
Abstract
Objectives
To investigate radiant energy, microhardness, and temperature rise in eight resin composites cured with a blue or violet-blue curing unit, using a curing protocol which exceeded manufacturer recommendations.
Materials and methods
Cylindrical composite specimens (d = 8 mm, h = 2 or 4 mm, n = 5 per experimental group) were light-cured for 30 s. Light transmittance through specimens was recorded in real time to calculate radiant energy delivered to the specimen bottom. Vickers microhardness was used to evaluate the polymerization effectiveness at depth. Temperature rise at the bottom of the specimens was measured in real time using a T-type thermocouple.
Results
Radiant energy delivered from the blue and violet-blue curing unit amounted to 19.4 and 28.6 J/cm2, which was 19 and 13% lower than specified by the manufacturer. Radiant energies at bottom surfaces (0.2–7.5 J/cm2) were significantly affected by material, thickness, and curing unit. All of the composites reached 80% of maximum microhardness at clinically relevant layer thicknesses. The benefit of using the higher-irradiance violet-blue curing unit was identified only in composites containing alternative photoinitiators. Temperature rise during curing ranged from 4.4 to 9.3 °C and was significantly reduced by curing with the lower-intensity blue curing unit and by increasing layer thickness.
Conclusion
Curing for 30 s, which can be regarded as extended considering manufacturer specifications, produced radiant energies which are in line with the recommendations from the current scientific literature, leading to adequate curing efficiency and acceptable temperature rise.
Clinical relevance
Extended curing time should be used to minimize concerns regarding undercuring of composite restorations.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The development of high-irradiance light-emitting diode (LED) curing units has led to the shortening of time recommended for light-curing of composite materials for direct restorations. Although the concept of mathematical reciprocity of curing time and irradiance has been invalidated [1], manufacturers of curing units continue to advertise high irradiances coupled with short curing time in an attempt to appeal to the practitioner’s demands for time savings [2]. Concerns about whether the curing time recommended by manufacturers is sufficient for an adequate polymerization at the restoration bottom have been raised due to the evidence of inferior cure produced by following manufacturer guidelines regarding layer thickness, curing unit irradiance, and curing time [3,4,5]. Additionally, it has been noted that curing time advertised by manufacturers is usually minimum time required for a sufficient cure in controlled laboratory conditions and not necessarily optimal for a more complex clinical setting [6]. The issue of suboptimal cure at the restoration bottom is clinically relevant because of its negative influence on mechanical properties and biocompatibility [7, 8]. The simplest way a practitioner can overcome these issues is by extending the curing time beyond manufacturer recommendations [9]; this approach has been shown to improve the degree of conversion and microhardness at the bottom of the composite layer [4, 8, 10], while also reducing the amount of elutable species [11, 12]. Also, extended curing time may help to mitigate the effect of spatial heterogeneity of the curing unit beam, thus producing more uniformly cured restorations [13].
On the other hand, curing with high-irradiance units for extended time raises concerns regarding possible overheating of the dental pulp [14]. Much work has been done on this topic, encompassing investigations of a wide variety of composite brands [15, 16], different radiant energies and spectral characteristics of curing units [17,18,19,20], simulations of the temperature rise within the pulpal chamber [16, 17, 19, 21, 22], and attempts to define the threshold temperature value which would indicate a potentially irreversible pulpal damage [23, 24]. Despite these efforts, the multiplicity of factors involved in the heat transfer [25] and its effect on the dental pulp makes it difficult to translate laboratory data into clinically meaningful inferences [6]. Consequently, no consensus currently exists on the reference temperature values, reached either within a composite specimen or within a pulpal chamber, which would indicate potential pulpal damage [26]. This renders laboratory investigations unable to determine the actual potential for irreversible pulpal pathoses [27]. However, laboratory studies remain useful for simulating the interplay of various factors and evaluating their influence on temperature rise in the polymerizing composite.
The present study investigated radiant energy, microhardness, and temperature rise in eight composite materials at layer thicknesses of 2 and 4 mm. A blue and a violet-blue LED curing units were activated for the longest curing “program” available (30 s), delivering radiant energies which exceeded most of the manufacturer recommendations. Null hypotheses assumed no effect of composite material, curing unit, and layer thickness on (I) radiant energy, (II) Vickers microhardness (MH), and (III) temperature rise at the bottom of the composite layer. Further null hypotheses assumed (IV) no correlation between radiant energy and MH and (V) no correlation between radiant energy and temperature rise.
Materials and methods
Composite materials and curing units
Four conventional and four bulk-fill resin composites were investigated. Detailed composition and manufacturer recommendations for curing time are shown in Table 1. To evaluate the effect of pigment additives used for the adjustment of shade, composites Tetric EvoCeram (TEC) and Tetric EvoCeram Bulk Fill (TECBF) were investigated in two different shades. These composite types also contained additional photoinitiators besides camphorquinone/amine. Composite specimens were light-cured using either a blue (Bluephase Style M8, Ivoclar Vivadent, Schaan, Liechtenstein) or a violet-blue curing unit (Bluephase Style, Ivoclar Vivadent). The blue curing unit is also known by the name “Monowave” (MW), while the violet-blue is referred to as “Polywave” (PW). Emission spectra and irradiances of the curing units are shown in Fig. 1.

