya S, Fukudo S, Shineha R, et al. High incidence of reflux esophagitis observed by routine endoscopic examination after gastric pull-up esophagectomy. World J Surg. 2003;27:580–583.
Shiraishi N, Hirose R, Morimoto A, Kawano K, Adachi Y, Kitano S. Gastric tube reconstruction prevented esophageal reflux after proximal gastrectomy. Gastric Cancer. 1998;1:78–79.
Washington K. 7th Edition of the AJCC cancer staging manual: stomach. Ann Surg Oncol. 2010;17:3077–3079.
Armstrong D, Bennett JR, Blum AL, et al. The endoscopic assessment of esophagitis: a progress report on observer agreement. Gastroenterology. 1996;111:85–92.
Omloo JM, Lagarde SM, Hulscher JB, et al. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the mid/distal esophagus: five-year survival of a randomized clinical trial. Ann Surg. 2007;246:992–1001.
Carboni F, Lorusso R, Santoro R, et al. Adenocarcinoma of the esophagogastric junction: the role of abdominal-transhiatal resection. Ann Surg Oncol. 2009;16:304–310.
Yoo CH, Sohn BH, Han WK, Pae WK. Long-term results of proximal and total gastrectomy for adenocarcinoma of the upper third of the stomach. Cancer Res Treat. 2004;36:50–55.
Harrison LE, Karpeh MS, Brennan MF. Total gastrectomy is not necessary for proximal gastric cancer. Surgery. 1998;123:127–130.
Shiraishi N, Adachi Y, Kitano S, Kakisako K, Inomata M, Yasuda K. Clinical outcome of proximal versus total gastrectomy for proximal gastric cancer. World J Surg. 2002;26:1150–1154.
Aihara R, Mochiki E, Ohno T, et al. Laparoscopy-assisted proximal gastrectomy with gastric tube reconstruction for early gastric cancer. Surg Endosc. 2010;24:2343–2348.
Sakamoto T, Fujimaki M, Tazawa K. Ileocolon interposition as a substitute stomach after total or proximal gastrectomy. Ann Surg. 1997;226:139–145.
Kim EM, Jeong HY, Lee ES, et al. Comparison between proximal gastrectomy and total gastrectomy in early gastric cancer. Korean J Gastroenterol/Taehan Sohwagi Hakhoe Chi. 2009;54:212–219.
Kim HK, Choi YH, Shim JH, et al. Endoscopic evaluation of the quality of the anastomosis after esophagectomy with gastric tube reconstruction. World J Surg. 2008;32:2010–2014.
Ikeda Y, Niimi M, Kan S, Shatari T, Takami H, Kodaira S. Clinical significance of tissue blood flow during esophagectomy by laser Doppler flowmetry. J Thorac Cardiovasc Surg. 2001;122:1101–1106.
Berthoud HR. The vagus nerve, food intake and obesity. Regul Pept. 2008;149:15–25.
Kojima K, Yamada H, Inokuchi M, Kawano T, Sugihara K. Functional evaluation after vagus-nerve-sparing laparoscopically assisted distal gastrectomy. Surg Endosc. 2008;22:2003–2008.
Kolh P, Honore P, Degauque C, Gielen J, Gerard P, Jacquet N. Early stage results after oesophageal resection for malignancy—colon interposition vs. gastric pull-up. Eur J Cardio Thorac Surg. 2000;18:293–300.
Walther B, Johansson J, Johnsson F, Von Holstein CS, Zilling T. Cervical or thoracic anastomosis after esophageal resection and gastric tube reconstruction: a prospective randomized trial comparing sutured neck anastomosis with stapled intrathoracic anastomosis. Ann Surg. 2003;238:803–812; discussion 812–804.
Nagaya M, Kato J, Niimi N, Tanaka S, Iio K. Proposal of a novel method to evaluate anastomotic tension in esophageal atresia with a distal tracheoesophageal fistula. Pediatric Surg Int. 2005;21:780–785.
Yajima K, Kosugi S, Kanda T, Matsuki A, Hatakeyama K. Risk factors of reflux esophagitis in the cervical remnant following esophagectomy with gastric tube reconstruction. World J Surg. 2009;33:284–289.
Adachi Y, Inoue T, Hagino Y, Shiraishi N, Shimoda K, Kitano S. Surgical results of proximal gastrectomy for early-stage gastric cancer: jejunal interposition and gastric tube reconstruction. Gastric Cancer. 1999;2:40–45.
Nesbakken A, Nygaard K, Westerheim O, Lunde OC, Mala T. Audit of intraoperative and early postoperative complications after introduction of mesorectal excision for rectal cancer. Eur J Surg. 2002;168:229–235.
Viklund P, Lindblad M, Lu M, Ye W, Johansson J, Lagergren J. Risk factors for complications after esophageal cancer resection: a prospective population-based study in Sweden. Ann Surg. 2006;243:204–211.
Lehnert T, Cardona S, Hinz U, et al. Primary and locally recurrent retroperitoneal soft-tissue sarcoma: local control and survival. Eur J Surg Oncol. 2009;35:986–993.
Lo CM, Fan ST, Liu CL, Lai EC, Wong J. Biliary complications after hepatic resection: risk factors, management, and outcome. Arch Surg. 1998;133:156–161.
Yasuda K, Shiraishi N, Adachi Y, Inomata M, Sato K, Kitano S. Risk factors for complications following resection of large gastric cancer. Br J Surg. 2001;88:873–877.
Blumberg N, Agarwal MM, Chuang C. Relation between recurrence of cancer of the colon and blood transfusion. Br Med J (Clin Res Ed). 1985;290:1037–1039.
McAlister FA, Clark HD, Wells PS, Laupacis A. Perioperative allogeneic blood transfusion does not cause adverse sequelae in patients with cancer: a meta-analysis of unconfounded studies. Brit J Surg. 1998;85:171–178.
Michiura T, Nakane Y, Kanbara T, et al. Assessment of the preserved function of the remnant stomach in pylorus-preserving gastrectomy by gastric emptying scintigraphy. World J Surg. 2006;30:1277–1283.
Kodama Y, Zhao CM, Kulseng B, Chen D. Eating behavior in rats subjected to vagotomy, sleeve gastrectomy, and duodenal switch. J Gastrointest Surg. 2010;14:1502–1510.
Tanizawa Y, Bando E, Kawamura T, et al. Influence of a positive proximal margin on oral intake in patients with palliative gastrectomy for far advanced gastric cancer. World J Surg. 2011;35:1030–1034.
Yuasa N, Miyake H, Yamada T, Ebata T, Nimura Y, Hattori T. Clinicopathologic comparison of Siewert type II and III adenocarcinomas of the gastroesophageal junction. World J Surg. 2006;30:364–371.
Gaca JG, Petersen RP, Peterson BL, et al. Pathologic nodal status predicts disease-free survival after neoadjuvant chemoradiation for gastroesophageal junction carcinoma. Ann Surg Oncol. 2006;13:340–346.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chen, XF., Zhang, B., Chen, ZX. et al. Gastric Tube Reconstruction Reduces Postoperative Gastroesophageal Reflux in Adenocarcinoma of Esophagogastric Junction. Dig Dis Sci 57, 738–745 (2012). https://doi.org/10.1007/s10620-011-1920-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-011-1920-7