Emission spectra and irradiances of the blue (a) and violet-blue (b) curing unit
Radiant energy
To determine the radiant energy delivered to the bottom of 2- and 4-mm-thick composite layers, the light intensity which passed through the mold aperture was measured by integrating sphere (IS, Gigahertz Optik GmbH, Puchheim, Germany), and real-time monitoring of the light transmittance during light-curing of composite specimens was performed using a charge-coupled device array fiber spectrometer (HR4000, Ocean Optics, Dunedin, FL, USA). Composite specimens were prepared in black cylindrical Teflon molds (d = 8 mm, h = 2 or 4 mm), covered with a polyethylene terephthalate (PET) film, and light-cured for 30 s. The light transmitted through the specimen during the light-curing was collected by a lens and led to the spectrometer which recorded irradiance as a function of time at the data collection rate of 20 s−1 using custom-made software. Radiant energy (J/cm2) was calculated by integrating the area under the irradiance vs. time curve.
Microhardness
Composite specimens of the same geometry as described for the radiant energy measurements (d = 8 mm, h = 2 or 4 mm) were prepared by pressing composite pastes in black Teflon molds, covering mold apertures with a PET film and light-curing for 30 s. The specimens were then stored in dark at 37 ± 1 °C for 24 h in order to complete the post-cure reaction [28]. MH was evaluated at specimen surface (designated as 0 mm) and at the bottom of 2- or 4-mm-thick specimens. Prior to performing indentations, specimen surfaces were wet ground using a silicon carbide paper in a sequence of decreasing roughness (grits 600, 800, and 1200) for 1 min per each roughness. This was followed by a fine polishing using aluminum oxide powder mixed with distilled water in a sequence of particle sizes of 1.0, 0.3, and 0.005 μm (1 min each). The specimens were then thoroughly rinsed with distilled water and blotted with cellulose pads. Five indentations per specimen were performed using a Vickers diamond pyramid in an MH tester (Miniload 2, Leitz, Oberkochen, Germany) with a load of 100 g and a dwell time of 10 s. All of the indentations were made at the central part of specimen surface in order to minimize the variability due to spacial inhomogeneity of the curing light. Vickers MH was calculated using the following equation: MH = 1.8544 × F/d2, where d is the indentation diagonal and F = m × g (g = 9.81 N/kg, m = load). As a measure of curing efficiency at depth, the following ratio was calculated:
Temperature rise
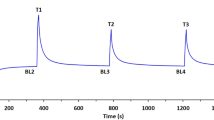
Composite specimens (d = 8 mm, h = 2 or 4 mm) were prepared in the same black Teflon molds as used for radiant energy and MH measurements. Specimen volumes were 100.5 and 200.1 mm3, respectively, corresponding to the amount of material which would be applied in a single layer in large cavities. Temperature rise was monitored in real time during the light-curing of 30 s by means of a T-type thermocouple which was positioned centrally at the bottom of composite specimens [29]. The custom-made software was used to record real-time temperature changes at the data collection rate of 20 s−1. To assess the heating effect of curing units alone, the temperature rise was measured at the bottom of the empty specimen compartment in the same manner.
The environmental temperature during all the tests was 22 ± 1 °C. For each test, five specimens per experimental group were prepared (n = 5).
Statistical analysis
Normality of distribution and homogeneity of variances were verified by Shapiro-Wilk’s and Levene’s test, respectively. For repeated MH measurements performed on the same specimen, sphericity was validated by Mauchly’s test. Mean values of temperature rise and radiant energy were compared by a three-way ANOVA with factors material, curing unit, and thickness. Mean MH values were compared using a mixed model ANOVA with material, curing unit, and thickness as independent factors and repeated measures of n = 5 per specimen as dependent observations. The mixed ANOVA was performed instead of averaging the MH data obtained from the same specimen in order to account for the clustering effect of repeated measures [30]. Tukey’s post hoc adjustment was used for multiple comparisons in all ANOVA models. Partial eta-squared statistics were used to describe the relative effect size for each factor. Pearson correlation analysis was used to relate radiant energy to the MH and temperature data. Statistical analysis was performed in SPSS 20 (IBM, Armonk, NY, USA) with α = 0.05. An exception to the overall α = 0.05 was done in the correlation analysis of radiant energy and MH, which used α = 0.1 due to the exploratory character of the analysis.
Results
Partial eta-squared values in Table 2 reflect the practical significance of factors material, curing unit, and thickness on radiant energy, MH, and temperature rise. Highly significant influence of all the factors on all dependent variables was observed. Most of the binary and ternary interactions were also significant.
Radiant energy delivered to the top surface of composite specimens amounted to 19.4 J/cm2 (MW) and 28.6 J/cm2 (PW). Radiant energies that reached the bottom surfaces were significantly affected by material, thickness, and curing unit and varied from 0.2 to 7.5 J/cm2 (Table 3).
Table 4 presents MH as a function of material, thickness, and curing unit. Conventional composites showed a significant MH decline at thicker layers, whereas the MH values of bulk-fill composites were statistically homogeneous throughout all layer thicknesses. The effect of curing unit was identified in TEC A2: significantly higher MH was attained with PW compared to MW at all layer thicknesses. The same was observed in TEC A3 but only at the surface (0 mm).
Figure 2 shows real-time light transmittance curves for the composites containing alternative initiators (TEC and TECBF). Higher light transmittance was identified for blue light (450 nm) compared to violet light (405 nm). Increasing the layer thickness from 2 to 4 mm diminished the blue light transmittance by 57% (TECBF-IVA) and 71% (TEC A2). For violet light, the corresponding reduction was 93% (TECBF-IVA) and 95% (TEC A2).

Real-time light transmittance curves for two composites containing alternative photoinitiators, recorded during curing using the violet-blue curing unit. Wavelengths of 405 and 450 nm, representing two emission peaks of the violet-blue curing unit, were considered separately. The presented curves are representative for all tested shades of TEC and TECBF
Table 5 shows MH values expressed as a percentage of the maximum MH value attained within each material. The dashed line marks the “80% of the maximum” threshold, which was considered an indicator of adequate cure. This threshold was surpassed by all bulk-fill composites, while in some conventional composites inferior cure was identified at 4 mm. Moreover, in two conventional composites (TEC A2 and TEC A3), the “80% of the maximum” requirement was marginally fulfilled at the layer thickness of 2 mm.
MH values measured at 2- and 4-mm-thick layers were correlated with the radiant energies delivered to the corresponding thicknesses. The Pearson correlation analysis was performed for each material separately and the results are shown in Table 6. Moderate correlations, significant at the 0.1 level, were identified for seven out of eight materials.
Maximum values of temperature rise measured at the bottom of composite specimens are summarized in Table 7. Overall, the temperature rise at the bottom of composite specimens was in the range of 4.4–9.3 °C. In the case of MW, the temperature rise measured at the bottom of the empty specimen compartment was significantly lower than the temperature rise at the bottom of composite specimens, while for PW, the temperature rise in the empty specimen compartment was statistically similar to the temperature rise at the bottom of composite specimens. Correlating temperature rise with radiant energy for all combinations of material × thickness × curing unit revealed a high and highly significant linear relationship (Fig. 3).

Correlation between radiant energy and temperature rise measured at the bottom of 2- and 4-mm-thick specimens
Real-time temperature curves for each combination of material × thickness × curing unit are shown in Fig. 4. Dashed vertical lines mark the curing time recommended by respective manufacturers, considering the nominal manufacturer-declared irradiances of the curing units. Most of the temperature rise occurred before the marked time, especially in bulk-fill composites, which reached a temperature plateau within the 10 s of curing (Fig. 4e–h). An additional observation from the real-time temperature curves is that for PW, the “30 s” curing mode actually lasted for 31 s.



Real-time temperature curves for various combinations of curing unit and layer thickness for conventional (a–d) and bulk-fill composites (e–h)
Discussion
This study investigated the influence of material composition, curing unit type, and layer thickness on radiant energy, MH, and temperature rise. Since all of the factors significantly affected the dependent variables, null hypotheses (I)–(III) were rejected.
Radiant energies required to adequately cure a composite layer are material-dependent and have been reported to vary between 6 and 36 J/cm2 [1, 31, 32]. Recent recommendations for practitioners mentioned 24–36 J/cm2 [1], which is comparable to incident radiant energies in the present study (19.4 J/cm2 for MW and 28.6 J/cm2 for PW), but exceeds most of the manufacturer recommendations, as these usually range between 10 and 20 J/cm2 (Table 1). In this sense, curing time, which seems “extended” considering the manufacturer guidelines, was in fact adequate for producing the recommended radiant energies [1]. Radiant energy measured at the bottom of 2- or 4-mm-thick layers was up to two orders of magnitude lower than the incident radiant energy (Table 3). This was caused by light attenuation which was highly influenced by material, thickness, and curing unit, as indicated by partial eta-squared values in Table 2. Significant interactions of the factor material with the other two factors indicate that the dependence of radiant energy on layer thickness and curing unit cannot be modeled generally for all materials because each material composition behaved differently. This fact is observable in Table 3: the effect size of thickness and curing unit on radiant energy differed from material to material. The pronounced dependence of the curing light attenuation on material composition can be understood in the context of the wide variability of optimal radiant energies measured in different studies [1, 31, 32].
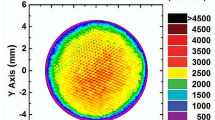
Manufacturers are known to overrate curing unit irradiances by specifying values which may be even two to three times higher than the real irradiance [33]. Additionally, spatial heterogeneity of the light beam leads to the discrepancy between the radiant energy received by the specimen and average radiant energy delivered through the whole aperture of the curing unit tip [34], since the inner part of the light guide often delivers more energy than the peripheral part [26]. Specimen diameter in the present study (8 mm) was close to the functional diameter of the light guide of 9 mm [13]; thus, the radiant energy measured through the mold opening should be similar to the averaged radiant energy of the whole light guide. However, the measured radiant energy values of 19.4 and 28.6 J/cm2 were 19 and 13% lower than the nominal values calculated from manufacturer specifications (24 and 33 J/cm2, respectively). Manufacturers’ practice of overrating the curing unit performance [6, 9, 33, 35] has practical implications since clinicians usually learn about the curing requirements from manufacturer brochures, which may provide imprecise information.
The MH values were predominantly influenced by material (partial η2 = 0.987), followed by thickness and curing unit, with partial η2 of 0.622 and 0.125, respectively. Besides having the largest effect size, the factor material showed significant interactions with other factors, indicating that different material compositions responded differently to curing units and layer thicknesses. In six out of eight materials, no statistically significant difference in MH was identified between the curing units (Table 4). In contrast, the benefit of using PW over MW was identified in TEC A2 and TEC A3, i.e., in the composites which contained both camphorquinone/amine and Lucirin TPO [6, 36, 37]: PW produced higher MH at all layer thicknesses for TEC A2 but only at the surface for TEC A3. The declining effectiveness of combined photoinitiators at increasing thicknesses has been reported to vary among different materials: the combination of camphorquinone/amine and Lucirin TPO was effective at up to 4–5 mm in model composites [14], while in commercial composites, the benefit of violet light may be completely lost already at 1.6 mm due to high light attenuation of shorter wavelengths [36, 38] (Fig. 2). What is interesting is that the effectiveness of combined photoinitiators in basically the same material composition (TEC) differed due to the shade difference. This can be explained by different ratios of the two photoinitiators [38] or, alternatively, by the effect of pigments which may intensely absorb wavelengths responsible for photo-activation [31]. The former explanation is more likely since the radiant energies at the bottom of composite layers were similar for both shades of TEC (Table 3). It should be noted that the benefit of curing with the violet-blue spectrum in TEC [32] was identified also at the specimen surface, i.e., that high radiant energies received at the surface did not compensate for the differences between curing units.
Calculating the ratio of MH at a particular layer thickness and the maximum attainable MH is a common means for evaluation of polymerization efficiency at depth (Table 5). The 80% of the maximum MH has been traditionally considered to indicate an acceptable cure [4, 8, 13, 39]; this requirement is expected to be fulfilled by following manufacturer’s instructions for use. Since manufacturer recommendations were exceeded in the present study, all of the composites fulfilled the “80% of the maximum” requirement at 2 mm for conventional and 4 mm for bulk-fill composites. However, the “80% of the maximum” criterion was met only marginally in the case of TEC A2 cured with MW and TEC A3 cured with either curing unit. Although this finding does not necessarily imply inferior clinical performance, it highlights the fact that significant inhomogeneity in mechanical properties through depth can exist despite the fact that the manufacturers’ recommendations for curing (10 s for > 1000 mW/cm2) were surpassed by a factor of 3.
Although conventional composites are not designed for use in layers thicker than 2 mm, a homogeneous cure throughout 4 mm was demonstrated to be attainable if sufficient radiant energy is used [14]. In our study, such a “bulk-fill” capability was identified in conventional composites Grandio (GRA) and TEC A2, which reached over 80% of the maximum MH at the bottom of 4-mm layers (Table 5): GRA was equally well cured by both curing units, whereas TEC A2 required the higher-irradiance violet-blue curing unit (PW). However, placing conventional composites at 4-mm-thick layers cannot be recommended on the basis of the MH data alone, as some other considerations, e.g., polymerization shrinkage and associated stress, need to be taken into account. Interestingly, TEC A3 did not reach the 80% of the maximum MH at 4 mm, demonstrating that the minor shade difference (A2/A3) may play an important role in limiting the polymerization efficiency at depth [38].
TECBF comprises camphorquinone/amine and a proprietary germanium-based photoinitiator system with maximum absorption in the violet range [40]. Unlike TEC, TECBF was homogeneously cured for up to 4 mm regardless of the curing unit (Table 5), thus showing no benefit of using PW over MW. The finding of a homogeneous cure in TECBF is in contradiction with several studies which reported a statistically significant MH decline at 4 mm when TECBF was cured using a blue LED curing unit at (1000 mW/cm2 × 20 s = 20 J/cm2) [39, 41] and a violet-blue curing unit at (1170 mW/cm2 × 30 s = 35.1 J/cm2) [4]. The decline in curing efficiency at depth was also identified in TECBF in a study which assessed MH immediately after light-curing [42], unlike the other mentioned studies [4, 39, 41] in which MH was measured 24 h post-cure. It remains unexplained why the decrease in curing efficiency at depth for TECBF was not observed in the present study, despite similar curing conditions to the studies in which it was identified.
The correlation of MH with the degree of conversion within a composite formulation is the foundation for the use of MH as an indirect measure of polymerization efficiency [6]. MH plotted as a function of radiant energy can be envisioned as asymptotically approaching the plateau at which saturation is reached, i.e., the radiant energy is sufficient to attain the maximum possible MH [43]. Before reaching the saturation point, radiant energy should correlate with MH [5]. This type of correlation was identified in seven out of eight composites (Table 6) and a moderate amount of variability in MH data was attributable to differences in radiant energy (R2 = 0.16–0.62). The lack of correlation between MH and radiant energy was observed only in X-tra fil (XF), which appears to have reached the saturation point for all combinations of curing unit × thickness. Thus, the fourth null hypothesis of no correlation between radiant energy and MH was rejected for all materials except XF.
As MW and PW differed by radiant energy and spectral emission, the relative contributions of these effects could not be separated. Additionally, two subtle differences between the curing units were identified: (I) the “30-s” curing mode actually lasted 31 s for PW and (II) the blue emission peak in MW was shifted by 9 nm towards lower wavelengths (Fig. 1), thus being less aligned with the camphorquinone absorption maximum at 468 nm [44]. This suggests that the beneficial effect of PW may not be only due to the presence of an additional violet peak but also because its blue peak was more effective in activating the conventional camphorquinone/amine photoinitiator system.
Temperature rise measured at the bottom of composite specimens (4.4–9.3 °C) was comparable to 6–8 °C reported in a study using similar specimen geometry [26]. In another study, 2-mm-thick composite layers separated from the pulpal chamber by 1-mm-thick dentin and cured with radiant energies comparable to those in the present study produced an intrapulpal temperature rise of 7–8 °C [27]. The aforementioned studies [26, 27] used thermocouples; however, other means of temperature measurements may record much higher values [45], e.g., a temperature rise of up to 43 °C was measured using infrared cameras [46]. Temperature rise due to the heating of the curing unit can also vary widely; a recent review article mentioned the range of 1.5–23.2 °C [47]. Such heterogeneity of experimental data suggests that quantitative results obtained in vitro cannot be easily interpreted in terms of the potential pulpal hazard [6, 48]. Considering these limitations, temperature values in this study were used only to assess the relative effects of material composition, curing unit, and layer thickness, with no attempt to relate the absolute temperature values to the potential for pulpal damage.
For MW, the temperature at the bottom of the composite specimens was higher than that of the empty specimen compartment, suggesting that material-dependent reaction exotherm was superimposed on the curing unit heating (Table 7). Conversely, in the case of PW, temperature values in the empty specimen compartment were statistically similar to those measured in composite specimens. This is probably because the heating contribution of PW dominated the measured temperature rise thereby masking the effect of reaction exotherm. Only TEC A3 and Gradia Direct Posterior (GDP) cured with PW at 4-mm thickness showed significantly lower temperatures compared to that of the empty specimen compartment, indicating a thermal insulating potential.
The effect of the composite amount on temperature rise is twofold. A larger amount of material represents a thicker insulating layer between the curing unit and specimen bottom at which temperature is measured. However, a larger amount of composite contains more C=C bonds and thus a larger amount of heat is released in the exothermic reaction [49]. The relative strengths of these two effects determine whether the increase in material amount acts to increase or decrease temperature rise during light-curing. Results of the present study suggest that the thermal insulating effect prevailed, as 4-mm layers consistently showed lower temperature rise than 2-mm layers (Table 7).
In ANOVA for temperature rise, curing unit type and layer thickness were more influential (partial η2 of 0.834 and 0.844, respectively) than material composition (partial η2 = 0.490). A high correlation between temperature rise and radiant energy for each material × thickness × curing unit combination (Fig. 3) suggests that temperature rise was mostly determined by variations in radiant energy reaching the specimen bottom; for an obtained R = 0.858, the coefficient of determination R2 = 0.74 means that 74% of the variability in temperature rise was attributable to changes in radiant energy. This is in line with previous studies which demonstrated that the highest contribution to the temperature rise originates from the curing unit [22, 50] and identified high linear correlations between radiant energy and temperature rise measured in the composite material [51] or in the pulpal chamber of anesthetized human teeth [52]. The fifth null hypothesis was thus rejected.
The shapes of temperature curves varied among different combinations of material, curing unit, and thickness (Fig. 4). Generally, for 2-mm layers, a steeper initial part and higher maximum values were observed compared to 4-mm layers. The temperature curves for bulk-fill composites reached maximum values within 5–10 s and plateaued thereafter. For conventional composites, temperature curves rose throughout the 30-s period at various slopes; however, most of the increase occurred within the first 10 s. These findings suggest that extending the curing time beyond manufacturer recommendations (dashed vertical lines in Fig. 4) produced a minor additional increase in temperature. This means that the maximum temperature gradient in clinical conditions would be established soon after activating the curing unit. Thus, analyzing peak temperature values without considering curing time provides an incomplete indication about the amount of heat which would be transferred to the dental pulp. For example, if TECBF was evaluated using curing time of 10, 20, and 30 s, almost the same peak temperatures would be recorded for all time points. However, the effect on pulpal tissue would differ due to different time available for heat transfer. Although the actual risk for pulpal health remains indeterminate [6, 45], the effect of time should at least be acknowledged in studies of temperature rise during light-curing of dental composites.
According to the findings of this study, temperature rise at the bottom of a composite layer can be minimized by the following approaches: (I) bulk-filling can help to mitigate the heating effect, as 4-mm layers always produced lower temperature than 2-mm layers, (II) using the lower-intensity curing unit (MW) can be advised because it produced similar cure as the higher-intensity curing unit (PW) at clinically relevant layer thicknesses, while consistently producing lower temperature than PW, and (III) if high-irradiance curing units are used, placing bulk-fill composites in 4-mm layers can be beneficial for minimizing the thermal effect on dental pulp.
Conclusions
Within the limitations of this study which evaluated radiant energy, curing efficiency, and temperature rise in composites which were light-cured for 30 s using a blue (648 mW/cm2) and a violet-blue (924 mW/cm2) LED curing unit, the following can be concluded:
-
1.
Curing with the lower-intensity curing unit produced less heat, whereas both curing units produced adequate cure at 2 mm for conventional composites and 4 mm for bulk-fill composites.
-
2.
The conventional composites containing combined photoinitiators benefitted from the use of violet-blue curing unit, while no benefit was identified in two bulk-fill composites with combined photoinitiators.
-
3.
Thicker composite layers may protect the pulp from thermal insult by producing lower temperature rise at the layer bottom.
-
4.
Temperature rise was mainly determined by radiant energy, suggesting that thermal hazard can be controlled by limiting curing parameters to optimal values.
-
5.
Most of the temperature rise occurred within 5–10 s after the start of light-curing; extending the curing time to 30 s resulted in a minor additional increase.
References
Price RB (2018) The dental curing light. In: Miletic V (ed) Dental composite materials for direct restorations. Springer International, Berlin, pp 43–62. https://doi.org/10.1007/978-3-319-60961-4_4
Rencz A, Hickel R, Ilie N (2012) Curing efficiency of modern LED units. Clin Oral Investig 16(1):173–179. https://doi.org/10.1007/s00784-010-0498-3
Nomoto R, McCabe JF, Hirano S (2004) Comparison of halogen, plasma and LED curing units. Oper Dent 29(3):287–294
Tarle Z, Attin T, Marovic D, Andermatt L, Ristic M, Taubock TT (2015) Influence of irradiation time on subsurface degree of conversion and microhardness of high-viscosity bulk-fill resin composites. Clin Oral Investig 19(4):831–840. https://doi.org/10.1007/s00784-014-1302-6
Karacolak G, Turkun LS, Boyacioglu H, Ferracane JL (2018) Influence of increment thickness on radiant energy and microhardness of bulk-fill resin composites. Dent Mater J 37(2):206–213. https://doi.org/10.4012/dmj.2017-032
Leprince J, Devaux J, Mullier T, Vreven J, Leloup G (2010) Pulpal-temperature rise and polymerization efficiency of LED curing lights. Oper Dent 35(2):220–230. https://doi.org/10.2341/09-203-L
Durner J, Obermaier J, Draenert M, Ilie N (2012) Correlation of the degree of conversion with the amount of elutable substances in nano-hybrid dental composites. Dent Mater 28(11):1146–1153. https://doi.org/10.1016/j.dental.2012.08.006
Miletic V, Pongprueksa P, De Munck J, Brooks NR, Van Meerbeek B (2017) Curing characteristics of flowable and sculptable bulk-fill composites. Clin Oral Investig 21(4):1201–1212. https://doi.org/10.1007/s00784-016-1894-0
Ernst CP, Price RB, Callaway A, Masek A, Schwarm H, Rullmann I, Willershausen B, Ehlers V (2018) Visible light curing devices—irradiance and use in 302 German dental offices. J Adhes Dent 20(1):41–55. https://doi.org/10.3290/j.jad.a39881
Zorzin J, Maier E, Harre S, Fey T, Belli R, Lohbauer U, Petschelt A, Taschner M (2015) Bulk-fill resin composites: polymerization properties and extended light curing. Dent Mater 31(3):293–301. https://doi.org/10.1016/j.dental.2014.12.010
Hogg C, Maier M, Dettinger-Maier K, He X, Rothmund L, Kehe K, Hickel R, Reichl FX (2016) Effect of various light curing times on the elution of composite components. Clin Oral Investig 20(8):2113–2121. https://doi.org/10.1007/s00784-015-1698-7
Ilie N, Obermaier J, Durner J (2014) Effect of modulated irradiation time on the degree of conversion and the amount of elutable substances from nano-hybrid resin-based composites. Clin Oral Investig 18(1):97–106. https://doi.org/10.1007/s00784-013-0934-2
Price RB, Labrie D, Rueggeberg FA, Sullivan B, Kostylev I, Fahey J (2014) Correlation between the beam profile from a curing light and the microhardness of four resins. Dent Mater 30(12):1345–1357. https://doi.org/10.1016/j.dental.2014.10.001
Palin WM, Leprince JG, Hadis MA (2018) Shining a light on high volume photocurable materials. Dent Mater 34(5):695–710. https://doi.org/10.1016/j.dental.2018.02.009
Shortall A, El-Mahy W, Stewardson D, Addison O, Palin W (2013) Initial fracture resistance and curing temperature rise of ten contemporary resin-based composites with increasing radiant exposure. J Dent 41(5):455–463. https://doi.org/10.1016/j.jdent.2013.02.002
Baroudi K, Silikas N, Watts DC (2009) In vitro pulp chamber temperature rise from irradiation and exotherm of flowable composites. Int J Paediatr Dent 19(1):48–54. https://doi.org/10.1111/j.1365-263X.2007.00899.x
Yazici AR, Muftu A, Kugel G, Perry RD (2006) Comparison of temperature changes in the pulp chamber induced by various light curing units, in vitro. Oper Dent 31(2):261–265. https://doi.org/10.2341/05-26
Ozturk B, Ozturk AN, Usumez A, Usumez S, Ozer F (2004) Temperature rise during adhesive and resin composite polymerization with various light curing sources. Oper Dent 29(3):325–332
Vandewalle KS, Roberts HW, Tiba A, Charlton DG (2005) Thermal emission and curing efficiency of LED and halogen curing lights. Oper Dent 30(2):257–264
Yap AU, Soh MS (2003) Thermal emission by different light-curing units. Oper Dent 28(3):260–266
Goodis HE, White JM, Gamm B, Watanabe L (1990) Pulp chamber temperature changes with visible-light-cured composites in vitro. Dent Mater 6(2):99–102. https://doi.org/10.1016/S0109-5641(05)80038-7
Ratih DN, Palamara JE, Messer HH (2007) Temperature change, dentinal fluid flow and cuspal displacement during resin composite restoration. J Oral Rehabil 34(9):693–701. https://doi.org/10.1111/j.1365-2842.2007.01764.x
Zach L, Cohen G (1965) Pulp response to externally applied heat. Oral Surg Oral Med Oral Pathol 19:515–530
Baldissara P, Catapano S, Scotti R (1997) Clinical and histological evaluation of thermal injury thresholds in human teeth: a preliminary study. J Oral Rehabil 24(11):791–801. https://doi.org/10.1111/j.1365-2842.1997.tb00278.x
Lin M, Xu F, Lu TJ, Bai BF (2010) A review of heat transfer in human tooth—experimental characterization and mathematical modeling. Dent Mater 26(6):501–513. https://doi.org/10.1016/j.dental.2010.02.009
Uhl A, Mills RW, Jandt KD (2003) Polymerization and light-induced heat of dental composites cured with LED and halogen technology. Biomaterials 24(10):1809–1820. https://doi.org/10.1016/s0142-9612(02)00585-9
Hannig M, Bott B (1999) In-vitro pulp chamber temperature rise during composite resin polymerization with various light-curing sources. Dent Mater 15(4):275–281. https://doi.org/10.1016/S0109-5641(99)00047-0
Par M, Gamulin O, Marovic D, Klaric E, Tarle Z (2014) Effect of temperature on post-cure polymerization of bulk-fill composites. J Dent 42(10):1255–1260. https://doi.org/10.1016/j.jdent.2014.08.004
Par M, Gamulin O, Marovic D, Skenderovic H, Klaric E, Tarle Z (2016) Conversion and temperature rise of remineralizing composites reinforced with inert fillers. J Dent 48:26–33. https://doi.org/10.1016/j.jdent.2016.03.008
Sever I, Klaric E, Tarle Z (2016) Accounting for measurement reliability to improve the quality of inference in dental microhardness research: a worked example. Clin Oral Investig 20(6):1143–1149. https://doi.org/10.1007/s00784-015-1600-7
Price RB, Fahey J, Felix CM (2010) Knoop hardness of five composites cured with single-peak and polywave LED curing lights. Quintessence Int 41(10):e181–e191
Santini A, Miletic V, Swift MD, Bradley M (2012) Degree of conversion and microhardness of TPO-containing resin-based composites cured by polywave and monowave LED units. J Dent 40(7):577–584. https://doi.org/10.1016/j.jdent.2012.03.007
Gomes M, DeVito-Moraes A, Francci C, Moraes R, Pereira T, Froes-Salgado N, Yamazaki L, Silva L, Zezell D (2013) Temperature increase at the light guide tip of 15 contemporary LED units and thermal variation at the pulpal floor of cavities: an infrared thermographic analysis. Oper Dent 38(3):324–333. https://doi.org/10.2341/12-060-L
Shimokawa CAK, Turbino ML, Giannini M, Braga RR, Price RB (2018) Effect of light curing units on the polymerization of bulk fill resin-based composites. Dent Mater 34:1211–1221. https://doi.org/10.1016/j.dental.2018.05.002
Price RB, Fahey J, Felix CM (2010) Knoop microhardness mapping used to compare the efficacy of LED, QTH and PAC curing lights. Oper Dent 35(1):58–68. https://doi.org/10.2341/09-055-L
Shimokawa C, Sullivan B, Turbino ML, Soares CJ, Price RB (2017) Influence of emission spectrum and irradiance on light curing of resin-based composites. Oper Dent 42(5):537–547. https://doi.org/10.2341/16-349-L
Palin WM, Senyilmaz DP, Marquis PM, Shortall AC (2008) Cure width potential for MOD resin composite molar restorations. Dent Mater 24(8):1083–1094. https://doi.org/10.1016/j.dental.2008.01.001
Price RB, Felix CA (2009) Effect of delivering light in specific narrow bandwidths from 394 to 515nm on the micro-hardness of resin composites. Dent Mater 25(7):899–908. https://doi.org/10.1016/j.dental.2009.01.098
Flury S, Peutzfeldt A, Lussi A (2014) Influence of increment thickness on microhardness and dentin bond strength of bulk fill resin composites. Dent Mater 30(10):1104–1112. https://doi.org/10.1016/j.dental.2014.07.001
Moszner N, Fischer UK, Ganster B, Liska R, Rheinberger V (2008) Benzoyl germanium derivatives as novel visible light photoinitiators for dental materials. Dent Mater 24(7):901–907. https://doi.org/10.1016/j.dental.2007.11.004
El-Damanhoury H, Platt J (2014) Polymerization shrinkage stress kinetics and related properties of bulk-fill resin composites. Oper Dent 39(4):374–382. https://doi.org/10.2341/13-017-L
AlShaafi MM, Haenel T, Sullivan B, Labrie D, Alqahtani MQ, Price RB (2016) Effect of a broad-spectrum LED curing light on the Knoop microhardness of four posterior resin based composites at 2, 4 and 6-mm depths. J Dent 45:14–18. https://doi.org/10.1016/j.jdent.2015.11.004
Rodrigues JA, Tenorio IP, Mello GBR, Reis AF, Shen C, Roulet JF (2017) Comparing depth-dependent curing radiant exposure and time of curing of regular and flow bulk-fill composites. Braz Oral Res 31:e65. https://doi.org/10.1590/1807-3107BOR-2017.vol31.0065
Jakubiak J, Allonas X, Fouassier JP, Sionkowska A, Andrzejewska E, Linden LÅ, Rabek JF (2003) Camphorquinone–amines photoinitating systems for the initiation of free radical polymerization. Polymer 44(18):5219–5226. https://doi.org/10.1016/s0032-3861(03)00568-8
Bouillaguet S, Caillot G, Forchelet J, Cattani-Lorente M, Wataha JC, Krejci I (2005) Thermal risks from LED- and high-intensity QTH-curing units during polymerization of dental resins. J Biomed Mater Res B Appl Biomater 72(2):260–267. https://doi.org/10.1002/jbm.b.30143
Al-Qudah AA, Mitchell CA, Biagioni PA, Hussey DL (2005) Thermographic investigation of contemporary resin-containing dental materials. J Dent 33(7):593–602. https://doi.org/10.1016/j.jdent.2005.01.010
Rueggeberg FA, Giannini M, Arrais CAG, Price RBT (2017) Light curing in dentistry and clinical implications: a literature review. Braz Oral Res 31(suppl 1):e61. https://doi.org/10.1590/1807-3107BOR-2017.vol31.0061
Park SH, Roulet JF, Heintze SD (2010) Parameters influencing increase in pulp chamber temperature with light-curing devices: curing lights and pulpal flow rates. Oper Dent 35(3):353–361. https://doi.org/10.2341/09-234-L
Lloyd CH, Brown EA (1984) The heats of reaction and temperature rises associated with the setting of bonding resins. J Oral Rehabil 11(4):319–324. https://doi.org/10.1111/j.1365-2842.1984.tb00582.x
Daronch M, Rueggeberg FA, Hall G, De Goes MF (2007) Effect of composite temperature on in vitro intrapulpal temperature rise. Dent Mater 23(10):1283–1288. https://doi.org/10.1016/j.dental.2006.11.024
Asmussen E, Peutzfeldt A (2005) Temperature rise induced by some light emitting diode and quartz-tungsten-halogen curing units. Eur J Oral Sci 113(1):96–98. https://doi.org/10.1111/j.1600-0722.2004.00181.x
Runnacles P, Arrais CA, Pochapski MT, Dos Santos FA, Coelho U, Gomes JC, De Goes MF, Gomes OM, Rueggeberg FA (2015) In vivo temperature rise in anesthetized human pulp during exposure to a polywave LED light curing unit. Dent Mater 31(5):505–513. https://doi.org/10.1016/j.dental.2015.02.001
Acknowledgments
Composite materials Tetric EvoCeram and Tetric EvoCeram Bulk Fill and curing units were generously provided by Ivoclar Vivadent.
Funding
This work received no external funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study, formal consent is not required.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Par, M., Repusic, I., Skenderovic, H. et al. The effects of extended curing time and radiant energy on microhardness and temperature rise of conventional and bulk-fill resin composites. Clin Oral Invest 23, 3777–3788 (2019). https://doi.org/10.1007/s00784-019-02807-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-019-02807-1